Utilization of Well-child Care Services for African-American Infants in a
Low-income Community: Results of a Randomized, Controlled
Case Management/Home Visitation Intervention
Mark A. Schuster, MD, PhD*‡; David L. Wood, MD, MPH*§; Naihua Duan, PhD*; Rebecca M. Mazel, MA*; Cathy D. Sherbourne, PhD*; and Neal Halfon, MD, MPH*‡i
ABSTRACT. Objective. To evaluate a case manage-ment/home visitation intervention to improve access to and utilization of well-child care (WCC) visits.
Study Design. Randomized, controlled trial with baseline and follow-up interview surveys. Mothers and infants in the intervention group were assigned to a case manager who made at least four home visits during the infant’s first year of life. In addition, the case managers contacted clients by telephone and mail to see if they had kept their WCC appointments and to follow up on other issues.
Sample and Data Collection. A population-based ran-dom sample of African-American mothers of newborns from South Central Los Angeles: 185 mothers in the intervention group and 180 in the control group com-pleted both interview surveys. The principal outcome variable was number of WCC visits. Additional outcome variables included the child’s type of insurance, the num-ber of months with insurance coverage during the first year of life, age when first enrolled in Medi-Cal, age at the first WCC visit, usual source of WCC, travel time to the usual source of care, whether the child had a regular provider, and whether the child ever needed care but did not get it.
Results. There was little change in the overall distri-bution of number of WCC visits during the first year of life. Comparisons of the cumulative numbers of visits for each possible cutoff showed that children in the inter-vention group were more likely than children in the control group to have at least four visits (81% vs 70%). Because this split was identified empirically rather than through an antecedent hypothesis, we conducted a Smir-nov test to account for multiple comparisons. This test showed a reduced level of significance. Other outcome variables did not show significant differences for the control and intervention groups.
Conclusions. In light of the high expense of this in-tervention, our evaluation shows that our moderate-intensity case management and home visitation program is not an effective way to increase the number of WCC visits. Pediatrics 1998;101:999 –1005; access to care, case management, home visitation, utilization, well-child care.
ABBREVIATIONS. WCC, well-child care; WIC, Special Supple-mental Nutrition Program for Women, Infants, and Children; SD, standard deviation; OR, odds ratio; CI, confidence interval.
C
hildren in poor communities typically face barriers that limit their access to medical care in general and to well-child care (WCC) in particular.1–9 These barriers include limited or noinsurance coverage, lack of a regular source of care, and lack of transportation to office visits. One strat-egy that has been considered for improving access to care and utilization of care is the provision of case management services. Case managers typically as-sess client needs, determine how to address their needs, help address them (often by coordinating multiple services), and determine whether the needs have been met.10 –13Case management has been used
with variable success to try to improve access to health care for infants from low-income families,14
drug-exposed infants,10,11 children in foster care,10,11
children with asthma,15 pregnant adolescents and
women,16 –21and adolescent parents.11,18,22
Case management programs use various strategies for reaching clients and learning about their needs. One approach is to incorporate home visitation into the program.23–25Home visits provide the case
man-ager with an opportunity to gain insights into the home life and to determine what services might help the family; home visits also eliminate the need for the client to travel to the case manager’s office. In the mid-1980s, Olds and colleagues26 –30began reporting
impressive results from a study of a prenatal and early childhood intervention in which nurses visited the home an average of nine times during pregnancy and 23 times during the first 2 years of the child’s life. This program improved maternal and child health, reduced rates of subsequent pregnancy, increased employment, and reduced government spending. A recent report of follow-up when the children were 15 years old showed that some of the effects of the intervention persisted.26 The initial success of this
intervention encouraged others to develop home vis-itation programs. These programs have varied in the number of home visits, type of providers visiting the home, services provided in the home, available re-sources, and program goals.14,24,31–36Some of the
pro-grams have been successful, particularly those that have closely followed the intensive Olds model,
From *RAND, Santa Monica, California; ‡the Department of Pediatrics, School of Medicine, andithe School of Public Health, University of Cali-fornia, Los Angeles, California; and §Shriners Hospitals for Children, Tampa, Florida.
Received for publication Jul 31, 1997; accepted Nov 17, 1997.
Reprint requests to (M.A.S.) RAND, 1700 Main St, PO Box 2138, Santa Monica, CA 90407-2138.
whereas some have had little impact on their target populations.
