R E V I E W
Physical activity programs for older people in the
community receiving home care services:
systematic review and meta-analysis
This article was published in the following Dove Press journal: Clinical Interventions in Aging
Elissa Burton1
Kaela Farrier1
Rose Galvin2
Shanthi Johnson3
N Frances Horgan4
Austin Warters5
Keith D Hill1
1School of Physiotherapy and Exercise Science, Curtin University, Perth, Western Australia, Australia;2School of Allied Health, Faculty of Education and Health Sciences, Health Research Institute, University of Limerick, Limerick, Ireland;3School of Public Health, University of Alberta, Edmonton, AB, Canada;4School of Physiotherapy, Royal College of Surgeons in Ireland, Dublin, Ireland;5Health Service Executive, Dublin North City and County Healthcare Organisation, Dublin, Ireland
Abstract:The proportion of older adults is increasing around the world and most wish to live in their home until they die. To achieve this, many will require services in the home to remain living independently. To maintain function (ie, strength, balance, and endurance), physical activity needs to be undertaken on a regular basis, and is essential as a person ages. Unfortunately, as people age there is a tendency to reduce activity levels, which often leads to loss of function and frailty, and the need for home care services. This updated systematic review includes a mix of study methodologies and meta-analysis, and investigated the effectiveness of physical activity/exercise interventions for older adults receiving home care services. Eighteen studies including ten randomized controlled trials meeting the
selec-tion criteria were identified. Many of the studies were multi-factorial interventions with the
majority reporting aims beyond solely trying to improve the physical function of home care clients. The meta-analysis showed limited evidence for effectiveness of physical activity for older adults receiving home care services. Future exercise/physical activity studies working with home care populations should consider focusing solely on physical improvements, and need to include a process evaluation of the intervention to gain a better understanding of the
association between adherence to the exercise program and other factors influencing
effectiveness.
Keywords:exercise, physical function, community care, reablement, seniors
Introduction
Populations throughout the world are increasing in age, with greater proportions of
older people than previously observed.1Most older people have a desire to live in
their home until they die2and to do this, they need to be able to complete activities
of daily living (ADLs) such as showering, dressing, eating, and toileting
indepen-dently. For some older adults these tasks become increasingly difficult due to health
issues, frailty or disability, and they require assistance to continue living in their
home.3This assistance is often provided by home or community care services and
is predominantly funded by the government in high income countries such as
Australia, Canada, and a number of European countries.4–6
Home care services can be delivered over the short or longer term.7Some
short-term reablement services (ie, goal-oriented, person-centered, often aimed at reduced long-term services) include physical activity or exercise programs, whereas the longer term services such as personal care (ie, showering), domestic assistance (ie, cleaning), gardening, transport, and social support usually do not. In order to assist
Correspondence: Elissa Burton School of Physiotherapy and Exercise Science, Curtin University, GPO Box U1987, Perth, Western Australia 6845, Australia
Tel +6 189 266 4926 Fax +6 189 266 3699 Email [email protected]
Clinical Interventions in Aging
Dove
press
open access to scientific and medical research
Open Access Full Text Article
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
an older person to continue living in their home and complete their ADLs, they need to maintain strength,
balance, and endurance.8,9
Improving or maintaining strength, balance, and endur-ance requires a desire to be active, the knowledge of what
to do, and the opportunity to be active.10,11 The World
Health Organization and many individual countries (ie, United States, Canada, Great Britain, Australia) have pro-duced National Physical Activity Guidelines for older
adults.12–15 They predominantly recommend 30
minutes of moderate intensity endurance physical activity every day such as walking or swimming, in addition to
strength and balance training twice a week.12–15 The
strength and balance components are essential for
main-taining independence and completing ADLs.16 Strength
and balance training also leads to many health benefits
such as increased strength and bone density, reduction in
sarcopenia, frailty, and chronic illness9,16–18 and has the
strongest evidence for preventing falls for older adults
living in the community.19 Unfortunately, these exercise
modalities are often overlooked when promoting physical activity recommendations to older adults, particularly
those receiving home care services.20
Many older home care clients walk to be active,
how-ever few participate in strength and balance programs.21It
can be difficult for home care clients to leave their home,
and typically, shopping and medical appointments are prioritized, particularly when assistance with transport is required. To support older adults receiving home care services to, at a minimum, maintain their strength and balance, and at best, improve it over time, promoting
physical activity within the home is required.
Organizations delivering home care services have the ideal opportunity to do this, as many home care workers deliver services from once a week to multiple times each
week. A previous systematic review22evaluated the
effec-tiveness of physical activity (exercise) programs for home care clients, however, at the time only eight articles were
identified. The evidence (ie, outcomes and assessments)
varied widely and was limited, as such, a meta-analysis could not be undertaken. Therefore, as the focus on older adults receiving home care services continues to increase, it is essential to identify whether further studies have been undertaken. This will help guide home and community care organizations to provide evidence-based care for their older clients and assist policy-makers to understand
the benefits of improved physical function for this older
population whom they heavily fund (eg, Irish government
spends €408 million on home support each year which
equates to 17 million visits).6 This current systematic
review looks at the recent evidence and where possible combines the randomized controlled trials (RCTs) (n=2) from the previous systematic review with more recently published studies, to determine the effectiveness of
physi-cal activity/exercise programs delivered specifically to
older adults receiving home care services.
Material and methods
Eligibility criteria
The review is limited to studies that met the following eligibility criteria:
● population: aged 65 years and older (at least 50% of
sample) and receiving home care services during the intervention. Home care services may include (but not limited to) personal care (showering), domestic assistance, transport, shopping or social care. These services are delivered in an older persons home by home or community care organizations (ie, munici-palities etc) and can be short-term or long-term ongoing services.
● Intervention: has to have a physical activity or
exer-cise aspect to the intervention.
● Comparison: for RCTs the comparison group will be
usual care (ie, which may include a current physical activity or exercise program used) or a non-active control group.
● Outcomes: the physical activity or exercise
interven-tion has to have been assessed using at least one physical performance outcome (ie, mobility, endur-ance, strength, balance).
● Setting: community-dwelling people only.
Any quantitative study could be included, eg, pilot or feasibility, pre- and post-test, retrospective, controlled trials or RCTs. Only peer-reviewed journal articles in English were included. No unpublished data (ie, reports), books, conference proceedings, theses, or poster abstracts were included. Exclusion criteria were: those living in residential care, and samples with >50% with a diagnosis of dementia or neurodegenerative disorder because they often require greater supervision and/or carer input to complete the physical activity/exercise intervention and therefore may not be representative of a typical home care service.
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
Information sources
Five databases were searched between October 2012 and August 2018: Medline (Proquest); CINAHL; PubMed; PsycInfo; and SportDiscus. The previous systematic review
search included articles between January 1982 to
September 2012. Reference lists from these papers were also scanned.
Search strategy
The search included the same mix of keywords as used in the previous systematic review. However, this updated
review also included “reablement” as a search term. An
example of the search strategy is presented in Table 1.
Study selection
Study selection was conducted in three stages. Stage one was the initial screening of the titles and scanning the abstracts against the eligibility criteria to identify poten-tial articles (completed by KF). Stage two included screening the full articles by two authors (EB and KF) to identify whether they met the eligibility criteria. In stage three, disagreements were resolved through discus-sion between EB and KF to achieve consensus, after referring to the eligibility criteria and protocol. The PRISMA checklist was used to ensure the results were
reported systematically.23
Data collection process
Each study in the review was evaluated using
a standardized extraction form, which included study design; purpose; intervention; study characteristics includ-ing sample size, sex proportion, participant age,
interven-tion type; and length of follow-up (Tables 2 and3).
Study quality
Study quality for the RCTs was assessed by two
indepen-dent researchers (KF and RG) using the Cochrane’s Risk
of Bias Tool.24 Categories assessed by the tool include
sequence generation, allocation concealment, blinding of participants, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other
sources of bias.24 RCT studies were assessed as having
“low”,“medium”or“high”risk of bias. Discussions were
undertaken between the reviewers and where required, a third researcher (EB), to form consensus.
