Examining Health Information Technology Implementations: Case of the Patient-Centered Medical Home
217
0
0
Full text
Figure
![Figure 3 Chain of logic from resources to rents (adapted from Barney) [127]](https://thumb-us.123doks.com/thumbv2/123dok_us/89882.2510230/55.918.168.737.374.626/figure-chain-logic-resources-rents-adapted-barney.webp)
![Figure 5 Itami classification of assets [142]](https://thumb-us.123doks.com/thumbv2/123dok_us/89882.2510230/64.918.208.710.118.351/figure-itami-classification-of-assets.webp)
+7
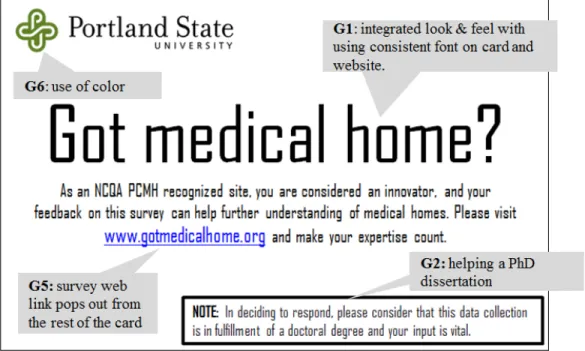
![Table 7 Postcard design goals--adapted from Dillman and Bowker [170]](https://thumb-us.123doks.com/thumbv2/123dok_us/89882.2510230/84.918.152.747.447.876/table-postcard-design-goals-adapted-dillman-bowker.webp)
![Table 8 Fax letter design goals--adapted from Dillman and Bowker [170]](https://thumb-us.123doks.com/thumbv2/123dok_us/89882.2510230/86.918.157.750.435.1046/table-fax-letter-design-goals-adapted-dillman-bowker.webp)
Outline
Related documents