We developed a case management intervention using home visitation to increase access to WCC (and immunizations) during the first year of life. Unlike more intensive home visitation programs, our inter-vention did not seek to transform the home environ-ment or to deliver health care services in the home. Rather, it was designed to bring case managers to the home to facilitate their work with mothers of young children. We evaluated this intervention with a ran-domized, controlled study design in a low-income urban African-American population that we had pre-viously found to have low immunization rates.37We
believed that such an intervention could overcome barriers to access and improve the utilization of WCC services because case managers would help enroll the infants in insurance plans, refer them to health care providers, teach parents why WCC visits are important, remind parents to take their children to WCC visits, and provide support when problems arose. Increasing WCC utilization was intended not only as a goal but also as a means of achieving another goal, which was to increase immunization rates. In this article, we report on the intervention’s impact on utilization of WCC and on other measures related to access to care. We report elsewhere the intervention’s impact on immunization rates.38,39
To enhance effectiveness of case management, we coordinated the intervention with the local Special Supplemental Nutrition Program for Women, In-fants, and Children (WIC) program, and the case managers worked out of WIC offices. We believed the intervention would be more likely to succeed and survive if affiliated with an established and popular program such as WIC.
METHODS Sample
The sample was drawn from birth certificates of African-Amer-ican infants born between February and May 1994 with addresses in 10 postal codes in the Compton Health District in South Central Los Angeles with high concentrations of low-income, African-American children. Every 2 weeks, the Los Angeles County Vital Statistics Branch provided us with names and addresses of all African-American women living in the study area who gave birth. Using a reverse phone directory, we recruited mothers by tele-phone or, if they did not have a tele-phone, in person. Of 606 African-American children born during the study period, 84 were ineligi-ble (ie, adopted, moved without forwarding address, deceased). Among the 522 mothers of eligible children, 419 mothers (80%) agreed to participate. A comparison of participants and nonpar-ticipants on 29 characteristics from the birth certificate showed differences only on insurance coverage and rate of minor compli-cations of labor.
Intervention
Mothers and infants in the intervention group were assigned to a case manager. There were two full-time case managers and one full-time supervisor who served as a part-time case manager. One case manager was replaced several months after the project began. The staff all had bachelor’s or master’s degrees in social sciences, and all had previous experience as case managers. They were African-American women familiar with the study population and with local health services. They received training on WCC sched-ules, immunization practices, and the local child health care system.
The case managers followed a protocol that included: a) an
initial assessment; b) collaboration with the mother in developing case management goals and a case service plan; c) brokerage and coordination of services; d) advocacy with large institutions, pub-lic assistance programs (eg, Medi-Cal, which is California’s Med-icaid program), and physicians’ offices; e) monitoring of health services utilization; and f) follow-up. The case managers sought to identify and help resolve barriers to receipt of WCC and immu-nizations, such as lapses in insurance coverage. They also tried to make sure that mothers understood the WCC visit and immuni-zation schedules and that they scheduled appropriate appoint-ments. The case managers did not have direct access to resources such as taxi vouchers; instead, they tried to help mothers gain access to existing resources in the community.
The protocol included four home visits during the infant’s first year of life. The first home visit included an in-depth assessment and occurred at an average infant age of 35.8 days [standard deviation (SD), 10.6; range, 16 to 81 days]. The subsequent three visits were scheduled for 2 weeks before the next WCC visit at which immunizations were due (typically 2 weeks before the 4-, 6-, and 12-month visits). In addition, the case managers contacted mothers by telephone and mail to see if they had kept their WCC appointments and to follow up on other issues. The mean number of completed home visits (excluding visits when the mother was not home) was 4.0 (SD, 1.9; range, 0 to 13 visits) and the mean number of completed telephone contacts was 7.5 (SD, 3.9; range, 0 to 20).
Both the control and intervention groups received a California State pregnancy and parenting booklet that provides information on various aspects of being a new parent, including recommended schedules for WCC visits and immunizations.
Evaluation
Trained RAND interviewers administered a baseline survey in the home before the intervention began and an exit survey after the intervention was complete. The average age of the infant at the time of the baseline interview was 17.7 days (SD, 8.3; range, 5 to 42 days), and the average age at the exit interview was 15.3 months (SD, 1.0; range, 13.9 to 18.2 months).
RAND staff randomized unidentified mother-infant pairs to intervention or control in blocks of four (ABBA, ABAB, etc). After the baseline interview was complete, the interviewer learned the result of randomization and revealed it to the mother: 209 were randomized to the intervention group and 210 to the control group. Among mothers randomized to the intervention, 32 (15.4%) declined the case management services. However, all but 3 of the 32 completed the exit interview survey; they also received the pregnancy and parenting booklet and a phone call at 3 months to confirm the recontact information for the exit survey. Analyses of the intervention group included these nonparticipants, because omitting them would limit comparability to the control group and because our goal was to determine the impact on a population for which case management services are made available. Baseline and exit surveys were completed by 185 mothers in the intervention group and by 180 in the control group.
