Western University Western University
Scholarship@Western
Scholarship@Western
Electronic Thesis and Dissertation Repository
3-21-2017 12:00 AM
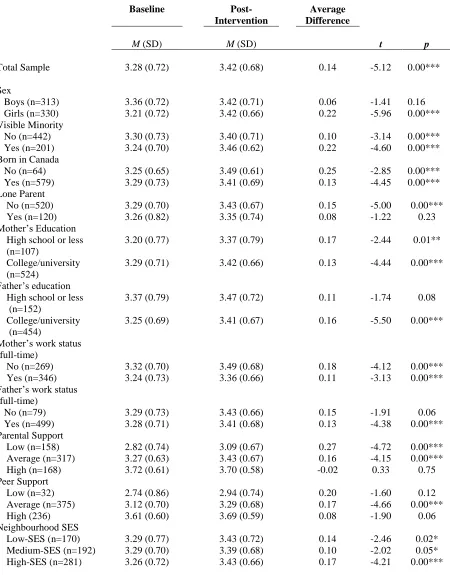
Examining the Impact of a Population-Based Intervention on
Examining the Impact of a Population-Based Intervention on
Children's Physical Activity Levels: The Grade 5 ACT-i-Pass
Children's Physical Activity Levels: The Grade 5 ACT-i-Pass
Program in London, Ontario
Program in London, Ontario
Christine E. Smith
The University of Western Ontario Supervisor
Dr. Jason Gilliland
The University of Western Ontario Graduate Program in Geography
A thesis submitted in partial fulfillment of the requirements for the degree in Master of Science © Christine E. Smith 2017
Follow this and additional works at: https://ir.lib.uwo.ca/etd
Part of the Human Geography Commons, and the Maternal and Child Health Commons
Recommended Citation Recommended Citation
Smith, Christine E., "Examining the Impact of a Population-Based Intervention on Children's Physical Activity Levels: The Grade 5 ACT-i-Pass Program in London, Ontario" (2017). Electronic Thesis and Dissertation Repository. 4427.
Abstract
Childhood obesity is a major public health concern caused in part by decreasing levels of
physical activity (PA). Identification of effective population level strategies for increasing
children’s PA levels is critical for improving overall health. This thesis is comprised of two
studies. Study 1 examines how naturally-occurring population-level PA interventions with
children have been evaluated in previous studies by conducting a systematic review. A total of
15 papers were included for review and results suggest that naturally-occurring population-based
PA interventions are generally effective in improving PA levels of children in a variety of PA
domains. Eleven studies included additional evaluation components to help justify results and
provide important contextual information. Using an ecological framework, Study 2 investigates
how the provision of a naturally-occurring population-based PA intervention in London, Ontario
impacted children’s PA levels. A total of 643 children completed baseline and post-intervention
surveys. Results showed a significant increase in PA over time, with significant increases for
girls, visible minorities, children born outside of Canada, children with low parental support, and
children from all neighbourhood SES groups. Sex and parental support were the only significant
predictors of change in PA. Examining naturally-occurring population-based PA interventions is
a beneficial opportunity that should be used by researchers to provide real-world evidence of
effective strategies to assess and increase children’s levels of PA.
Keywords
Co-Authorship Statement
Both integrated articles within this thesis will be submitted for publication in
peer-reviewed journals. Chapter 2 and Chapter 3 are my original work, with Dr. Jason Gilliland, Dr.
Andrew Clark and Dr. Piotr Wilk as co-authors on Chapter 3. I am the primary author and
performed all data collection, analysis, and writing of each article. Dr. Jason Gilliland designed
the evaluation of the ACT-i-Pass study, and Dr. Gilliland, Dr. Clark, and Dr. Wilk were involved
Acknowledgements
I would first and foremost like to thank my supervisor, Jason Gilliland. Your knowledge,
passion, and experience within academia allowed me to develop my research abilities and gain
invaluable skills, which I will always be grateful for.
Dr. Andrew Clark, it has been a pleasure working with you on the ACT-i-Pass project
since I started at the HEAL in 2014. You have been such a patient mentor during my time as a
graduate student and I don’t know what I would have done without your support, guidance and
good humour. I have learned so much from you.
Christine Mitchell and Sarah McCans, no words can describe how appreciative I am to
have had the support from both of you throughout this process. You both helped me through the
difficult times I experienced on this journey and I don’t know what I would have done without
your encouragement and friendship.
To all my lab mates, it has been a pleasure working alongside all of you for the past two
years. It is through this supportive environment that we are able to all succeed, and for that, I am
truly thankful. I would like to thank all our community partners in the ACT-i-Pass project and all
the students, parents, teachers, principals and school staff that participated in the project. I would
like to acknowledge the field work leaders who helped with this project, especially Sabrina Sater,
Christine Mitchell, Joannah Campbell; and more than 20 additional undergraduate research
assistants for there time and dedication to this project.
Finally, to my family and friends, thank you for all the love and support you have given
me. You have all patiently listened to my rants, been there throughout the difficult times, and
Table of Contents
Abstract... i
Keywords ... i
Co-Authorship Statement ... ii
Acknowledgements ... iii
Table of Contents ... iv
List of Tables ... vii
List of Figures... viii
List of Appendices ... ix
Introduction ... 1
Research Context ... 1
Intervention Studies ... 4
Theoretical Framework ... 5
Research Objectives ... 8
Thesis Format ... 10
References ... 12
Using Natural Experiments to Evaluate Population-level PA Interventions with Children: A Systematic Review ... 22
Introduction ... 22
2.1.1. Measuring Physical Activity ... 23
Methods ... 26
2.2.1. Eligibility Criteria ... 26
2.2.2. Search Strategy and Selection of Studies ... 26
2.2.3. Data Extraction ... 29
Evidence Synthesis ... 29
2.3.1. General Characteristics of the Reviewed Studies ... 29
2.3.2. Types of Methods and Measures Used ... 32
2.3.3. Physical Activity Outcomes ... 33
2.3.4. Other Factors that Influenced PA Outcomes ... 38
Discussion... 39
2.4.1. Strengths and Limitations ... 43
2.4.2. Suggestions for Future Research ... 43
Conclusions ... 44
References ... 45
Impact Evaluation of the ACT-i-Pass Program: Assessing the Effectiveness of a Naturally-Occurring Population-Level PA Intervention for Children ... 65
Background... 65
3.1.1. Factors Associated with Children’s PA ... 66
3.1.2. Intervention Studies ... 68
3.1.3. Details of the Grade 5 ACT-i-Pass Intervention ... 69
3.1.4. Study Objectives ... 71
Methods ... 72
3.2.2. Study Population and Recruitment ... 72
3.2.3. Data Collection ... 73
3.2.4. Measures ... 74
3.2.5. Statistical Analyses ... 77
Results ... 78
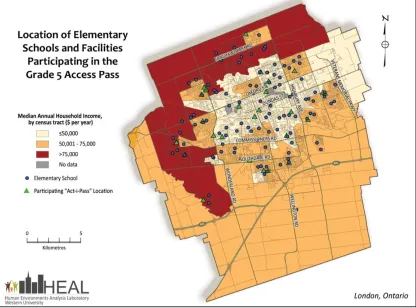
3.3.1. Characteristics of the Sample ... 78
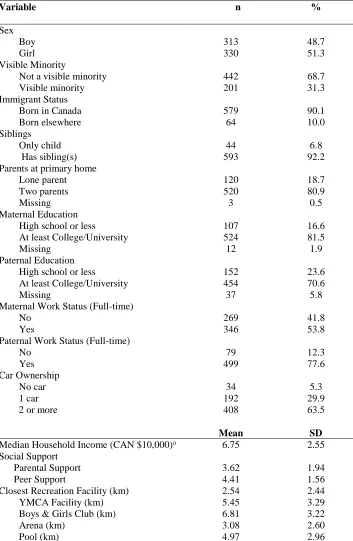
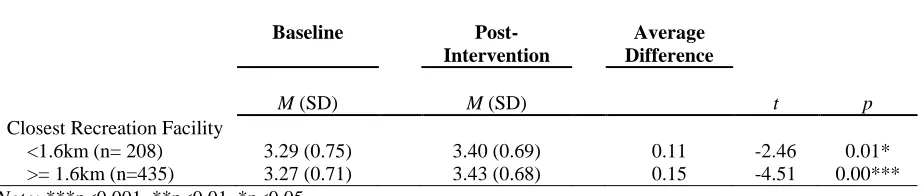
3.3.2. Average Differences in Self-Reported PA ... 80
3.3.3. Regression Analyses ... 82
Discussion and Conclusion... 85
3.4.1. Strengths and Limitations ... 89
Conclusion ... 90
References ... 91
Synthesis ... 101
Summary of the Findings ... 101
Research Contributions ... 102
Limitations ... 105
Implications for Policy and Practice... 106
Future Research ... 109
Conclusions ... 111
References ... 113
APPENDICES ... I
List of Tables
Table 1.1 Prominent theories in physical activity research provided by Buchan et al. (2012) &
Glantz et al. (2008). ... 6
Table 2.1 General characteristics of the papers reviewed. ... 31
Table 2.2 Measurement characteristics of the reviewed papers ... 33
