Incident
Response
Plan
INCIDENT RESPONSE PLAN (IRP)
Version: 2Summary:
The aim of this plan is to provide a framework by which Southern Health NHS Foundation Trust will prepare for and undertake its role in a major incident. This Incident Response Plan details the planning and response of the Trust during a Major Incident.
The Civil Contingencies Act 2004 (CCA 2004) and the NHS England Emergency Preparedness Resilience & Response Guidance (EPRR) 2013 set out the legal and NHS responsibilities that the Trust has a duty to meet.
Keywords (minimum of 5): (To assist policy search engine)
Resilience, Emergency Planning, Business Continuity Policy, Business Continuity Management
Target Audience: All employees of Southern Health NHS Foundation
Trust. Non-Executive Directors, Volunteers, Governors and Contractors.
Next Review Date: 31.01.16
Approved & Ratified by: Emergency Preparedness, Resilience and Response Working Group
Date of meeting: 31st July 2014
Emergency Preparedness, Resilience and Response Working Group
Date of meeting: 26th August 2014
Date issued: 26.08.15
Author: Philip Rudin, Business Continuity & Emergency Preparedness Officer
Sponsor: Julie Jones
Version Control
Change RecordDate Author Version Page Reason for Change
24/01/14 BC Advisor on behalf of Head of Risk and Business Continuity
0.1 Development of new IRP
27/01/14 BC Advisor on behalf of Head of Risk and Business Continuity
0.2 Further development of new IRP
03/14 BCRM 0.3 Further development of new IRP
11/04/14 BCRM 0.4 Further development of new IRP
14/04/14 BCRM 0.5 Further development of new IRP
23/04/14 BCRM 0.6 Further development of new IRP
28/04/14 BCRM 0.7 Further development of new IRP
07/05/14 BCRM 0.8 Further development of new IRP
06.06.14 BCRM 0.9 Additional comments from EPRR WG
15.09.14 BCRM 1.0 Approval and ratification from EPRR
WG
26.08.15 Philip Rudin 2 33,34 Review and update communications cascade
Reviewers/contributors
Name Position Version Reviewed &
Date
Stuart Brown Business Continuity Advisor 1
Tim Pettis Business Continuity & Resilience Manager 1
David Griffiths EPM UHS 1
Tim Pettis BCRM 1
EPRR WG members Various 1
Philip Rudin Business Continuity & Emergency Preparedness Officer
IMMEDIATE ACTION
If you have received
notification that a Major
Incident has been declared
DO NOT READ THIS PLAN
NOW BUT FIND
Your relevant action card
and
Table of CONTENTS PART 1 INCIDENT RESPONSE PLAN
SECTION 1 PLANNING EPRR Responsibilities SECTION 2 ALERTING
Declaration of a Major Incident and Alerting Routes SECTION 3 RESPONSE
Activation of the Plan SECTION 4 RECOVERY Stand Down and Recovery PART 2 ANNEXES Annex A Media Liaison Annex B Vulnerable People Annex C
Mutual Aid Process Annex D
Templates Annex E Data Sharing Annex F
EPRR Guidance Document Annex G
Set up of Incident Co-ordination Centre (ICC) Annex H
Memorandum of Understanding between SHFT and NHS England (Wessex) for reciprocal ICC arrangements
Equality and Diversity
PART 3 SUPPORTING INFORMATION 1. Emergency Planning Cycle
2. Document Management 3. Training
4. Exercises
5. Supporting Documentation 6. Useful Websites
7. Trust Supporting Plans 8. Distribution Lists
INCIDENT RESPONSE PLAN EXECUTIVE SUMMARY
The aim of this plan is to provide a framework by which Southern Health NHS Foundation Trust (SHFT) prepare for and undertake its role in a major incident. This Incident Response Plan (IRP) details the planning and response of the Trust during a Major Incident.
NHS Organisations are responsible for providing health services on behalf of the population they serve. The Trust has the following principle roles in an emergency preparedness and response:
Co-operate with other responding agencies (including Clinical Commissioning Groups) in the business of emergency planning;
Share information for the purposes of emergency preparedness and response; Support the NHS England (Wessex) and (Thames Valley) Area Team in the local
co-ordination of NHS funded health services;
Represent the ‘local NHS’ at a multi-agency Tactical Co-ordinating Group if required; and Share resources as necessary when they are required to respond to a significant incident or
emergency.
The Civil Contingencies Act 2004 (CCA 2004) and the NHS England Emergency Preparedness Resilience & Response Guidance (EPRR) 2013 set out the legal and NHS responsibilities that the Trust has a duty to meet.
All staff and clinicians who work within the Trust may have a role in supporting the response to a major incident. It is, therefore, important that clear plans are made available to ensure the Trust maximises the skill and commitment of all partners in circumstances that will test us all. This plan has been developed with the support of colleagues and it is fundamental to the Trust’s ability to respond to a major incident that everybody is aware of its content and their own responsibilities.
Dr Chris Gordon
Accountable Emergency Officer (AEO) Southern Health NHS Foundation Trust
SECTION 1
PART 1
INCIDENT RESPONSE PLAN
SECTION 1 PLANNING
1.
Emergency Preparedness Resilience & Response (EPRR) Responsibilities
Introduction
1.1 The aim of this Plan is to provide the framework whereby Southern Health NHS Foundation Trust (SHFT) will prepare for, respond to and recover from a major incident, or emergency, regardless of cause. The Plan is divided into 4 parts:
PART 1 - Plan Details PART 2 - Annexes
PART 3 - Supporting Information PART 4 - Action Cards
1.2 The objectives of this Plan are:
To outline SHFT’s responsibilities for emergency preparedness, resilience, response and recovery, and those of specific divisions and staff members;
To define what constitutes a major incident or emergency;
To outline the structures, systems, processes and procedures that are in place to ensure that SHFT, in collaboration with partner agencies, is prepared for, can respond to and recover from major incidents and emergencies;
To outline the roles and responsibilities of key partner organisations; and
To outline the national, regional and local NHS response, and how this dovetails with other multi-agency partners through multi-agency command and control.
1.3 The Civil Contingencies Act 2004 (CCA 2004) and the NHS Commissioning Board Emergency Preparedness, Resilience and Response (EPRR) Guidance documents set out the legal and statutory responsibilities that SHFT has a duty to meet. They are outlined in para. 5.1. 1.4 SHFT has the following key roles in the event of a major incident or emergency:
Maintenance of critical services
Identification of vulnerable people in the community who may be affected by the major incident, and supporting delivery of care to them;
Support to acute hospitals in the early discharge of patients into the community and to community hospitals;
Use of its minor injury and community facilities to support the major incident response; Provision of nursing support to displaced people in conjunction with Local Authorities at
Humanitarian Assistance Centres by advising people with regard to medical problems and linking with local GPs and pharmacies; and
Provision of vaccination or prophylaxis as required mitigating the effects of a major incident relating to public health.
1.5 All SHFT staff may have a role in supporting the response to a major incident. It is therefore important that clear plans are made available to ensure SHFT maximises the skill and
commitment of all staff in circumstances that will test us all. It is therefore fundamental to the Trust’s ability to respond to a major incident that everybody is aware of this policy’s content and their own responsibilities.
1.6 This Plan is available from the SHFT website and staff intranet. Scope
1.7 This plan describes how Southern Health NHS Foundation Trust will meet its statutory responsibilities for major incident preparation, response and recovery and as such applies to all staff in all services and in all Divisions.