Mothers provided informed consent to participate in the study. The study was approved by RAND’s Human Subjects Protection Committee.
Dependent Variables
The principal outcome variable for this study is the number of WCC visits, which is a measure of utilization. Utilization is con-sidered a measure of realized access to care;2this definition is
particularly relevant for utilization of WCC services because they are recommended for all children independent of health or other characteristics. In California, WCC visits for most children in low-income families are paid for by the Child Health and Devel-opment Program, which follows the American Academy of Pedi-atrics’ recommendation for six WCC visits during the first year of life: at 2 weeks and 2, 4, 6, 9, and 12 months.40Therefore, we report
the number of WCC visits during the first year of life capped at six or more.
coverage during the first year of life, the child’s age when first enrolled in Medi-Cal (if ever enrolled), the child’s age at the first WCC visit, whether the child had a particular provider he/she usually saw for medical care, the length of time it took to get to the usual source of care (,15 minutes,,30 minutes), and whether the child ever needed care but did not get it.
Independent Variables
We use independent variables that we believed might be re-lated to use of WCC services. Maternal characteristics include age at birth of the child, years of formal education, employment dur-ing the year before the child’s birth, marital status at the baseline interview, cohabitation status at baseline (living with a spouse or partner), and number of living children (including the newborn). These characteristics are included in the Anderson and Aday model of access to health care.2
Low birth weight is used as a marker of health status and is defined as#5.5 pounds.
An adequacy of prenatal care utilization index is used as a marker for the mother’s predisposition to seek preventive care for her child. It divides prenatal care into four ranked categories: 1) inadequate, 2) intermediate, 3) adequate, and 4) adequate plus.41
A life-difficulties index serves as an indicator of household financial distress. The mothers reported whether they or others in the household had done any of the following during the prior 12 months because of problems with money or employment: sold or pawned belongings or property, borrowed or used more credit than they wanted to, skipped a meal or could not buy food, put off going to the doctor, fell behind in paying bills, lost their home or were evicted, had their phone disconnected, or lost welfare or food stamps.
Analysis Methods
For descriptive analyses with dichotomous and nominal vari-ables, we used significance tests based on Pearson’sx2statistics.
For continuous variables, we used a two-samplettest. WhereP
values are not specified, aPvalue of .05 was used as the cut-off for statistical significance. All tests were two-tailed.
We used the Smirnov test to compare the distributions of WCC visits between the intervention and control groups.42,43This test
compares the empirical distribution functions for the two groups and uses the maximum difference between the two functions as the test statistics. The test rejects the null hypothesis that the two distributions are the same if the maximum difference exceeds a threshold value. Because the underlying distributions are discrete, we used Monte Carlo integration to obtain the threshold value and
Pvalues for the test as it is applied to our data.
To confirm findings from the descriptive analyses, we con-ducted logistic regressions with the dichotomous outcome vari-able: zero to three visits versus four or more visits. (We used this derived variable because, as shown in the results section, there seemed to be a shift from zero to three visits to four or more visits for the intervention group compared with the control group.) We first conducted these analyses with the intervention versus control group as the sole predictor variable, without controlling for any covariates. This analysis is justified by randomization of the vention assignment, which guarantees that, on average, the inter-vention and control groups are balanced with respect to covari-ates. However, some imbalance could remain because of random fluctuations in the intervention assignment, so we conducted a sensitivity analysis to verify that the estimated intervention effect is not sensitive to the possible imbalance between the intervention and control groups. Specifically, we expanded the logistic regres-sion model to control for important covariates (described above in the independent variables section) that we hypothesized might relate to use of WCC services. Finally, we added mediating vari-ables that described whether mothers had obtained help with gaining access to care for their children.
RESULTS Demographic and Other Characteristics
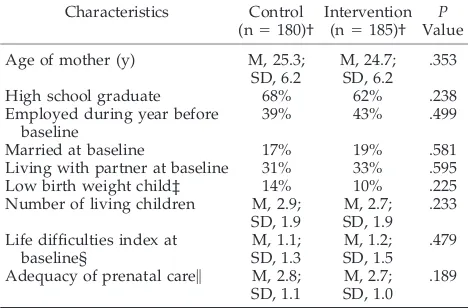
The intervention and control groups showed no significant differences for demographic and other variables, suggesting that randomization was suc-cessful in balancing the two groups (Table 1). For the
sample as a whole, the average age of mothers at the child’s birth was 25.0 years. These mothers had an average of 2.5 living children, including the new-born. Sixty-five percent of mothers were high school graduates. When the study began, 34% were living with a partner, including 18% who were married.
