Combination of the L1 Broad-Spectrum SPF
10PCR Assay and a Novel
E6 High-Risk Multiplex Type-Specific Genotyping PCR Assay
Dirk van Alewijk,aBernhard Kleter,aMaarten Vent,aJean-Marc Delroisse,bMaurits de Koning,aLeen-Jan van Doorn,aWim Quint,a Brigitte Colaub
DDL Diagnostic Laboratory, Rijswijk, The Netherlandsa; GlaxoSmithKline Vaccines, Rixensart, Belgiumb
Human papillomavirus (HPV) epidemiological and vaccine studies require highly sensitive HPV detection and genotyping
sys-tems. To improve HPV detection by PCR, the broad-spectrum L1-based SPF10PCR DNA enzyme immunoassay (DEIA) LiPA
system and a novel E6-based multiplex type-specific system (MPTS123) that uses Luminex xMAP technology were combined
into a new testing algorithm. To evaluate this algorithm, cervical swabs (nⴝ860) and cervical biopsy specimens (nⴝ355) were
tested, with a focus on HPV types detected by the MPTS123 assay (types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, 6, and 11). Among the HPV-positive samples, identifications of individual HPV genotypes were compared. When all MPTS123 targeted
genotypes were considered together, good overall agreement was found ( ⴝ0.801, 95% confidence interval [CI], 0.784 to 0.818)
with identification by SPF10LiPA, but significantly more genotypes (P<0.0001) were identified by the MPTS123 PCR Luminex
assay, especially for HPV types 16, 35, 39, 45, 58, and 59. An alternative type-specific assay was evaluated that is based on detec-tion of a limited number of HPV genotypes by type-specific PCR and a reverse hybridizadetec-tion assay (MPTS12 RHA). This assay showed results similar to those of the expanded MPTS123 Luminex assay. These results confirm the fact that broad-spectrum PCRs are hampered by type competition when multiple HPV genotypes are present in the same sample. Therefore, a testing algo-rithm combining the broad-spectrum PCR and a range of type-specific PCRs can offer a highly accurate method for the analysis of HPV infections and diminish the rate of false-negative results and may be particularly useful for epidemiological and vaccine studies.
T
he development of cervical cancer is associated with persistent human papillomavirus (HPV) infection. HPVs constitute a group of viruses associated with benign and malignant lesions of the cutaneous and mucosal epithelia. So far, more than 150 differ-ent HPV genotypes have been iddiffer-entified, of which more than 50 have been detected in the anogenital area (2). Epidemiologic re-search has classified 18 HPV genotypes as (probably) high risk (HR), based on their association with cervical cancer, i.e., HPV-16, -18, -26, -31, -33, -35, -39, -45, -51, -52, -53, -56, -58, -59, -66, -68, -73, and -82 (5). In contrast, other genotypes (e.g., HPV-6 and -11) are considered low-risk (LR) genotypes, since they are not commonly associated with the development of cervical carci-noma.Diagnosis of HPV infection is based on the detection of HPV genomic DNA in biological specimens by molecular methods, such as liquid hybridization (e.g., the Hybrid Capture assay [Qia-gen]) or PCR (reviewed by Schiffman et al. [18]). Liquid hybrid-ization detects HPV DNA by direct probe hybridhybrid-ization and can distinguish between groups of high-risk and low-risk HPV geno-types, but it only permits the identification of a limited set of individual genotypes (i.e., HPV-16, -18, and -45) (17,20). PCR methods amplify parts of the HPV DNA genome, resulting in high analytical sensitivity and specificity. The degree of genetic hetero-geneity across the HPV genome among different HPV genotypes enables two approaches for effective diagnosis (3). PCR can em-ploy either type-specific (TS) primers (3,25), which detect only individual HPV genotypes, or broad-spectrum primers. which permit simultaneous amplification of a broad spectrum of HPV genotypes (4,7,11–13,21,23). TS PCR assays are very specific but may be hampered by the existence of uncharacterized viral variant
sequences that do not efficiently match the selected TS PCR prim-ers. Broad-spectrum PCR assays are based on the use of primers that target relatively well-conserved genomic sequences, permit-ting the simultaneous amplification of a range of HPV genotypes in a single PCR test (4,6,11). However, since broad-spectrum PCR primers do not have the same sensitivity and specificity for each genotype, the amplification efficiency may differ among in-dividual genotypes. More importantly, the broad-spectrum PCR assays are affected by competition between the different HPV ge-notypes present in the same sample (24). Due to this competition effect, broad-spectrum PCR assays may underestimate the pres-ence of HPV genotypes when they are present at relatively low concentrations in multiple infections. For clinical trials that assess the efficacy and safety of prophylactic HPV vaccines, virological endpoints, such as incidental or persistent HPV infection, are im-portant markers. It is therefore essential to have an established efficient method for HPV detection and also genotyping methods with high analytical sensitivity to detect any HPV infection, even one at low viral load. This aim is clearly different from HPV diag-nosis in a clinical setting, where the sensitivity should be clinically
Received23 October 2012Returned for modification26 November 2012 Accepted24 January 2013
Published ahead of print30 January 2013
Address correspondence to Dirk van Alewijk, [email protected].
Copyright © 2013, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.02831-12
on May 16, 2020 by guest
http://jcm.asm.org/
relevant in order to identify women at risk for development of cervical cancer (10,19).
Previously, we described a testing algorithm that comprised a combination of the broad-spectrum SPF10PCR DNA enzyme
im-munoassay (DEIA) LiPA system (here referred to as the SPF10
system) with type-specific PCR DEIA systems for HPV-16 and HPV-18 (24). In the present study, we evaluated a multiplex type-specific PCR method comprising an expanded set of type-type-specific PCR assays for detection and identification of 16 HPV genotypes. This new system, named MPTS123, comprises 3 different multi-plex PCR assays with type-specific primers for amplification of individual HPV genotypes. The MPTS123 system uses the mi-crobead-based Luminex xMAP technology and an automated, high-throughput readout with the Luminex 100 or 200 IS system (Luminex Corporation, Austin, TX), which permits detection of 14 HR HPV genotypes (i.e., HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) and 2 individual LR HPV genotypes (i.e., HPV-6 and -11). Whereas the SPF10 system identifies HPV
through the L1 region of the viral genome, the MPTS123 system uses type-specific PCR aimed at the E6 region. We also evaluated an alternative assay, based on type-specific PCR and a reverse hybridization assay (RHA). This assay, designated MPTS12 RHA, uses the same multiplex PCR assays as MPTS1 (HPV-18, -31, -33, and -35) and MPTS2 (HPV-16, -45, -52, -58, and -59).
