r
International Journal of Current
Medical and Pharmaceutical
Research
Available Online at http://www.journalcmpr.com
REVIEW ARTICLE
IMMEDIATE IMPLANTS- A REVIEW
Kale Rutuja P., Chacko Lisa., Rakhewar P. S and Shah Tanvi H
Department of Periodontics, S.M.B.T Dental College, Hospital and Research Centre,
Sangamner 422608, Ahmednagar – India
ARTICLE INFO ABSTRACT
Immediate implants are placed in fresh extraction sockets immediately after tooth extraction. This helps reduce the treatment time and preserves the dimensions of alveolar ridge. Several anatomical and surgical factors need to be considered before placement of immediate implants. The surgical requirements for immediate implantation include extraction with the least trauma possible, preservation of the extraction socket walls and thorough alveolar curettage to eliminate all pathological material. Primary stability must be obtained during immediate implant placement. Many authors consider that it is easier to obtain primary stability with rough surfaces, aggressive thread design, and tapered implants. Although some of the early implant practitioners assume that long term implant survival depended on placement on healed alveolar ridge, the growing body of evidence confirms that immediate implant placement yields excellent and predictable results. Several studies have showed that the survival rates of implants placed immediately, early, delayed, or late seemed to be similar in the short term and amount to approximately 95%.
This article reviews available literature to delinate the socket physiology following extraction, indications, contraindications, advantages and disadvantages along with the decisional criteria and surgical technique for immediate implant installation.
Copyright © 2017 Kale Rutuja P. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
INTRODUCTION
Immediate implant is defined as implant placement in a fresh
extraction socket immediately after tooth extraction.1Immediate placement of a dental implant was described for the first time in 1976 by Schulte and Heimke.2 Since then several clinical and histologic investigation have demonstrated its virtues.3-8 The installation of implants in extraction sockets was advocated as a means to firstly reduce the number of surgical procedures, secondly to preserve the dimensions of the alveolar ridge, and also, to reduce the interval between the removal of the tooth and the insertion of the implant supported restoration.9 To begin with this procedure was considered unpredictable, but with the development of new protocols and improved diagnosis, it now has similar final results to other loading protocols and in some cases even better.10
Successful immediate implant placement may be possible in all regions of the jaws, although immediate placement of implants in sockets of molars is more challenging.1
Recently immediate/early placement protocols have gained a growing interest and application to become an acceptable treatment approach particularly in the aesthetic zone.11This is because the extraction of teeth resulting from pathologic
changes or trauma usually causes the loss of the hard and soft tissues.12
In regard to the placement of immediate implants, several factors should be considered, the anatomy of the extraction site, the surgical procedure, the gain of time, the predictability of osseointegration and the aesthetic result of the restoration.12 Other factors to be considered are the patient’s aesthetic demands, the operator’s knowledge, experience and clinical skills; and the topography and state of health of extraction site.12
Socket Physiology
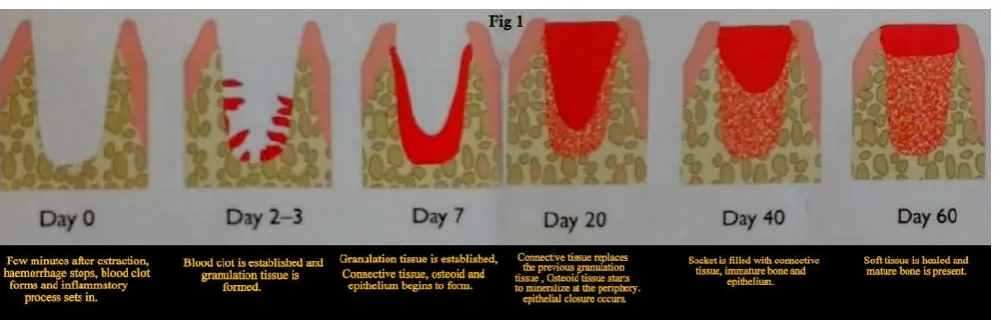
After tooth extraction the principal alterations occur in early stages, namely within the first 8 weeks, while the remodelling process may take up to 12 months following extraction. The principal alteration is volumetric in nature, i.e., there is a reduction in alveolar crest thickness that is greater than the vertical reduction. Vertical crest resorption is greater in the buccal plate than in the lingual and palatal areas. Without the use of any preventive measures, the socket bone loss is approximately 50%, especially in the maxilla.1,13-16