Study quality was reviewed by two researchers (KF, EB) for all other included papers, using the National Institute for Health and Care Excellence (NICE)
guide-lines appraisal checklist.25The internal and external
valid-ity of the included papers were assessed by addressing key aspects of study design such as participant characteristics, allocation and intervention details, outcomes assessed, and
methods of analyses.25Each study was awarded an overall
study quality grading (ie, ++ all or most of the checklist
criteria have been satisfied, where they have not, it was
deemed unlikely to alter the conclusions; + some of the
checklist criteria have been satisfied, where they have not,
it is unlikely these will alter the conclusions; and–few or
no checklist criteria have been satisfied and are likely or
very likely to alter the conclusions).25
Data analysis
Physical performance outcome measures from the RCTs
included in this current review and the previous review22
were collated to determine whether there were two or
more studies that utilized the same outcome measures.26
For those studies that did, a meta-analysis was undertaken. Authors were contacted if data were not available within the published article. Four performance outcomes were utilized in the meta-analyses and all were measured using continuous data: Timed Up and Go (TUG),
sit-to-stand five times, grip strength, and walking speed. The
mean difference (MD) and 95% CIs were calculated. Review Manager (RevMan) version 5.3 was used to con-duct the analyses and generate forest plots with a random
Table 1Search strategy
1 Community care
2 Community health care
3 Home care
4 Community nursing
5 Home and community care
6 Home support
7 Community rehabilitations
8 Restorative care
9 Reablement
10 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9
11 Physical activity
12 Exercis*
13 11 or 12
14 Ageing
15 Aging
16 Aged
17 Older
18 Elderly
19 14 or 15 or 16 or 17 or 18
20 10 and 13 and 19
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
T able 2 Summar y of included randomized contr olled trial (RCT) studies Refer ence (coun-tr y) study design Study purpose Sample siz e; % female; a g e (y ears) (SD) comparator P opulation Outcomes and measur e-ment; follo w-up Inter v ention effect Bur ton et al, 28 (Australia) Pragmatic randomized con-tr olled trial Determine whether LiFE w ould be undertak en mor e often and result in gr eater functional gains than the current structur ed ex er -cise pr ogram deliv er ed as part of a restorativ e home car e ser vice LiFE =40; 75%; 80.2 years (6.4) Structur ed ex er cise =40; 90%; 79.6 years (6.2) Ye s Living in P erth suburbs (W estern Australia) re ferr ed for a restorativ e home car e ser vice Functional re ach, chair sit-to-stand (1 and 5), TUG, T andem walk, FES, ABC Scale, Vitality Plus Scale, The Late Life Function and Disability instruments 8 w eeks LiFE gr oup signi fi cantly impr ove d in 95% (19 of 20) of outcome measur es, compared with the structur ed ex er cise gr oup , which signi fi cantly impr ov ed in 70% (14 of 20). Bur ton et al, 29 (Australia) Pragmatic randomized con-tr olled trial Examine ov er the longer term, the effectiv eness and maintenance of a (modi fi ed) LiFE compared to the curr ent, structur ed ex er cise pr ogram used in a restorativ e home care ser vice LiFE =40; 75%; 80.2 years (6.4) Structur ed ex er cise =40; 90%; 79.6 years (6.2) Ye s Living in P erth suburbs (W estern Australia) re ferr ed for a restorativ e home car e ser vice Functional re ach, chair sit-to-stand (1 and 5), TUG, T andem walk, FES, ABC Scale, Vitality Plus Scale, The Late Life Function and Disability instruments, 6 month fall histor y 8 w eeks and 6 months A signi fi cant main effect of time was found for all measur es. LiFE show ed signi fi cantly gr eater impr ov ement than the structur ed ex er cise gr oup for tandem walk, ABC score, and Vitality Plus scale Danilovich et al, 30 (USA) Randomized contr olled trial T o test the effects of SFL ex er cise pr ogram on the ph ysical perfor -mance and self-rated health of older adults enr olled in the Community Car e Pr ogram, a Medicaid waiv er pr ogram 42; 83%; 74.8 years Inter vention =24; 83%; 74.1 years Contr ol =18; 83%; 75.6 ye ars Ye s Community-dwelling older adults receiving HC A ser vices thr ough the Community Car e Systems, Inc. in Illinois Grip and quadriceps str ength using a hand-held dynamometer , TUG, 10 ft gait speed, Self-Ef fi cacy for Ex er cise, pain, and PR OMIS-global health 12 w eeks Effect sizes w er e moderate for grip str ength, pain, and PR OMIS-global health. SFL participants sig-ni fi cantly impr ov ed median quad-riceps and TUG (median only) scor es compared to contr ols. No adv erse health ev ents and high pr ogram satisfaction w er e reported. Frailty pr e valence in the contr ol gr oup incr eased wher eas it decr eased in the SFL gr oup . Danilovich et al, 31 (USA) Randomized contr olled trial Determine the feasibility of train-ing HC As to lead the SFL pr o-gram with their Community Car e Pr ogram clients 42; 83%; 74.8 years (8.8) Inter vention =24; 83%; 74.1 years (9.9) Contr ol =18; 83%; 75.6 ye ars (8.1) Ye s Community-dwelling older adults receiving HC A ser vices thr ough the Community Car e Systems, Inc. in Illinois Client and HC A pr ogram satis-faction rates, HC A SFL training e valuation information and SFL fi delity rates 12 w eeks It is feasible for HC As to imple-ment SFL safely with clients. Participants vie w ed SFL as highly satisfactor y and HC As w er e able to adapt SFL for their clients. HC As ha ve high job satisfaction, and leading SFL enhances w ork achie ve ment and pride ( Continued )
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
T able 2 (Continued). Refer ence (coun-tr y) study design Study purpose Sample siz e; % female; a g e (y ears) (SD) comparator P opulation Outcomes and measur e-ment; follo w-up Inter v ention effect King et al, 32 (Ne w Zealand) Cluster ran-domized contr olled trial Evaluate the impact of a restorativ e home car e ser vice, compared with usual care for community-dwelling older people 186; 74%; 79 years Restorative =93; 69.9%; 78.4 years (6.5) Contr ol =93; 77.4%; 80.5 ye ars (6.3) Ye s Older people receiving assistance fr om a home care agency in Ne w Zealand SF-36, Nottingham Extended ADL, TUG, Master y scale , DSSI 4 and 7 months Signi fi cant bene fi t in health-related quality of life (SF-36) at 7 months compared to usual car e, particularly in the mental health component. A signi fi cantly higher number of older people in the inter vention gr oup w er e identi-fi ed for reduced paid care giver support or discharge Parsons et al, 33 (Ne w Zealand) Cluster ran-domized contr olled trial T o determine the impact of a re storative model of home care on social support and ph ysical function among community-dw elling older people Inter vention =108; 71.3%; 79.1 years (6.9) Usual car e =97; 60.8%; 76.9 years (7.6) Ye s Community-dwelling people older than 65 ye ars (55 years if Maori or Paci fi c Islander) w er e eligible if the y w er e ne w referrals to the car e coor dination agency for home care in Ne w Zealand SPPB, DSSI 6 months Inter vention gr oup had a gr eater mean incr ease in ph ysical function ov er time than the usual car e gr oup as determined by ov erall SPPB Renehan et al, 36 (Australia) Randomized con-tr olled trial Determine feasibility and accept-ability of a community-deliv er ed post-hospital falls pr e ve ntion pr o-gram, incorporating ex er cise, medication re vie w , and education 13; 53.8%; 82.2 years (9.7) Inter vention =7; 57.1%; 84.0 years (6.4) Contr ol =6; 50% 75.8 ye ars (11.6) Ye s Recently discharged fr om a hospital within metr opolitan Melbourne, Australia after being admitted for a fall and a ne w or existing client of the community home care organization Quality of life (A QoL-8D), falls, fall risk (FR OP-Com), FES-I, Fried Frailty Criteria, Katz ADL, quali-tative falls inter vie w . Inter vention only: fi ve times sit-to-stand, 4 test balance scale (feet together , semi-tandem, tandem and one leg stand), TUG 6 months The ex er cise component of the multifactorial inter ve ntion was highly valued by inter vention par -ticipants. Five falls during inter -vention period: inter vention gr oup: 3; contr ol gr oup: 2. No signi fi cant changes in ph ysical outcome measur es. Saeterbakk en et al, 37 (Norwa y) Randomized contr olled trial Determine the effects of a 10-w eek home-based str ength train-ing pr ogram on ph ysical function tests, le vel of ph ysical activity , muscle str ength, and RFD among frail old adults receiving home car e ser vices 23; 73.9% Inter vention =11; 86.5 ye ars (6.4) Contr ol =12; 83.5 years (5.7) Ye s Older adults living at home and in need of home care due to func-tional disabilities and/or medication Leg extension and elbow fl exion maximal str ength and RFD , pr e-ferr ed/max walking speed, stair climb, 5x chair rise and ph ysical activity (acceler ometer) 10 w eeks Inter vention gr oup signi fi cantly impr ov ed peak RFD in leg extension ( Continued )
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
T
able
2
(Continued).