The aim of the present study was to evaluate the multiplex type-specific HPV genotyping system and the added value of the expanded set of type-specific PCR assays when used in a combined testing algorithm together with the broad-spectrum SPF10PCR
DEIA LiPA system for epidemiologic and vaccination studies, which require a highly sensitive HPV identification test for cervi-cal swab and biopsy samples.
MATERIALS AND METHODS
Plasmids.Plasmids containing HPV genomic DNA were used as the
am-plification targets in various experiments for the evaluation of both the MPTS12 RHA and MPTS123 systems (produced by Labo Biomedical Products BV, Rijswijk, The Netherlands). Except for HPV-59, -89, -90, and a variant of HPV-35, all these plasmids contain the complete viral genomic DNA. PCR amplimers derived from HPV plasmid clones were analyzed for the determination of analytical specificity and sensitivity of the MPTS12 RHA and MPTS123 systems. The majority of these plasmids were kindly provided by E.-M. de Villiers, Heidelberg, Germany (HPV-6, -11, -13, -16, -18, -40, -45, -51, and -53), R. Ostrow, Minneapolis, MN (HPV-26), A. Lorincz, Silver Spring, MD (HPV-31, -35, and -56), and T. Matsukura, Tokyo, Japan, (HPV-58, -59, -62, -67, and -69), G. Orth, Paris, France (HPV-30, -33, -34, -39, -42, -52, -54, -55, -66, -68, -70, and -74). Synthetic plasmids containing part of the L1 region were generated by Genscript USA Inc., Piscataway, NJ (HPV-35v, -89, and -90), using reference HPV sequences from GenBank. Serial (10-fold) plasmid dilu-tions were prepared in 10 mM Tris-HCl (pH 8.0) in a background of DNA equivalent to 106cells/ml genomic MOLT-4 DNA in order to mimic
cer-vical specimens. To assess specificity, a range of 106to 108copies of
plas-mid per PCR assay mixture was used.
To mimic mixed HPV infections, different amounts of plasmids con-taining different HPV genotype genomes were mixed and tested in relative amounts ranging from 1:1 to 106:1. In absolute amounts, mixtures started
at 50 copies per PCR assay of an HPV plasmid. The other second plasmid mixed in ranged, in 10-fold dilution series, from 50 to 5⫻107copies per
PCR mixture. The series for HPV-11, HPV-35v, and HPV-66 started at 500 copies per PCR mixture. Mixtures were prepared in 10 mM Tris-HCl (pH 8.0) and MOLT-4 DNA. Mixtures were tested as follows. HPV-18 was tested in combination with HPV-31, HPV-33, or HPV-35 (all types
am-plified by PCR mix MPTS1). HPV-16 was tested in combination with HPV-45, HPV-52, HPV-58, or HPV-59 (all types amplified by PCR mix MPTS2). HPV-35v was tested in combination with HPV-6, HPV-11, HPV-39, HPV-51, HPV-56, HPV-66, or HPV-68 (all types amplified by PCR mix MPTS3). Each mixture was subjected to amplification and iden-tification with the MPTS123 system as well as the SPF10system.
Clinical materials.Cervical specimens used in this study were 860
cervical swab samples from the HPV-008 study (NCT00122681), which had been collected in PreservCyt, and 355 formalin-fixed, paraffin-em-bedded biopsy samples from women participating in epidemiological studies (see Heracles and Scale [22]). The studies complied with the Hel-sinki Declaration of 1975, as revised in 1983. Appropriate ethical commit-tee approval and informed consent for additional HPV DNA analyses were obtained. The panel of cervical scrape samples comprised a total of 760 samples initially found positive by SPF10PCR-DEIA and 100 samples
found negative by SPF10PCR-DEIA. DNA was extracted from 200l of
each scrape specimen by using the MagNAPure LC DNA isolation proce-dure (Roche Diagnostics), using the total nucleic acid isolation kit, and DNA was eluted in 100-l volumes.
Total DNA was isolated from biopsy section materials by proteinase K treatment. Three tissue sections of 8m were treated with 250l protei-nase K lysis buffer (1 mg/ml proteiprotei-nase K, 45 mM Tris-HCl, 0.9 mM EDTA, and 0.45% Tween 20; pH 8.0) and incubated at 70°C for 16 to 24 h. Proteinase K was heat inactivated by incubation at 96°C for 10 min. DNA preparations from biopsy specimens were diluted 1/10 in diethyl pyrocar-bonate-treated water before testing by PCR to prevent inhibition.
All PCR assays were performed on aliquots from the same DNA prep-aration, and the amount of DNA input was not quantified; 10l was used for each PCR.
SPF10system.The SPF10HPV DEIA and LiPA25 version 1 are
pro-duced by Labo Biomedical Products, Rijswijk, The Netherlands, and are based on licensed Innogenetics technology (12, 13). The SPF10 PCR
primer set detects a broad spectrum of HPV genotypes by amplification of a small fragment of 65 bp from the L1 region of HPV. Reverse primers contain a biotin label at the 5=end, enabling capture of the reverse strand onto streptavidin-coated microtiter plates. Captured amplimers are de-natured by alkaline treatment, and the captured strand is detected by a defined cocktail of digoxigenin-labeled probes, allowing detection of a broad spectrum of HPV genotypes. This method is designated an HPV DEIA, and the results are an optical density value. The same SPF10
am-plimers were used to identify the HPV genotype by reverse hybridization to the LiPA25 genotyping strip (version 1). This line probe assay contains probes for 25 different HPV genotypes (i.e., HPV types 6, 11, 16, 18, 31, 33, 34, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 66, 68/73, 70, and 74).