WCC Visits
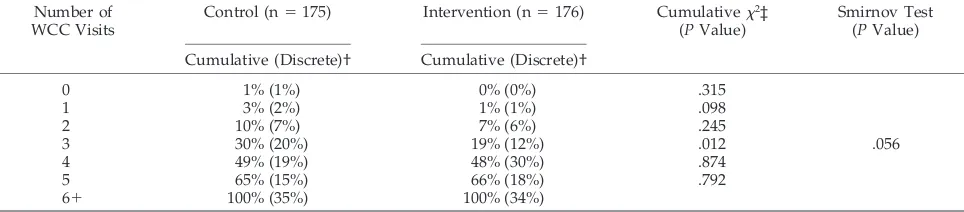
The mean number of WCC visits for the interven-tion and control groups was 4.6 (SD, 1.3) vs 4.4 (SD, 1.5;P5.880). The x2for the discrete distribution of
WCC visits for the intervention and control groups (these values are shown in parentheses in Table 2) was not significant (P5.088). Because there seemed to be a sizable change in the number of children having three versus four visits, we compared cumu-lative numbers of visits (eg, one visit vs two or more visits; one to two visits vs three or more visits, etc). One of these comparisons showed a significant dif-ference at the level of one to three visits versus four or more visits between the intervention (19% vs 81%) and control groups (30% vs 70%) (P5.012) (Table 2). Because this split was identified empirically rather than through an antecedent hypothesis, we con-ducted a Smirnov test to account for multiple com-parisons. This test showed a reduced level of signif-icance withP5.056.
We did not want to miss a possible threshold effect of the intervention between three and four visits, so we conducted a series of logistic regressions with the dichotomous outcome variable: zero to three visits versus four or more visits. There was a positive effect of the intervention [odds ratio (OR), 1.87; confidence interval (CI), 1.14 to 3.07;P5 .014] when it was the sole predictor variable. The addition of demographic variables and other characteristics potentially related to use of WCC services showed the intervention effect to be fairly robust, with only a small change in its odds-ratio or significance (OR, 1.81; CI, 1.08 to
TABLE 1. Sample Characteristics, by Control and Interven-tion Group*
Characteristics Control
(n5180)†
Intervention (n5185)†
P
Value
Age of mother (y) M, 25.3;
SD, 6.2
M, 24.7; SD, 6.2
.353
High school graduate 68% 62% .238
Employed during year before baseline
39% 43% .499
Married at baseline 17% 19% .581
Living with partner at baseline 31% 33% .595
Low birth weight child‡ 14% 10% .225
Number of living children M, 2.9; SD, 1.9
M, 2.7; SD, 1.9
.233
Life difficulties index at baseline§ M, 1.1; SD, 1.3 M, 1.2; SD, 1.5 .479
Adequacy of prenatal care\ M, 2.8; SD, 1.1
M, 2.7; SD, 1.0
.189
* Abbreviations: M, mean; SD, standard deviation.
† The n for some variables is slightly lower because some respon-dents did not answer all questions.
‡ Low birth weight is defined as less than or equal to 5.5 pounds. § The life-difficulties index is an 8-point index with 1 point for each life difficulty experienced during the prior year.
\The adequacy of prenatal care index divides prenatal care into four ranked categories: 1 5inadequate; 25 intermediate; 35
3.03; P 5 .024). None of the additional predictor variables was significant: whether the child had low birth weight; the mother’s age, completion of high school, employment, cohabitation, number of living children, life difficulties, and adequacy of prenatal care.
Alternative Sources of Assistance
One potential explanation for the intervention hav-ing only a small impact on WCC visits might be that it substituted for assistance that mothers would have obtained from other sources (eg, case managers not affiliated with the intervention, other professionals, family, friends) if there had been no intervention. However, the case management group was signifi-cantly more likely than the control group to have obtained help (from any source) with most of the following: finding a doctor (52% vs 31%, P, .001), finding a doctor for sick care (46% vs 25%,P,.001), getting a doctor’s appointment (35% vs 23%, P 5 .009), getting to the doctor’s office (44% vs 35%,P5 .086), getting treatment for a child’s health problems (39% vs 28%, P 5 .024), getting information about insurance (48% vs 32%,P5.002), and getting infor-mation about when to go for check-ups or immuni-zations (60% vs 38%,P ,.001).
We included these examples of help in the logistic regression with the multiple predictors described above. None was significant, and there was little change in the intervention effect (OR, 1.88; CI, 1.10 to 3.24;P5.022), indicating that the effect of the inter-vention was independent of these alternative sources of assistance.