Table 2.3 Results of the reviewed papers by physical activity domain ... 34
Table 2.4 Integrated review table with data extracted from articles examining naturally-occurring population-level PA interventions with children ... 59
Table 3.1 Characteristics of the Study Participants (n=643) ... 79
Table 3.2 Average differences in self-reported PA from baseline to post-intervention by subgroups (n=643) ... 81
List of Figures
Figure 1.1 Ecological model adapted from Mitchell et al. (2016) & Sallis et al. (2006) ... 8
Figure 2.1 Systematic Review Flow Chart ... 28
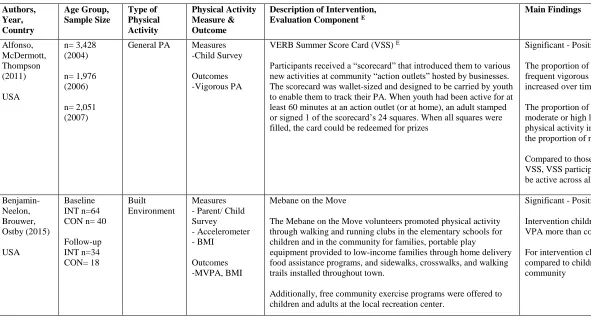
Figure 3.1 Location of elementary schools and facilities participating in the ACT-i-Pass
List of Appendices
Appendix A Location of Schools and Facilities Participating in the ACT-i-Pass Program ... I
Appendix B Recruitment Letter ... II
Appendix C ACT-i-Pass Child Survey ... IV
Appendix D ACT-i-Pass Parent Survey ... XI
Appendix E Physical Activity Questionnaire for Children (PAQ-C) ... XVII
Introduction
Research Context
Over the last 25 years, the dramatic increase in obesity rates among children and
adolescents has become a major public health concern in Canada (Chaput et al., 2012; Colley et
al., 2011; Janssen et al., 2005). According to Statistics Canada (2015), almost one third of
children and youth ages 5 to 17 years are classified as overweight or obese. While
epidemiological studies show a steady trend in the rate of overweight and obesity in youth
(Allison et al., 2015; Roberts et al., 2012), disparities between socioeconomic and ethnic groups
are growing (Singh et al., 2010).
Obesity is the result of a sustained energy imbalance from an increase in energy intake
and/or decrease in energy expenditure (Hill et al., 2012); however, understanding the complexity
of this energy imbalance is a continued challenge. Childhood obesity is problematic for a number
of reasons, primarily the several negative consequences related to physical health, mental health,
quality of life and longevity (Gurvinder et al., 2012; Halfon et al., 2013; Jansen et al., 2013;
Must et al., 1999; Schwimmer et al., 2003). Numerous clinical studies have confirmed a link
between childhood obesity and cardiovascular disease, hypertension, type II diabetes mellitus,
metabolic syndrome, orthopaedic issues, asthma, fatty liver disease and gastrointestinal diseases
issues (Must et al., 1999; Reilly et al., 2011; Pulgarón et al., 2013). In addition to the
health-related outcomes, obesity is associated with a plethora of negative psychological outcomes
including low self-esteem, body dissatisfaction, social isolation, anxiety, and depressive
symptoms (Puder & Munsch, 2010;Pulgarón et al., 2013; Wardle & Cooke, 2005).
address this health issue. Physical activity (PA) is one such lifestyle factor that can directly
impact the obesity levels of children by increasing energy expenditure. Engaging in regular PA
during childhood protects against the risk factors associated with obesity (Janssen & LeBlanc,
2010; Shaibi et al., 2008). PA is also associated with psychological and social benefits such as
improved academic performance, higher self-esteem, enhanced social support and reduced
depressive symptoms (Trudeau & Shephard, 2010; Piko et al., 2006). Despite the benefits, a
majority of children do not engage in enough PA, as only 9% of Canadian children (age 5-17)
meet Canada’s recommended guidelines of 60 minutes of moderate-to-vigorous intensity on
most days of the week (ParticipACTION, 2016).
The overarching purpose of this thesis is to contribute to our understanding of the
determinants of children’s PA levels. More specifically, this thesis focuses on population-level
interventions designed to increase children’s PA. The aim is to provide a comprehensive
understanding of factors that may impact children’s PA, in addition to contributing research to
develop more effective intervention strategies based on the findings.
Reasons for not engaging in physical activity are complex, as the behaviour is highly
variable and influenced by multiple factors at different levels (Sallis et al., 2006). A number of
socio-demographic factors (age, ethnicity, sex, SES and immigrant status) have been identified
as underlying determinants of PA in children (Brodersen et al., 2007; Bryan et al., 2006; Colley
et al., 2011; Mitchell et al., 2016; Sallis et al., 2000; Singh et al., 2008). Patterns of decline in PA
show that age is a critical factor (Sallis et al., 2000), as many studies suggest that PA declines
rapidly from childhood to adolescence, with more dramatic decreases for females (Brodersen et
al., 2007; Canadian Fitness & Lifestyle Research Institute [CFLRI], 2010; Colley et al., 2011;
genders showed a reduction in PA levels and an increase in sedentary behaviours beginning at
age 11 (Brodersen et al., 2007). Intervening during this stage of development and establishing
active lifestyles early is crucial in order for PA habits to persist into adulthood (Telama et al.,
2005). While PA levels have been shown to be low for Canadian children in general (Colley et
al., 2011), certain sub-groups of children and recent immigrants face an increased risk for
insufficient activity levels (Brodersen et al., 2007; Bryan et al., 2006; Gordon-Larsen et al.,
1999; Singh et al., 2008)
In addition, several social factors are suggested to influence children’s PA. Social support
from parents and peers demonstrate positive effects on children’s PA (Beets et al., 2006; Barkley
et al., 2014; Duncan et al., 2005). Several studies suggest that parents positively influence their
children’s PA through supportive actions, such as encouraging children to play, providing
transportation to PA opportunities, watching children participate in activities and actively
engaging with children (Beets et al., 2006; Duncan et al., 2005; Sallis et al., 2000; Trost &
Loprinzi, 2011; Welk, Wood, & Morss, 2003). Similarly, research on peer support suggests that
the presence and supportive actions from friends improves physical levels (Duncan et al., 2005;
Salvy et al., 2009). Although the presence of social support positively impacts children’s activity
levels, inconsistencies exist in terms of methods used to assess social support and what types of
supportive actions are related to increased PA levels (Beets et al., 2010; Sallis et al., 2000)
On a broader scale, numerous studies have linked supportive neighbourhood environments
(e.g., parks and recreational facility proximity) to increased PA behaviour (Davison & Lawson,
2006; Giles-Corti & Donovan, 2002; Mitchell et al., 2016; Norman et al., 2006; Powell et al.,
2003; Gordon-Larsen et al., 2006; Mitchell et al., 2016; Roemmich et al., 2006; Tucker et al.,
2009; Powell et al., 2007). Gordon-Larsen and colleagues (2006) found that youth who lived in a
neighbourhood with one recreational facility were more likely to engage in 5 or more bouts of
moderate-to-vigorous PA per week. The presence of recreational facilities may depend on the
socio-economic status (SES) of the neighbourhood, as research suggests that individuals who
live in low and medium SES neighbourhoods had fewer PA resources (i.e., areas used for PA
such as parks, community centers, dance studios) available and fewer free PA opportunities,
compared to high SES neighbourhoods (Estabrooks et al., 2003; Gorden-Larsen et al., 2006).