Following is the timeline that illustrates the socket healing process. This timeline may however vary from author to patient:17
Article History:
Received 12th November, 2016 Received in revised form 27th December, 2016
Accepted 26th January, 2017 Published online 28th February, 2017
Key words:
Though there is presence of mature bone after 2 months, bone remodelling may continue even 1 year after extraction until there is normalization with adjacent edentulous bone level. However, the majority of bone alterations (Fig 1) occur during these first months.18-20
Indications10,12
All tooth extraction without active infection (caries, crown or root fractures, endodontic problems)
Traumatic tooth avulsion with bone walls preserved
Temporary tooth root resorption with permanent tooth agenesis
Contraindications10,12
Absence of bone walls surrounding dental implant
Insufficient apical bone to achieve primary stability
Presence of anatomic limitation (inferior dental nerve or sinus)
Acute periapical infection
Surgical technique for immediate implants
The procedure for immediate implant placement must be considered different from the conventional method regardless of whether the esthetics is compromised. Nevertheless, ideal three-dimensional (3D) implant positioning (Fig 4) must be assessed as well as appropriate implant diameter according to the socket morphology.15,21-24
In order to preserve the integrity of alveolar bone walls dental extraction should be performed with no bone fractures. Periodontal ligament (PDL) should be broken with a microsurgical scalpel or periotomes. (Fig 2a ,Fig 2b)
A number of instruments and technologies are currently on the market to assist the surgeon in implementing atraumatic extraction therapy. These range from simple hand instruments (Periotomes, lexi-cuts) to powered and ultrasonic, piezoelectric devices.
Mesiodistal or buccolingual movements should be avoided to prevent breakage of thin bone walls (Fig 2c, Fig 2d)
Buccal wall must be kept to prevent bone loss in this area, which is most susceptible to resorption. (Fig 2e)
Complete debridement of all the alveolar walls with curettes, which should also be used to assess socket morphology and integrity. (Fig 2f)
Implant drilling should be performed towards the palatolingual area and the implant head should not emerge too buccally, achieving primary stability from the apical area of the socket (at least 3-5mm of inmate bone-to-implant contact (BIC), maintaining atleast 2mm from the external buccal wall,3mm in-between implants and 1.5mm from the natural tooth. The use of surgical stent is recommended to orient implant placement (Fig 2g, Fig 2h)
In case of biradicular premolars and canines and maxillary and mandibular molars implants are placed preferentially in the centre of the socket (anchoring to the interradicular septum) or in the palatal root. In maxillary molars, owing to the presence of 3 roots, primary stability is often challenging and delayed implant placement should be considered.16
If the gap distance is significant, grafting may be necessary to avoid soft tissue growth and allow the implant to osseintegrate. (Fig 2i, Fig 2j)
Primary closure of the wound should be achieved by soft tissue (pedicled flap, connective tissue graft or coronal position of the flap) or covered by a resorbable membrane to protect the surgical area. A non-submerged technique can also be attempted with predictable outcomes with the use of a provisional restoration or a healing abutment.
Advantages10,12
Fewer surgical interventions required.
Shorter treatment time.
Ideal 3-dimensional implant positioning references.
Presumptive preservation of alveolar bone at the site of the tooth extraction.
Soft tissue esthetics and maintenance.
Disadvantages10,12
The morphology of the site, leading to increased surgical difficulty.
The presence of periapical pathology.
The absence/reduction of keratinized tissue.
Esthetic compromise with thin tissue biotypes.