Problems Addressed by Case Managers
The largest category of problems addressed by case managers covered issues related to WIC and food. Twenty-three percent of mothers raised these issues at least once, and most of them wanted help obtaining formula. Other categories that applied to at least 5% of mothers included: help with WCC pay-ments (14%), difficulty with transportation (10%), lack of insurance (8%), other social service needs (6%), issues related to the immunization schedule (6%), family problems (5%), and issues with the in-fant’s WCC provider (5%).
Additional Measures of Access
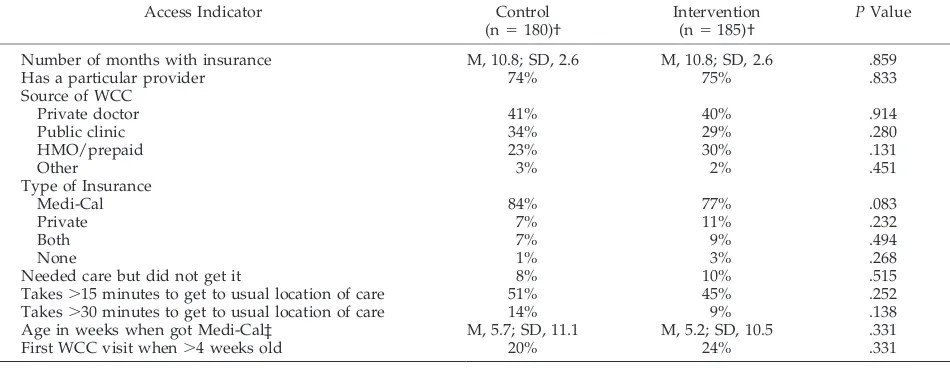
Comparisons of the intervention and control groups were not statistically significant for addi-tional measures of access: type of insurance, months of insurance coverage, usual source of WCC, identi-fication of a regular health care provider, age at Medi-Cal enrollment (if ever enrolled), length of time to go from home to usual location of care, not ob-taining needed care, and having the first WCC visit after the child reached 4 weeks old (Table 3).
Cost of the Intervention
The total cost of the intervention (not including costs associated with evaluating the intervention or studying the control group) was $238 662, or an av-erage of $1587 per participant.
DISCUSSION
This moderate-intensity case management inter-vention had a small impact on utilization of WCC during the first year of life. It was associated with moving a group of children who would have re-ceived zero to three WCC visits into the four or more visits category; however, the evidence supporting the statistical significance of this change is not strong. Given the intensity and cost of the intervention, we had hoped for a larger and more definitive effect.
As with any randomized, controlled intervention, we must consider the possibility that participation in the control group improved the outcome variable, in this case, utilization of WCC services. Both the con-trol group and the intervention group received a California State pregnancy and parenting booklet that covered the recommended timing of WCC visits, and they received the baseline survey, which in-cluded items on WCC. The control group also re-ceived a tracking phone call at 3 months, which could have reminded mothers that they were being observed. It seems unlikely that any of these could have had as much influence as the case management intervention. Because our analyses are based on self-report data, there may be inaccuracies in mothers’ reports of the number of WCC visits or other vari-ables. If there are such inaccuracies, we think they consist of mothers in the intervention group being more likely than mothers in the control group to
TABLE 2. Percentage of Children Who Received No More Than the Specified Number of Well-child Care Visits (Cumulative) and the Percentage Who Received the Exact Number of Well-child Care Visits (Discrete) by Control and Intervention Groups*
Number of WCC Visits
Control (n5175) Intervention (n5176) Cumulativex2‡
(PValue)
Smirnov Test (PValue) Cumulative (Discrete)† Cumulative (Discrete)†
0 1% (1%) 0% (0%) .315
1 3% (2%) 1% (1%) .098
2 10% (7%) 7% (6%) .245
3 30% (20%) 19% (12%) .012 .056
4 49% (19%) 48% (30%) .874
5 65% (15%) 66% (18%) .792
61 100% (35%) 100% (34%)
* Abbreviation: WCC, well child care.
† Discrete refers to the percentage of children who had the exact number of visits listed for that row. Cumulative refers to the percentage of children who had equal to or fewer than the number of visits listed for that row.
overreport the number of WCC visits. Correction of such a bias would reinforce the conclusion that the intervention had had limited impact on the number of WCC visits.
Even though the intervention had little impact on utilization of WCC visits, it was associated with a 13 percentage point increase in the immunization rate at 12 months, which was reported in an earlier article.38
We had expected that a major route for increasing immunization rates would be through an increase in WCC visits. However, there are other ways that a new program might improve immunization rates, such as by improving the spacing of visits or by teaching parents about the importance of vaccina-tion. Using the immunization rates reported in the earlier article38and the distribution of WCC visits for
the case management and control groups reported in this article, we calculated that only 1 percentage point of the 13 percentage point increase was attrib-utable to the shift in category of WCC visits (from zero to three visits to four or more), and the rest was attributable to a change in immunization rates within visit categories. This result may indicate that case managers were more effective at providing educa-tion about the need for immunizaeduca-tions and at getting children immunized when they went for WCC visits than in increasing the number of visits they had.