Intervention Studies
The multiple factors that influence children’s PA underscore the need to develop effective
interventions to modify these factors. Interventions are an effective tool for testing current
understandings and learning from the action taken in order to identify effective strategies that
improve children’s PA (Hawe & Potvin, 2009).
A growing number of studies are examining the effectiveness of community-based
interventions to promote children’s PA. Children spend a considerable amount of time outside of
school and community-based interventions provide an opportunity to research children in their
natural environment by increasing PA opportunities within the community (Brand et al., 2014;
van Sluijs et al., 2011; Perry et al., 2012; Sallis et al., 2008). Community-based interventions are
desirable as they allow for a greater reach of the targeted population, pooled resources to
enhance interventions (Bopp & Fallon, 2008), and have the potential to achieve population-level
change in PA levels (Sallis et al., 2008). Current research suggests that the most effective and
sustainable PA interventions involve large-scale collaboration among multiple sectors of the
Sallis et al., 2008). While large-scale collaborations are effective, they can be challenging to
organize, as it requires the coordination of many different groups in order to develop, implement
and evaluate an intervention (Bopp & Fallon, 2008).
Most researchers are not in a position to develop community-level interventions
independently, partly due to the resources (i.e., time, cost, administration, staff) needed to
conduct an intervention at the population-level. To bypass this issue, researchers can take
advantage of already occurring community-based interventions and evaluate them as a ‘natural
experiment.’ A natural experiment can be used to evaluate interventions where individuals in
experimental conditions are determined by nature or other factors outside the control of the
researchers (Craig et al., 2012; Petticrew et al., 2005). Natural experiments can also be referred
to as occurring’ interventions. The terms ‘natural experiment’ and
‘naturally-occurring’ are used interchangeably throughout the thesis, as the terms both represent
interventions that are initiated by an external agency and are not under the direct control of
researchers.
Natural experiments allow researchers to evaluate population-level PA interventions that
may not be possible as a controlled experiment and provide evidence of real-world effectiveness
(Petticrew et al., 2005). Although natural experiments have potential to evaluate population-level
change, they are not frequently used in PA interventions with children (Petticrew et al., 2005).
Theoretical Framework
In the past, theories and frameworks largely focused on the social influences and
psychological mechanism that impact PA behaviour. PA research and practice has been guided
Self-Determination Theory, and Transtheoretical Model (Buchan, Ollis, Thomas, Baker, 2012). A
brief description of each theory can be found in Table 1.1.
Table 1.1 Prominent theories in physical activity research provided by Buchan et al. (2012) & Glantz et al. (2008).
Name of Theory or Framework Description
Social Cognitive Theory Social Cognitive Theory suggests that behaviour, cognition, and other personal features have reciprocal relationships with environments. When predicting behaviour, self-efficacy has been found as the most powerful factor to consider.
Theory of Planned Behaviour Theory of Planned Behaviour builds upon the Theory of Reasoned Action and posits that the most important predictor of behaviour is behavioural intention. Intention is a determinant of one’s attitude, subjective norms and perceived control over performing the behaviour
Self-Determination Theory Self-Determination Theory focuses on how a person attains the motivation for starting new health behaviours and maintaining them. This theory states that human behaviour is driven to meet three basic needs: competence, autonomy, and relatedness. Behavioural outcomes will occur when these three basic needs are met.
Transtheoretical Model Behaviour change has been characterized as a five-stage process or continuum related to a person’s readiness to change: pre-contemplation, contemplation, preparation, action and maintenance. Each stage is characterized by different psychosocial and behaviour changes.
Although these theories and frameworks present different features, the core purpose is
focused on changing individual behaviour. The application of these theories has greatly
enhanced our understanding of key psychological influences and processes related to PA
behaviour (Buchan et al., 2012). A number of effective PA interventions have used these
theories, though little has changed in terms of PA outcomes for children (Buchan et al., 2012).
The focus on individual change limits the long-term maintenance of the behaviour (Bock et al.,
population-wide impact, as other sources of influence (i.e., social support, community, built environment)
are not considered (Sallis et al., 2008).
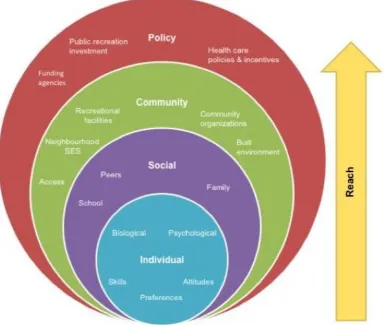
Recently, there has been a growing interest towards the application of ecological models in
PA research and practice, due to their ability to guide comprehensive population-wide
approaches to changing PA behaviours (Sallis et al., 2008). Ecological models of health address
a behaviour using a range of factors across multiple levels of influence including intrapersonal
(i.e., sex, age, attitudes), interpersonal (i.e., social support, household income), community,
physical environment, and policy (Sallis et al., 2008) (see Figure 1.1).
When developing comprehensive interventions to target PA, ecological models provide a
useful approach as they systematically assess mechanisms of change at the multiple levels of
influence. While this approach is relevant for population-level interventions, it is also useful for
addressing how place interacts with behaviour. PA occurs in specific places and the ecological
model provides a framework to identifying the characteristics of places that facilitate or hinder
PA (Sallis et al., 2006; Sallis et al., 2008). For these reasons, an ecological model of health
guides this thesis in order to develop a more thorough understanding of the multiple levels of
Figure 1.1 Ecological model adapted from Mitchell et al. (2016) & Sallis et al. (2006)
Research Objectives
The overarching objective of this research is to contribute to a growing body of literature
assessing the effectiveness of population-based PA interventions with children. This research
aims to better understand how naturally-occurring population-based interventions influence
children’s PA and what other factors promote or hinder children’s PA. This understanding is
necessary to develop effective strategies, guide future intervention and inform policy-makers
To achieve these objectives, this research uses both primary and secondary data. First,
secondary literature will be used to conduct an integrative review to address the following
research question:
(1) How have naturally-occurring population-based PA interventions with children been
evaluated in previous studies?
Primary data will then be used to evaluate a population-level PA intervention to address the
following research question:
(2) How does the provision of a naturally-occurring population-level intervention change
children’s level of PA over time in London, ON?
To answer the first research question, this study draws data from existing literature to
identify articles that examine naturally-occurring population-level PA interventions with children
to determine how these studies are being evaluated and what methods and measures are used.
This review aims to summarize and evaluate previous literature by identifying gaps in current
research, identifying prominent issues in the studies, and exploring which methods and measures
have been used successfully.
To address the second research question, this study draws data from a city-wide initiative
launched by London’s Child and Youth Network (CYN) called the Grade 5 ACT-i-Pass project
(ACT-i-Pass). London, Ontario is a mid-sized Canadian city located in Southwestern Ontario
with approximately 366,151 inhabitants, 23% of whom (84,080) were 19 years of age or younger
according to the 2011 Census of Canada (Statistics Canada, 2012). The ACT-i-Pass program
developed by the CYN (www.londoncyn.ca) provided all grade five children in the City of
study used a longitudinal cohort design to evaluate the impact of a naturally-occurring
intervention on children’s PA levels (Gilliland et al., 2015). During the study period, participants
were recruited to register for the program and parental consent was provided to those students
who took part in the research portion. Data collection comprised of four measurement periods
over an 18-month period in which children and parents completed self-report questionnaires
about their socio-demographics (i.e., sex, age, race, family composition), postal code, leisure
time activity, PA levels, barriers to PA, perceived accessibility to and use of recreational
facilities in their neighbourhood, and perceived parental and peer support. This thesis focuses
specifically on two measurement periods (baseline and post-intervention), approximately a
12-month period between each questionnaire. Methods are explained in greater detail in each
integrated article (Chapter 2 and Chapter 3).