MPTS123 PCR Luminex system.The MPTS123 PCR Luminex
sys-tem comprises three type-specific PCRs (designated MPTS1, MPTS2, and MPTS3) that generate small biotinylated amplimers of 55 to 139 bp from the HPV E6 region. MPTS1 targets HPV-18, -31, -33, and -35; MPTS2 targets HPV-16, -45, -52, -58, and -59; MPTS3 targets HPV-6, -11, -35v, -39, -51, -56, -66, and -68. To analyze the PCR products generated by the three multiplex PCR mixes, the system uses the microbead-based Lu-minex xMAP technology and an automated, high-throughput readout by the Luminex 100 or 200 IS system (Luminex Corporation, Austin, TX). Taken together, the MPTS123 system permits detection of 16 HPV geno-types (i.e., HPV-6, -11, -16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, and -68). The assay was performed according to the manufactur-er’s instructions (Labo Biomedical Products BV, Rijswijk, The Nether-lands). Briefly, all three biotinylated MPTS123 PCR products derived from a sample were added in combination to the provided bead mix in one readout reaction. Subsequently, the mixture was heated to denature the double-stranded PCR products to allow subsequent hybridization un-der stringent conditions with the immobilized HPV probes on the beads. After stringent washing, which removed unbound PCR product, the beads were incubated with streptavidin-conjugated R-phycoerythrin
on May 16, 2020 by guest
http://jcm.asm.org/
(SAPE) detection conjugate, which binds to the biotin label attached to the HPV amplimer. After another stringent wash, which removed un-bound SAPE, the readout was performed according to the Luminex in-strument settings. The results are the median fluorescence intensity (MFI) levels per HPV type for each specimen tested. The presence of a signal higher than or equal to 100 MFI (no background subtraction) is consid-ered a positive reaction. All 16 HPV MPTS123 genotypes were identified by a single probe, except for HPV-16 and HPV-35. These two genotypes were identified by two slightly different probes to cover the sequence heterogeneity between the viral variant in the targeted region. For inter-pretation of the test results, no distinction was made between samples positive for HPV type 16 variant (HPV-16v) or HPV-16, and they were both scored as HPV-16 positive. Likewise, no distinction was made be-tween samples positive for HPV type 35 variant (HPV-35v) or HPV-35, and they were both scored as HPV-35 positive.
MPTS12 RHA system. Besides the Luminex bead-based HPV
MPTS123 system, a reverse hybridization-based variant assay named the MPTS12 RHA was evaluated. The MPTS12 RHA system permits detec-tion of 9 HR HPV genotypes (i.e., HPV-16, -18, -31, -33, -35, -45, -52, -58, and -59) and includes 2 sets of multiplex PCRs (MPTS1 and MPTS2). To analyze the PCR products generated by the two multiplex PCR mixes, the system uses a strip-based RHA technology. This system is based on visual interpretation of the strips and does not require a Luminex reader. The PCR products from MPTS1 and MPTS2 that can be genotyped by the MPTS12 RHA system can also be analyzed by the MPTS123 system. How-ever, the third multiplex type-specific PCR (i.e., MPTS3) can only be analyzed by the MPTS123 Luminex system. The assay was performed according to the manufacturer’s instructions (Labo Biomedical Products BV, Rijswijk, The Netherlands).
Sequence analysis.Prior to sequence analysis of the MPTS amplimers
generated by the type-specific primers, amplimers were identified on aga-rose gels. Fragments of the expected amplimer size were cut from the gel, purified, and subjected to sequence analysis as well as MPTS123 Luminex analysis. Bands of an unexpected size were tested individually with the MPTS123 Luminex system only. For sequence analysis, purified am-plimers were treated with USB ExoSAP-IT (Isogen Life Science, De Meern, The Netherlands) to remove unconsumed deoxynucleoside triphosphates and primers. Purified amplimers were directly sequenced according to the manufacturer’s instructions for the BigDye Terminator cycle sequencing kit (Applied Biosystems Europe BV, Bleiswijk, The Netherlands), using forward and reverse primers. The sequence products were subsequently read using an ABI Avant genetic analyzer. The resulting DNA sequences were analyzed with Vector NTI Advance version 9.0 soft-ware and compared with all known HPV types present in the National Center for Biotechnology Information (NCBI) database by utilizing nu-cleotide-nucleotide BLAST (BLASTN) searches (http://www.ncbi.nlm .nih.gov/BLAST/).
Statistic analyses.For mutual comparison of the positivity rates of
the SPF10and MPTS123 systems, the two-tailed McNemar test was
used. The level of agreement was determined using Cohen’s kappa statistics. The level of statistical significance was set at 0.05. All analyses were performed using VassarStats tools (http://www.vassarstats.net/).
RESULTS
Specificity of the MPTS123 PCR Luminex system.The specificity
of the MPTS123 PCR Luminex system was first evaluated with PCR products derived from a panel of cloned HPV genotypes (i.e., HPV-6, -11, -13, -16, -18, -26, -30, -31, -33, -34, -35, -39, -40, -42, -43, -44, -45, -51, -52, -53, -54, -56, -58, -59, -66, -67, -68, -68a, -69, -70, -73, -74, -82IS39, -82MM4, and -85).
To challenge the specificity of the PCR amplification, the plas-mids were used at a high-copy-number input in the PCR, resulting in a high yield of PCR product. All amplimers were analyzed in the Luminex system, and amplimers of the targeted types (for which there were specific probes in the Luminex system) demonstrated
highly specific hybridization, with MFI values between 1,166 and 9,217, while background signals varied between 0 and 9 MFI. None of the untargeted types (for which there are no probes in the Luminex system) yielded an MFI value above the cutoff of 100 MFI (data not shown). These results confirmed the high specific-ity of both detection and identification of HPV genotypes by the MPTS123 assay.
Second, a selected panel of 85 cervical swab specimens that had previously tested positive for a single HPV infection with the SPF10system was analyzed to assess the specificities of the primers
and probes involved in the MPTS123 system. Sequences obtained from MPTS123 amplimers of the expected size were found to contain the expected HPV type, thus confirming the specificity of the MPTS123 PCR primers to be excellent (100%) in single HPV-infected samples.
Sensitivity of the MPTS123 system. The sensitivity of the
MPTS123 system was evaluated on 10-fold serial dilutions of plas-mid clones of HPV types 6, 11, 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68 in a background of human (MOLT-4) DNA. Dilution series were tested in independent runs, generating a total of at least 24 results per dilution. This allowed the calculation of copy number and the 95% detection rate (95% confidence inter-val [CI]). The analytical sensitivity of the MPTS123 system ranged from 1 to 20 copies per PCR assay, except for HPV types 11 and 39, for which the analytical sensitivities (95% CI) were 30 to 40 copies per PCR assay (data not shown).
Use of type-specific PCR assays in combination with a
broad-spectrum SPF10PCR as a HPV testing algorithm.In our previous
study (24), we showed that the combination of the SPF10system
with a TS16- and TS18-PCR DEIA system was more accurate for identification of HPV-16 and -18 infections than the SPF10system
alone. In the present study, we expanded the spectrum of type-specific PCR targets to a total of 16 HPV genotypes.
First, the HPV detection rates by the MPTS123 and SPF10
sys-tems were compared for a series of 860 cervical swab samples. The SPF10PCR DEIA detected a total of 760 HPV-positive samples,
whereas the MPTS123 system detected only 737 HPV-positive samples. This difference can be explained by the fact that SPF10is
a broad-spectrum PCR assay that detects at least 50 different HPV genotypes, whereas the MPTS123 system detects only 16 HPV genotypes.