Refer
ence
(coun-tr
y)
study
design
Study
purpose
Sample
siz
e;
%
female;
a
g
e
(y
ears)
(SD)
comparator
P
opulation
Outcomes
and
measur
e-ment; follo
w-up
Inter
v
ention
effect
Ste
vens-Lapsley
et
al,
34
(USA)
Randomized
contr
olled
trial
T
o
determine
whether
a
pr
ogre
ssiv
e
multicomponent
ph
ysical
therap
y
inter
vention
in
the
home
setting
can
impr
ove
functional
mobility
for
decondi-tioned
older
adults
following
acute
hospitalization
compared
to
usual
car
e
rehabilitation
22;
63.6%;
85.4
years
(7.8)
Inter
vention
=12;
70%;
83
ye
ars
(6.8)
Usual
car
e
=9;
58.3%;
87
ye
ars
(8.8)
Ye
s
Older
adults
with
multiple
chr
onic
conditions,
who
w
er
e
discharged
fr
om
the
Acute
Car
e
for
the
Elderly
unit
of
the
Univ
ersity
of
Colorado
Hospital,
with
ph
ysician
re
ferrals
for
home
health
ph
ysical
therap
y
4
m
walking
speed,
modi
fi
ed
Ph
ysical
P
erformance
Test,
SPPB,
six
minute
walk
test
30
and
60
da
ys
Inter
vention
gr
oup
had
signi
fi
-cantly
gr
eater
impr
ov
ements
in
walking
speed,
modi
fi
ed
ph
ysical
performance
test,
and
SPPB
scor
es
compared
with
the
usual
car
e
gr
oup
at
60
da
ys
T
untland
et
al,
35
(Norwa
y)
Randomized
contr
olled
trial
In
ve
stigate
the
effectiv
eness
of
reablement
(multicomponent
home-based
re
habilitation)
in
older
adults
compared
with
usual
car
e
in
relation
to
daily
activities,
ph
ysical
functioning,
and
health-related
quality
of
life
Inter
vention
=31;
71%;
79.9
years
(10.4)
Contr
ol
=30;
63.3%;
78.1
ye
ars
(9.8)
Ye
s
P
eople
applying
for
,
or
referr
ed
to
,
home-based
ser
vices
due
to
functional
decline
in
one
or
mor
e
ADL
in
a
rural
municipality
in
Norwa
y
COPM
was
used
to
measur
e
self-per
ceiv
ed
activity
performance
and
satisfaction
with
perfor
-mance.
Health-r
elated
quality
of
life
(COOP/W
onka),
TUG,
grip
str
ength
3
and
9
months
Signi
fi
cant
impr
ov
ements
in
mean
scor
es
fa
voring
reablement
in
COPM
performance
at
3
and
9
months
and
ov
erall
tr
eatment,
and
for
COPM
satisfaction
at
9
months
and
ov
erall
tr
eatment
Abbre
viations:
LiFE,
Lifestyle-integrated
Functional
Ex
er
cise
pr
ogram;
TUG,
Timed
Up
and
Go;
FES,
Falls
self-Ef
fi
cacy
Scale;
ABC
,
Activities
speci
fi
c-Balance
Con
fi
dence
Scale;
SFL,
Str
ong
For
Life;
HC
A,
home
car
e
aide;
ADL,
activities
of
daily
living;
DSSI,
Duk
e
Social
Support
Index;
SPPB,
Short
P
erformance
Ph
ysical
Batter
y;
FR
OP-Com,
Falls
Risk
for
Older
P
eople
–
Community
Setting;
FES-I,
Falls
self-Ef
fi
cacy
Scale
–
International;
RFD
,
Rate
of
Fo
rce
Dev
elopment;
COPM,
Canadian
Occupational
P
erformance
Measur
e.
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
T able 3 Summar y of inter vention implementation for randomized contr olled trial (RCT) studies Refer ence Implementation strateg y Inter ve ntion Bur ton et al, 28 , 29 L iF E an d str uc tu re d ex e rc is e p rog ra m w e re de liv e re d b y ca re ma na ge rs as p art of a res tor at iv e h om e ca re se rvi ce . C lie n ts w e re vis ite d ev ery 10 – 1 4 da ys b y th e ir ca re manager (a verage 3 vi si ts) to offer suppo rt , e nco u ragem e nt an d to pr o gr ess e x e rc is es. E x e rc is e w as ju st on e as p e ct of th ei r se rvi ce tha t w as d is cu ss e d d ur in g th es e vi sit s LiFE inter vention =7 balance and 6 low er limb str ength ex er cises incorporated into ev er yda y activities. Ex er cises w er e explained by car e manager and a descriptiv e manual was giv en to clients. Contr ol gr oup: structure d ex er cises =3x per da y 5 re petitions of 6 str ength and 2 balance ex er cises (15 – 20 minutes). Ex er cises w er e pr ovided on a sheet illustrating ex er cises. Danilovich et al, 30 , 31 HC As attended a half-da y SFL training session. HC As completed SFL with their clients 2x per w eek for the fi rst 2 w eeks of the pr ogram with clients completing a thir d session independently . After the initial 2-w eek period, HC As pr ovided their clients motivation at each usual care visit (2 – 3x per w eek) to perform SFL 3 times a w eek for an additional 10 w eeks. 12 w eeks SFL; 35-minute D VD that includes a warm up , 11 upper and low er extr emity ex er cises using therabands for re sistance , and a cool down. King et al, 32 P ai d ca re giv e rs u nd e rto ok 2 tr ain in g pr o gra m s b as e d o n a re sto ra tiv e ca re p hi lo so ph y d e sig n e d to o p ti mi ze ind e p en d e nc e in o ld e r p eo p le , ta ki n g ap p ro x ima te ly 5 and 1 8 w e ek s. Co or d in at or (ex p e ri e n ce d re gi ste re d n u rs e ) u n de rt oo k an in it ia l in -de p th as se ss m en t wi th th e p art ic ip an t u si n g T A R G ET , le ad in g to a su p p ort pl an fo r p ai d ca re gi ve rs to im p le m e n t at vis it s w ith p art ic ip an ts , ra n gin g fr om da ily to fo rtn ig ht ly . C oo rdi n ato rs pr ov id e d e n h an ce d su pe rvi sio n for p aid ca reg iv e rs by u n de rta ki n g co m -p u ls ory 2 -h ou r fort n ig h tly me e ti n gs an d al so pr ov id e d fo llow -u p co n su lt ati on s w it h p art ic ip ant (ph o n e ca ll o r vis it) e ve ry 3 m on th s, an d a fu ll re -a ss e ss m e nt at 1 2 mo n th s Repetitive ADL ex er cises designed to optimize independence and to further support par ticipant in re aching their goals Parsons et al, 33 Inter vention gr oup completed a goal facilitation tool (T ARGET) with a needs asses-sor to determine their needs and to establish the aims for the episode of care. Ser vices w er e structur ed accor ding to the principles of re storative home care (independence focused with individually tailore d activity pr ograms). HC As then completed tasks outlined in the support plan for each individual. Ho me ca re se rv ice s in clu de d d om e sti c ta sks ,pe rs on al ca re, sh op p in g, an d in d iv id ua lize d act iv it ie s (w alk in g or e x e rc is e p ro gr ams /o th e r act iv it ie s ai me d at im p ro vi n g fu n ct io n al ab ilit y) . In the in te rv e n tio n gr ou p 6 1 .7 % (n = 6 6) o f th e su p po rt p la n s de sc ri b ed su ch in di vi du al iz e d ac ti vit ie s as op p o se d to 1 5 % (n = 1 4 ) in th e u su