Courtesy: Federico Hernandez Alfaro.Controversial Issues In Implant Dentistry.
Guidelines for Immediate Implant Placement In Single Post Extraction Site
Mauro merlidelinated six anatomical factors and two surgical factors for immediate implant placement in single postextraction site.25
Anatomical Factors
Biologic width of the periodontium: In Periodontology, the
vertical biologic width of healthy gingival tissue is described as a relatively constant dimension. In conditions of periodontal health and integrity, it measures approximately 3mm.Biological width of periodontium at the implant placement site should be adequate.
Gingival biotype: The thick gingival biotype often features
dense, fibrotic soft tissue with an underlying bone volume that is also thick. The thin gingival biotype is characterised by the presence of thin soft tissue and is likely to present fenestrations or dehiscences in the underlying bone structures. A thin gingival biotype contraindicates immediate implant placement especially in anterior maxillary area.
Position of buccal gingival margin: A more coronal buccal
gingival margin may indicate implantation immediately after extraction, while a margin at the same height or apical to the equivalent tooth makes a different approach preferable.
Alveolar bone crest height in interproximal area:When the
distance between the interproximal alveolar bone crest and contact point is equal to or less than 5mm (or similarly, when the distance between the adjacent tooth’s interproximal alveolar crest and the CEJ is roughly 2mm), it would be possible to contemplate immediate implant placement. However, when these distances are greater, immediate implant placement would very likely result in esthetic failure.(Fig 3)
Buccal alveolar bone crest height: The bone crest may be
classified as high, normal, or low according to a distance from the free gingival margin of less than 3mm, 3mm, or more than 3mm, respectively. This classification, as proposed by Kois (1994)26 and Vacek et al (1994)27 permits the assumption that high and normal crests will be reasonably stable in terms of post extraction soft tissue healing (greater gingival margin stability) while low crests tend to be unstable.
Buccal alveolar bone wall thickness: Some authors28 believe
that atleast 1mm of buccal alveolar bone thickness is desirable to obtain marginal stability. Unless reconstructive bone treatment is performed, placement of an implant in a socket with reduced thickness (less than 1mm) or with a buccal alveolar bone deficit will inevitably be followed by soft tissue recession with potential exposure of the implant collar 29,30 and lack of harmony between the implant supported prosthetic crown and adjacent natural crowns. In the posterior sextants, any presence of limiting anatomical structures may be considered a further anatomical factor to be taken into consideration.
Surgical Factors:25
3D implant positioning in alveolar bone
Prosthetically guided endosseous implant placement (or 3D placement) requires consideration of three dimensions:
Mesiodistal
Buccopalatal/lingual
Apicocoronal.
Mesiodistal dimension- It is important to consider the
horizontal biologic width (approximately 1.3mm) surrounding the implant by avoiding implant placement too close to one of the patient’s own teeth. 31-33 Failure to ensure a correct mesiodistal space will lead to bone crest resorption and consequent reduction in papilla height.34,35An interproximal distance of at least 1.5mm should therefore be maintained between the implant platform and the periodontal attachment of the interproximal tooth .36(Fig 4a)
Ideal 3D implant positioning
Apicocoronal position: apical from CEJ of adjacent teeth (tissue level implants 2mm, bone level implants 3 mm, from the gingival level of the future restoration).
Buccopalatal position: 1.5-2 mm towards the palatal, maintaining minimally 2mm of buccal wall.