Subsequently, the MPTS123 and SPF10systems were compared
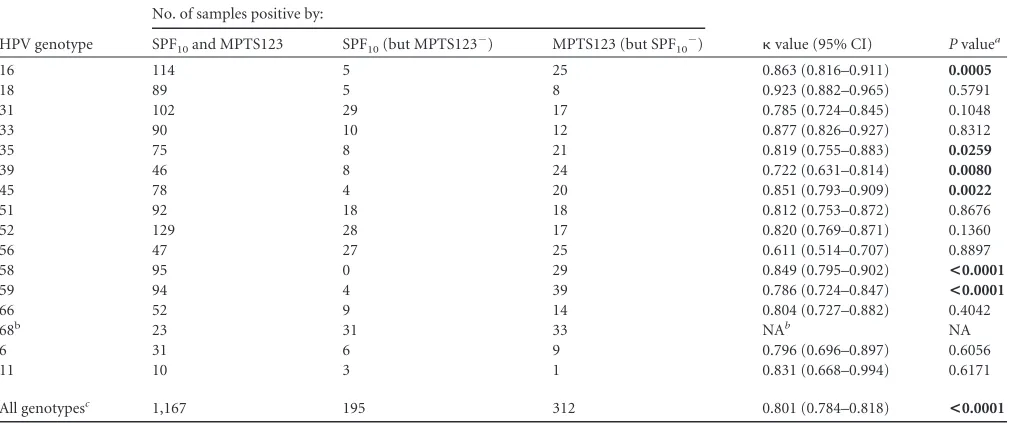
for identifying individual MPTS123 targeted genotypes (i.e., HPV-6, -11, -16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, and -68) in the same clinical (swab) samples (data not shown). In 506 (58.8%) out of 860 samples, both systems yielded genotyping results that were identical (both methods yielded completely identical common genotyping results). Compatible results (i.e., both methods showed one or more of the common genotypes) were found in 292 (34.0%) out of 860 samples. Discor-dant results (i.e., no similarity between the common genotypes detected by the two methods, or a positive versus negative result) were found in 62 (7.2%) out of 860 samples. The individual geno-typing results are shown inTable 1. The MPTS123 and SPF10
systems showed very good overall agreement ( ⫽0.801; 95% CI, 0.784 to 0.818) when all typing results of the MPTS123-targeted genotypes were taken into account. Regarding the 16 HPV geno-types commonly targeted by both systems, a total of 1,167 samples were found positive by both the MPTS123 and SPF10systems ( Ta-ble 1). However, significantly more HPV genotypes (P⬍0.0001)
on May 16, 2020 by guest
http://jcm.asm.org/
were identified by the MPTS123 system than by the SPF10system.
In these samples, the MPTS123 system identified a total of 312 HPV genotype infections that were not detected by the SPF10
sys-tem. Conversely, 195 genotype infections were identified by the SPF10system but remained undetected by the MPTS123 system.
At the individual HPV genotype level (Table 1), the agreement between both systems (kappa values) ranged from 0.611 to 0.923. At this level, a statistically significant difference between the de-tection rates of the MPTS123 and SPF10systems was found for
HPV genotypes 16, 35, 39, 45, 58, and 59, and the MPTS123 sys-tem appeared more sensitive. Further analysis revealed that the majority of these samples contained multiple genotypes (Table 2). Within this specific set of samples, for which the MPTS123 system detected HPV genotypes that were not detected by the SPF10
sys-tem, the proportion of samples containing more than 3 HPV notypes was higher (60.1%) than in samples for which HPV ge-notypes were only detected by the SPF10 system (37.9%). This
indicates that the MPTS123 system higher detection rate in these samples was mainly due to the presence of multiple HPV
geno-types, which is consistent with the hypothesis that broad-spec-trum PCR assays such as the SPF10system are hampered by
com-petition when multiple HPV genotypes are present.
When the broad-spectrum SPF10 system and type-specific
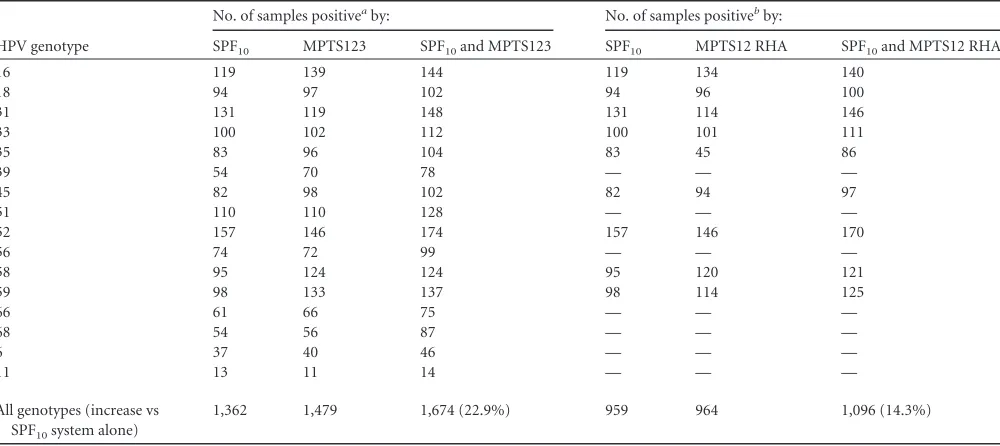
MTPS123 system were combined into a testing algorithm, the overall identification rate of individual HPV genotypes increased. As shown inTable 3, this was observed for all 16 HPV genotypes. For example, the SPF10system identified HPV-16 in 119 samples,
whereas MPTS123 found HPV-16 in 139 samples. When we com-bined the results from both systems, HPV-16 was identified in 144 samples.
Overall, a total of 1362 HPV genotypes were identified by using SPF10alone (Table 3). When MPTS123 results were added, a total
of 1,674 HPV genotypes were detected, which was an increase of 22.9%. Conversely, a total of 1,479 HPV genotypes were found by using the MPTS123 system alone. When SPF10system results were
added, a total of 1,674 HPV genotypes were detected, which was an increase of 11.6%.