Some reasons for low utilization may not have been under the control of case managers. Anderson, Aday, and colleagues2,44,45 have shown that
popula-tion characteristics (eg, household composipopula-tion) as well as health system characteristics (eg, source of care) influence access to care. We did not expect case managers to influence population characteristics, but we had thought they would have more influence on structural aspects of the health care system, such as whether children had a regular provider and where they received health care. One might have expected that case management would be effective at helping eligible mothers enroll their children in Medicaid. However, even without assistance from our case managers, almost all children in the control group
had health insurance, so there may have been little need in this population for additional help in obtain-ing Medicaid.
In this intervention, case managers had specific goals but only general resources to achieve them. They tried to improve WCC (and immunization) rates by teaching mothers about the importance of these services and then reminding and persuading mothers to obtain them for their children. In addi-tion, the case managers provided general support and did some troubleshooting by making phone calls and referrals. However, the case managers had no access to specific services related to their goals. For example, they were not affiliated with a mobile van that could bring WCC to the home; they were not operating out of a clinic that was trying to increase its patient base.
Case managers may be more effective when they have resources to use in overcoming specific barriers, when they are helping people gain access to under-utilized programs and entitlements, or when they are closely associated with the provision of the service that is needed. This may be why the most frequent reason mothers sought help from our case managers was to obtain infant formula. Even though improved nutrition was not a specific goal of the intervention, the case managers were located at WIC, and provi-sion of formula was one of the few concrete services they could offer. Our study may indicate that with-out resources greater than their own energy and enthusiasm, case managers will have only a limited impact on utilization of health services.
The home visitation component of the study might have provided more dramatic benefit in an interven-tion with different goals. In this study, the home visit provided a convenient place to meet, it gave the case manager a general sense of the home functioning of the family, and it may have conveyed to the mothers that the case managers considered WCC and immu-nizations important enough to visit the home. How-ever, there were few times when meeting in the home provided insights that helped the case
manag-TABLE 3. Indicators of Access, by Control and Intervention Groups*
Access Indicator Control
(n5180)†
Intervention (n5185)†
PValue
Number of months with insurance M, 10.8; SD, 2.6 M, 10.8; SD, 2.6 .859
Has a particular provider 74% 75% .833
Source of WCC
Private doctor 41% 40% .914
Public clinic 34% 29% .280
HMO/prepaid 23% 30% .131
Other 3% 2% .451
Type of Insurance
Medi-Cal 84% 77% .083
Private 7% 11% .232
Both 7% 9% .494
None 1% 3% .268
Needed care but did not get it 8% 10% .515
Takes.15 minutes to get to usual location of care 51% 45% .252
Takes.30 minutes to get to usual location of care 14% 9% .138
Age in weeks when got Medi-Cal‡ M, 5.7; SD, 11.1 M, 5.2; SD, 10.5 .331
First WCC visit when.4 weeks old 20% 24% .331
* Abbreviations: WCC, well child care; M, mean; SD, standard deviation.
ers achieve their specific goals. Home visitation may be more appropriate and effective when it is focused on the living environment, in other words, when the intervention is related to what the case manager may find in the home environment or to a service that is best provided there. For example, clinical-based an-ticipatory guidance about injury prevention might be enhanced if home visitors inspected the home for injury risks and showed parents how to child-proof it.27 Olds and Kitzman24 have concluded that home
visitation interventions are most likely to be success-ful if they are comprehensive, have frequent visits (more than the average number in our intervention), are staffed by trained professionals, and serve higher-risk families.
Our study must be considered along with similar case management and home visitation interven-tions,14,24,26 –36 many of which have also had mixed
results in achieving desired outcomes. A few studies have looked specifically at WCC visits as an outcome variable. One study of home visitation for African-American mothers found small differences in WCC visits among the intervention and control groups, but higher immunization rates among the former.32
Another intervention achieved only a small increase in WCC visits and concluded that “home visits may not be the most appropriate outreach method when the sole purpose of the outreach is to encourage parents to seek well-child screenings.”36 A third
study in which a public health nurse made the home visits found an increase in visits but little change in immunization rates.14
In the context of these prior studies, our study indicates that one must be cautious in advocating our type of case management as a means of improving utilization of WCC services. This is not to say that case management or home visitation is not a useful means of improving specific outcomes, particularly when it is provided in a more intensive manner than our program (eg, Olds et al26). But our intervention
does not seem to be a very effective approach for improving such a general outcome as WCC visits for a population whose major risk factor for inadequate visits is living in a low-income community. Given the high expense of the intervention, it is difficult to recommend it for purposes of increasing access to and utilization of WCC.