al ca re gr o u p . Renehan et al, 36 Participants w er e appr oached 1 – 2 w eeks after discharge, inter vention included a medication re vie w , falls pr e vention education, and home-based ex er cise individually pr escribed and modi fi ed accor ding to pr e-existing frailty by ex er cise ph ysiologist (visits at w eeks 1, 2, 4, and 8 for ex er cise pr ogr ession), participants w er e pr ovided diagrams of ex er cises and instruction on ex er cise safety . Participant ’ s primar y nurse who regularly visited for other matters pr ovided encouragement. Thre e to fi ve times per w eek 20 – 30 minutes graduated low er limb str engthening and balance ex er cises (Otago Ex er cise Pr ogramme) Saeterbakk en et al, 37 A pr ofessional training instructor was pr esent at ev er y training session to mak e sure of the corr ect technique, intensity , and numbers of sets. S u per vi sed pr o gr essi ve st re ngth tr aini n g pr ogram m e 60 m inut e s 2x w e ek fo r 1 0 w eeks, 10 – 12 re p e ti ti o n s 2 – 3 set s squats, b o x lift s, seat e d ro w , chest p re ss, an d b ic ep s cur l. ( Continued )
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
T able 3 (Continued). Refer ence Implementation strateg y Inter ve ntion Ste vens-Lapsley et al, 34 Patients placed in the p rogr essiv e mu lticomp onent inter vention gr oup w er e referr e d to h o me health agency an d w er e see n by a sin gle ph ysical therapist who w as trained to p rovide th e pr ogr e ssiv e inter ve ntion. Tw o to thr ee ph ysical therap y visits p er w e ek for 3 0 da ys. Pr og re ss iv e mu lti co mp o ne n t p hys ica l th e ra p y in te rv e nt io n co n sis te d o f A DL tr ain ing (b at h ro om tr an sf e rs , b e d m ob ilit y, an d ca r tra n sf er s) , e vi de n ce -b as e d m ob ili ty tr ain ing (i n do or w alk in g, ga it tra in in g on fl at gr ou n d an d st air s, an d o ut do or w alk in g tr an si ti o n in g to an in de p e n de n t d ail y w al k in g p ro gr am) an d pr og res siv e str e n gt h tr ain in g (3 se ts 8 rep e tit ion s m ax su p in e le g p re ss , sta n di n g h ip e x te n sio n , b o dy -w e ig h t re si ste d pl an ta r fl exio n , se at e d pr ess and seat e d ro w u si n g the Shut tl e M in i P ress). P ar ti ci p ants w er e giv e n a h om e e x e rci se pr og ra m to co n ti n ue b as ic e x e rc is e s af te r di sch ar ge. T untland et al, 35 O cc u p ati on al an d p h ys ic al th e ra p is ts u se d C O P M to id en tif y ac ti vi ty lim ita tio ns p e r-ce iv e d as im p ort an t b y th e pa rti ci pa nt an d d e ve lo p e d a re h ab ilit ati on p la n w ith a m ax im u m re h ab ilit ati on pe rio d of 3 m o nt h s. T h e ra p is ts su p e rv is e d H C A w h os e fo cu s w as o n sti mu la ti n g th e p arti ci pa nt s to pe rf or m th e d ail y ac ti vi ti es th e ms el ve s, ra th er th an le tt in g o th e rs d o it fo r th e m, ph ys io th e ra p is t an d /o r o cc u p ati on al th e ra p is t vi sit ed p art ic ip ant s for a mi n im u m o f 1 h ou r e ac h w e ek . A ll H CAs att ain e d tra in in g b e fo re the in te rv en tio n wa s im p le m en ted . T h e ra p is ts h ad w ee k ly in fo rma l lu n ch m e e ti n gs w ith H CAs in o rde r to e ns ur e go od co m mu n ic at io n and fol lo w -u p o f in d iv id u al p art ic ip an ts Individualized re ablement pr ogram including training in daily activities (dr essing, food pr eparation, vacuuming, bus transport), adaptations to the en vir onment or the activity to simplify activity performance, and ex er cise pr ograms such as indoor or outdoor walking with or without walking aids, climbing stairs, transferring, and performing ex er cises to impr ove str ength, balance or fi ne motor skills. The ex er cises w er e incorporated into daily routines and participants w er e give n a manual explaining each of the ex er cises and encouraged to train on their own Abbre viations: LiFE, Lifestyle-integrated Functional Ex er cise pr ogram; SFL, Str ong Fo r Life; HC A, home car e aide; T ARGET , Towar ds Achie ving Realistic Goals in El ders Tool; ADL, activities of daily living; COPM, Canadian Occupational P erformance Measur e.
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
effects model applied and using the inverse variance
DerSimonian and Laird method.27 Heterogeneity was
assessed using the I2statistic and by visual inspection of
the forest plots. Statistical significance was set atp<0.05
for all analyses.
Results
Study selection
Eight thousand seven hundred and fifty eight papers were
found in thefive databases. After removing duplicates from
each database and then across databases, 1,679 articles remained. Articles were screened by title and 1,266 were
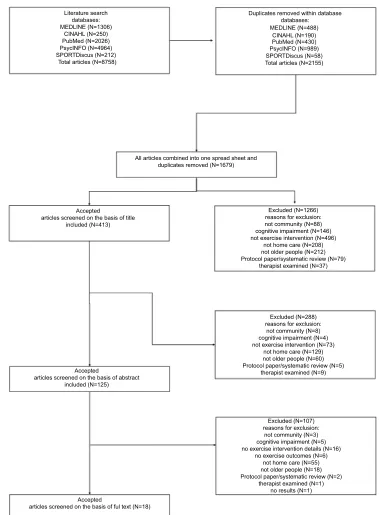
excluded. Reasons for exclusion are presented inFigure 1–
the study flow chart. Article abstracts were then read and
a further 288 excluded, leaving 125 articles to be screened by full text. One hundred and seven studies were excluded and 18 studies were accepted to be included in the review.
Study characteristics
The 18 studies in the review included ten RCTs;28–37 six
single group pre- and post-test studies;38–43one feasibility
study;44and one retrospective study.45
There were 1,118 participants across the 18 studies,
ran-ging from eight in a pilot study39to 228 in the retrospective
study.45The average age of all participants was 80.4 (±3.3)
years and ranged from 74.5–85.4 years; 71.8% of the
parti-cipants were female. Seven studies were conducted in the
United States;30,31,34,38,41,42,45six in Australia;28,29,36,39,43,44
two in New Zealand32,33 and Norway;35,37 and one in
Hong Kong.40
Interventions
RCTsThe average age of the 656 participants in the ten RCTs
was 80.4 (±3.7) years, ranging from 74.5–85.4 years and
included an average of 69.6% females. A number of dif-ferent interventions were trialed. However, the majority
focused on strength and balance training.Table 2presents
a summary of the included RCT studies and Table 3
out-lines the interventions implemented.