[image:4.585.41.551.78.291.2]When we used the MPTS12 RHA assay instead of the MPTS123 TABLE 1HPV type identification by using the SPF10and the MPTS123 systems for 860 swab samples
HPV genotype
No. of samples positive by:
value (95% CI) Pvaluea SPF10and MPTS123 SPF10(but MPTS123⫺) MPTS123 (but SPF10⫺)
16 114 5 25 0.863 (0.816–0.911) 0.0005
18 89 5 8 0.923 (0.882–0.965) 0.5791
31 102 29 17 0.785 (0.724–0.845) 0.1048
33 90 10 12 0.877 (0.826–0.927) 0.8312
35 75 8 21 0.819 (0.755–0.883) 0.0259
39 46 8 24 0.722 (0.631–0.814) 0.0080
45 78 4 20 0.851 (0.793–0.909) 0.0022
51 92 18 18 0.812 (0.753–0.872) 0.8676
52 129 28 17 0.820 (0.769–0.871) 0.1360
56 47 27 25 0.611 (0.514–0.707) 0.8897
58 95 0 29 0.849 (0.795–0.902) <0.0001
59 94 4 39 0.786 (0.724–0.847) <0.0001
66 52 9 14 0.804 (0.727–0.882) 0.4042
68b 23 31 33 NAb NA
6 31 6 9 0.796 (0.696–0.897) 0.6056
11 10 3 1 0.831 (0.668–0.994) 0.6171
All genotypesc 1,167 195 312 0.801 (0.784–0.818) <0.0001
a
Based on McNemar’s test.Pvalues shown in bold are significant (⬍0.05).
bNA, not available because the SPF
10LiPA cannot distinguish between HPV-68 and -73.
c
Restricted to MPTS123-detectable genotypes (i.e., HPV-16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, -68, -6, and -11).
TABLE 2Positive samples among cervical swab specimens that showed significant genotype differences based on the MPTS123 system only or the SPF10system only
HPV genotype
Based on MPTS123 only Based on SPF10only
Total no. of positive samples
No. of HPV genotypes/sample
Total no. of positive samples
No. of HPV genotypes/samplea
1 2 ⱖ3 1 2 ⱖ3
16 25 5 6 14 5 0 3 2
35 21 2 4 15 8 2 4 2
39 24 2 11 11 8 0 4 4
45 20 3 5 12 4 1 1 2
58 29 4 8 17 0 0 0 0
59 39 2 11 26 4 2 1 1
All genotypes (% of total) 158 18 (11.4) 45 (28.5) 95 (60.1) 29 5 (17.2) 13 (44.8) 11 (37.9)
aRestricted to MPTS123-detectable genotypes (i.e., HPV-16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, -68, -6, and -11).
on May 16, 2020 by guest
http://jcm.asm.org/
[image:4.585.42.545.588.715.2]Luminex assay, similar results were obtained (Table 3). When we compared the analytical performance (i.e., specificity and sensi-tivity) of the two systems, the MPTS12 RHA and the MPTS123 system itself showed identical results. Analysis of the same am-plimers for the swab samples described in this study resulted in an overall agreement of 97.1% (data not shown).
Although the MPTS12 RHA only targets 9 HPV genotypes, more HPV genotype were identified with the combination of the SPF10and MPTS12 RHA systems than by either system alone.
Addition of MPTS12 RHA data resulted in a 14.3% increase above that for the SPF10system alone.
When we compared the MPTS12 RHA and MPTS123 Lu-minex systems in combination with the SPF10 system, some dif-ferences were revealed for certain HPV types. As shown inTable 3, significantly more samples were found positive for HPV-35 and -59 with the MPTS123 system. For HPV-35 this difference was expected, because the MPTS123 assay includes an additional probe and primer pair that detect variants of HPV-35. The differ-ence observed for HPV-59 mainly included samples with MFI values in the range of approximately 100 to 1,600 (data not shown). In cases of mutual recognition, higher MFI signals in the range of approximately 500 to 5,500 were found (data not shown). Sequence analysis confirmed that an HPV-59 variant was in-volved, which contained a single mismatch in the probe region for this genotype. This HPV-59 variant is not recognized by the very stringent MPTS12 RHA system. The stringency of the MPTS123 system is slightly lower for HPV-59; it still allows specific detection of the HPV-59 variants but yields relatively lower signals.
In addition to testing of cervical swabs, we also evaluated a series of 355 cervical biopsy samples for the presence of MPTS123-targeted HPV genotypes, using both the MPTS123 and SPF10
sys-tems; results were similar to those obtained for cervical swabs (data not shown). Both systems were compared for individual MPTS123-targeted HPV genotypes identified in the biopsy
spec-imens. In 272 (76.6%) out of 355 samples, both systems yielded genotyping results that were identical. Compatibility was found in 44 samples (12.4%). Discordance (including negative results) was found in 39 samples (11.0%). Individual genotyping revealed very good overall agreement when all typing results were considered together ( ⫽0.890; 95% CI, 0.864 to 0.915), but it did not show significant differences. However, at the individual level, signifi-cant differences were observed for genotypes HPV-16 and -68. For HPV-16, out of 355 biopsy specimens, 97 samples were found positive by both systems, 4 samples were found positive by the SPF10system only, and 18 samples were found positive by the
MPTS123 system only ( ⫽0.846; 95% CI, 0.784 to 0.908;P⫽ 0.005). Further analysis of the 4 samples that were found positive for HPV-16 by the SPF10system only revealed that 3 samples
con-tained a single HPV genotype. Further analysis of the 18 samples that were found positive for HPV-16 by the MPTS123 system only revealed that 17 (94.4%) contained multiple HPV genotypes. For HPV-68, out of 355 biopsy specimens, 2 samples were found pos-itive by both assays, 10 samples were found pospos-itive by the SPF10
system only, and no sample was found positive by the MPTS123 system only ( ⫽0.225; 95% CI,⫺0.177 to 0.688;P⫽0.0077). Because the SPF10system cannot distinguish between HPV-68
and -73 (12), samples found positive by the SPF10system only
were further analyzed using the digene HPV genotyping LQ test (Qiagen, Hilden, Germany), and all samples were all found posi-tive for HPV-73.