Buccopalatal/lingual dimension- Once placed, the implant
must have a suitable thickness of buccal bone in a buccolingual direction in order to prevent the inevitable horizontal and vertical resorption of the alveolar wall from causing a reduction in bone thickness with consequent soft tissue recession.28 Adequate alveolar bone wall thickness of atleast 1mm must be present. (Fig 4b)
Apicocoronal dimension- Lastly, the implant must also be
placed correctly in coronoapical terms. By failing to safeguard peri-implant vertical biologic width, an excessively apical position will lead to vertical bone resorption, which inevitably causes circumferential soft tissue recession.37-39(Fig 4c)
Choice of implant type and characteristics
A correct choice of implant diameter is essential because an excessively large platform may reduce the quantity of peri-implant bone. It is therefore advisable to opt, whenever possible, for the smallest-diameter implant that will not compromise the biomechanical requirements of the tooth being replaced and is appropriate to the patient’s risk profile. In order to reduce the risk of the abutment screw loosening, which is particularly high with single implants, an internal connection system is preferable. Another important consideration is the macroscopic morphology of the endosseous implant. Suitable screw shape contributes to good primary stability, which is essential to achieving osteointegration.
Guidelines For Immediate Implant Placement For Multiple
Missing Teeth Mauro merlialso put forth certain principal
factors to be considered during immediate implant placement for multiple missing teeth:25
Implant positioning
Number and distribution of implants.
Implant positioning
Multiple missing teeth require the same accuracy in positioning implants in the alveolar bone buccopalatally, mesiodistally and apicocoronally (known as 3D placement)40It is additionally important to take into consideration the angle and interproximal bone peak between two adjacent implants.25
The same consideration applies here as those made during buccopalatal and apicocoronal positioning for single missing tooth
Apicocoronal Dimension 25- If implant is positioned too
apically, vertical bone resorption and most likely soft tissue recession will result. 37-39It should be clarified, however, that in the event of multiple missing teeth, a further factor to consider regarding positioning is relationship between the different apicocoronal positions of each implant (Fig 5f, 5g
)
Mesiodistal dimension-Several authors clearly highlighted the
need to safeguard horizontal biologic width (approximately 1.3mm) around the implant.33,41,42 Therefore, if minimum recommended distance between implant and tooth in a mesiodistal direction is 1.5mm, the distance between two adjacent implants should never be less than 3 mm (Fig 5A Fig5b) because a lesser distance will probably impede formation of an adequately supported interimplant papilla of satisfactory height.40
Buccopalatal dimension-The implant must be provided with
adequate buccal bone thickness to ensure that the inevitable horizontal and vertical resorption of the buccal alveolar wall does not cause a reduction in bone thickness and consequent soft tissue recession.29(Fig 5C Fig 5D)
Courtesy: Mauro merli. Implant therapy- The integrated treatment plan; Volume 1;Diagnosis and treatment plan.
Correct preplaned angulation will help to further reduce differences in bone level between implants, avoid unfavourable positioning in relation to anatomical structures, and optimize emergence profiles, thereby improving both the esthetic outcome and the ease of hygiene around the prosthetic restoration.
Interproximal bone peak between contiguous implants
When planning the bone peak between contiguous implants, horizontal interimplant distance should be atleast 3mm, while in the vertical dimension the most coronal portion of the bone peak should have a distance of 4 mm (or at the most 5 mm) with respect to the planned prosthetic contact point (Fig 6)
Number and distribution of implants
The correct number and topographic distribution of implants are proportionate to the degree of edentulism and play a key role in achieving a successful functional and esthetic outcome of the implant prosthetic restoration.
With partially edentulous patients, depending on the number and location of missing teeth, the principles to apply when determining correct implant location are:25
If at all possible, avoid contiguous implants in esthetic areas (alternate with a pontic)
Avoid cantilevers (especially in a distal direction)
Follow the key implant position rule; i.e., try to place implants in canine and if possible molar positions.
Place the lowest possible number of implants allowed by biomechanical requirements
The implant prosthetic treatment plan must among other things consider the number and topographic distribution of implants.
Implant Primary Stability
An important clinical factor to ensure osseointegration is primary implant stability; in the case of immediate implants, this is mandatory. There are several methods described to measure this parameter. The most common are insertion torque (N/cm) and resonance frequency analysis (RFA), which can be measured using several devices (Fig 7).10 These measurements may be used as references to determine implant stability using the implant stability quotient (ISQ).
