M
ACIEJG
UZIŃSKI1, 2, B
ARBARAH
ENDRICH2, M
AREKS
ĄSIADEK1, 2Embolization of Intracranial Arteriovenous
Malformations – Personal Experience
Embolizacja wewnątrzczaszkowych malformacji tętniczo−żylnych
– doświadczenia własne
1 Department of General Radiology, Interventional Radiology and Neuroradiology, Silesian Piasts University
of Medicine in Wrocław, Poland
2 Marciniak Memorial Hospital, Wrocław, Poland
Adv Clin Exp Med 2008, 17, 1, 69–75 ISSN 1230−025X
ORIGINAL PAPERS
© Copyright by Silesian Piasts University of Medicine in Wrocław
Abstract
Background. Intracranial arteriovenous malformations (AVMs) are among the most frequent developmental abnormalities of brain vessels. The most serious complication of AVM is intracranial hemorrhage. The most often used treatment methods include microsurgical techniques, endovascular embolization, and radiosurgery.
Objectives.The purpose of this study was to analyze own experience in the embolization of brain malformations.
Material and Methods.The material consists of 43 embolizations in 32 patients (19 women and 13 men) aged 17–70 years (mean age: 42 years) between 2002–2006. Intravascular access to the malformations was gained by introducing a microcatheter via the femoral artery and placing its tip in the AVM nidus. Histoacrylic glue obliter− ating the pathological vessels was then administered through the catheter.
Results.In 17 cases the AVMs were located in the left cerebral hemisphere and in 15 cases in the right one. The esti− mated size of the nidus ranged from 10 to 120 mm (mean: 30 mm). The reduction in the size of the nidus during one or more embolization sessions ranged from 10% to 100% (mean: 64%). Complications, including intensification of already existing symptoms or the manifestation of new ones, appeared altogether in five patients, two of whom suf− fered hemorrhage after the embolization and in the three other cases there was probably brain ischemia.
Conclusions.Intravascular embolization of AVMs (one or many sessions) should be an initial method of treating most malformations. Due to the small number of complications and the continuous development of intravascular techniques it seems that embolization could become a leading method in treating arteriovenous brain malforma− tions, especially small and medium−sized ones. It could be used as a single modality or part of multimodal treat− ment (Adv Clin Exp Med 2008, 17, 1, 69–75).
Key words:intracranial arteriovenous malformations, AVM, brain AVM, endovascular embolization.
Streszczenie
Wprowadzenie. Wewnątrzczaszkowe malformacje tętniczo−żylne (AVMs – Intracranial Arteriovenous Malforma− tions) są jednymi z najczęstszych wad rozwojowych naczyń mózgowych. Ich najpoważniejszym powikłaniem są krwawienia wewnątrzczaszkowe. Obecnie jest możliwe leczenie malformacji za pomocą technik mikrochirurgicz− nych, radioterapii celowanej (radiosurgery) lub embolizacji wewnątrznaczyniowej.
Cel pracy. Analiza doświadczeń własnych w embolizacjach malformacji tętniczo−żylnych wewnątrzczaszkowych.
Materiał i metody. Materiał stanowiły 43 embolizacje wewnątrznaczyniowe AVM przeprowadzone u 32 chorych w wieku 17–70 lat (średnio 42 lata) w latach 2002–2006. Podczas zabiegu za pomocą systemu cewników wpro− wadzonych przez tętnicę udową, uzyskiwano dostęp do gniazda naczyniaka i podawano porcje kleju histoakrylo− wego obliterującego patologiczne naczynia.
Wyniki.W 17 przypadkach AVM były umiejscowione w lewej półkuli mózgu, a w 15 – w prawej. Malformacja naj− częściej zajmowała płaty ciemieniowe (u 17 chorych). Wielkość gniazda naczyniaka wynosiła 10–120 mm, średnio około 30 mm. W wyniku embolizacji patologicznych naczyń doprowadzających krew do malformacji uzyskiwano zmniejszenie wielkości gniazda podczas jednej lub wielu sesji o 10–100%, średnio o około 64%. Powikłania w po− staci pogłębienia już istniejących albo pojawienia się nowych objawów ogniskowych wystąpiły u 5 chorych, z cze− go u 2 były spowodowane krwawieniem po zabiegu, a u 3 prawdopodobną przyczyną było niedokrwienie.
Intracranial arteriovenous malformations (AVMs), also known as intracranial arteriovenous angiomas, are among the most frequent develop− mental congenital abnormalities of brain vessels. The incidence of AVMs in the human population is estimated at 0.018–0.6% [1]. The characteristic feature of an AVM is a net of feeding arteries and wide draining veins which communicate directly without intervening capillaries and form the so− called nidus (nest). In a small number of cases, no nidus is present, and these malformations are known as arteriovenous fistulas. It is estimated that up to 90% of AVMs are clinically silent and are diagnosed during autopsy [2]. However, AVMs significantly increase the risk of intracranial hem− orrhage. The occurrence of hemorrhage is the first manifestation of AVM in about half of the patients. Other symptoms include seizures, cluster or migraine headaches, and various focal neurologi− cal symptoms resulting from inadequate blood supply to the brain caused by high flow in the mal− formed vessels (steal syndrome) [3–6]. It is esti− mated that 9% of intracranial hemorrhages and 2% of all strokes are caused by AVMs, and AVM is the most frequent cause of spontaneous hemorrhage in young patients [1, 4]. The risk of recurrent hemor− rhage in the first year is 7% and in subsequent years 3% [7]. Moreover, about 1% of seizures are caused by AVMs [1]. Therefore, diagnosing AVMs and establishing an appropriate treatment is of great importance.