The two Burton et al28,29 RCTs utilized the
Lifestyle-integrated Functional Exercise (LiFE) program which incor-porates seven balance and seven strength exercises into an
older person’s daily living activities.46,47 The intervention
was compared with a structured exercise program that focused on strength and balance also in an RCT over two
time periods; 8-week intervention28 and a 4-month
maintenance period.29 It must be noted the control group
was active and received the structured exercise program that was delivered within the usual restorative care service. Whereas, Danilovich et al created the Strong For Life (SFL) resistance training program, which included a 35-minute
DVD to assist home care aides to deliver the program.30,31
The exercise intervention in King et al’s study32 used
exercises that optimized independence, incorporating
repe-titive functional ADLs. Parsons et al33 used a similar
exercise intervention, again with the aim of optimizing independence and improving functional ability by incor-porating individualized activities, 62% of the support plans described included these activities with their participants compared to 15% for the control group (ie, usual care).
Stevens-Lapsley et al34utilized a progressive
multicom-ponent physical therapy intervention for 60 days to improve functional mobility for older adults who had just left
hospi-tal. Tuntland et al35trialed a reablement intervention, which
was individualized for each participant. The exercise pro-grams typically included indoor or outdoor walking, climb-ing stairs, transferrclimb-ing, engagclimb-ing in strength and balance
training, and improving fine motor skills. Similar to the
LiFE program utilized by Burton et al,28 many of the
exercises were incorporated into ADLs. In a further study
by Saeterbakken et al,37 they conducted a 10-week
fully-supervised strength training intervention which was deliv-ered twice a week to participants.
Other studies
The other eight studies that were not RCTs included 462 participants, with an average age of 80.5 (±3.0) ranging
from 76.8–83.8 years and included an average of 74.8%
females. Table 4 presents a summary of the included
studies that are not RCTs and Table 5 the interventions
implemented. Bamgbase and Dearmon38reported
deliver-ing a 6-month individualized home exercise program with no other detail, and the main aim was preventing falls by using a multi-factorial intervention.
Burton et al39conducted a feasibility study utilizing the
LiFE program (previously described) to determine whether this intervention type could be delivered more broadly within a restorative care service. In a more recent study,
Burton et al44 conducted a feasibility study that explored
whether community care support workers who are non-allied health trained could deliver the LiFE exercise program to community care clients. It was determined that there were no adverse events and it was possible for this population to
deliver this falls prevention exercise program.44
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
The home care clients in Gallagher et al’s study45 received an individualized home exercise program which
was designed to address clients’ identified impairments
and falls hazards in the home. This study found that the Missouri Alliance for Home Care tool (MAHC-10) and interdisciplinary program was effective in identifying and
managing those who had fallen in their home.45
The 6-month intervention delivered by Kwok and
Tong40 was a multicomponent exercise program,
consisting of flexibility, strength, balance, and aerobic
exercises, either delivered by a physiotherapist in
a center or by a care worker in the home. The physiother-apy-led center-based intervention was found to improve physical function, quality of life, and fall incidence, whereas the home-based care worker led program had no
effect on physical function and self-rated health.40
Muramatsu et al41 conducted a motivational
enhance-ment and three chair-bound moveenhance-ments program delivered
Literature search databases:
Duplicates removed within database databases:
All articles combined into one spread sheet and duplicates removed (N=1679)
Accepted
articles screened on the basis of title included (N=413)
Excluded (N=1266) reasons for exclusion: not community (N=88) cognitive impairment (N=146) not exercise intervention (N=496)
not home care (N=208) not older people (N=212) Protocol paper/systematic review (N=79)
therapist examined (N=37)
Excluded (N=288) reasons for exclusion:
not community (N=8) cognitive impairment (N=4) not exercise intervention (N=73)
not home care (N=129) not older people (N=60) Protocol paper/systematic review (N=5)
therapist examined (N=9)
Excluded (N=107) reasons for exclusion:
not community (N=3) cognitive impairment (N=5) no exercise intervention details (N=16)
no exercise outcomes (N=6) not home care (N=55) not older people (N=18) Protocol paper/systematic review (N=2)
therapist examined (N=1) no results (N=1) Accepted
articles screened on the basis of ful text (N=18) Accepted
articles screened on the basis of abstract included (N=125) MEDLINE (N=1306)
CINAHL (N=250) PubMed (N=2026) PsycINFO (N=4964) SPORTDiscus (N=212)
MEDLINE (N=488) CINAHL (N=190) PubMed (N=430) PsycINFO (N=989) SPORTDiscus (N=58) Total articles (N=8758) Total articles (N=2155)
Figure 1Flow chart of study selection.
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
T
able
4
Summar
y
of
included
non-randomized
contr
olled
trial
(RCT)
studies
Refer
ence
(coun-tr
y)
Study
design
Study
purpose
Sample
siz
e;
%
female;
a
g
e
(y
ears)
(SD)
comparator
P
opulation
Outcomes
and
measur
e-ment
follo
w-up
Inter
v
ention
effect
Bamgbade
and
Dearmon,
38
(USA)
Quasi-experimental
sin-gle
gr
oup
study
pr
e
and
post-test
Evaluate
the
impact
of
a
fall
assessment
tools
and
patient-speci
fi
c
fall
pr
e
vention
pr
ograms
in
re
ducing
the
inci-dence
of
falls
and
fall-r
elated
inju-ries
among
older
patients
receiving
home
HHS
30;
sex
unknown;
aged
65
and
ov
er
No
Receiving
nursing
care
ser
vices
on
a
long-term
basis.
Suffer
var
ying
degr
ees
of
ph
ysical,
mobility
,
or
cognitiv
e
impair
-ments,
such
as
diabetes,
str
ok
e,
and
urinar
y
incontinence
Number
of
falls
and
falls
with
injuries
6
months
Reduction
of
falls
and
major
injuries.
Bur
ton
et
al,
39
(Australia)
Quasi-experimental
single
gr
oup
study
pr
e-and
post-test
(pilot)
Determine
whether
a
LiFE
was
suitable
for
deliv
er
y
in
a
restorativ
e
home
car
e
ser
vice
8;
75%;
80.8
years
(5.9)
No
Curr
ent
restorativ
e
home
car
e
clients,
living
in
P
erth
(W
estern
Australia)
Functional
re
ach,
chair
sit-to-stand
(1
and
5),
TUG,
T
andem
walk,
FES,
ABC
Scale,
Vitality
Plus
Scale,
The
Late
Life
Function
and
Disability
instruments,
PASE,
Acceler
ometer
,
LiFE
Assessment
tool, 8w
eeks
Dif
fi
culties
using
the
acceler
-ometer
and
LiFE
Assessment
tool.
Signi
fi
cant
impr
ove
ment
in
FES,
tandem
walk,
Late
Life
Function
total
scor
e,
and
PASE
Bur
ton
et
al,
44
(Australia)
F
easibility
study
To
in
vestigate
the
feasibility
of
community
care
w
ork
ers
deliv
er
-ing
a
falls
pr
e
vention
ex
er
cise
pr
ogram
to
older
clients,
at
low
or
medium
risk
of
falling,
as
part
of
an
existing
ser
vice
pr
ovision
29;
65.5%;
82.7
(8.7)
years No
Older
adults
receiving
at
least
one
community
car
e
ser
vice
fr
om
a
participating
community
care
organization
or
an
RAS
assessment,
living
in
P
erth,
W
estern
Australia
FR
OP-Com,
Ph
ysical
Activity
Readiness
Questionnair
e
(P
ARQ)
and
LiFE
assessment
tool
mea-sur
ed
at
baseline.
Client
and
staff
pr
ogram
satisfaction
measur
ed
post-test. 8w
eeks
LiFE
ex
er
cise
pr
ogram
was
safely
deliv
er
ed
by
RAS
assessors
and
support
w
ork
ers,
with
no
adve
rse
e
ve
nts
reported.
The
majority
of
clients
(82%)
repor
ted
enjo
ying
the
ex
er
cises,
59%
felt
it
made
a
positiv
e
change
to
their
health.
Ex
er
cise
adher
ence:
4.8
(SD:
2.2)
da
ys
per
w
eek.