PA remains a complex health behaviour influenced by a range of factors across multiple
levels (i.e., intrapersonal, interpersonal, community, environment). Accordingly, this thesis
hypothesizes that factors at each of these levels may impact the success of interventions and
therefore seeks to understand the factors that are associated with change in children’s PA. This
research accounts for several variables known to influence PA occurring at the individual-,
social- and neighbourhood-level.
Thesis Format
This thesis follows an integrated article format, comprised of two independent but related
studies. Both studies examine how naturally-occurring population-based PA interventions
influence children’s PA levels. While each study has the same overarching objective, the specific
objectives are met using different approaches. The first study aims to provide insight on how
intervention in London, Ontario. In doing so, this thesis aims to provide more knowledge of
effective population-level PA interventions with children. Brief descriptions of each thesis
chapter are provided below.
Chapter 2 reviews existing literature examining naturally-occurring population-level PA
interventions with children by conducting a systematic review. This review identifies the current
methods and measures used to evaluate PA, identifies successful and unsuccessful components
of the studies, and what external factors influence PA outcomes.
Chapter 3 examines how the provision of a naturally-occurring population-level PA
intervention changes children’s level of PA over time in London, Ontario. This study addresses
whether the intervention was successful in improving children’s PA levels, examines differences
in pre- and post-intervention PA in subgroups of children, and investigates individual, social and
neighbourhood characteristics that predict PA change.
Chapter 4 summarizes and connects the findings from each integrated article. This chapter
References
Allison, K. R., Irving, H. M., Adlaf, E. M., Faulkner, G. E. J., Boak, A., Manson, H. E. (2015).
Ten-year trends in overweight/obesity among Ontario middle and high school students and
their use in establishing baseline measures for government reduction targets. Canadian
Journal of Public Health, 106(8), e514–e519. http://doi.org/10.17269/CJPH.106.5175
Beets, M. W., Weaver, R. G., Turner-Mcgrievy, G., Huberty, J., Ward, D. S., Pate, R. R., …
Beighle, A. (2015). Making policy practice in afterschool programs: A randomized
controlled trial on PA changes. American Journal of Preventive Medicine, 48(6), 694–706.
http://doi.org/10.1016/j.amepre.2015.01.012
Beets, M. W., Cardinal, B. J., & Alderman, B. L. (2010). Parental Social Support and the PA –
Related Behaviors of Youth : A Review. Health Education & Behavior : The Official
Publication of the Society for Public Health Education, 37(October), 621–644.
http://doi.org/10.1177/1090198110363884
Beets, M. W., Vogel, R., Forlaw, L., Pitetti, K. H., & Cardinal, B. J. (2006). Social support and
youth PA: The role of provider and type. American Journal of Health Behavior, 30, 278–
289. http://doi.org/10.5993/AJHB.30.3.6
Bock, B. C., Marcus, B. H., Pinto, B. M., & Forsyth, L. H. (2001). Maintenance of PA Following
an Individualized Motivationally Tailored Intervention. Ann Behav Med, 23(2), 79–87.
http://doi.org/10.1207/S15324796ABM2302_2
Bopp, M., & Fallon, E. (2008). Community-based interventions to promote increased PA: a
primer.\n. Applied Health Economics and Health Policy , 6(4), 173–87. Retrieved from
http://adisonline.com/healtheconomics/pages/articleviewer.aspx?year=2008&issue=06040&
article=00001&type=abstract
Brand, T., Pischke, C. R., Steenbock, B., Schoenbach, J., Poettgen, S., Samkange-Zeeb, F., &
Zeeb, H. (2014). What works in community-based interventions promoting PA and healthy
Brown, H. E., Atkin, A. J., Panter, J., Wong, G., Chinapaw, M. J. M., & van Sluijs, E. M. F.
(2016). Family-based interventions to increase PA in children: A systematic review,
meta-analysis and realist synthesis. Obesity Reviews, 17(4), 345–360.
http://doi.org/10.1111/obr.12362
Buchan, D. S., Ollis, S., Thomas, N. E., & Baker, J. S. (2012). PA behaviour: An overview of
current and emergent theoretical practices. Journal of Obesity, 2012.
http://doi.org/10.1155/2012/546459
Brodersen, N. H., Steptoe, A., Boniface, D. R., & Wardle, J. (2007). Trends in PA and sedentary
behaviour in adolescence: ethnic and socioeconomic differences. British Journal of Sports
Medicine, 41(3), 140–4. http://doi.org/10.1136/bjsm.2006.031138
Bryan, S. N., Tremblay, M. S., Pérez, C. E., Ardern, C. I., & Katzmarzyk, P. T. (2006). PA and
ethnicity: evidence from the Canadian Community Health Survey. Canadian Journal of
Public Health. Revue Canadienne de Sante Publique, 97, 271–276.
Canadian Fitness & Lifestyle Research Institute. (2010). Kids CAN PLAY ! 2009. Public
Health, 1–3.
Chaput, J. P., Lambert, M., M, M. E., Tremblay, M. S., O’Loughlin, J., & Tremblay, A. (2012).
PA vs. sedentary time: Independent associations with adiposity in children. Pediatric
Obesity, 7 (3), 251–258. http://doi.org/10.1111/j.2047-6310.2011.00028.x
Christiansen, L. B., Toftager, M., Ersbøll, A. K., & Troelsen, J. (2014). Effects of a Danish
multicomponent PA intervention on active school transport. Journal of Transport & Health,
1(3), 174–181. http://doi.org/10.1016/j.jth.2014.05.002
Colley, R. C., Garriguet, D., Janssen, I., Craig, C. L., Clarke, J., & Tremblay, M. S. (2011). PA
of Canadian children and youth : Accelerometer results from 2007-2009 Canadian Health
Measures Survey. Statistics Canada Catalogue No. 82-003-XPE Health Reports, 22(82),
Craig, P., Cooper, C., Gunnell, D., Haw, S., Lawson, K., Macintyre, S., … Thompson, S. (2012).
Using natural experiments to evaluate population health interventions: new Medical
Research Council guidance. Journal of Epidemiology and Community Health, 66(12),
1182–6. http://doi.org/10.1136/jech-2011-200375
Davison, K. K., Edmunds, L. S., Wyker, B. A., Young, L. M., Sarfoh, V. S., & Sekhobo, J. P.
(2011). Feasibility of increasing childhood outdoor play and decreasing television viewing
through a family-based intervention in WIC, New York State, 2007-2008. Preventing
Chronic Disease, 8(3), A54. Comparative Study, Journal Article, Research Support, U.S.
Gov’t, Non-P.H.S.
Davison, K. K., & Lawson, C. T. (2006). Do attributes in the physical environment influence
children’s PA? A review of the literature. International Journal of Behavioral Nutrition and
PA, 3(19). http://doi.org/10.1186/1479-Received
Ding, D., Sallis, J. F., Kerr, J., Lee, S., & Rosenberg, D. E. (2011). Neighborhood environment
and PA among youth: A review. American Journal of Preventive Medicine, 41(4), 442–455.
http://doi.org/10.1016/j.amepre.2011.06.036
Duncan, S. C., Duncan, T. E., & Strycker, L. a. (2005). Sources and types of social support in
youth PA. Health Psychology : Official Journal of the Division of Health Psychology,
American Psychological Association, 24(1), 3–10. http://doi.org/10.1037/0278-6133.24.1.3
Eather, N., Morgan, P. J., & Lubans, D. R. (2011). Improving health-related fitness in children:
the fit-4-Fun randomized controlled trial study protocol. BMC Public Health, 11(1), 902.
Journal Article, Randomized Controlled Trial, Research Support, Non-U.S. Gov’t.
http://doi.org/10.1186/1471-2458-11-902
Estabrooks, P. a, Lee, R. E., & Gyurcsik, N. C. (2003). Resources for PA participation: does
availability and accessibility differ by neighborhood socioeconomic status? Annals of
Behavioral Medicine : A Publication of the Society of Behavioral Medicine, 25, 100–104.