Definitions
The following definitions are terms widely used in Emergency Preparedness, Resilience & Response (EPRR) by multi-agency organisations and the NHS:
‘Emergency’:
The Civil Contingencies Act 2004 defines an ‘emergency’ as: ‘An event or situation which threatens serious damage’ to: Human welfare in a place in the UK
The environment of a place in the UK
The security of the UK or of a place in the UK’ ‘Major Incident’:
For the purposes of this plan, a ‘major incident’ is defined as:
‘Any accident, incident, natural disaster or hostile act which demands special arrangements to cope with casualties or to counter actual or potential effects on the provision of services.’
‘Major Incident Standby’:
For the purposes of this plan, a ‘major incident standby’ is defined as:
‘a heightened state of readiness prior to a possible declaration of a major incident by a provider, emergency service or NHS England (Wessex and/or Thames Valley).’
‘Significant Incident’:
NHS England guidance defines a ‘significant incident’ as:
‘Any occurrence that presents serious threat to the health of the community, disruption to the service or causes (or is likely to cause) such numbers or types of casualties as to
require special arrangements to be implemented by hospitals, ambulance trusts or other acute or community provider organisations.’
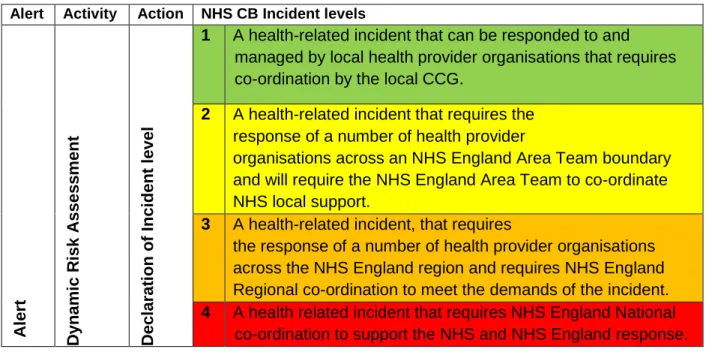
NHS Levels of Response for Incidents
Alert Activity Action NHS CB Incident levels
A lert D yn ami c R isk A ss es s ment D ec larat ion o f Inc ide n t lev el
1 A health-related incident that can be responded to and managed by local health provider organisations that requires co-ordination by the local CCG.
2 A health-related incident that requires the response of a number of health provider
organisations across an NHS England Area Team boundary and will require the NHS England Area Team to co-ordinate NHS local support.
3 A health-related incident, that requires
the response of a number of health provider organisations across the NHS England region and requires NHS England Regional co-ordination to meet the demands of the incident. 4 A health related incident that requires NHS England National
co-ordination to support the NHS and NHS England response. 1.8 Furthermore, the NHS needs to be ready to respond to a variety of risks and threats identified
in the National Risk Register assessment by the Cabinet Office and the Local Resilience Forum Community Risk Registers.
Furthermore, NHS England identifies three levels of response relating to the numbers of casualties from an incident or incidents. Although SHFT is not an acute trust, it is likely that in an incident with large numbers of casualties that the trust will be required to assist under mutual aid. The table below illustrates this into the following general level of casualties:
NHS Level No’s of Casualties
Description Local Response NHS England Response
Major = 10s Individual Trusts handle incident within
established areas
Local NHS activate local Command, Control, Communication and Co-ordination (C4)
arrangements -
participate in local multi-agency arrangements
NHS England and DH (Emergency Preparedness Department) informed
Mass = 100s Large scale Possible closure /evacuation.
Local NHS activate local Command, Control, communication,
NHS England (Wessex) or (Thames Valley) activates C4 Arrangements to
Major health facility or persistent disruption over time Collective mutual aid from neighbours Coordination (C4) Arrangements – participate in local multi-agency arrangements All Trusts link to NHS Command arrangements – NHS South coordinates mutual aid
coordinate health care across region
Consider implementation of revised clinical protocols DH(EPD) notified and available to support NHS England (Wessex) or (Thames Valley) Catastrophic = 1000s Incident of such proportions that it severely disrupts health & social care and other support functions – Response exceeds collective local capacities
Local plans activated – NHS England (Wessex) or (Thames Valley) activates C4 advised and Trusts link to NHS Command arrangements
for coordination and mutual aid
Potential for more than one NHS Area Team region to be affected and each activates own Strategic Command arrangements DH (EPD ) National MI Coordination Centre activated – national co-ord strategic response and mobilisation of mutual aid
1.9 Types of Incident External incidents
Examples of external incidents leading to the activation of SHFT business continuity plans and this Incident Response Plan are:
Large scale accidents – rail, motorway or air;
Slowly emerging incident – an infectious disease such as Pandemic influenza; Toxic gas plume drifting over the area – from a fire at an industrial site;
Headline news report – leading to a health scare and
Deliberate release of a Chemical, Biological, Radiological or Nuclear, explosives (CBRNe) substances.
Internal incidents
Examples of internal incidents are: Loss of facilities due to fire, flood; Loss of ICT support;
Staff illness due to seasonal or pandemic flu; Serious untoward incident;
Denial of access to a Trust site, due safety or security incidents; Supply Chain failure such as fuel, power, water; essential supplies and Loss of key personnel.
This Plan’s associated Business Continuity Policy describes SHFTs Business Continuity Management arrangements and the SHFT Business Continuity Management programme. The Business Continuity Policy requires all services in all divisions to regularly review and update their Business Continuity Plans which make up the Business Continuity Plan for the Trust. However, it should be noted that the same Command and Control arrangements are in place for either a major or business continuity incident.
1.10 Big bang
NHS England explains the definition of a “Big Bang” incident as follows:
‘A health service major incident is classically triggered by a sudden major transport or industrial accident. The ambulance service and receiving hospitals will be the first health responders. What may not be so obvious at first, however, are the wider health
implications. A major incident may also build slowly from a series of smaller incidents such as might occur on a fogbound motorway’.
Big Bang Incidents will in most cases cause significant numbers of casualties or fatalities, and may require large scale evacuation.
In all cases these types of incidents a multi-agency response is required. 1.11 Rising Tide Incidents
NHS England explains a “Rising Tide” incident in the following way:
‘The problem creeps up gradually, such as occurs in a developing infectious disease, epidemic or a winter bed availability crisis. There is no clear starting point for the major incident and the point at which an outbreak becomes ‘major’ may only be clear in retrospect’.
1.12 Cloud on the Horizon Incidents
NHS England explains a “Cloud on the Horizon” incident in the following way:
‘An incident in one place may affect others following the incident. Preparatory action is needed in response to an evolving threat elsewhere, even perhaps overseas, such as a major chemical or nuclear release, a dangerous epidemic or an armed conflict involving British troops. A chemical or radiation incident may literally cause a cloud on the horizon. In a similar way, but on a longer time scale the progress of a ’flu epidemic can be
observed and predicted’. 1.13 Headline News
Headline News incidents may be highly local, and remain so, or have the potential to develop into regional or national interest stories.
Alternately they may start as national or regional stories but develop to have a local impact.
In any event it is essential that the Director of Communications & Media Team are given an immediate briefing to enable them to make a judgement regarding the best course of action.
1.14 Deliberate or Terrorist Incidents
Terrorist-related incidents require a specialist response from trained and properly equipped staff. All Chemical, Biological, Radiological and Nuclear, explosives (CBRNe) incidents, whether a likely to be terrorist-related, or will be treated as such by responder organisations. 1.15 Mass Casualties
A mass casualty incident is defined by NHS England as:
‘A disastrous single or simultaneous event(s) or other circumstances where the normal major incident response of several NHS organisations must be augmented by
extraordinary measures in order to maintain an effective, suitable and sustainable response’.