DISCUSSION
[image:5.585.43.543.77.300.2]Detection and identification of HPV genotypes in cervical swabs and biopsy specimens strongly depend on the accuracy and the precision of the methods used. Because vaccine trials include sur-rogate virological endpoints, such as incident or persistent infec-tion, to assess the efficacy of candidate (prophylactic) HPV vac-cines, it is crucial that highly reliable and robust testing methods TABLE 3Comparison of HPV genotyping algorithms encompassing the SPF10, MPTS123, and/or MPTS12 RHA systems for 860 swab samples
HPV genotype
No. of samples positiveaby: No. of samples positivebby:
SPF10 MPTS123 SPF10and MPTS123 SPF10 MPTS12 RHA SPF10and MPTS12 RHA
16 119 139 144 119 134 140
18 94 97 102 94 96 100
31 131 119 148 131 114 146
33 100 102 112 100 101 111
35 83 96 104 83 45 86
39 54 70 78 — — —
45 82 98 102 82 94 97
51 110 110 128 — — —
52 157 146 174 157 146 170
56 74 72 99 — — —
58 95 124 124 95 120 121
59 98 133 137 98 114 125
66 61 66 75 — — —
68 54 56 87 — — —
6 37 40 46 — — —
11 13 11 14 — — —
All genotypes (increase vs SPF10system alone)
1,362 1,479 1,674 (22.9%) 959 964 1,096 (14.3%)
a
Restricted to MPTS123-detectable genotypes (i.e., HPV-16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, -68, -6, and -11).
bRestricted to MPTS12 RHA-detectable genotypes (i.e., HPV-16, -18, -31, -33, -35, -45, -52, -58, and -59). —, not applicable because the type is not detected by the MPTS12 RHA
system.
on May 16, 2020 by guest
http://jcm.asm.org/
be used (8). The aim of the present study was to evaluate a novel HPV testing algorithm that contained an L1 broad-spectrum PCR assay (for 25 HPV types) as well as an E6 multiplex type-specific PCR (for 16 HPV types).
In this study, we evaluated two type-specific PCR systems (MPTS12 RHA and MPTS123), separately and in combination with the SPF10system. The MPTS12 RHA system targets 9
high-risk HPV genotypes by two multiplex PCRs followed by reverse hybridization. The MPTS123 system targets 14 high-risk and 2 low-risk HPV genotypes and uses three multiplex PCRs followed by use of the Luminex xMAP technology. Highly equivalent re-sults were obtained for these two type-specific HPV genotyping systems for the commonly targeted genotypes. Both systems can be used to analyze cervical swabs as well as cervical biopsy speci-mens.
The SPF10system permits detection of a very broad range of
HPV genotypes, whereas the type-specific assays specifically am-plify a smaller group of HPV genotypes. Therefore, the overall HPV detection rates of these systems cannot be directly compared. Moreover, the composition of the panel of 860 samples was based on initial results with the SPF10system.
Comparison of the MPTS123 system with the SPF10system for
identification of the commonly targeted HPV genotypes indicated in a high concordance. Overall, 92.8% of the cervical swabs yielded an identical or compatible result. The MPTS123 system identified significantly more samples containing HPV-16, -35, -39, -45, -58, and -59 than did the SPF10system. Similar results
were obtained for biopsy specimens, for which there was high overall agreement (89.0%), but significantly more samples were found positive for HPV-16 by the MPTS123 assay. In contrast, the SPF10PCR LiPA did not identify significantly more positive
sam-ples for any specific genotype.
This effect is mainly caused by a competition effect for the spectrum PCR assay. It is known that for any broad-spectrum PCR assay, competition can occur between multiple HPV genotypes. Consequently, HPV genotypes that are pres-ent at a low concpres-entration can remain undetected, as they are outcompeted by HPV genotypes present at high concentra-tions. This was also shown by the finding that the number of HPV genotypes per sample identified by MPTS123 was higher than that by SPF10 (Table 2). These results show that PCR
competition between the multiple HPV types when using a broad-spectrum PCR-based assay can be circumvented by us-ing a type-specific PCR assay.
In addition to competition, sampling may play a role, espe-cially for samples containing low viral loads. It seems most likely that the false-negative results of the MPTS123 system were due to sampling errors in samples with low viral loads. The sampling effect for biopsy specimens can be substantial, since only a very small part of a cervical biopsy sample is represented in the assay. In general, a biopsy specimen comprises a much smaller part of the cervicovaginal area than a swab.
The third effect that may play a role is the occurrence of variant target sequences. By definition, broad-spectrum PCR assays (such as the SPF10) are aimed at highly conserved primer target
se-quences. The advantage of this approach is that it amplifies a broad range of viral types, and the likelihood that sequence vari-ation (which would lead to false-negative results) occurs at these positions is limited. In contrast, type-specific PCR primers are by definition aimed at sequences that differ between types. This
per-mits highly specific detection and identification of an HPV geno-type. However, additional (and unknown) variation among these target sequences may also cause false-negative results, due to mis-matched PCR primers.
The SPF10system targets the L1 region, while the MPTS123
system is aimed at E6 sequences. Targeting two different parts of the HPV genome can be advantageous and increase the reliability of the testing algorithm. If amplification in one part fails, e.g., due to integration of viral DNA into the host genome, it is likely that the other PCR assay will still be effective. There is no constant disruption site in the viral genome, and the transitions from viral to cellular sequences can be found anywhere from early E1 to the late genes (26).
As described elsewhere (1), the efficacy of PCR amplifica-tion is inversely correlated to the length of the amplimer gen-erated from formaldehyde-fixed paraffin-embedded carci-noma samples. By using type-specific primer pairs, which amplify short fragments of approximately 100 bp or less, effec-tive analysis of formalin-fixed, paraffin-embedded biopsy specimens is possible. Since all PCR products generated by the SPF10and MPTS systems yield very small fragments, these
as-says are optimally suited for analysis of formalin-fixed paraf-fin-embedded biopsy specimens.
Either system can be used as a stand-alone system and allow detection and identification of HPV genotypes. However, com-bining the broad-spectrum and the type-specific PCR assays in one algorithm brings together the advantages of both systems and results in more accurate HPV testing. The SPF10system is an
es-tablished standard for clinical and epidemiologic HPV studies (9,
14–16,27). In earlier studies (24), we showed that complementing the SPF10system with the type-specific PCR DEIA systems for
HPV-16 and HPV-18 resulted in higher HPV detection rates for these types than with the SPF10system alone. In the present study,
we expanded the spectrum of type PCRs to a total of 16 HPV genotypes, and we confirmed that the combination of a broad-spectrum PCR-based assay with a series of type-specific PCRs in one algorithm resulted in a more accurate system to determine HPV type, preventing false-negative results.
Given these observations, it can be concluded that detection of HPV genotypes by combination of broad-spectrum and spe-cific PCR assays provides optimal diagnostic test results. The type-specific PCR can compensate for the competition expected with the broad-spectrum PCR. Conversely, a broad-spectrum PCR can compensate for unknown sequence variation at the target sites of the type-specific primers. Finally, running both assays reduces the sampling error effect of single assays. This was already described in our previous study (24) and was confirmed in the present study, in which we used the expanded set of MPTS123 type-specific PCR assays. Implementation of the MPTS12 RHA or MPTS123 Lu-minex system did not change the concept of the algorithm, but we found differences in the number of different genotypes identified by type-specific PCR only (Fig. 1).