Gallagher
et
al,
45
(USA)
Retr
ospectiv
e
Determine
concurrent
based
validity
of
the
MAHC-10
with
the
P
erformance
Oriented
Mobility
Scale
(Tinetti),
and
determine
the
bene
fi
t
of
the
Balanced
Appr
oach
rehabilitation
pr
ogram.
228;
sex
unknown;
aged
65
and
ov
er
No
Patients
re
ferre
d
for
home
car
e
ser
vices
to
Catholic
Home
Car
e
MAHC-10
and
Tinetti
scor
es
6
months
Ther
e
was
w
eak
but
signi
fi
cant
negativ
e
re
lationship
betw
een
the
MAHC-10
and
pr
e-Tinetti
scor
es.
Signi
fi
cant
differe
nces
in
Tinetti
score
s
betw
een
pr
e-and
post-inter
vention
(
Continued
)
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
T able 4 (Continued). Refer ence (coun-tr y) Study design Study purpose Sample siz e; % female; a g e (y ears) (SD) comparator P opulation Outcomes and measur e-ment follo w-up Inter v ention effect Henw ood et al, 43 (Australia) Single gr oup study pr e-and post-test De velop an HC A-led ex er cise pr ogram for older adults with aged care needs and e valuate the bene fi ts fr om both the perspec-tiv e of the HC A and the person receiving the pr ogram 50; 74%; 82.1 years (6.1) No Older adults receiving gove rn-ment-funded domestic assistance or personal car e in Brisbane, Australia SPPB, falls, hours of sleep , visits to a general or clinical practice health pr ofessional, emergency depart-ment/hospital, ex er cise compli-ance, SF-36 18 w eeks Signi fi cantly impr ove d SPPB scor e, 19% re duction in par ticipants classi fi ed as frail and a re duction in health car e ser vice access of 47% acr oss the inter vention Kw ok et al, 40 (Hong K ong) Quasi-experimental pr e-and post-test Compar e the effects of an ex er -cise pr ogram super vised by a ph ysiotherapist at a da y training center with an ex er cise pr ogram deliv er ed by a care w ork er at home on ph ysical function, quality of life , and fall incidence in com-munity-dw elling older adults Center -based =24; 70.8%; 84.4 years (6.9) Home-based =26; 73.1%; 83.2 years (7.0) 5 center -based and 4 home-based participants had MMSE <12 Ye s Clients admitted to the Enhanced Home and Community Car e Ser vice team, re siding in the W ong T ai Sin District (Hong K ong). Suffering fr om chr onic diseases with moderate or se ver e le vel of impairment Elderly Mobility Scale, BBS, Numeric Pain Rating Scale, SF-12, and fall incidence 6 months Center -based participants had sig-ni fi cant impr ov ement in all out-comes and less falls compared to home-based participants Muramatsu et al, 41 (USA) Single gr oup study pr e-and post-test Test and enhance the feasibility of HM pr ogram deliv er ed by HC As for community-dwelling older adults in a Medicaid-funded home car e setting 54; 78%; 77 (63 – 101) years; almost 1/3 had mild cognitive impair -ment No Receiving in-home support ser -vices thr ough the Illinois Departm ent on Aging Community Car e Pr ogram, Chicago Daily activity dif fi culties and dependency (HM6, BADL, IADL), performance of 3 HM mov ements, SSPB, self-rated general health and pain, FES-I, falls, and ex er cise re lated social support 4 months Clients ‘ daily activity function and health outcomes impr ov ed signi fi -cantly . The pr ogram was w ell-re ceiv ed by clients, high re tention rates among clients (93%) Park and Chodzk o-Zajk o , 42 (USA) Single gr oup study pr e-and post-test Assess the feasibility of imple-menting simple, safe, non-equipment ev idence-based mov e-ments (HM pr ogram) using an affor dable and sustainable HC A based deliv er y model that re aches the maximum possible number of frail older adults living at home but who ar e at risk of nursing home admission 13; 84.6%; 76.8 years (11.4) No Older adults re ceiving home car e ser vices pr ovided by Help at Home and Family Ser vice; home visit pr ograms funded by Older American ’ s Act in the State of Illinois Evaluation sur ve ys and inter vie ws with clients, HC As, and site dir ectors. Functional ability of cli-ents: 30-seconds chair stand, 30-seconds arm curl (5 pounds for females, 8 pounds for males) and chair sit and re ach 4 months Clients signi fi cantly impr ov ed number of arm curls in 30 sec-onds. No signi fi cant impr ov ement in chair stand or chair sit and re ach. Most participants had a positiv e per ception and high satisfaction with the pr ogram. HM could be safely and successfully disseminated to frail older adults Abbre viations: MAHC-10, Missouri Alliance for Home Car e tool; LiFE, Lifestyle-integrated Functional Ex er cise pr ogram; FES, Falls self-Ef fi cacy Scale; ABC , Activities speci fi c-Balance Con fi dence Scale; TUG, Timed Up and GoP ASE, Ph ysical Activity Scale for the Elderly; RAS, Regional Assessment Ser vice; HC A, home care aide; SPPB, Short P erformance Ph ysical Batter y; FR OP-Com , Falls Risk for Older P eople – Community Setting; MMSE, Mini Mental State Examination; BBS, Berg Balance Scale; BADL, Basic Activities of Daily Living; IADL, Instrumental Activities of Daily Living; HM, Health y Moves ; FES -I, Falls self-Ef fi cacy Scale – International.
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
T able 5 Inter vention implementation of included non-randomized contr olled trial (RCT) studies Refer ence Implementation strategy Inter v ention Bamgbade and Dearmon, 38 Staff pr oviding nursing car e to patients of the privately owned home health car e agency w er e educated on the fall pr e vention pr ogram MAHC-10 fall risk assessment tool, medication re vie w pr ocess and management plan, home safety assessment, patient-and family-speci fi c education, individualized home-based ex er cise regimen Bur ton et al, 39 LiFE pr ogram was deliv er ed by car e managers as part of a restorativ e home car e ser vice. Car e managers explained to the client the differ ent ex er cises and how these ex er cises could be incorporated into their daily routines, manual also pr ovided. Clients w er e visited e ver y 10 – 14 da ys by their care manager (a ve rage 3 visits) to monitor how w ell the client was performing the fi rst ex er cises agr eed to and to encourage the client to start doing others. Ex er cise was just one aspect of their ser vice that was discussed during these visits 7 balance and 6 low er limb str ength ex er cises incorporated into e ver yda y activities Bur ton et al, 44 Staff completed a 4-hour training session on deliv ering the LiFE ex er cise pr ogram. Each staff member re ceiv ed 3 client folders, a staff folder and a LiFE trainer ’ s manual. Community car e w ork ers follow ed-up with their clients either during their usual ser vices or on a fortnightly basis 7 balance and 6 str ength ex er cises to complete whilst undertaking usual daily activities Gallagher et al, 45 Staff was trained in assessing risk factors and in fall pr e vention measur es. The training sessions took place ov er a 6-hour period and w er e follow ed-up by performance-based competencies and case studies. Patients w er e e valuated with MAHC-10, score s ≥ 4 of 10 (indication of high risk for falls) starte d on the Balanced Appr oach rehabilitation pr ogram. The CHC falls scre ening and Balanced Appr oach re habilitation pr ogram was designed to re duce the risk of falls in a home care population using an inter disciplinar y appr oach T reatment fr om ph ysical and occupational therapists aims to impr ov e gait, balance, balance con fi dence and reduce fall risk thr ough individualized home ex er cise pr ogram designed to addre ss impairments and home safety/mobility adaptations. The home pr ogram is in place for as long as the patient demonstrates a bene fi to r until safety/independence is achie ved (a verage 8 visits, 45 – 60 minutes each) Henw ood et al, 43 HC As attended a 1-da y w orkshop and receiv ed a printed manual containing detailed instructions for each ex er cise, information on health y lifestyle beha viors, and an ov er vie w of common barriers and enablers to ex er cise particip ation. HC As visited clients we ekly or fortnig htly for 60 – 90 minutes with at least 10 minutes assisting and monitoring client par ticipation in the ex er cise pr ogram 5 str ength ex er cises (chair stand, seated leg extension, standing calf raise, wall push-ups, theraband seated rows, pr ogressing to 3 sets of 12 repetitions), 3 balance ex er cises (single leg stand for up to 20 seconds on each side , tight rope walk of 10 steps forwar d and back, 10 re petitions side to side step). Clients w er e encouraged to ex er cise on most, pr eferably all da ys Kw ok et al, 40 Parti cipants chose to receiv e ex er cise training at either a da y training center under super vision of a ph ysiotherapist (gr oups of 6 – 10 participants) or individually at home assisted by a car e w ork er . Ph ysiotherapists pr ovided training to all care w ork ers and monitore d their performance e ver y 2 – 3 months thr ough on-site super vision to ensure quality of the training pr ogram at home 6 month fl exibility , str ength, balance, and aer obic ex er cise pr ogram with pain management, 1 – 2 sessions per w eek lasting appr o ximately 60 minutes ( Continued )