1.16 Mass Fatalities
A Mass Fatality incident is one that involves numbers of deaths that exceed the capacity afforded by normal major incident arrangements. This will invariably need a multi–agency response and require the triggering of the respective Local Resilience Forum Mass Fatality Plan or National Emergency Mortuary Arrangements (NEMA).
Each incident will be judged on the circumstances at the time.
Considerations which determine whether to declare a Mass Fatalities emergency include:
The number of deceased; Fragmentation of bodies;
Is the incident which resulted in the deaths a terrorist or other criminal act; Current mortuary capacity;
Are there other similar incidents elsewhere in the Region or United Kingdom; Are the deceased contaminated in any way; and
Is there a requirement for a forensic post-mortem.
The decision to declare a Mass Fatalities emergency will be made by the appropriate HM Coroner in conjunction with the Chair of the Strategic Coordinating Group (SCG) for the respective Local Resilience Forum.
1.17 Civil Contingencies Act 2004
The Civil Contingencies Act 2004 (CCA 2004) categorises responding agencies into Category 1 and Category 2 responders and places statutory duties on the identified organisations.
Category 1 responders have the following statutory duties placed on them: To carry out a risk assessment of their operational area;
To have emergency plans;
To have business continuity plans; To warn and inform the public;
To co-operate with other responders through the Local Resilience Forum (LRF); and To share information with other responders.
Southern Health NHS Foundation Trust is a Category 1 Responder organisation Category 2 responders have the following statutory duties placed on them:
To co-operate with other responders; and To share information with other responders. 1.18 Health & Social Care Act 2012
The Health & Social Care Act 2012 places additional duties on NHS organisations to maintain emergency plans and to have in place formal business continuity arrangements as well as:
Ensuring contracts with provider organisations contain relevant emergency preparedness, resilience (including business continuity) and response elements;
Supporting NHS England in discharging its EPRR functions and duties locally;
Providing a route of escalation for the Local Health Resilience Partnership (LHRP) should a provider fail to maintain necessary EPRR capacity and capability; and
Ensuring representation on the Local Health Resilience Partnership. Local Resilience Forum (LRF)
1.19 The emergency services normally provide most of the initial response, supported by the local authorities, utility companies (gas, water, telecommunications and electricity) and voluntary (third sector) organisations. The emergency services main role will most frequently be to save life. The Fire and Rescue Service is responsible for rescuing survivors. The Ambulance
Service is responsible for triaging casualties, treating casualties and transferring casualties to hospital. The Police are responsible for taking the lead in co-ordinating the multi-agency response, as well as investigating crime scenes and identifying responsibility for cause (if criminal activity suspected).
1.20 The Civil Contingencies Act (CCA) 2004 states that multi-agency emergency preparedness is undertaken in areas known as a Local Resilience Forum based on police constabulary
Local Resilience Forum (LRF) Hampshire and Isle of Wight and Local Resilience Forum Thames Valley (includes Berkshire, Buckinghamshire, Milton Keynes and Oxfordshire) and information about each LRF can be found on the following websites:
LRF Hampshire and Isle of Wight - http://www3.hants.gov.uk/localresilienceforum.htm
LRF Thames Valley - http://thamesvalleylrf.org.uk/
1.21 The following local organisations make up the Local Resilience Forum Hampshire and Isle of Wight and are categorised under the CCA 2004 as follows:
Category 1 Responders Health
Southern Health NHS Foundation Trust
South Central Ambulance Service NHS Foundation Trust Hampshire Hospitals NHS Foundation Trust
Portsmouth Hospitals NHS Foundation Trust
University Hospital Southampton NHS Foundation Trust Isle of Wight NHS Trust
NHS England - Wessex Area Team Public Health England - Wessex Partner Organisations
Hampshire Constabulary
Hampshire Fire & Rescue Service Hampshire County Council
Portsmouth City Council Southampton City Council Isle of Wight Council
Hampshire’s 11 District & Borough Councils
(this includes Eastleigh, New Forest, Test Valley, Winchester councils) The Environment Agency
Maritime & Coastguard Agency – Her Majesty’s Coastguard Category 2 Responders
Fareham & Gosport Clinical Commissioning Group Isle of Wight Clinical Commissioning Group
North Hampshire Clinical Commissioning Group
North East Hampshire & Farnham Clinical Commissioning Group Portsmouth Clinical Commissioning Group
South Eastern Hampshire Clinical Commissioning Group Southampton City Clinical Commissioning Group
West Hampshire Clinical Commissioning Group Utilities - gas, water and electric supply companies Network Rail & train operating companies
Harbour authorities and ferry companies Telephone operating companies
The Highways Agency
1.22 The following local organisations make up the Local Resilience Forum Thames Valley and are categorised under the CCA 2004 as follows:
Category 1 Responders Health
Berkshire Healthcare Foundation Trust Buckinghamshire Hospitals NHS Trust Buckinghamshire Urgent Care Services Burns and critical/trauma network
Central Southern Commissioning Support Unit
Heatherwood & Wexham Park Hospital NHS Foundation Trust Milton Keynes Hospital NHS Foundation Trust
NHS Blood and Transplant
NHS England South (Supra Regional Office) NHS England Thames Valley Area Team Nuffield Orthopaedic Centre NHS Trust Oxford Health NHS Foundation Trust Oxford University Hospitals NHS Trust Public Health England Centre Thames Valley Royal Berks Hospital NHS Foundation Trust
South Central Ambulance Service NHS Foundation Trust Thames Valley Emergency Access
Partner Organisations Thames Valley Police
Oxfordshire Fire and Rescue Service Royal Berkshire Fire and Rescue Service Bracknell Forest Council
Buckinghamshire County Council Cherwell District Unitary Council Oxford City Council
Oxfordshire County Council Reading Borough Council
South Oxfordshire District Council Slough Council
Vale of White Horse District Council West Berkshire Council
West Oxfordshire District Council Windsor & Maidenhead Council Wokingham Borough Council The Environment Agency Category 2 Responders
Oxfordshire Clinical Commissioning Group
Newbury and District Clinical Commissioning Group North and West Reading Clinical Commissioning Group
South Reading Clinical Commissioning Group Wokingham Clinical Commissioning Group
Bracknell and Ascot Clinical Commissioning Group
Windsor, Ascot and Maidenhead Clinical Commissioning Group Slough Clinical Commissioning Group
Chiltern Clinical Commissioning Group
Aylesbury Vale Clinical Commissioning Group Milton Keynes Clinical Commissioning Group Swindon Clinical Commissioning Group
Utilities - gas, water and electric supply companies Network Rail & train operating companies
Telephone operating companies Airport operators
The Highways Agency
1.23 Hampshire & Isle of Wight LRF and Thames Valley LRF have a formal meetings structure to facilitate the business of the LRF and health is represented on many of them by the NHS England (Wessex) and (Thames Valley) Area Team respectively.