In conclusion, our novel testing algorithm, which combines a broad-spectrum PCR assay and a range of type-specific PCR as-says offers a highly accurate method for the analysis of HPV infec-tions and diminishes the rate of false-negative results. These new levels of precision and reliability of the testing algorithm may al-low for infection endpoints to be used as primary endpoints in clinical studies of prophylactic HPV vaccines for HPV-associated
on May 16, 2020 by guest
http://jcm.asm.org/
cancers for which no other reliable surrogates exist, e.g., head and neck cancers.
ACKNOWLEDGMENTS
GlaxoSmithKline Biologicals, Rixensart, Belgium, funded this study. We thank the HPV-008 and HERACLES/SCALE study groups for their work. We are also grateful to Aurélie Bellanger for the statistical support during the validation of the assay.
B.C. and J.-M.D. are employees of the GlaxoSmithKline group of companies. B.C. owns shares and options to shares in GSK. B.C., L.-J.V.D., and W.Q. are designated inventors on a variety of patents owned by GSK. DDL Diagnostic Laboratory received grants in the frame of a research collaboration with GSK.
REFERENCES
1.Baay MF, Quint WG, Koudstaal J, Hollema H, Duk JM, Burger MP, Stolz E, Herbrink P.1996. Comprehensive study of several general and type-specific primer pairs for detection of human papillomavirus DNA by PCR in paraffin-embedded cervical carcinomas. J. Clin. Microbiol.34: 745–747.
2.Bernard HU, Burk RD, Chen Z, van Doorslaer K, Hausen H, de Villiers EM.2010. Classification of papillomaviruses (PVs) based on 189 PV types and proposal of taxonomic amendments. Virology401:70 –79. 3.Chan SY, Delius H, Halpern AL, Bernard HU.1995. Analysis of genomic
sequences of 95 papillomavirus types: uniting typing, phylogeny, and tax-onomy. J. Virol.69:3074 –3083.
4.de Roda Husman AM, Walboomers JM, van den Brule AJ, Meijer CJ, Snijders PJ.1995. The use of general primers GP5 and GP6 elongated at their 3=ends with adjacent highly conserved sequences improves human papillomavirus detection by PCR. J. Gen. Virol.76:1057–1062. 5.de Sanjose S, Quint WG, Alemany L, Geraets DT, Klaustermeier JE,
Lloveras B, Tous S, Felix A, Bravo LE, Shin HR, Vallejos CS, de Ruiz PA, Lima MA, Guimera N, Clavero O, Alejo M, Llombart-Bosch A, Cheng-Yang C, Tatti SA, Kasamatsu E, Iljazovic E, Odida M, Prado R, Seoud M, Grce M, Usubutun A, Jain A, Suarez GA, Lombardi LE, Banjo A, Menendez C, Domingo EJ, Velasco J, Nessa A, Chichareon SC, Qiao YL, Lerma E, Garland SM, Sasagawa T, Ferrera A, Hammouda D, Mariani L, Pelayo A, Steiner I, Oliva E, Meijer CJ, Al-Jassar WF, Cruz E, Wright TC, Puras A, Llave CL, Tzardi M, Agorastos T,
Garcia-Barriola V, Clavel C, Ordi J, Andujar M, Castellsague X, Sanchez GI, Nowakowski AM, Bornstein J, Munoz N, Bosch FX. 2010. Human papillomavirus genotype attribution in invasive cervical cancer: a retro-spective cross-sectional worldwide study. Lancet Oncol.11:1048 –1056. 6.Gravitt PE, Manos MM.1992. Polymerase chain reaction-based methods
for the detection of human papillomavirus DNA. IARC Sci. Publ.119: 121–133.
7.Gravitt PE, Peyton CL, Apple RJ, Wheeler CM.1998. Genotyping of 27 human papillomavirus types by using L1 consensus PCR products by a single-hybridization, reverse line blot detection method. J. Clin. Micro-biol.36:3020 –3027.
8.Harper DM, Franco EL, Wheeler C, Ferris DG, Jenkins D, Schuind A, Zahaf T, Innis B, Naud P, De Carvalho NS, Roteli-Martins CM, Teixeira J, Blatter MM, Korn AP, Quint W, Dubin G.2004. Efficacy of a bivalent L1 virus-like particle vaccine in prevention of infection with human papillomavirus types 16 and 18 in young women: a randomised controlled trial. Lancet364:1757–1765.
9.Harper DM, Franco EL, Wheeler CM, Moscicki AB, Romanowski B, Roteli-Martins CM, Jenkins D, Schuind A, Costa Clemens SA, Dubin G.
2006. Sustained efficacy up to 4.5 years of a bivalent L1 virus-like particle vaccine against human papillomavirus types 16 and 18: follow-up from a randomised control trial. Lancet367:1247–1255.
10. Hesselink AT, van Ham MA, Heideman DA, Groothuismink ZM, Rozendaal L, Berkhof J, van Kemenade FJ, Massuger LA, Melchers WJ, Meijer CJ, Snijders PJ.2008. Comparison of GP5⫹/6⫹-PCR and SPF10-line blot assays for detection of high-risk human papillomavirus in sam-ples from women with normal cytology results who develop grade 3 cer-vical intraepithelial neoplasia. J. Clin. Microbiol.46:3215–3221. 11. Hildesheim A, Schiffman MH, Gravitt PE, Glass AG, Greer CE, Zhang
T, Scott DR, Rush BB, Lawler P, Sherman ME. 1994. Persistence of type-specific human papillomavirus infection among cytologically nor-mal women. J. Infect. Dis.169:235–240.
12. Kleter B, van Doorn LJ, Schrauwen L, Molijn A, Sastrowijoto S, ter Schegget J, Lindeman J, ter Harmsel B, Burger M, Quint W. 1999. Development and clinical evaluation of a highly sensitive PCR-reverse hybridization line probe assay for detection and identification of anogeni-tal human papillomavirus. J. Clin. Microbiol.37:2508 –2517.
13. Kleter B, van Doorn LJ, ter Schegget J, Schrauwen L, van Krimpen K, Burger M, ter Harmsel B, Quint W.1998. Novel short-fragment PCR assay for highly sensitive broad-spectrum detection of anogenital human papillomaviruses. Am. J. Pathol.153:1731–1739.