Studies comparing implant stability between delayed and immediately placed implants seem to indicate lower ISQ values in immediately placed implants compared with implants placed in pristine bone.10 Although these differences tend to disappear over time, ISQ values seem to increase progressively during healing over the first few months in immediate implants.10
Implant design may also have an effect in the primary stability
that it is easier to obtain primary stability with rough surfaces, aggressive thread design, and tapered implants.10
Complications and Management of Risk Factors With Immediate Implants
Pre-surgical implant side evaluation- Selecting the most
appropriate angulation of the pilot drills is important. Failure to do so, may result in perforation of alveolar bone plates during drilling.
Prevention of cortical bone lamella- Atraumatic extraction
should be implemented to minimize bone trauma. If insufficient labial bony support is present and implants are placed without additional measures, the survival rates is severely impaired.
Prevention of thermal drilling trauma- Thermal trauma by
overheating when using wide diameter implants can be avoided if the increase of rotation speed at constant rpm is considered. Permanent internal irrigation should be maintained to reduce drilling temperature in the bone and prevent heat necrosis.
Crestal bone-to-implant gap- The use of an implant design
that mimics the shape of a natural tooth root should be considered. Whenever a circumferential defect of more than 1.0 mm exists around the cervical aspect of the implant grafting and the use of barrier membrane is preferred.
Inflammation and purulence- Delayed implant placement is
considered if any purulent exudate is present during the course of surgery. Antibiotic therapy is initiated whenever there is evidence of acute infection.
Primary closure- In cases when an implant design is employed
which does not mimic the anatomic root form, primary closure of the soft tissues is recommended. If primary closure is not achievable, the use of vertical relaxing incisions and/ or horizontal ribboning of the periosteum should be considered.
Temporary restoration post implant placement-The literature
advocates the wearing of a prosthesis not earlier than 2 weeks post-implant placement to prevent early trauma to the gingival site above the implant. The area should be left without pressure during the entire healing period by an appropriate temporary restoration.
Implants and occlusion- Peri-implant bone loss is more
pronounced in implants which are subject to eccentric loads due to lateral protrusive movements. It is essential that the occlusion is adjusted in such a way that the implant is just out of contact with the opposing tooth at a position of lightest occlusal contact and does not bear excessive loads in lateral or protrusive excursions of the mandible. A single implant supported canine guidance should be avoided.
Prosthodontic Complications- Prosthodontic complications
prosthesis. Shallow placement makes esthetic restoration difficult if a minimal amount of gingival tissue is present. Components bringing the prosthesis to a level close to the implant body itself help with this type of problem.
Survival Rate
Several studies43-49 in the literature have shown that the survival rates of implants placed immediately, early, delayed, or late seemed to be similar in the short term and amount to approximately 95%. It is reported that implants with a machined surface have a lower survival outcome than implants with a rough surface.25
CONCLUSION
Current evidence suggests a high success rate of 95% with immediate implant placement when case selection criteria have been well followed. Immediately placed dental implants is a predictable treatment option that depends mainly on; good patient/case selection, following proper surgical technique, achieving good primary stability and maintaining primary stability. Hence immediate dental implant case selection based on sound clinical practice and research can maximize the advantages afforded by immediate implants and minimize treatment failures.
References
1. Othman Shibly, Nishith Patel, Jasim M. Albandar, Ahmad Kutkut. Bone regeneration Around Implants in Periodontally Compromised Patients: A Randomized Clinical Trial of the effect of Immediate Loading. J
periodontal 2010 Dec;81(12): 1743-51
2. Schulte W, HeimkeG. The Tubinger immediate implants. Quintessenz 1976;27:17-23.
3. Schnitman PA, Wohrle PS, Rubenstein JE. Immediate xed interim prostheses supported by two-stage threaded implants: Methodology and results. J Oral
Implantology 1990;16:96-105.
4. Henry P, Rosenberg I. Single-stage surgery for rehabilitation of the edentulous mandible: Preliminary results. Pract Periodontics Aesthet Dent 1994;6:15-22, quiz 24.