1.24 Local Community Risks & Threats
A formal risk assessment of hazards and risks is undertaken by a multi-agency LRF risk assessment group every year as required by the Civil Contingencies Act 2004. Health assessments feed directly into each Local Resilience Forum’s Community Risk Register. For LRF Hampshire & Isle of Wight, this can be found at:
http://www3.hants.gov.uk/localresilienceforum/community-risk-register.htm
Top risks on Hampshire & Isle of Wight LRF Community Risk Register (2013) are:
Ref Category Description Risk Rating
H9 Industrial Accident Large toxic chemical release VERY HIGH HL2 Industrial Accident Local industrial accident involving toxic
release
VERY HIGH H18 Severe Weather Low temperatures and heavy snow VERY HIGH H19 Severe Weather Major coastal & tidal flooding affecting >2
UK regions
VERY HIGH H21 Severe Weather Severe inland flooding affecting > 2 UK
regions
VERY HIGH HL16 Severe Weather Local coastal / tidal flooding affecting > 1
region
VERY HIGH HL17 Severe Weather Local coastal / tidal flooding affecting 1
region
VERY HIGH H23 Human Health Influenza-type Disease (pandemic) VERY HIGH H40 Telecoms No notice loss due to localised incident VERY HIGH H43 Telecoms – human
error
Widespread loss of telecoms at regional level up to 5 days
VERY HIGH
http://thamesvalleylrf.org.uk/useful-links/publications/risk-register.ashx
Top risks on Thames Valley LRF Community Risk Register (2013) are:
Ref Category Description Risk Rating
H17 Severe Weather Storms and Gales VERY HIGH
H18 Severe Weather Low temperatures and heavy snow VERY HIGH
H50 Severe Weather Drought VERY HIGH
H21 Severe Weather Severe inland flooding affecting > 2 UK regions
VERY HIGH HL18 Severe Weather Local / Urban flooding (fluvial or surface
run-off).
VERY HIGH
HL19 Severe Weather Local fluvial flooding VERY HIGH
H36 International Events International disruption to oil supply VERY HIGH 1.25 National Risk Register
The National Risk Register of Civil Emergencies July 2013 edition provides an updated government assessment of the likelihood and potential impact of a range of different civil emergency risks (including naturally and accidentally occurring hazards and malicious threats) that may directly affect the UK over the next 5 years. It can be found at:
https://www.gov.uk/government/publications/national-risk-register-for-civil-emergencies-2013-edition
1.26 National Threat Level - the level of threat from terrorism is under constant review by the Security Services:
Low an attack is unlikely
Moderate an attack is possible, but not likely
Substantial an attack is a strong possibility
Severe an attack is highly likely
Critical an attack is expected imminently The latest threat level can be viewed at:
https://www.mi5.gov.uk/home/the-threats/terrorism/threat-levels.html
Emergency Preparedness in the Health Sector 1.27 Local Health Resilience Partnership (LHRP)
The Local Health Resilience Partnership is a strategic forum for organisations in the local health sector. The LHRP facilitates health sector preparedness and planning for emergencies at Local Resilience Forum level. It supports the NHS, Public Health England (PHE) and local
authority (LA) representatives on the LRF in their role to represent health sector Emergency Planning, Resilience and Response (EPRR) matters
Due to the wide geographical spread of the Trust, the Organisation is part of the Hampshire and Isle of Wight LHRP and Thames Valley LHRP. The key responsibilities of the LHRP are to:
Facilitate the production of local sector-wide health plans to respond to emergencies and contribute to multi-agency emergency planning;
Provide support to both NHS England (Wessex) and (Thames Valley) and Public Health England (PHE) in assessing and assuring the ability of the health sector to respond in partnership to emergencies at an LRF level; and
Remind all constituent organisations that they remain responsible and accountable for their effective response to emergencies in line with their statutory duties and obligations. As with LRFs, the LHRP has no collective role in the delivery of emergency response and are described as having non-collective responder status
Membership for both LHRPs includes the Accountable Emergency Officers from:
NHS England Wessex and Thames Valley Area Team - Director of Operations & Delivery (co-chair)
Lead Director of Public Health (co-chair) Statutory Ambulance Service
Public Health England NHS Acute Hospitals NHS Foundation Trusts
NHS Community & Mental Health Providers Clinical Commissioning Groups
Independent Health Sector Voluntary Sector
1.28 Local Health Resilience Partnership Sub-Group
The LHRP Sub-Group comprises the responsible managers from each of the above organisations and public health representatives from each Local Authority and is responsible for the planning and delivery of the EPRR agenda for the LHRP.
1.29 NHS England EPRR Guidance (2013)
Key responsibilities outlined within the guidance documents are that:
The Chief Executive is responsible for ensuring that SHFT has an Incident Response Plan and is able to respond to a major incident;
The SHFT Board is regularly briefed with reports on SHFTs preparedness, additional risks, training and exercising;
An Executive Director Lead is nominated;
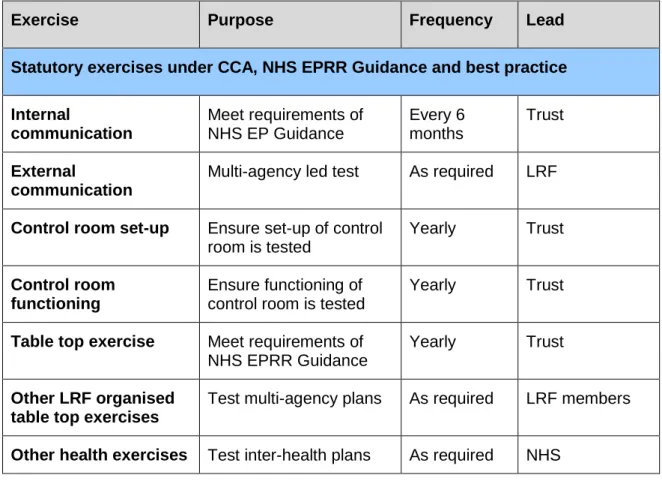
A communications exercise is carried out every 6 months; A table top exercise is carried out yearly; and
1.30 NHS England EPRR responsibilities
The NHS England (Wessex) and (Thames Valley) Area Teams are the Health EPRR lead for their specific geographical area and as such has specific planning and response
responsibilities which include:
Maintaining a health emergency planning network, co-chaired by its Lead Director for EPRR, and the Director for Public Health via the Local Resilience Health Partnership ensuring all NHS organisations in the area meet at least quarterly to agree health resilience issues;
Representing the local health economy at LRF Strategic level;
The NHS England Area Team Lead Director for EPRR is responsible for ensuring the local NHS contributes fully to any local multiagency training and exercising programme, especially, but not limited to, exercises that are of a statutory requirement for local high risk sites.
Ensuring NHS Trusts within the area comply with NHS Commissioning Board, Core Standards for EPRR 2013 and their statutory duties under the CCA 2004;
Maintaining strong links with NHS England, South in its leadership role
In a large scale incident coordinating and strategically managing the NHS response across the geographical area of operation;
Ensuring a mechanism for local organisations (particularly Local Authority, Police and Ambulance Trusts) to access through a single point of contact, NHS Primary Care and Community Services;
Ensuring the Director on Call has clearly delegated authority to mobilise and direct the resources of any NHS organisations across the area during an incident. This authority can be used when necessary without reference back to others. This senior level delegated responsibility is critical if the Director on-call is required to attend the multi-agency Strategic Coordinating Group, or Gold Command;
To liaise with Public Health England to establish and support a Scientific and Technical Advice Cell (STAC) to provide science and technical advice to the Strategic Coordinating Group and Police Incident Commander during an major incident or emergency;
Jointly access the public health impact of a major incident, with Public Health England and Local Authority, Director of Public Health; and
Provide a strategic view on long term threats. 1.31 NHS England, South EPRR responsibilities
In the event of a major incident that crosses LRF borders, or is of such size that the NHS within a large operational area would be overwhelmed, NHS England, South is responsible for
coordinating necessary contingency arrangements across the wider area, which could include the use of other area or national assets and liaison with central government departments. 1.32 Southern Health NHS Foundation Trust EPRR responsibilities
SHFT major incident planning responsibilities are to:
Provide assurance of a 24/7/365 managed response;
Appoint/nominate a Lead Director as the Accountable Emergency Officer for Emergency Preparedness, Resilience and Response (EPRR) who is responsible for
SHFT emergency planning. This person should report to the board regularly on risks to delivering EPRR across the trusts services;
Maintain an emergency planning network, chaired by the Accountable Emergency Officer which meets at least quarterly to agree and commission work stream activity on resilience issues;
Undertake EPRR assurance via a mapping exercise and where there are capacity gaps, and take appropriate measures to ensure c;
Maintain a sufficiently resourced and adequately qualified and competent Emergency Preparedness, Resilience and Response Team, which can manage the day-to-day EPRR work, and support the Lead Director for EPRR and Board;
Maintain a 24/7 on-call rota that includes response and incident support;
Ensure sufficient testing and exercising of communication plans in accordance with the 2013 NHS Commissioning Board Guidance. This should include testing both in hours and out of hours;
Contribute fully to any local multi-agency training and exercising programme, especially, but not limited to, exercises that are of a statutory requirement for local high risk sites, i.e. Nuclear Power installations, chemical plants, sports grounds etc;
Ensure compliance with the Civil Contingencies Act 2004;
Ensure compliance with the NHS Commissioning Board EPRR Guidance 2013; Communicate the availability of the Incident Response Plan, and undertake regular
review and testing of the plan; and
Maintain strong links with both NHS England Area Teams Wessex and Thames Valley in emergency planning leadership role and other health organisations within the Local Health Resilience Partnerships and Local Resilience Forums.