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
by home care aides for their clients over a 4-month
interven-tion. Results showed a significant improvement in physical
fitness, self-rated health, pain interference, Short Physical
Performance Battery (SPPB) total score, SPPB balance
tests, and fear of falling.41Park and Chodzko-Zajko42also
conducted a 4-month intervention called“Healthy moves for
aging well”which incorporated a physical activity
interven-tion with a lifestyle behavior change counseling method called Brief Negotiation. The activity portion of the
interven-tion was the same as that used by Muramatsu et al.41Arm
curl was the only functional ability outcome that reported
improvement between pre- and post-testing (p=0.021).42
Henwood et al’s43 Active@Home 18-week program
included weight bearing and balance exercises and was tailored to the level of the participant. The exercise pro-gram was delivered by home care support workers, with at least 10 minutes of their service time spent monitoring the
exercises.43Significant improvement was found for
func-tional capacity as measured by the SPPB and a 19%
reduction in participants classified as frail.43
Outcome measures
RCTsThere was a variety of outcome measures utilized by the
included studies. The main physical test utilized byfive of
the RCTs was the TUG test.28–30,32,35 Unfortunately
Danilovich et al30 could only provide medians and
inter-quartile ranges rather than means and SDs for the TUG,
and only the intervention phase data of Burton et al’s28
study were included to provide similarity with the other studies included which assessed the post-intervention
per-iod. Four of the RCTs28,33,37,48 used the sit-to-stand five
times test and these data have been included in a meta-analysis.
Two RCTs33,34 utilized SPPB but unfortunately, after
many emails, the authors were unable to obtain the data
required for the Stevens-Lapsley et al34study. Therefore,
no meta-analysis could be conducted. The grip strength
test30,35 and gait speed/walking tests were used in two
RCTs each respectively.30,34 The data from the
Stevens-Lapsley et al34study were not available, however, Tinetti
et al’s study which was included in the previous systematic
review, measured walking speeds and was included in the meta-analysis.
Other studies
The SPPB test was used in two of the non-RCT studies38,43
and five of these studies also collected data on
T
able
5
(Continued).
Refer
ence
Implementation
strategy
Inter
v
ention
Muramatsu
et
al,
41
HC
As
receiv
ed
4
hours
of
training
on
how
to
deliv
er
the
HM
pr
ogram.
At
the
initial
visit
(a
verage
27
minutes,
range
10
–
45
minutes)
HC
As
assessed
re
adiness
for
PA,
had
their
clients
set
personally
meaningful
goals,
and
taught
the
3
chair
-bound
mov
ements.
HC
As
re
minded
their
clients
of
their
personal
PA
goal/r
ou-tines
as
part
of
their
regular
home
care
and
logged
their
HM
activities.
Fr
equency
of
HC
A
home
visits
depended
on
the
client
’
s
care
needs
assessed
by
the
Illinois
Determination
of
Needs
instrument
(typically
3x
per
w
eek
or
12
hours
per
w
eek)
Each
da
y
clients
completed
15
arm
curls
2
times
(holding
a
1-pound
w
eight
supplied
by
the
pr
oject,
or
a
soup
can
or
water
bottle),
ankle
point
and
fl
ex
up
to
30
seconds
on
each
foot
3
times
and
seated
step-in-place
up
to
1
minute
Park
and
Chodzk
o-Zajk
o
,
42
HC
As
attended
a
training
session
to
deliv
er
HM,
this
included
how
to
teach
the
clients
the
3
chair
bound
mov
ements
whilst
utilizing
Brief
Negotiation
techniques
as
a
motivational
tool.
HC
As
visited
the
client
in
the
home
and
w
er
e
ask
ed
to
deliv
er
the
HM
pr
ogram
on
a
re
gular
basis
for
a
4-month
time
period
Each
da
y
clients
completed
15
–
20
arm
curls
2
times
(holding
a
1-pound
w
eight,
either
soup
can
or
water
bottle),
ankle
point
and
fl
ex
w
orking
up
to
30
seconds
on
each
foot
3
times
and
seated
step-in-place
w
orking
up
to
1
minute
Abbre
viations:
MAHC-10,
Missouri
Alliance
for
Home
Car
e
tool;
LiFE,
Lifestyle-integrated
Functional
Ex
er
cise
pr
ogram;
CHC
,
Catholic
Home
Car
e;
HC
A,
home
care
aid
e;
PA,
ph
ysical
activity;
HM,
Health
y
Mov
es.
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
falls,38,40,41,43,45as did Renehan et al36in their RCT. Other physical performance measures used by single studies included functional reach, sit-to-stand one time, tandem walk (including tandem walk errors), and the six minute walk test. Health-related quality of life was measured using the SF-36, SF-12, EQ5D, AQol-8D, and the COOP/Wonka.
Falls related assessments included the falls efficacy scale,
activity-specific balance scale, the Falls Risk for the Older
Person living in the Community and the MAHC-10 falls assessment tool.
Dropout and adherence to exercise
interventions
Participant withdrawal rates ranged from 3.9%–3323.3%,37
with an average dropout rate of 13.5% (±7.0). Adherence
rates were reported in seven of the studies.28,29,37,38,41,43,44
Bamgbade and Dearmon38stated 17% (n=5) of their
parti-cipants performed the exercises as instructed over the 2
months. In Burton et al’s28,29RCT studies, the intervention
group reported completing the activities 4.9 times/week during the intervention period (8 weeks) and 4.1 times/ week across the 6-month study, and the control group 4.4 times/week during the intervention (8 weeks) and 3.7 times/ week across the 6 months. In the 8-week study, adherence to exercise interventions delivered by community care
sup-port workers was resup-ported at 4.9 (±2.2) times per week.44
Henwood et al43reported adherence of 5.1 (±0.6) sessions
per week across the 18-week intervention and Saeterbakken
et al37 noted 84% adherence in the 10-week intervention.
Muramatsu et al41 reported half of their participants had
completed 5–7 days training each week at the end of the
intervention (4 months), 32% (n=16) 2–7 days/week at the
end, 16% “low“(“low“not described) and 2% did not do
any of the exercises.
Quality of the studies
In general, the quality of the ten RCT studies was rated
“medium” to “high”, suggesting low risk of bias.
Assessment details for potential bias in each study is
presented in Table 6. The two Burton et al28,29 studies
and Saeterbakkan et al's study37did not blind their
parti-cipants, assessors or those delivering the intervention (ie, care managers) and were therefore deemed to be high risk
for blinding. Allocation concealment was unclear forfive
of the studies and some were deemed not free of bias by the reviewers due to uneven or small sample size groups.
Sequence generation and incomplete outcome data
appeared to be well described and were at low risk of bias for the majority of studies.
Similar to the RCTs, the quality of the eight other studies was between ++ and + on the assessments, where
it was deemed that most had satisfied the criteria for
internal and external validity. It must be noted however, that all but one study did not have a comparison group, which meant a number of criteria were consequently not
reported.Table 7presents the assessment of quality for the
non-RCT studies included in the review.