5. Schnitman PA, Wohrle PS, Rubenstein JE, DaSilva JD, Wang NH. Ten-year results for Branemark implants immediately loaded with xed prostheses at implant placement. Int J Oral Maxillofac Implants
1997;12: 495-503.
6. 21. Tarnow DP, Emtiaz S, Classi A. Immediate loading of threaded implants at stage 1 surgery in edentulous arches: Ten consecutive case reports with 1- to 5-year data. Int J Oral Maxillofac Implants
1997;12:319-324.
7. Ericsson I, Nilson H, Lindh T, Nilner K, Randow K. Immediate functional loading of Branemark single tooth implants. An 18 months’ clinical pilot follow-up study. Clin Oral Implants Res 2000;11:26-33.
8. Grunder U. Immediate functional loading of immediate implants in edentulous arches: Two-year results. Int J Periodontics Restorative Dent
2001;21:545-551.
9. Devorah-Schwartz Arad, Nathan Gulayev and GavrielChaushu. Immediate versus non-immediate implantation for full arch fixed reconstruction following extraction of all residual teeth. A
Retrospective Comparitive study. J Periodontal vol.71 No. 6 pg no. 923-928 june 2000.
10. Federico Hernandez Alfaro. Controversial issues in implant dentistry.
11. Momen A. AtiehNabeel H. M. Alsabeeha Warwick J. Duncan Rohana K. de Silva Mary P. Cullinan Donald Schwass Alan G. T. Payne Immediate single implant restorations in mandibular molar extraction sockets: a controlled clinical trial. Clin. Oral Impl. Res. 24, 2013, 484–496
12. Charles A. Babbush. Dental Implants-The Art and Science.
13. Adell R, Lekholm U, Rockler B, Branemark PI. A 15year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg
1981;10: 387-416.
14. Chen ST, BeagleJ, JensenSS, ChiapascoM, Drby I. Consensus statements and recommended clinical procedures regarding surgical techniques. Int J Oral
Maxillofac Implants 2009;24(suppl):272-278.
15. Davarpanah M, Szmukler-Moncler S. Immediate loading of dental implants theory and clinical practice. Chicago: quintessence Books,2008.
16. Chen ST, DarbyIB, Reynolds EC. A prospective clinical study of non-submerged immediate implants: clinical outcomes and esthetic results. Clin Oral
Implants Res 2007;18:552-562
17. Amler MH. The time sequence of tissue regeneration in human extraction wounds. Oral Surg Oral Med
Oral Pathol 1967;27: 309-318.
18. Atwood DA. Reduction of residual ridges a major oral disease entity. J Prosthet Dent 1971;26:266-279. 19. Block MS,MercanteDE, LiretteD, MohamedW,
RyserM, CastellonP. Prospective evaluation of immediate and delayed provisional single tooth restorations. J Oral MaxillofacSurg 2009;67(Suppl 11):89-107.
20. Andreasen J O, Petersen J K, Laskin D M. Textbook and color atlas of tooth impactions, diagnosi, treatment. Copenhagen:Munksgaard,1997
21. Canullo L, lurlaro G, lannello G. Double-blind randomized controlled trial study on post-extraction immediately restored implants using the switching platform concept: soft tissue response. Preliminary report. Clin Oral Implants Res 2009;20:414-420. 22. Fugazzotto P A. Treatment options following single
rooted tooth removal: a literature review and proposed hierarchy of treatment selection. J periodontal
2005;76:821-831.
23. Block M, Colour atlas of dental implant surgery,1sted.Philadelphia:WB Saunders,2001.
24. Douglass GL, Merin R L. The immediate dental implant. J Calif Dent Assoc 2002;30:362-365,8-74.
25. Mauro merli. Implant therapy – the integrated treatment plant; volume 1; Diagnosis and surgical therapy
26. Kois JC. Altering gimgival levels: The restorative connection. I. Biologic variables. J EsthetRestor Dent
1994;6:3-7.