1.33 Southern Health NHS Foundation Trust Emergency Response Responsibilities SHFT major incident response responsibilities are to:
Ensure an appropriate 24/7/365 managed response to a local incident;
Support the local system wide response, including cross boundary mutual aid for emergency response;
Continue to maintain provision and provide local system management for routine capacity issues, diversion and winter pressures;
Ensure the Director on Call has clearly delegated authority to mobilise and direct SHFT resources across the SHFT area during an incident. This executive authority is able to be used when necessary without reference back to others and is critical if the Director on Call is required to attend the multi-agency Strategic Coordinating Group; and
Maintain a capacity to provide 24/7/365 coordination to an incident via a suitably equipped Incident Coordination Centre with trained staff over a continual 24 hour period and of up to two weeks duration.
1.34 Individual Responsibilities of Southern Health NHS Foundation Trust Staff a. The Chief Executive
The Chief Executive is responsible for ensuring the trust:
is able to comply with its statutory duties as a Category One Responder under the Civil Contingencies Act 2004;
Guidance documents 2013 and has appropriate major incident Command, Control Communication, Coordination and Cooperation (C5) arrangements in place; has an Executive Director of the Board designated the Accountable Emergency
Officer (AEO) to take lead responsibility for emergency preparedness, resilience and response;
has a Non-Executive Director nominated to support the designated Lead
Executive Director (AEO) for emergency preparedness, resilience and response has an adequately resourced qualified and competent Emergency Preparedness,
Resilience and Response Team to support the Lead Executive and Non-Executive Directors in the discharge of their emergency preparedness duties;
that the Board receives regular reports, at least annually, regarding emergency preparedness to include reports on exercises, training and testing, and assurance that adequate resources are available for the discharge of emergency
preparedness responsibilities; and
has overall accountability for the SHFT response to a major incident. b. EPRR Accountable Emergency Officer (AEO)
To ensure the Trust has adequate plans in place and that EPRR is adequately resourced with the staff trained and plans tested;
To represent the Trust at Local Health Resilience Partnership (LHRP) meetings; To act as the Accountable Emergency Officer so as to ensure that the Trust:
• is compliant with the statutory EPRR requirements as set out in the Civil Contingencies Act (2004); the NHS Planning Framework and the NHS standard contract as applicable;
• is properly prepared and resourced for dealing with a major incident or civil contingency event;
• that any providers the trust commissions, have robust business continuity planning and response arrangements in place which reflect standards set out in the Framework for Health Services Resilience (PAS 2015) and ISO 22301;
• has a robust surge capacity plan that provides an integrated organisational response and that it has been tested with other providers and parties in the local communities served;
• complies with any requirements of the NHS England (Wessex & Thames Valley) in respect of the monitoring of compliance;
• provide NHS England (Wessex & Thames Valley) with such information as it may require for the purpose of discharging its functions; and
• is appropriately represented at any governance meetings, sub-groups or working groups of the Local Health Resilience Partnership (LHRP) or Local Resilience Forum (LRF).
c. On-Call Director, Divisional and Area Managers on Call Will:
be available and contactable 24 hours, 7 days a week during their period on call; Have access to their On Call Information Pack and Trust ID card at all times; Have key contact numbers programmed in their mobile phone i.e. all SHFT Flextel
in and out of hours), and the contact numbers for their teams (both in and out of hours);
Ensure they can travel within 2 hours to the SHFT Incident Coordination Centre (ICC) based on the Trust headquarters site. If circumstances prevent travel to the ICC within 2 hours, make arrangements with a colleague to fulfil this function; Undertake emergency planning training at least annually and participate in an
exercise at least every two years;
Abstain from drinking alcohol during their period on call as it may be necessary to undertake a key role in the management of a major incident or emergency, and drive to the SHFT Incident Coordination Centre or other sites, as required;
d. The Director on Call will:
Provide advice and support to Divisional Managers on Call for operational issues out of hours;
be the main point of contact for Serious Incident Requiring Investigation (SIRI) out of normal working hours;
be the main point of contact for media related concerns out of hours ensuring close liaison with the SHFT Communications on Call for media related support; strategically manage SHFT services during periods of demand fluctuations; Lead on out of hours systems resilience teleconferences for SHFT;
Lead on SHFT Business Continuity incidents to Red Essential Services and Amber Services which could be scaled down if necessary;
In the event of a major incident or emergency undertake the role of Incident Commander (Gold) making an initial assessment of the level of response and
resources required, implementing the Incident Response Plan and Action Cards, and strategically managing SHFT services;
activate the SHFT Incident Management Team and open the SHFT ICC, calling in support staff as appropriate;
Contact and/or liaise with NHS England Director on Call/Clinical Commissioning Group(s) on call in the event of a major incident and as appropriate;
Notify and brief other Executive team members as required;
Provide SHFT situation reports to NHS England Area Team and/or CCG ICC(s); as requested, attend the Strategic Co-ordinating Group or NHS England, Area Team
ICC locations;
proactively communicate with SHFT staff regarding the major incident or emergency and ensure relevant guidance and advice is available;
Ensure SHFT staff are not exposed to unnecessary health and safety or other risks, and that adequate shift and rota breaks are built into prolonged incident management arrangements; and
Ensure support to any activated local authority Rest Centre(s) if required. e. The Divisional and Area Managers on Call will:
Provide advice and support to operational issues out of hours; and
Inform the appropriate Manager at the start of the next working day of any incident. Out of hours
Liaise with the Director On Call as appropriate;
Lead on SHFT Business Continuity incidents to Green Services which could be discontinued if necessary;
Coordination Centre, or SHFT Incident Team in the event of a major incident or Emergency; and
Provide Divisional/Area situation reports to the Director on Call.
1.35 Head of Risk and Business Continuity
The Head of Risk and Business Continuity supported by the Business Continuity and Resilience Manager, the organisations Emergency Preparedness, Resilience and Response Manager, is responsible for coordinating SHFT’s major incident
emergency preparedness by:
Leading the development, coordination and performance monitoring of SHFT’s major incident, business continuity and response planning arrangements; Representing SHFT across Local Resilience Forums, major incident planning
Networks;
Identifying national, regional and local emergency planning policy changes and developments that impact on SHFT and translating these into operational practice; providing assurance to the SHFT Board and senior managers on the resilience of
SHFTs major incident planning and response arrangements;
Identifying major incident planning training needs, ensuring appropriate training is delivered so that SHFT staff understand their role and responsibilities in a major incident response and are competent to perform them;
ensuring the mobile phone numbers of key Executive and senior managers are registered with the Mobile Telecoms Privileged Access Scheme (MTPAS); during a major incident supporting the Incident Commander as appropriate during a major incident ensuring the preservation and protection of all documents
relating to the major incident, collating and archiving as appropriate;
Ensuring a debrief takes place immediately following a major incident, and a thorough debrief shortly after the major incident; and
compiling a report of the SHFT major incident response with recommendations for change and ensuring the Incident Response Plan, associated Plans and Action Cards, Business Continuity Management Policy and Business Continuity Plans, and Risk Management Policy are updated as necessary.