Fu, Y., Gao, Z., Hannon, J. C., Burns, R. D., & Brusseau, T. a. (2015). Effect of the SPARK
Program on PA, Cardiorespiratory Endurance, and Motivation in Middle-School Students.
Journal of PA & Health, (November), 534–542. http://doi.org/10.1123/jpah.2015-0351
Giles-Corti, B., & Donovan, R. J. (2002). The relative influence of individual, social and
physical environment determinants of PA. Social Science & Medicine, 54, 1793–1812.
http://doi.org/10.1016/S0277-9536(01)00150-2
Glasgow, R. E., Lichtenstein, E., & Marcus, A. C. (2003). Why don ’ t we see more translation of health promotion research to practice ? R ..., 93(8), 1261–1267.
http://doi.org/10.2105/AJPH.93.8.1261
Gordon-Larsen, P., McMurray, R., & Popkin, B. (1999). Adolescent PA and inactivity vary by
ethnicity: The National Longitudinal Study of Adolescent Health. The Journal of
Pediatrics, 135(3), 301–306. http://doi.org/10.1016/S0022-3476(99)70124-1
Gordon-Larsen, P., Nelson, M. C., Page, P., & Popkin, B. M. (2006). Inequality in the built
environment underlies key health disparities in PA and obesity. Pediatrics, 117(2), 417–
424. http://doi.org/10.1542/peds.2005-0058
Kalra, G., De Sousa, A., Sonavane, S., & Shah, N. (2012). Psychological issues in pediatric
obesity. Industrial Psychiatry Journal, 21(1), 11. doi:10.4103/0972-6748.110941
Kropski, J. A., Keckley, P. H., & Jensen, G. L. (2008). School-based obesity prevention
programs: an evidence-based review. Obesity (Silver Spring, Md.), 16(5), 1009–1018.
Journal Article, Review. http://doi.org/10.1038/oby.2008.29
Halfon, N., Larson, K., & Slusser, W. (2013). Associations between obesity and comorbid
mental health, developmental, and physical health conditions in a nationally representative
sample of us children aged 10 to 17. Academic Pediatrics, 13(1), 6–13.
Hawe, P., & Potvin, L. (2009). What is population health intervention research? Canadian
Journal of Public Health Revue Canadienne de Santé Publique, 100(1), Suppl I8-14.
http://doi.org/http://dx.doi.org/10.17269/cjph.100.1748
Hill, J. O., Wyatt, H. R., & Peters, J. C. (2012). Energy balance and obesity. Circulation, 126(1),
126–32. http://doi.org/10.1161/CIRCULATIONAHA.111.087213
Huhman, M. E., Potter, L. D., Duke, J. C., Judkins, D. R., Heitzler, C. D., & Wong, F. L. (2007).
Evaluation of a national PA intervention for children - VERB (TM) campaign, 2002-2004.
AMERICAN JOURNAL OF PREVENTIVE MEDICINE, 32(1), 38–43. article.
http://doi.org/10.1016/j.amepre.2006.08.030
Jansen, P. W., Mensah, F. K., Clifford, S. A., Tiemeier, H., Nicholson, J. M., & Wake, M.
(2013). Development of mental health problems and overweight between ages 4 and 11
years: A population-based longitudinal study of Australian children. Academic Pediatrics,
13(2), 159–167. http://doi.org/10.1016/j.acap.2012.12.001
Janssen, I., & Leblanc, A. G. (2010). Systematic review of the health benefits of PA and fitness
in school-aged children and youth. The International Journal of Behavioral Nutrition and
PA, 7, 40. http://doi.org/10.1186/1479-5868-7-40
Janssen, I., Katzmarzyk, P. T., Boyce, W. F., Vereecken, C., Mulvihill, C., Roberts, C., Currie,
C., Pickett, W.(2005). Comparison of overweight and obesity prevalence in school-aged
youth from 34 countries and their relationships with PA and dietary patterns. Obesity
Reviews, 6(13), 123–132. http://doi.org/10.1111/j.1467-789X.2005.00176.x
Mitchell, C. A., Clark, A. F., & Gilliland, J. A. (2016). Built environment influences of childrens
physical activity: Examining differences by neighbourhood size and sex. International
Journal of Environmental Research and Public Health, 13(1). article. Retrieved from
Must, A., & Strauss, R. S. (1999). Risks and consequences of childhood and adolescent obesity.
International Journal of Obesity and Related Metabolic Disorders, 23, S2–S11.
http://doi.org/10.1038/sj/ijo/0800852
Norman, G., Nutter, S., Ryan, S., Sallis, J. F., Calfas, K. J., & Patrick, K. (2006). Community
Design and Access to Recreational Facilities as Correlates of Adolescent PA and
Body-Mass Index. Journal of PA and Health, 3(Suppl 1), S118–S128.
Owen, N., Glanz, K., Sallis, J. F., & Kelder, S. H. (2006). Evidence-based approaches to
dissemination and diffusion of PA interventions. American Journal of Preventive Medicine,
31(4 Suppl), S35-44. Journal Article, Research Support, Non-U.S. Gov’t, Review.
http://doi.org/10.1016/j.amepre.2006.06.008
ParticipACTION. Are Canadian kids too tired to move? (2016). The 2016 ParticipACTION
Report Card on PA for Children and Youth. Toronto: ParticipACTION; 2016.
Pate, R. R., Trost, S. G., Mullis, R., Sallis, J. F., Wechsler, H., & Brown, D. R. (2000).
Community interventions to promote proper nutrition and PA among youth. PREVENTIVE
MEDICINE, 31(2, 2, S), S138–S149. article. http://doi.org/10.1006/pmed.2000.0632
Perry, C. K., Garside, H., Morones, S., & Hayman, L. L. (2012). PA interventions for
adolescents: An ecological perspective. Journal of Primary Prevention, 33, 111–135.
http://doi.org/10.1007/s10935-012-0270-3
Petticrew, M., Cummins, S., Ferrell, C., Findlay, A., Higgins, C., Hoy, C., … Sparks, L. (2005).
Natural experiments: An underused tool for public health? Public Health, 119(9), 751–757.
http://doi.org/10.1016/j.puhe.2004.11.008
Piko, B. F., & Keresztes, N. (2006). PA, psychosocial health, and life goals among youth.
Journal of Community Health, 31(2), 136–145. http://doi.org/10.1007/s10900-005-9004-2
American Journal of Preventive Medicine, 33(4 SUPPL.).
http://doi.org/10.1016/j.amepre.2007.07.002
Puder, J. J., & Munsch, S. (2010). Psychological correlates of childhood obesity. International
Journal of Obesity, 34(S2), S37-S43. doi:10.1038/ijo.2010.238
Pulgarón, E. R. (2013). Childhood Obesity: A Review of Increased Risk for Physical and
Psychological Comorbidities. Clinical Therapeutics, 35(1), A18–A32.
http://doi.org/10.1016/j.clinthera.2012.12.014
Quigg, R. ., Reeder, A. I. ., Gray, A. ., Holt, A. ., & Waters, D. . (2012). The effectiveness of a
community playground intervention. Journal of Urban Health, 89(1), 171–184. article.
http://doi.org/10.1007/s11524-011-9622-1
Reilly, J. J., & Kelly, J. (2011;2010;). Long-term impact of overweight and obesity in childhood
and adolescence on morbidity and premature mortality in adulthood: Systematic review.
International Journal of Obesity, 35(7), 891-898. doi:10.1038/ijo.2010.222
Roberts, K. C., Shields, M., de Groh, M., Aziz, A., & Gilbert, J. A. (2012). Overweight and
obesity in children and adolescents: results from the 2009 to 2011 Canadian Health
Measures Survey. Health Reports / Statistics Canada, Canadian Centre for Health
Information, 23(3), 37–41. http://doi.org/82-003-XPE
Roemmich, J. N., Epstein, L. H., Raja, S., Yin, L., Robinson, J., & Winiewicz, D. (2006).
Association of access to parks and recreational facilities with the PA of young children.