ACKNOWLEDGMENTS
This study was supported by the Centers for Disease Control and Prevention, Atlanta, GA.
We are indebted to the mothers who participated in this study and to the staff of REI-WIC who assisted with it; to Ronald M. Anderson, PhD, and Robert E. Merrill, MD, for comments on a draft of this article; and to Reena S. Kaul, MPH, and Yuko Sano, AB, for research assistance.
REFERENCES
1. Cornelius LJ. Barriers to medical care for White, Black, and Hispanic American children.J Natl Med Assoc.1993;85:281–288
2. Halfon N, Inkelas M, Wood D. Nonfinancial barriers to care for children and youth.Annu Rev Public Health. 1995;16:447– 472
3. Halfon N, Newacheck PW. Childhood asthma and poverty: differential impacts and utilization of health services.Pediatrics. 1993;91:56 – 61 4. Newacheck PW, Halfon N. Preventive care use by school-aged children:
differences by socioeconomic status.Pediatrics. 1988;82:462– 468
5. Rioportella-Muller R, Selby-Harrington ML, Richardson LA, Donat PLN, Luchok KJ, Quade D. Barriers to the use of preventive health care services for children.Public Health Rep. 1996;111:71–77
6. Short PF, Lefkowitz DC. Encouraging preventive services for low-income children: the effect of expanding Medicaid.Med Care. 1992;30: 766 –780
7. St Peter RF, Newacheck PW, Halfon N. Access to care for poor children: separate and unequal?JAMA.1992;267:2760 –2764
8. Wood DL, Hayward RA, Corey CR, Freeman HE, Shapiro MF. Access to medical care for children and adolescents in the United States. Pediat-rics. 1990;86:666 – 673
9. Guendelman S, Schwalbe J. Medical care utilization by Hispanic children: how does it differ from Black and White peers?Med Care.
1986;24:925–940
10. Berkowitz G, Halfon N, Klee L. Improving access to health care: case management for vulnerable children.Soc Work Health Care. 1992;17: 101–123
11. Halfon N, Berkowitz G, Klee L. Development of an integrated case management program for vulnerable children.Child Welfare.1993;72: 379 –396
12. Moore ST. A social work practice model of case management: the case management grid.Soc Work.1990;35:444 – 448
13. Netting FE, Williams FG, Jones-McClintic S, Warrick L. Policies to enhance coordination in hospital-based case management programs.
Health Soc Work.1990;15:15–21
14. Erkel EA, Morgan EP, Staples MA, Assey VH, Michel Y. Case manage-ment and preventive services among infants from low-income families.
Public Health Nurs.1994;11:352–360
15. Wissow LS, Warshow M, Box J, Baker D. Case management and quality assurance to improve care of inner-city children with asthma.Am J Dis Child.1988;142:748 –752
16. Buescher PA, Roth MS, Williams D, Goforth CM. An evaluation of the impact of maternity care coordination on Medicaid birth outcomes in North Carolina.Am J Public Health.1991;81:1625–1629
17. Graham AV, Frank SH, Zyzanski SJ, Kitson GC, Reeb KG. A clinical trial to reduce the rate of low birth weight in an inner-city Black population.
Fam Med.1992;24:439 – 446
18. Korenbrot CC, Showstack J, Loomis A, Brindis C. Birth weight out-comes in a teenage pregnancy case management project.J Adolesc Health Care.1989;10:97–104
19. Oakley A, Rajan L, Grant A. Social support and pregnancy outcome.Br J Obstet Gynaecol.1990;97:155–162
20. Piper JM, Mitchel EF, Ray WA. Evaluation of a program for prenatal care case management.Fam Plann Perspect.1996;28:65– 68
21. Spencer B, Thomas H, Morris J. A randomized controlled trial of the provision of a social support service during pregnancy: the South Manchester family worker project.Br J Obstet Gynaecol.1989;96:281–288 22. Brindis C, Barth RP, Loomis AB. Continuous counseling: case manage-ment with teenage parents.J Contemporary Soc Work.1987;68:164 –172 23. Aaronson M. The case manager-home visitor.Child Welfare.1989;68:
339 –346
24. Olds DL, Kitzman H. Review of research on home visiting for pregnant women and parents of young children.Future Child.1993;3:53–92 25. Weiss HB. Home visits: necessary but not sufficient.Future Child.1993;
3:113–128
26. Olds DL, Eckenrode J, Henderson CR, et al. Long-term effects of home visitation on maternal life course and child abuse and neglect: fifteen-year follow-up of a randomized trial.JAMA.1997;278:637– 643 27. Olds DL, Henderson CR Jr, Kitzman H. Does prenatal and infancy
home visitation have enduring effects on qualities of parental caregiving and child health at 25 to 50 months of life?Pediatrics.1994; 93:89 –98
28. Olds DL, Henderson CR Jr, Phelps C, et al. Effect of prenatal and infancy nurse home visitation on government spending. Med Care.