1.36 Director of Workforce and Communications
The Director of Workforce and Communications is responsible for ensuring that: Human Resource policies ensure all staff are aware of their responsibility to
support SHFT in responding effectively to incidents, major incidents and emergencies;
Staff records include information on staff dependencies and skills to allow for Redeployment;
Ensuring senior HR staff are aware of their responsibilities in the event of an incident, major incident or similar emergency;
during a major incident or emergency, HR services are prioritised to enable the SHFT workforce to meet the needs of the situation i.e. timely recruitment of staff, retired staff, and volunteers;
Workforce issues as a result of a request for mutual aid from another organisation resulting in the temporary transfer of staff between organisations are managed; and A list of staff involved in the major incident is maintained and that those staff have
access to appropriate support services such as occupational health and
counselling, and that any necessary changes to the Services Level Agreements are negotiated.
1.37 Director of Finance
The Director of Finance is responsible for:
ensuring that adequate resources are made available for the discharge of SHFTs emergency planning responsibilities;
recognising the need for a contingency budget; ensuring that emergency cost codes are available;
Leading the recovery following a major incident, both financial and general; and
That Service Level Agreements are in place with all suppliers and contractors who have comprehensive emergency planning and business continuity arrangements
The Director of Finance is also the SHFT Designated Security Management Executive Director and responsible for the overall management of SHFTs security, and for ensuring this policy and associated plans and action cards comply with national best practice and are relevant to SHFT, its services and premises. 1.38 Head of Information, Communication and Technology
During a major incident the SHFT Incident Team, and other key staff, will require robust access to the Information Communication and Technological (ICT) systems. The Head of ICT is responsible for:
Developing plans to ensure the SHFT Incident Team, and other key staff, have access to ICT support during a major incident both inside and outside of office hours;
Ensuring there are Emergency Planning and Generic email accounts available to the Incident Team to use within the Incident Coordination Centre;
ensuring there are comprehensive Business Continuity and Disaster Recovery (DR) Plans for all ICT services;
ensuring these plans are well communicated to the Senior and Area Managers on Call, clinical and ICT staff; and
Developing mutually beneficial relationships with partner organisations to allow for mutual aid.
1.39 Director of Communications & Media
The Associate Director of Communications is responsible for: Maintaining the On Call communications rota;
Developing and maintaining the SHFT major incident communications plan; Providing a representative at the NHS England communications group;
Providing a representative at Local Resilience Forum(s) Warning & Informing group Maintaining links with NHS England communications team and with other local
NHS Trust communications leads and as required during an incident;
Ensuring that the SHFT communication staff have had the appropriate training Taking part in exercises as required;
Having appropriate mechanisms in place to establish telephone lines for the public; and Developing beneficial relations with the media.
1.40 Divisional Directors, Area and Service Managers
Divisional Directors, Area and Service managers are responsible for ensuring: Sufficient resources are allocated to deliver the requirements of this policy and
assurance arrangements are in place to monitor compliance;
All staff are familiar with this Incident Response Plan, its associated Plans and Action Cards, and their services Business Continuity Plans;
That their Division, Area, and Service can contribute to the SHFT response to major incidents, emergencies or any situation that may challenge the delivery of services;
That every Division, Area and Service has a nominated lead for emergency planning and business continuity which is clearly defined and resourced; That the Divisional nominated lead for emergency planning and business
continuity is an active member of the Trust’s Business Continuity and Resilience Group;
That robust Business Continuity Plans are in place for all services, sites and functions within their Division, Area or Service;
Ensuring Business Continuity Plans are tested and exercised at least annually, and records maintained of these tests and exercises;
Ensuring staff are released to attend major incident training;
Identifying any unmet training needs at supervision and appraisal; and Maintaining an up to date list of the names and contact details (in and out of
hours) of the staff within their teams.
1.41 All Southern Health NHS Foundation Trust employees All SHFT employees are responsible for:
On appointment and periodically thereafter familiarising themselves with the SHFT Incident Response Plan, associated plans and action cards, and their service’s Business Continuity Plan;
Familiarising themselves with how they should report for duty should a major
incident occur, and their roles and responsibilities within a major incident; Attending major incident training, and for identifying any unmet training needs at
supervision and appraisal;
Participating in major incident and business continuity exercises as required; Being vigilant to the security of premises and staff;
Ensuring that any change in their home address or contact details is reported to their line manager to enable up to date out of hours contact lists to be maintained;
Cooperating with SHFT during a major incident, undertaking duties within their scope of practice as and where requested, cooperating with redeployment into different roles at different sites, working flexibly to meet the needs of their service, and for fulfilling their contractual duties wherever possible; and
Having up to date formal identification cards on their persons at all times while on
Duty.
During a major incident SHFT employees are expected to make every effort to attend work. If this is not possible e.g. for safety reasons employees must report this each day. If it is possible for employees to work at home they can do so as long as this is with the agreement of their line manager and they can arrange cover. If employees are unable to attend work and cannot work at home, they can, with agreement from
their line manager, use flexi time or outstanding lieu days, take annual leave or take unpaid leave or make up the hours subsequently.
In relation to a major incident/emergency, it will be a Corporate decision to exceptionally grant special leave.
1.42 Southern Health NHS Foundation Trust responsibilities to its staff
A major incident will impact on the availability of SHFT staff to undertake their normal duties. Similarly SHFT staff may be required to work longer hours than normal, and may be adversely affected by the incident either personally or professionally. SHFT has a responsibility to ensure that staff welfare is considered and promoted.
The SHFT policy An Emergency Event: Guidelines on Managing the Workforce Issues provides the framework whereby SHFT ensures it is able to continue its functions while meeting its responsibilities to its staff. The policy An Emergency Event: Guidelines on Managing the Workforce Issues will take precedence over all existing HR policies in the event of a major incident. The decision to implement the policy will be taken by the Incident Commander/Director on Call in liaison with the Director of Workforce and Communications, Chief Executive, or appropriate deputy. SHFT will ensure that:
Staff welfare is considered and promoted during and following a major incident.
Occupational Health and or the Trust’s CISM team are informed of any staff involved in a major incident so that any necessary follow up support can be given; and
Staff have access to an Employee Assistance Programme (which gives independent advice, information and provides a counselling service).
1.43 Southern Health NHS Foundation Trusts Responsibilities to vulnerable people The CCA 2005 places a duty on Category 1 Responders (i.e. SHFT) to have regard for the needs of vulnerable people in a major incident. It is difficult to define in advance who would be vulnerable in any particular major incident or emergency. However there are three categories of vulnerable people that should always be considered:
Those who have mobility difficulties i.e. with a physical or mental disability, a medical condition, pregnant women;
Those with mental health problems;
Others who are dependent, such as children, people with learning disabilities, the frail elderly, those dependant on drugs dressings, or medical equipment; and People with sensory difficulties e.g. blindness, deafness, or who are unable to
understand instructions e.g. non-English speakers. 1.44 NHS 111 Service EPRR responsibilities
In the event of a major incident, 111 services can be used to support the response by
answering public questions about the health effects of incidents and to give advice to the public either by agreed statements or via predetermined algorithms to provide a single point of
access for all non-emergency NHS services. 1.45 Equality & Diversity
Equality is about creating a fairer society where everyone has the opportunity to fulfil their potential. Diversity is about recognising and valuing difference in its broadest sense.