Preventive Medicine, 43(6), 437–441. http://doi.org/10.1016/j.ypmed.2006.07.007
Sallis, J. F., Owen, N., & Fisher, E. B. (2008). Ecological models of health behavior. Health
Behavior and Health Education: Theory, Research, and Practice, 4th edition.
http://doi.org/10.7326/0003-4819-116-4-350_1
Sallis, J. F., Cervero, R. B., Ascher, W., Henderson, K. a, Kraft, M. K., & Kerr, J. (2006). An
Sallis, J. F., Prochaska, J. J., & Taylor, W. C. (2000). A review of correlates of PA of children
and adolescents. Medicine & Science in Sports & Exercise, 32(1), 963–975. Comparative
Study, Journal Article, Review. http://doi.org/10.1097/00005768-200005000-00014
Sallis, J. F., McKenzie, T. L., Alcaraz, J. E., Kolody, F., & Hovell, M. F. (1997). The effects of a
2-year physical education program ( SPARK ) on ... American Journal of Public Health,
87(8).
Salvy, S., Roemmich, J., Bowker, J., Romero, N. D., Stadler, P. J., & Epstein, L. H. (2009). Effet
of peer and friends on youth PA and motivation to be physically active. Journal of Pediatric
Psychology, 34(2), 217–225. http://doi.org/10.1093/jpepsy/jsn071
Schwimmer, J. B., Burwinkle, T. M., & Varni, J. W. (2003). Health-Related Quality of Life of
Severely Obese Children and Adolescents. JAMA: The Journal of the American Medical
Association, 289(14), 1813–1819.
Shaibi, G. Q., Faulkner, M. S., Weigensberg, M. J., Fritschi, C., & Goran, M. I. (2008).
Cardiorespiratory fitness and PA in youth with type 2 diabetes. Pediatric Diabetes, 9(7),
460–463. http://doi.org/10.1111/j.1399-5448.2008.00407.x
Singh, G. K., Siahpush, M., & Kogan, M. D. (2010). Rising Social Inequalities in US Childhood
Obesity, 2003-2007. Annals of Epidemiology, 20(1), 40–52.
http://doi.org/10.1016/j.annepidem.2009.09.008
Singh, G. K., Yu, S. M., Siahpush, M., & Kogan, M. D. (2008). High levels of physical inactivity
and sedentary behaviors among US immigrant children and adolescents. Archives of
Pediatrics & Adolescent Medicine, 162(8), 756–763.
http://doi.org/10.1001/archpedi.162.8.756
Statistics Canada (2015). Body mass index of children and youth, 2012 to 2013. Retrieved from
Released October 24, 2012. Retrieved from http://www12.statcan.gc.ca/census-recensement/2011/dp-pd/prof/index.cfm?Lang=E
Telama, R., Yang, X., Viikari, J., Välimäki, I., Wanne, O., & Raitakari, O. (2005). PA from
childhood to adulthood: A 21-year tracking study. American Journal of Preventive
Medicine, 28(3), 267–273. http://doi.org/10.1016/j.amepre.2004.12.003
Toftager, M., Christiansen, L. B., Kristensen, P. L., & Troelsen, J. (2011). SPACE for PA - a
multicomponent intervention study: study design and baseline findings from a cluster
randomized controlled trial. BMC PUBLIC HEALTH, 11. article.
http://doi.org/10.1186/1471-2458-11-777
Trost, S., & Loprinzi, P. (2011). Parental influences on PA behavior in children and adolescents:
A brief review. American Journal of Lifestyle Medicine, 5(2), 171–181.
http://doi.org/10.1177/1559827610387236.
Trost, S. G., Pate, R. R., Sallis, J. F., Freedson, P. S., Taylor, W. C., Dowda, M., & Sirard, J.
(2002). Age and gender differences in objectively measured PA in youth. Medicine and
Science in Sports and Exercise, 34(2), 350–355.
http://doi.org/10.1097/00005768-200202000-00025
Tucker, P., Irwin, J. D., Gilliland, J., He, M., Larsen, K., & Hess, P. (2009). Environmental
influences on PA levels in youth. Health & Place, 15, 357–363.
http://doi.org/10.1016/j.healthplace.2008.07.001
Trudeau, François; Shephard, R. J. (2009). Relationships of PA to Brain Health and the
Academic Performance of Schoolchildren. American Journal of Lifestyle Medicine, x, 1–13.
http://doi.org/10.1177/1559827609351133.
Wardle, J., & Cooke, L. (2005). The impact of obesity on psychological well-being. Best
Practice & Research. Clinical Endocrinology & Metabolism, 19(3), 421–440.
Welk, G. J., Wood, K., & Morss, G. (2003). Parental Influences on PA in Children: An
Exploration of Potential Mechanisms. Pediatric Exercise Science, 15, 19–33.
van Sluijs, E. M. F., Kriemler, S., & McMinn, A. M. (2011). The effect of community and
family interventions on young people’s PA levels: a review of reviews and updated
systematic review. British Journal of Sports Medicine, 45(11), 914–22.
http://doi.org/10.1136/bjsports-2011-090187
van Sluijs, E. M. F., McMinn, A. M., & Griffin, S. J. (2007). Effectiveness of interventions to
promote PA in children and adolescents: systematic review of controlled trials. Bmj.,
335(7622), 703. http://doi.org/10.1136/bmj.39320.843947.BE
Verstraete, S. J. M., Cardon, G. M., De Clercq, D. L. R., & De Bourdeaudhuij, I. M. M. (2007).
A comprehensive PA promotion programme at elementary school: the effects on PA
physical fitness and psychosocial correlates of PA. PUBLIC HEALTH NUTRITION, 10(5),
Using Natural Experiments to Evaluate
Population-level PA Interventions with Children: A
Systematic Review
Introduction
Engaging in regular PA during childhood is associated with numerous health benefits and
protects against risk factors associated with obesity (Janssen & LeBlanc, 2010; Shaibi et al.,
2008). According to Canadian recommendations (Janssen & LeBlanc, 2010; Tremblay et al.,
2010), to obtain the health benefits associated with PA, children should have at least 60 minutes
of moderate to vigorous activity (MVPA) every day. Unfortunately, only 9% of Canadian
children (age 5-17) meet Canada’s recommended guidelines of 60 minutes of MVPA on most
days of the week (Shields, 2006; Tremblay et al., 2010; ParticipACTION, 2016).
The decline in children’s PA has generated considerable interest in assessing and
promoting PA among children, as obesity rates have almost tripled among Canadian children in
the last three decades (Colley et al., 2011; Chaput et al., 2012; Janssen et al., 2005). Reasons for
the decline in children’s PA is complex, as this behaviour is influenced by a range of factors at
multiple levels of influence from intrapersonal and interpersonal, to community and policy
(Bauman et al., 2012; Sallis et al., 2000; Van Der Horst et al., 2007). A number of
socio-demographic factors such as age, sex, ethnicity, socio-economic status (SES), and immigrant
status have been identified as underlying determinants of PA in children (Brodersen et al., 2007;
Bryan et al., 2006; Colley et al., 2011; Sallis et al., 2000; Singh et al., 2008). Children’s
interpersonal networks have also been found to influence PA behaviour, as several studies
suggest that social support from parents and peers positively influence PA in children (Beets et
al., 2006; Duncan et al., 2005; Trost & Loprinzi, 2011; Welk, Wood, & Morss, 2003). On a
levels of PA. As a number of correlates of PA in children have been identified, it becomes
crucial to assess the effectiveness of interventions aimed at increasing PA.
This paper aims to establish the current state of evidence related to naturally-occurring
population-based PA interventions with children by conducting a systematic review. This study
addresses the following objectives: 1) to summarize and evaluate previous literature by exploring
the methods and measures that have been used in evaluations, 2) to examine the associated PA
outcomes, and 3) to identify factors that influence the success of PA interventions. The
information generated in this review will inform researchers and policy-makers about relevant
evidence-based strategies to modify PA at a population-level.