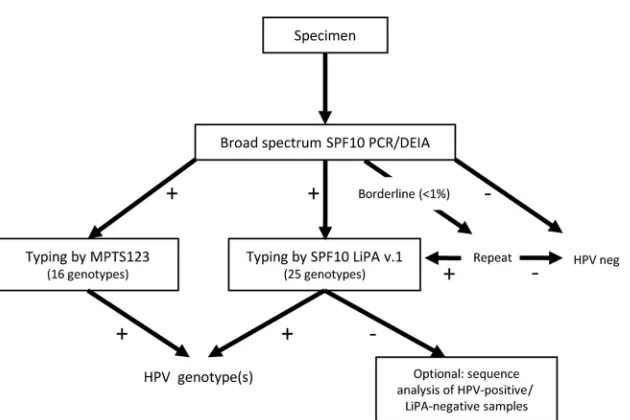
FIG 1Upgraded HPV testing algorithm. DNA was isolated from cervical scrapes by use of the MagNa Pure LC instrument and subjected to SPF10PCR. The PCR
products were analyzed in a DEIA with specific probes. If the SPF10PCR DEIA system yielded a negative result, the sample was considered HPV negative. Samples
with borderline DEIA results were retested. Samples that were borderline after retesting with the SPF10PCR DEIA were also analyzed with the LiPA and the
MPTS123 systems (not shown in this figure). Amplimers from SPF10PCR DEIA-positive samples were tested by LiPA (version 1.0, which contains probes for 25
genotypes) to determine the HPV genotype. All samples positive by the SPF10PCR DEIA system were also tested by the MPTS123 system (or MPTS12 RHA [for
9 genotypes]).
on May 16, 2020 by guest
http://jcm.asm.org/
[image:7.585.138.453.60.270.2]14. Kreimer AR, Gonzalez P, Katki HA, Porras C, Schiffman M, Rodriguez AC, Solomon D, Jimenez S, Schiller JT, Lowy DR, van Doorn LJ, Struijk L, Quint W, Chen S, Wacholder S, Hildesheim A, Herrero R.2011. Efficacy of a bivalent HPV 16/18 vaccine against anal HPV 16/18 infection among young women: a nested analysis within the Costa Rica Vaccine Trial. Lancet Oncol.12:862– 870.
15. Paavonen J, Jenkins D, Bosch FX, Naud P, Salmeron J, Wheeler CM, Chow SN, Apter DL, Kitchener HC, Castellsague X, de Carvalho NS, Skinner SR, Harper DM, Hedrick JA, Jaisamrarn U, Limson GA, Dionne M, Quint W, Spiessens B, Peeters P, Struyf F, Wieting SL, Lehtinen MO, Dubin G.2007. Efficacy of a prophylactic adjuvanted bivalent L1 virus-like-particle vaccine against infection with human pap-illomavirus types 16 and 18 in young women: an interim analysis of a phase III double-blind, randomised controlled trial. Lancet369:2161– 2170.
16. Paavonen J, Naud P, Salmeron J, Wheeler CM, Chow SN, Apter D, Kitchener H, Castellsague X, Teixeira JC, Skinner SR, Hedrick J, Jaisamrarn U, Limson G, Garland S, Szarewski A, Romanowski B, Aoki FY, Schwarz TF, Poppe WA, Bosch FX, Jenkins D, Hardt K, Zahaf T, Descamps D, Struyf F, Lehtinen M, Dubin G.2009. Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): final analysis of a double-blind, randomised study in young women. Lan-cet374:301–314.
17. Perrons C, Jelley R, Kleter B, Quint W, Brink N.2005. Detection of persistent high risk human papillomavirus infections with hybrid capture II and SPF10/LiPA. J. Clin. Virol.32:278 –285.
18. Schiffman M, Wentzensen N, Wacholder S, Kinney W, Gage JC, Castle PE.2011. Human papillomavirus testing in the prevention of cervical cancer. J. Natl. Cancer Inst.103:368 –383.
19. Snijders PJ, van den Brule AJ, Meijer CJ.2003. The clinical relevance of human papillomavirus testing: relationship between analytical and clini-cal sensitivity. J. Pathol.201:1– 6.
20. Thai H, Rangwala S, Gay T, Keating K, McLeod S, Nazarenko I, O’Neil D, Pfister D, Loeffert D.2009. An HPV 16, 18, and 45 genotyping test based on hybrid capture technology. J. Clin. Virol.45(Suppl. 1):S93–S97. 21. Tieben LM, ter Schegget J, Minnaar RP, Bouwes Bavinck JN, Berkhout
RJ, Vermeer BJ, Jebbink MF, Smits HL.1993. Detection of cutaneous and genital HPV types in clinical samples by PCR using consensus prim-ers. J. Virol. Methods42:265–279.
22. Tjalma WA, Fiander A, Reich O, Powell N, Nowakowski AM, Kirschner B, Koiss R, O’Leary J, Joura EA, Rosenlund M, Colau B, Schledermann D, Kukk K, Damaskou V, Repanti M, Vladareanu R, Kolomiets L, Savicheva A, Shipitsyna E, Ordi J, Molijn A, Quint W, Raillard A, Rosillon D, De Souza SC, Jenkins D, Holl K.24 July 2012. Differences in human papillomavirus type distribution in high-grade cervical intraepi-thelial neoplasia and invasive cervical cancer in Europe. Int. J. Cancer
132:854 – 867.
23. van den Brule AJ, Pol R, Fransen-Daalmeijer N, Schouls LM, Meijer CJ, Snijders PJ.2002. GP5⫹/6⫹PCR followed by reverse line blot analysis enables rapid and high-throughput identification of human papillomavi-rus genotypes. J. Clin. Microbiol.40:779 –787.
24. van Doorn LJ, Molijn A, Kleter B, Quint W, Colau B.2006. Highly effective detection of human papillomavirus 16 and 18 DNA by a testing algorithm combining broad-spectrum and type-specific PCR. J. Clin. Mi-crobiol.44:3292–3298.
25. Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA, Shah KV, Snijders PJ, Peto J, Meijer CJ, Munoz N.1999. Human papilloma-virus is a necessary cause of invasive cervical cancer worldwide. J. Pathol.
189:12–19.
26. Wentzensen N, Vinokurova S, von Knebel DM.2004. Systematic review of genomic integration sites of human papillomavirus genomes in epithe-lial dysplasia and invasive cancer of the female lower genital tract. Cancer Res.64:3878 –3884.
27. Wheeler CM, Castellsague X, Garland SM, Szarewski A, Paavonen J, Naud P, Salmeron J, Chow SN, Apter D, Kitchener H, Teixeira JC, Skinner SR, Jaisamrarn U, Limson G, Romanowski B, Aoki FY, Schwarz TF, Poppe WA, Bosch FX, Harper DM, Huh W, Hardt K, Zahaf T, Descamps D, Struyf F, Dubin G, Lehtinen M.2012. Cross-protective efficacy of HPV-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by nonvaccine oncogenic HPV types: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol.13:100 –110.