In preparing these arrangements for the Trust’s response to an emergency, the Trust has been mindful of its obligations under the Equality Act 2010. The Equality Duty ensures that public bodies consider the needs of all individuals in shaping policy, delivering services and in relation to their own employees. It encourages public bodies to understand how different people will be affected by their activities so that policies and services are appropriate and accessible to all and meet different people's needs.
SECTION 2
Declaration of a Major Incident and Alerting Routes
2.1
Declaration of a Major Incident
2.2 National Alerting Messages
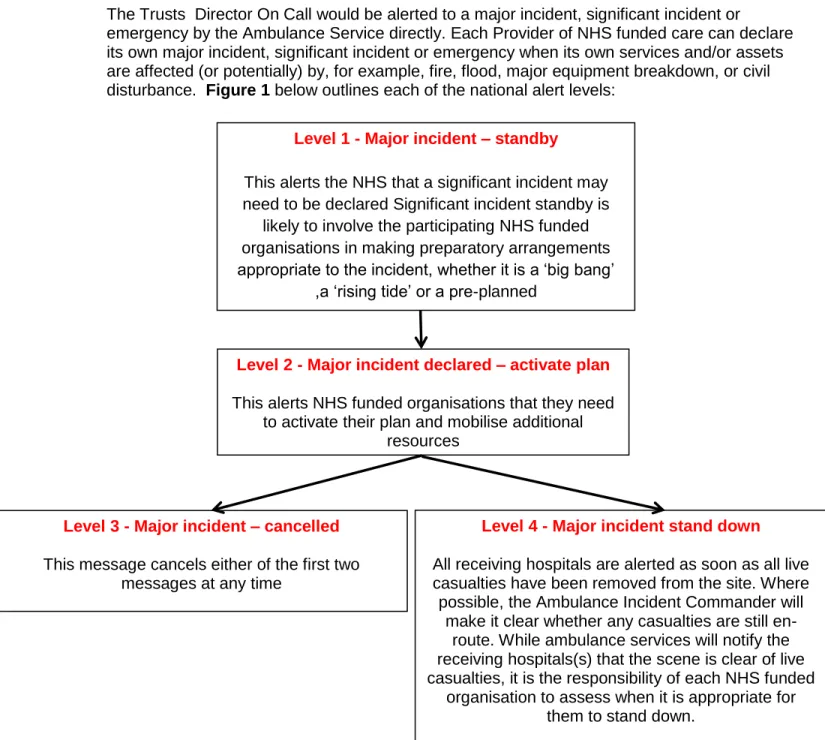
The Trusts Director On Call would be alerted to a major incident, significant incident or
emergency by the Ambulance Service directly. Each Provider of NHS funded care can declare its own major incident, significant incident or emergency when its own services and/or assets are affected (or potentially) by, for example, fire, flood, major equipment breakdown, or civil disturbance. Figure 1 below outlines each of the national alert levels:
Level 1 - Major incident – standby
This alerts the NHS that a significant incident may need to be declared Significant incident standby is
likely to involve the participating NHS funded organisations in making preparatory arrangements appropriate to the incident, whether it is a ‘big bang’
,a ‘rising tide’ or a pre-planned
Level 2 - Major incident declared – activate plan
This alerts NHS funded organisations that they need to activate their plan and mobilise additional
resources
Level 3 - Major incident – cancelled
This message cancels either of the first two messages at any time
Level 4 - Major incident stand down
All receiving hospitals are alerted as soon as all live casualties have been removed from the site. Where possible, the Ambulance Incident Commander will
make it clear whether any casualties are still en-route. While ambulance services will notify the receiving hospitals(s) that the scene is clear of live casualties, it is the responsibility of each NHS funded
organisation to assess when it is appropriate for them to stand down.
2.3 Alert Triggers
The On Call Director will be the lead for the Trust if:
A ‘Major Incident’ or a ‘Major Incident Standby’ is declared; There are very serious capacity issues;
An incident has received, or is likely to receive, challenging media coverage; Incidents that may affect the services of multiple provider organisations;
Significant flooding, fires and incidents involving the release CBRN or hazardous materials with the potential to cause casualties, regardless of whether they are declared major incidents;
Requests for local NHS attendance at Strategic Co-ordinating Groups, their sub-groups, or any equivalent that requires strategic NHS support; and
See Figure 2 for escalation of incidents and establishment of co-ordination arrangements for Level 1 – 4 incidents in Wessex and Thames Valley.
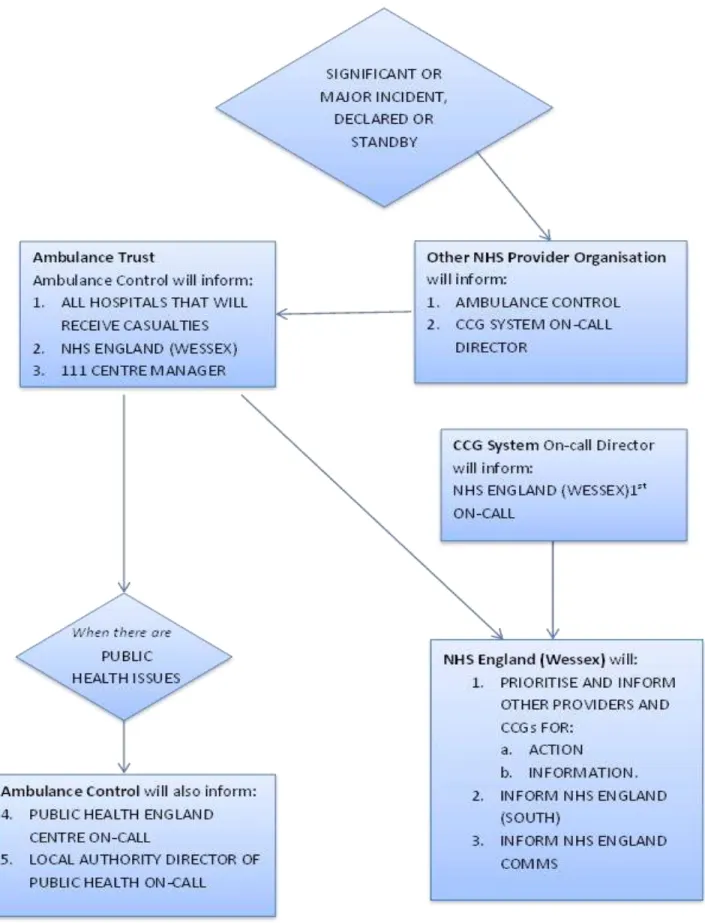
2.4 Major Incidents Declared by the Statutory Ambulance Service (Figure 3)
The ambulance service is responsible for informing receiving hospitals and the NHS England (Wessex) and (Thames Valley) Area Team whenever the service declares a ‘major incident’ or ‘major incident standby’. NHS England (Wessex) and (Thames Valley) Area Team is also responsible for advising the regional office of NHS England (South) of any major incidents or other significant incidents.
2.5 Major Incidents Declared by a Provider/this Trust
NHS funded provider organisations are responsible for informing their commissioning CCGs and the ambulance service whenever they are activated or declare a ‘major incident’ or ‘major incident standby’. The CCGs will in turn inform the NHS England (Wessex) and (Thames Valley) Area Teams.