2.1.1. Measuring Physical Activity
Due to the unique nature of children’s PA, there are a variety of different measures that
have been used to assess PA in children, with each measure possessing distinct advantages and
disadvantages (Trost, 2007; Warren et al., 2010). Measures used to assess PA can be
characterized as either objective measures (i.e., heart-rate monitor, accelerometers, pedometers)
or subjective measures (i.e., self-report, direct observation). In recent years, the use of
accelerometers has increased dramatically, as it is an attractive device due to its small size,
modest cost and is a viable measure to use with children and adolescents (Sylvia et al., 2015;
Trost, 2007). Accelerometers provide an objective measure of PA by assessing the body during
movement by capturing the frequency, duration and intensity of movement (Strath et al., 2013;
Trost, 2007). In terms of subjective measures, self-reports continue to be the most widely used
due to the ease of administration, low cost, and convenience for large sample sizes (Trost, 2007).
Determining the most appropriate measure to quantify PA in children presents a number of
challenges for researchers, as there is usually a trade off between the accuracy and practicality of
a measure (Welk et al., 2000). Understanding this trade off is particularly important for
developing and testing PA interventions.
2.1.2. Community-Based Interventions
Interventions are often used to test different theories, strategies and methods in hopes of
achieving positive PA outcomes. Over the last 20 years there has been a dramatic increase in the
number of PA interventions on children (van Sluijs et al., 2016). Despite the large scope of
research, reviews on the effectiveness of PA interventions have demonstrated limited efficacy for
changing children’s overall PA levels ( Kahn et al., 2002; Metcalf et al., 2012; van Sluijs et al.,
2007). Community-based PA interventions are suggested to be the most effective approach with
the greatest potential to achieve population-level change in children’s PA levels (Pate et al.,
2000; Sallis et al., 2008). Considering the amount of time children spend outside of school, the
community setting can promote leisure time PA by increasing opportunities for PA within the
community (Brand et al., 2014; van Sluijs et al., 2011; Perry et al., 2012). A number of
community-based interventions involve cross-sector collaborations with community groups,
academic institutions, organizations, recreation facilities, schools and policy-makers (Pate et al.,
2000; Sallis et al., 2008). This collaborative approach towards developing and implementing
community-based interventions also allow for greater reach of target groups, pooled resources,
and a more secure foundation for long-term sustainability (Bopp & Fallon 2008).
2.1.3. Natural Experiments
Community-based PA interventions have the potential to achieve population-level
independently. To overcome this issue, researchers can evaluate already occurring interventions
as a ‘natural experiment,’ where individuals in experimental conditions are determined by nature
or factors outside the control of the researchers (Craig et al., 2012; Petticrew et al., 2005). For
instance, outcomes of interest can be examined between populations newly exposed to policies
or environmental changes with those unexposed (intervention and comparison groups), or
compare changes within the same population before and after a program or policy is initiated
(pre-post observations) (Mayne et al., 2015). To illustrate, Fuller et al. (2013) used a natural
experiment to determine if a bicycle share program increases the likelihood of biking in
Montreal, Quebec based on residential exposure. This approach is often a useful way of
understanding the impact of large-scale interventions on health outcomes that may not be
possible to study as a controlled experiment (Craig et al., 2012). As a result, natural experiments
produce good external validity that other research designs are unable to achieve, as they provide
evidence for the direct impact of an intervention in real-world settings (Craig et al., 2012;
Giles-Corti et al., 2015; Glasgow et al., 2004; Hunter et al., 2014; Petticrew et al., 2005; Ramanathan
et al., 2008). There are inherent limitations that exist with this approach, notably, the many
sources of potential bias such as confounding and threats to causal inference that should be taken
into consideration when measuring study outcomes (Craig et al., 2012).
While it is still a relatively underused tool in PA interventions with children, an
increasing number of studies have utilized a natural experimental approach, particularly in
environmental interventions that target active travel or built environment changes (Benton et al.,
2016; Carlin et al., 2016; Sallis et al., 2006). However, the utility of a natural experimental
approach for evaluating population-level PA interventions is not well understood, as there are no
a need to not only assess PA outcomes, but also gather evidence on the methodologies currently
used to better understand how natural experiments can be effectively used to evaluate
population-based PA intervention with children.
Methods
2.2.1. Eligibility Criteria
A systematic review was conducted to identify articles published since 2000 that examine
naturally-occurring population-level PA interventions with children to determine the current
methods and measures used to evaluate PA, assess PA outcomes, and identify successful and
unsuccessful components of the studies and what external factors influence PA outcomes.
Eligible studies were selected by searching electronic databases (as of March 2016) and
reference lists of relevant articles. Various combinations of several search terms were used in
order to capture relevant articles (i.e., physical activity, play, children, youth, intervention,
natural experiment, evaluation, community, population). Search terms were inputted into four
electronic databases: PubMed, Web of Science, Sport Discus, and Engineering Village
(GEOBASE, Inspec, and Compendex). The selected databases cover a range of fields from social
science, health, engineering, and applied science.
2.2.2. Search Strategy and Selection of Studies
Articles were included if they met the following criteria: published between 2000-2016;
focused on children or adolescents (between 6-18 years); conducted community- or
population-based interventions; the intervention or program was naturally-occurring; PA was the primary
outcome variable (i.e., objective or subjective measure); and articles were written in English. For
the purpose of this review, the terms community- and population-based interventions are
population of children. For example, a community or population for an intervention could be a
single school or neighbourhood, or as large as a city. This allowed for a greater spectrum of
articles that used a natural experimental approach. Similarly, the age range used for inclusion of
articles was broad in order to capture all relevant interventions that targeted school-aged children
that used a natural experimental approach. Interventions were considered to be
naturally-occurring if the article stated that the program or intervention was initiated by an external agency
and it was not under the direct control of the researchers.
Articles were excluded based on the following criteria: focused on pre-school ages,
adults, or a clinical population (i.e., obese children); examined the general population with no
distinct analyses for children, or a subset of population (i.e., only girls); were family-based,
school-based, or primary care interventions; and studies that primarily focused on nutrition.
Some school-based interventions were included if it was clear that PA was taking place outside
of school hours or if schools were used as the method of recruitment and data collection.
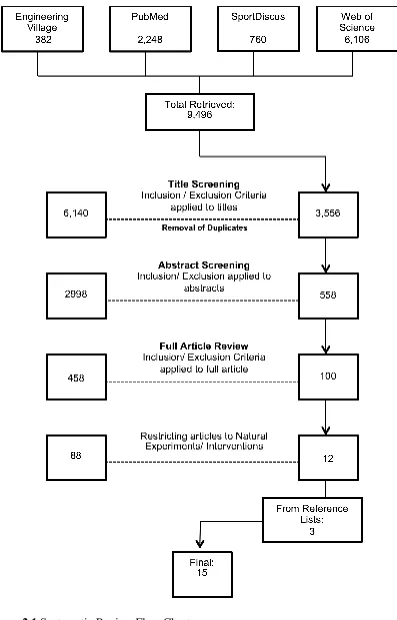
The initial search returned 9,496 articles (see Figure 2.1). The titles of all the articles
were screened and a total of 3,556 potentially relevant articles were identified. The title
screening resulted in 6,140 articles being excluded, of which 510 were duplicates. Abstract
screening resulted in the exclusion of 2998 articles. Of the remaining 558 articles, the full text
was reviewed and 458 were deemed not to satisfy inclusion criteria. Of the remaining 100
articles, 88 were removed, as they did not meet the definition of a natural experiment. Finally,
reviewing the reference lists of the relevant articles identified an additional 3 articles. A total of
2.2.3. Data Extraction
Data on the study design, study location, total sample size, sample age, year of
publication, PA domain, PA measures, intervention components, evaluation components and
findings were extracted for each article that met the inclusion criteria and tabulated (see
Appendix A at the end of the chapter). Since the purpose of this review is to determine how
naturally-occurring population-based PA interventions have been evaluated, outcomes associated
with PA, physical fitness, or anthropometric measures related to PA (i.e., body composition,
BMI) were reviewed. Additional outcomes related to evaluation components and external factors
were also reviewed.