1993;3:1–20
29. Olds DL, Henderson CR Jr, Tatelbaum R, et al. Improving the delivery of prenatal care and outcomes of pregnancy: a randomized trial of nurse home visitation.Pediatrics.1986;77:16 –28
30. Olds DL, Henderson CR Jr, Tatelbaum R, et al. Improving the life-course development of socially-disadvantaged mothers: a randomized trial of nurse home visitation.Am J Public Health.1988;78:1436 –1445 31. Black MM, Dubowitz H, Hutcheson J, Berenson-Howard J, Starr RH Jr.
A randomized clinical trial of home intervention for children with failure to thrive.Pediatrics.1995;95:807– 814
32. Hardy JB, Streett R. Family support and parenting education in the home: an effective extension of clinic-based preventive health care services for poor children.J Pediatr.1989;115:927–931
infancy home visitation by nurses on pregnancy outcomes, childhood injuries, and repeated childbearing: a randomized controlled trial.
JAMA.1997;278:644 – 652
34. Margolis PA, Lannon CM, Stevens R, et al. Linking clinical and public health approaches to improve access to health care for socially disad-vantaged mothers and children.Arch Pediatr Adolesc Med.1996;150: 815– 821
35. McCarton CM, Brooks-Gunn J, Wallace IF, et al. Results at age 8 years of early intervention for low-birth-weight premature infants: the infant health and development program.JAMA.1997;277:126 –132
36. Selby-Harrington M, Sorenson JR, Quade D, Stearns SC, Tesh AS, Donat PLN. Increasing Medicaid child health screenings: the effectiveness of mailed pamphlets, phone calls, and home visits.Am J Public Health.
1995;85:1412–1417
37. Wood D, Donald-Sherbourne C, Halfon N, et al. Factors related to immunization status among inner-city Latino and African-American preschoolers.Pediatrics.1995;96:295–301
38. Wood D, Halfon N, Donald-Sherbourne C, et al. Increasing immuniza-tion rates among inner-city, African-American children: a randomized trial of case management.JAMA.1998;279:29 –34
39. Wood D, Schuster M, Donald-Sherbourne C, Duan N, Mazel R, Halfon N. Reducing missed opportunities to vaccinate during child health visits.Arch Pediatr Adolesc Med.1998;12:238 –243
40. American Academy of Pediatrics, Committee on Psychological Aspects of Child and Family Health.Guidelines for Health Supervision II.Elk Grove Village, IL: American Academy of Pediatrics; 1988
41. Kotelchuck M. An evaluation of the Kessner adequacy of prenatal care index and a proposed adequacy of prenatal care utilization index.Am J Public Health.1994;84:1414 –1420
42. Massey FJ Jr. The distribution of the maximum deviation between two sample cumulative step functions.Ann Math Statistics.1951;22:125–128 43. Smirnov N. On the estimation of the discrepancy between empirical curves of distributions of two independent samples.Bull Math de l’Universite de Moscou.1939;2:Fasc.:2
44. Anderson RM, Aday LA, Lyttle CS, Cornelius LJ, Chen MS.Ambulatory Care and Insurance Coverage in an Era of Constraint.Chicago, IL: Pluribus Press; 1987
DOI: 10.1542/peds.101.6.999
1998;101;999
Pediatrics
Sherbourne and Neal Halfon
Mark A. Schuster, David L. Wood, Naihua Duan, Rebecca M. Mazel, Cathy D.
Management/Home Visitation Intervention
Low-income Community: Results of a Randomized, Controlled Case
Utilization of Well-child Care Services for African-American Infants in a
Services
Updated Information &
http://pediatrics.aappublications.org/content/101/6/999
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/101/6/999#BIBL
This article cites 42 articles, 7 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/home_care_sub
Home Health
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.101.6.999
1998;101;999
Pediatrics
Sherbourne and Neal Halfon
Mark A. Schuster, David L. Wood, Naihua Duan, Rebecca M. Mazel, Cathy D.
Management/Home Visitation Intervention
Low-income Community: Results of a Randomized, Controlled Case
Utilization of Well-child Care Services for African-American Infants in a
http://pediatrics.aappublications.org/content/101/6/999
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.