2.6 Major Incidents Declared by the NHS England (Figure 4)
The NHS England (Wessex) and (Thames Valley) Area Teams are responsible for informing the ambulance services and CCGs of any national, regional or area ‘major incident’, ‘major incident standby’ or similar message where there is a need to respond locally or cross border mutual aid is required. The Ambulance Service will then inform Acute Hospitals and theCCGs will inform other provider organisations.
Notes:
1. Other activation messages Other activation messages include:
Mass Casualty Incident
Operation Plato (also known as MTFA)
Off Site Nuclear Emergency (‘OSNE’ at sites regulated by the Office of Nuclear Regulations and the Defence Nuclear Safety Regulator)
Major Accident (at a site regulated by Control of Major Accident Hazards regulations)
The cascade of information will be as this ‘major’ and ‘significant’ incident cascade and the relevant plans should be activated.
2. Scene clear and stand down
Ambulance services will cascade their own ‘scene clear’ and ‘stand down’ messages to
receiving hospitals. Those messages relate to the ambulance service response and are shared for information. Other NHS organisations should not stand down their own response without authorisation of their own strategic leadership and without notifying the relevant CCG and NHS England offices.
3. Primary care
NHS England will issue messages to providers of primary care services in office hours. Out of hours messages will be passed by the ambulance service to the 111 centre manager(s) – (tbc - can they do GP OOHs?)
4. South West Ambulance Service NHS Foundation Trust (SWASFT) & Dorset
SWASFT use an automated messaging system to cascade messages. Cascade messages include an instruction to dial into a recorded situation report. Organisations dialling into the recorded report are asked to input a unique PIN so that SWASFT can identify which
organisation has received the situation report. On-call staff should ensure that they are aware of their organisation’s unique PIN issued by SWASFT.
The use of an automated cascade by SWASFT fits the process described in the cascade flow chart – SWASFT will advise public health on-call when necessary and NHS England will ensure that NHS partners not directly affected are aware of the incident.
5. Other communication
This cascade diagram does not prevent or preclude any other communications but is the only process for formal distribution of significant and major incident declaration and stand-by messages within the NHS in Dorset, Hampshire and the Isle of Wight.
6. NHS England (Wessex) 2 tier on-call
In the summer of 2015 NHS England (Wessex) will move from a single to a two-tier on-call system. The NHS England (Wessex) 1st on-call will be contacted via a pager service on 07623 503888.
Figure 4 - The Cascade of ‘Major Incident’ and ‘Major Incident Standby’ declarations by the NHS England (Wessex) and (Thames Valley) Area Teams
The cascade above is relevant when an incident has an impact on organisations across different boundaries as is likely during Level 2, 3 and 4 Incidents. In these cases, the NHS England (Wessex) and (Thames Valley) Area Teams will co-ordinate the response.
CCG Provider Provider Provider Provider Provider Provider CCG Provider Provider Provider NHS England
(Wessex) Local Resilience
Forum (SCG) Partners (incl. ambulance, PH, & PHE) Local Resilience Forum (SCG) Partners (incl. ambulance, PH, & PHE) NHS England (Thames Valley) NHS England (South) CCG
2.7 Trust Incident Response Plan Activation
Any On Call Manager may considerthe activation of the Incident Response Plan, regardless of any formal alerting message. Such action may be taken when it is apparent that severe weather or an environmental hazard may demand the implementation of special arrangements or when a spontaneous response by members of the public results in the presentation of major incident, casualties at any health care setting e.g. acute or community hospital, walk-in centre, health centre, GP Practice or minor injuries unit.
2.8 Alerting Routes
Major Incident alerts will normally come through the Trust’s Director On Call on a 24 hour basis. The call may come from one or more of the following organisations/groups:
Provider organisations such as: Wessex Area:
South Central Ambulance NHS Foundation Trust
Hampshire Hospitals NHS Foundation Trust (Basingstoke or Winchester sites) Frimley Park NHS Foundation Trust
University Hospital Southampton Foundation Trust Salisbury NHS Foundation Trust
Royal Bournemouth & Christchurch NHS Foundation Trust Solent NHS Foundation Trust
Independent Health Organisations Thames Valley Area:
South Central Ambulance NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Buckinghamshire Hospitals NHS Trust Buckinghamshire Urgent Care Services Burns and critical/trauma network
Central Southern Commissioning Support Unit
Heatherwood & Wexham Park Hospital Foundation Trust Milton Keynes Hospital NHS Foundation Trust
NHS Blood and transplant
Nuffield Orthopaedic Centre NHS Trust Oxford Health NHS Foundation Trust Oxford University Hospitals NHS Trust Royal Berkshire Hospital Foundation Trust Independent Health Organisations
Primary Care: Local GPs
Other health professionals Pharmacies
National activation by the Department of Health via: NHS England Wessex or Thames Valley Area Team(s) Mutual Aid Response:
Neighbouring Clinical Commissioning Groups (in Hampshire, Southampton, Portsmouth, Dorset, Wiltshire and Thames Valley)
Internal Incident:
Members of Trust’s staff Primary Care:
Local GPs
Out of Hours Primary Care Provider Other health professionals
Pharmacies
For a ‘major incident’ or ‘major incident standby’, the Trust On Call Director will normally contact the West Hampshire CCG- Lead CCG On Call Director to alert them to the situation. In the absence of this arrangement, contact with the On Call Director of either NHS England (Wessex) or (Thames Valley) must be made via:
The response to many local incidents will be co-ordinated by the Clinical Commissioning Group in the area where the incident occurred. The CCG will, however, still provide the NHS England (Wessex) and (Thames Valley) On Call Director with an overview of the incident and actions being taken.
The NHS England (Wessex) and (Thames Valley) On Call Director will liaise with the
ambulance service and agree the level of response with the CCG or CCGs whose area(s) are directly affected by the incident.
NHS England South will inform NHS England (Wessex) and (Thames Valley) of any incident requiring a regional or national response and Area Team support. In these cases NHS England (South) will liaise with NHS England (Wessex) and (Thames Valley) which will in turn
co-ordinate the response of the NHS in Wessex with the appropriate CCGs.
NHS England (Wessex) On Call Director
Tel. 07623 503 888 (PAGER)
NHS England (Thames Valley) On Call Director
Tel : 07623505519 (PAGER Call sign: NHS 43)
Hold for the operator and leave a message including your name
and contact details
The responsibility of the NHS England (Wessex) and (Thames Valley) On Call Director for ‘cascading’ an alert message will depend on the nature of the message and whether it originates from a provider organisation or the NHS England regional or national offices. 2.9 Declaration of a Major Incident Standby
A major incident declaration may be preceded by the declaration of a major incident standby which is used when the NHS is warned that a major incident may need to be declared. Again this may come from any source and the alerting routes would be the same as in para. 2.4 above.
2.10 NHS Alert Escalation/Incident Levels
Table 1 below describes the 4 broad levels of escalation and provides broad parameters for decision making. These are different to the above National Alert Levels above but the severity of the Major Incident will have differing impacts upon the local health economy. It is the responsibility of the senior manager leading the NHS response at any particular time to decide, in conjunction with colleagues, what level of command is appropriate for the local NHS. The NHS England (Wessex) and (Thames Valley) Area Teams have an Escalation Framework that sets out the procedures across both areas to manage day to day variations in demand across the health and social care system as well as the procedures for managing significant surges in demand. The purpose is to ensure that all partners, health and social care have a mechanism to access additional short term capacity in the right part of the system when demand peaks.
This framework provides a consistent and co-ordinated approach to the management of pressures in NHS England’s (Wessex) and (Thames Valley) acute and emergency care systems, where local escalation triggers have already been applied and yet the pressure on capacity and the need to mitigate against the possibility of compromising patient care, require additional support from other service providers, including those which cross CCG and Area Team boundaries.