28. BuserD, von Arx T. Surgical procedure in partially edentulous patients with ITI implants. Clin Oral
Implants Res 2000;11 (suppl 1):83-100.
29. Buser D, M artin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla Anatomic and surgical considerations. Int J Oral
Maxillofac Implants 2004;19(suppl):43-61
30. Belser U, BuserD, Higginbottom F. Consensus statements and recommended clinical procedures regarding esthetics in implant dentistry. Int J Oral
Maxillofac Implants 2004;19(suppl):S73 S74
31. Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-inter-implant bone crest. J Periodontol 2000;71:546-549.
32. Tarnow D, Elian N, Fletcher P et al. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J
Periodontol 2003;74:1785-1788.
33. Scarano A, Assenza B, Piattelli M et al. Interimplant distance and crestal bone resorption: A histologic study in the canine mandible. Clin Implant Dent Relat Res 2004;6:150-156.
34. Esposito M, Ekestubbe A, Grondahl K. Radiological evaluation of marginal bone loss at tooth surfaces facing single Branemark implants. Clin Oral Implants Res 1993;4:151-157.
35. Thilander B, Odman J, Jemt T. Single implants in the upper incisor region and their relationship to the adjacent teeth. An 8 year follow-up study. Clin Oral
Implants Res 1999;10:346-355.
36. Krennmair G, Piehslinger E, Wagner H. Status of teeth adjacent to single-tooth implants. Int J Prosthodont
2003;16:524-528.
37. Hermann JS, Conchran DL, Nummikoski PV, Buser D. Crestal bone changes around titanium implants. A radiographic evaluation of unloaded nonsubmerged and submerged implants in the canine mandible. J
Periodontol 1997;68:1117-1130.
38. Hermann JS, Buser D, Schenk RK, Cochran DL. Crestal bone changes around titanium implants. A histometric evaluation of unloaded unsubmerged and submergedimplants in the canine mandible. J
Periodontol 2000;71:1414-1424.
39. Piattelli A,Vrespa G, Petrone G, Lezzi G, Annibali S, Scarano A. Role of the microgap between implant and abutment . A retrospective histologic evaluation in monkeys. J Periodontol 2003; 74:346-352.
40. Grunder U, Gracis S, Capelli M. Influence of the 3D bone to implant relationship on esthetics. Int J
Periodontics Restorative Dent 2005;25:113-119.
41. Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-inter-implant bone crest. J Periodontol 2000;71:546-549.
42. Tarnow D, Elian N, Fletcher P, et al. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J
Periodontol 2003;74:1785-1788.
43. Esposito M, Grusovin MG, Willings M, Coulthard P, Worthington HV. The effectiveness of immediate, early, and conventional loading of dental implants: A Cochrane systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants 2007;22: 893-904.
44. Botticelli D, Renzi A, Lindhe J, Berglundh T. Implants in fresh extraction sockets: A prospective 5-year followupclinicalstudy. Clin Oral Implants Res
2008;19:12261232.
45. Donati M, La Scala V, Billi M, Di Dino B, Torrisi P, Berglundh T. Immediate functional loading of implants in single tooth replacement: A prospective clinical multicenter study. Clin Oral Implants Res
2008;19: 740-748.
46. Ostman PO. Immediate/early loading of dental implants. Clinical documentation and presentation of a treatment concept. Periodontol 2000 2008;47:90-112. 47. Avila G, Galindo P, Rios H, Wang HL. Immediate
implant loading: Current status from available literature. Implant Dent 2007;16:235-245.
48. Kim SH, Choi BH, Li J. Peri-implant bone reactions at delayed and immediately loaded implants: An experimental study. Oral Surg Oral Med Oral Pathol
Oral RadiolEndod 2008;105:144-148.
49. Schropp L, Kostopoulos L, Wenzel A. Bone healing following immediate versus delayed placement of titanium implants into extraction sockets: A prospective clinical study. Int J Oral Maxillofac
Implants 2003; 18:189-199.