Evidence Synthesis
2.3.1. General Characteristics of the Reviewed Studies
A total of 15 papers were reviewed. A majority of the studies were conducted in the
United States (11/15), while Australia, New Zealand, United Kingdom and Canada had one
study each. Sample sizes ranged from 55 to 7455. Nine of the studies were conducted with
children (ages 6-12 years), five studies included both children and adolescents, and only one
study targeted only adolescents (ages 13-18 years). Among the reviewed studies, duration of the
study period varied from 5 weeks to 3 years. Only five of the studies reported the use of a
theoretical framework or approach for the intervention that included social cognitive theory,
social ecological framework, social marketing principles and an infrastructure/capacity building
approach. In terms of the types of PA examined, five studies focused on active travel, five
studies targeted built environment, three studies conducted interventions aimed at general PA,
Active travel interventions typically focused on promoting walking or biking to and from
school either through walking school bus programs or safe routes to school programs. Of the
built environment studies, three involved park renovations and two included more
comprehensive changes throughout the community such as the creation of sidewalks, crosswalks,
walking trails, and bike racks. All three studies targeting general PA were part of the same
intervention (VERB), a mass media campaign based on social marketing principles that
promoted PA as cool, fun, and easy. One of these studies adapted VERB into a summer program
and partnered with community-based organizations to offer PA opportunities. The two studies
that used after-school settings both involved adapting programing to include a new PA
component in local community organizations; one study partnered with the YMCA, and the other
study included the YMCA and Boys and Girls Club in delivering the intervention.
PA was generally measured using subjective measures as eight of the studies used only
subjective measures and seven studies used a combination of subjective and objective measures.
Eleven studies included an additional evaluation component in tandem with evaluating the
Table 2.1 General characteristics of the papers reviewed.
General Characteristics of the Papers Reviewed
Characteristics of Paper Number of Articles
Study Design
Quasi-experimental
Repeated cross-sectional (control group) 6 Longitudinal (control group) 4 Longitudinal (no control group)a 1
Cross-sectional (control group) 1 Non-experimental
Longitudinal (no control group) 2 Repeated cross-sectional (no control group) 1
Total Sample Size
1-100 3
101-500 6
500+ 6
Geographic Origin
Australia 1
Canada 1
New Zealand 1
UK 1
United States 11
Theory or Framework Used
Social cognitive theory 2 Social ecological framework 1 Alternative approaches 2
Not reported 10
Age Group
Children (6-12) 10
Adolescent (13-18) 1
Both 5
PA Domain
Active travel 5
After school 2
Built environment 5
General PA 3
PA Measures
Objective 1
Subjective 9
Both 5
Evaluation Measures
PA only 4
Other evaluation component 11
Note: a One study created control group based on participants exposure level to the
2.3.2. Types of Methods and Measures Used
The studies identified in the literature search used several types of research designs. Of
the 15 studies, the most frequently used was a quasi-experimental research design with pre/post
measures (12/15). Of these 12, a majority of the studies included a control group for except one
study that used a statistical technique to create a control group based on participant’s exposure to
the intervention (Huhman et al. 2005). Three of the studies used a non-experimental research
design that included pre/post measures (but no control group). Eight of the studies used a
cross-sectional study design where different individuals were assessed at pre/post measurement
periods, and the other seven studies used longitudinal study design to assess the same individuals
at pre/post measurement periods.
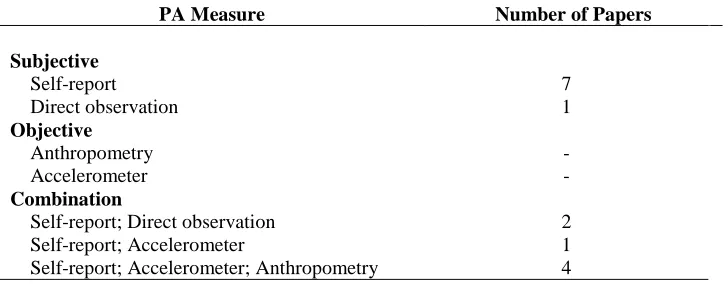
Common among population-based PA interventions, almost half of the studies used only
self-report measures to obtain PA outcomes (7/15) (see Table 2.2). Self-reports included child
surveys such as the national Youth Risk Behaviour Survey (YRSB) and the Youth Media
Campaign Longitudinal Survey (YMCLS). The YRBS is a biennial survey conducted by the
Center for Disease Control and Prevention (CDC) to monitor priority health risk behaviours of
adolescents nationwide (CDC, 2016), whereas the YMCLS is an interviewer-administered
telephone survey designed to evaluate the effects of the CDC VERB campaign. Both measures
have been found to have acceptable reliability (Brener et al., 2004; Welk et al., 2007). Other
studies that used self-report measures developed intervention specific questionnaires or used
classroom tallies. Five of the studies used accelerometers in combination with self-report
measures, four of which also included anthropometric measures. The only anthropometric
Less frequently used was direct observation, as only three studies used this measure, two
of which used direct observation in combination with self-report. The direct observation
measures included System for Observing Fitness Instruction Time (SOFIT) and System for
Observing Play and Recreation (SOPARC). SOFIT is used to measure participants PA levels and
lesson context, whereas SOPARC is used to measure park user characteristics and PA behavior.
Table 2.2 Measurement characteristics of the reviewed papers
PA Measure Number of Papers
Subjective
Self-report 7
Direct observation 1
Objective
Anthropometry -
Accelerometer -
Combination
Self-report; Direct observation 2 Self-report; Accelerometer 1 Self-report; Accelerometer; Anthropometry 4
2.3.3. Physical Activity Outcomes
Given the range of measures used, outcome measures for PA were highly varied between
the studies and included MVPA, total daily PA, self-report of PA, direct observation of PA,
proportion of students who walked to school, and change in BMI. Overall, the studies showed
positive changes in PA outcomes. Based on the type of PA, the majority of positive outcomes
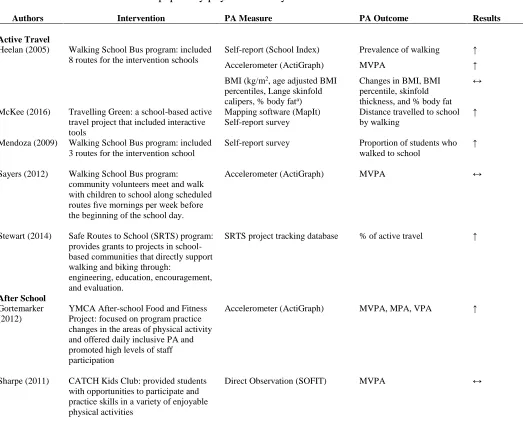
Table 2.3 Results of the reviewed papers by physical activity domain
Authors Intervention PA Measure PA Outcome Results
Active Travel
Heelan (2005) Walking School Bus program: included 8 routes for the intervention schools
Self-report (School Index)
Accelerometer (ActiGraph)
BMI (kg/m2, age adjusted BMI
percentiles, Lange skinfold calipers, % body fata)
Prevalence of walking
MVPA
Changes in BMI, BMI percentile, skinfold thickness, and % body fat
↑ ↑ ↔
McKee (2016) Travelling Green: a school-based active travel project that included interactive tools
Mapping software (MapIt) Self-report survey
Distance travelled to school by walking
↑
Mendoza (2009) Walking School Bus program: included 3 routes for the intervention school
Self-report survey Proportion of students who
walked to school
↑
Sayers (2012) Walking School Bus program:
community volunteers meet and walk with children to school along scheduled routes fıve mornings per week before the beginning of the school day.
Accelerometer (ActiGraph) MVPA ↔
Stewart (2014) Safe Routes to School (SRTS) program: provides grants to projects in school-based communities that directly support walking and biking through:
engineering, education, encouragement, and evaluation.
SRTS project tracking database % of active travel ↑
After School
Gortemarker (2012)
YMCA After-school Food and Fitness Project: focused on program practice changes in the areas of physical activity and offered daily inclusive PA and promoted high levels of staff participation
Accelerometer (ActiGraph) MVPA, MPA, VPA ↑
Sharpe (2011) CATCH Kids Club: provided students
with opportunities to participate and practice skills in a variety of enjoyable physical activities