Effectiveness of intervention programs
Results from seven of the RCTs were included in the
meta-analyses.28,30,32,33,35,37,48,49Two authors responded to data
requests30,35and their data have been included in the
meta-analysis, one other author responded but did not provide
their data.34
Table 6Randomized controlled trial (RCT)–assessment of risk of bias of RCTs
Study Sequence
generation
Allocation concealment
Blinding Incomplete
outcome data
Selective out-come reporting
Free of other bias
Burton et al,28 + + - + + ?
Burton et al,29 + + - + + ?
Danilovich et al,30 + ? + + ?
-Danilovich et al,31 + ? + + ?
-King et al,32 + ? + + + ?
Parsons et al,33 ? ? + + +
-Stevens-Lapsley et al,34 + ? + + +
-Tuntland et al,35 + + ? + +
-Saeterbakken et al,37 + + - - ?
-Renehan et al,36 + + + + -
-Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020
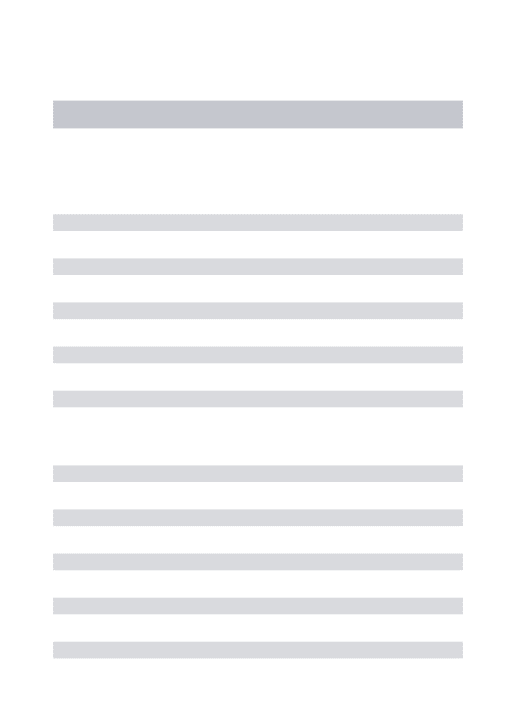
Figures 2–5present the data in forest plots for the TUG,
sit-to-stand five time, grip strength, and walking speed
respec-tively. Heterogeneity for TUG (I2=62%) and sit-to-standfive
times (I2=65%) was high. The grip strength and walking speed
(meters per second) analyses had no heterogeneity (I2=0).
Sit-to-stand five times was also analyzed in subgroups because
there appeared to be two samples that had better function28,48
and two poorer function.33,37 The difference between those
with better function and those with poorer function was
sig-nificant (χ2=4.05, df=1 (p=0.04),I2=75.3%). However,
hetero-geneity was high and there was no significant improvement
overall between the intervention and control groups for
sit-to-standfive times across the four studies. Walking speed was the
only test which reported an overall significant (MD: 0.02,
p<0.001) difference. In this case, it favored the usual care (ie,
control) group in Tinetti et al's49study. TUG, sit-to-standfive
times, and grip strength showed no statistically significant
difference between the groups for these tests.
Discussion
This systematic review identified a further 18 studies, since the
previous systematic review was published,22which examined
the effectiveness of physical activity/exercise interventions for older adults receiving home care services. Previously there were no studies included from Australia, however, in the last 6 years, six studies have been conducted, providing evidence for Australian home care agencies and national and state governments who fund these services. Disappointingly, we found no published studies from a number of large countries who provide home care services to older adults such as the United Kingdom, European countries (ie, the Netherlands, Ireland, Germany), and Scandinavia (other than Norway), and no studies from low to middle income countries.
Lack of consistency in methodology and measures has limited the potential to conduct meaningful meta-analyses in this area. Of the four outcomes that were analyzed by
meta-analysis, only walking speed changed significantly between
the intervention and control groups. On this occasion, the control group demonstrated faster walking speeds than the intervention group. This was predominantly due to Tinetti
et al’s49study, which reported a faster walking speed (m/s)
for the usual care group at 6 months than the intervention group. However, walking speeds were found to be the same for each group at 12 months, which was 6 months
post-intervention.49 Tinetti et al49 did note that the intervention
group was significantly more likely to be using a walking
stick than the control group at the end of the 6-month inter-vention. The intervention group also had more visits from
T able 7 Randomized contr olled trial (RCT) – assessment of quality of non-RCT papers Study 1.1 1.2 1.3 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 2.9 2.10 3.1 3.2 3.3 3.4 3.5 3.6 4.1 4.2 4.3 4.4 4.5 4.6 5.1 5.2 Bamgbade and Dearmon, 38 + NR NR NA + NA NA NA NA NA ++ ++ ++ + ++ + ++ NA + NA NA NR NR + NR -+ Burton et al, 44 ++ + + NA ++ NA NA NA NA NA ++ ++ ++ ++ + ++ ++ NA ++ NA NA NR NR ++ ++ + ++ Henw ood et al, 43 ++ + + NA ++ NA NA NA NA NA + ++ + + + ++ ++ NA + NA NA NR NR ++ + -+ Kwok and T ong, 40 ++ ++ ++ + + -+ + ++ + ++ + ++ + ++ + ++ ++ + ++ ++ + ++ ++ + ++ + Muramatsu et al, 41 + + ++ NA ++ NA NA NA NA NA ++ ++ ++ + ++ + ++ NA + NA NA NR NR ++ + + + Park and Chodzk o-Zajk o , 42 ++ + + NA + NA NA NA NA NA ++ ++ ++ + ++ + + NA ++ NA NA NR NR ++ + + + Burton et al, 44 ++ + + NA ++ NA NA NA NA NA ++ ++ ++ + ++ ++ ++ NA ++ NA NA NR NR ++ NR + ++ Gallagher et al, 45 + + + NA + NA NA NA NA NA NA ++ ++ ++ ++ + ++ NA + NA NA ++ ++ ++ ++ + + Notes: 1.1: Is the sour ce population or sour ce ar ea w ell described?; 1.2 :Is the eligible population or ar ea re pr esentative of the sour ce population or ar ea? ; 1.3: Do the selected participants or areas repres ent the eligible population or area ?; 2.1: Allocation to inter vention (or comparison). How was selection bias minimized?; 2.2: W er e inter ventions (and comparisons) wel l describ ed and appr opriate?; 2.3: W as the allocation concealed?; 2.4: W er e participan ts or inv estigators blind to exposure and comparison?; 2.5: W as the exposur e to the inter vention and comparison adequate?; 2.6: W as contamination accept ably low?; 2.7: W er e other inter ventions similar in both gr oups?; 2.8: W er e all participants accounted for at study conclusion?; 2.9: Did the setting re fl ect usual UK practice?; 2.10: Did the inter vention or contr ol comparison re fl ect usual UK practice?; 3.1: W er e outcome measur es reliable?; 3.2: W er e all outcome measur ements complete?; 3.3: W er e all important outcomes assessed?; 3.4: W er e outcomes re le vant?; 3.5: W er e there similar follow-up times in expos ur e and comparison gr oups?; 3.6: W as follow-up time meaningful?; 4.1: W er e exposure and comparison gr oups similar at baseline? If not, wer e these adjusted?; 4.2: W as intention to tr eat analysis conducted?; 4.3: W as the study suf fi ciently pow er ed to detect an inter vention effect (if one exists); 4.4: W er e the estimates of effect size given or calculable?; 4.5: W er e the analytical methods appr opriate?; 4.6: W as the precis ion of inter vention effects giv en o r calculable? W er e they meaningful?; 5.1: Ar e the study re sults internally valid (ie, unbiased)?; 5.2: Ar e the fi ndings generalizable to the sour ce population (ie, externally valid)?
Clinical Interventions in Aging downloaded from https://www.dovepress.com/ by 118.70.13.36 on 20-Aug-2020