Until the early 1990s the only widely available method of treating an AVM was microsurgery. The development of treatment using embolization and radiotherapy led to a significant change in the ther− apy of AVMs. Currently, the selection of treatment methods is multidirectional and requires neurosur− gical and neuroradiological consultation to estab− lish the best therapy. Factors such as the size and the location of the AVM, age of the patient, and the experience of the center are taken into account. It is usually a multimodal treatment that is applied nowadays: microsurgical resection or radiotherapy is preceded by intravascular embolization. Thanks to embolization it is possible to reduce the size of the malformation in most cases, and sometimes even to obliterate the AVM nidus completely. Intensive development of angiographic techniques (rotation angiography with 3D reconstruction, color intensity projection (CIP), and Dyna−CT, which allows performing CT scans directly on the
angiographic table) together with a minimization of catheter equipment result in much better meth− ods of qualification for intravascular procedures, which in turn allows increased patient safety dur− ing surgery and an assured further development of this method of treatment.
As there is a huge variety of AVMs, an indi− vidual therapy should be established for each and every patient, taking into consideration the pattern of the AVM as well as the clinical state of the patient and the experience of the center. The pur− pose of our study was to analyze own experience in the embolization of brain arteriovenous malfor− mations.
Material and Methods
Between 2002 and 2006, 43 embolizations in 32 patients (19 women and 13 men, age range: 17–70, average age: 42 years) were performed at the Radiology Department of Marciniak Memorial Hospital in Wrocław. All the procedures were pre− ceded by angiographic examination of brain ves− sels and were carried out under general anesthesia. Intravascular access to the malformation was gained by puncture of the femoral artery using the Seldinger method and a diagnostic catheter of a dia− meter of 5–6 French (F). Its distal part was placed in the internal carotid artery or in the vertebral artery. Then 3000 to 5000 units of heparin (70 units per kg) were administered to prevent thrombotic complications. After that, the diagnostic catheter was changed to a guiding catheter, through which a microcatheter with a diameter of 1.2 to 1.8 F was introduced. Before introduction, the tip of the microcatheter was hot−formed in water vapor to adjust its shape to the anatomical conditions of the intracranial arteries. The microcatheter was intro− duced through the guiding catheter using a guide wire and its tip was placed in the AVM’s nidus. Afterwards, superselective digital angiography was carried out to determine the exact localization of the microcatheter tip. When the tip was consid− ered to be placed correctly (only the pathological vessels were opacitied) and after thorough rinsing the lumen of the microcatheter with 5% glucose solution (to prevent intracatheter glue polymeriza− tion), one or two portions of glue which obliterates pathological vessels were administered. We used a mixture of histoacrylic glue (N−Butyl−Cyanoacryl)
wo niewielką liczbę powikłań oraz dalszy rozwój techniki zabiegów wewnątrznaczyniowych wydaje się, że stanie się wiodącą metodą w leczeniu, zwłaszcza małych i średnich malformacji tętniczo−żylnych; zarówno jako metoda samodzielna, jak i skojarzona (Adv Clin Exp Med 2008, 17, 1, 69–75).
and a contrast agent, Lipiodol, in a concentration of 25–40%. The amounts of the mixture applied to the nidus ranged from 0.4 to 1.5 ml. After applica− tion of every portion, a follow−up angiography was performed. Three patients were given two portions of obliterating glue during one session. After all the surgeries the patient’s condition was assessed. Most of the patients (24 of the 32) had one embolization session, 5 needed two sessions of embolization at a few months’ intervals, and three patients needed three sessions.
Results
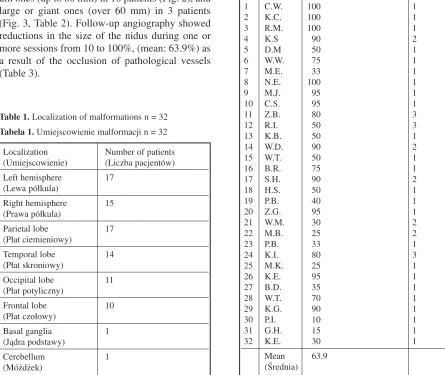
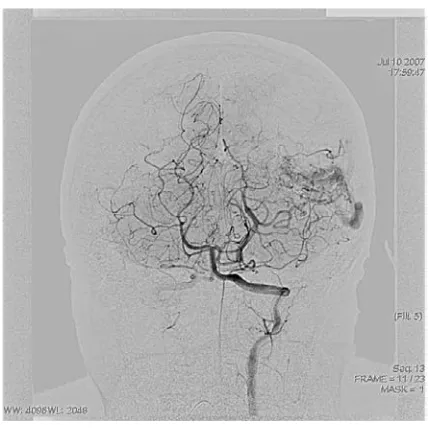
In 17 cases the AVMs were located in the left cerebral hemisphere and in 15 cases in the right. The malformations involved most often the pari− etal lobes (17 patients), followed by the temporal lobes (14 patients), occipital lobes (11), and frontal lobes (10 patients). Some AVMs covered more than one lobe. Few lesions were localized in the basal ganglia and in the cerebellum (Table 1). The size of the nidus ranged from 10 to 120 mm (mean: 30 mm). Small malformations (up to 30 mm) were diagnosed in 13 patients (Fig. 1), medi− um ones (up to 60 mm) in 16 patients (Fig. 2), and large or giant ones (over 60 mm) in 3 patients (Fig. 3, Table 2). Follow−up angiography showed reductions in the size of the nidus during one or more sessions from 10 to 100%, (mean: 63.9%) as a result of the occlusion of pathological vessels (Table 3).
Complications in the form of intensification of previously existing symptoms or the manifestation of new ones appeared altogether in 5 patients, 2 of whom suffered hemorrhage after the embolization procedure (confirmed by CT examination), while in the three other patients the complications were probably caused by ischemia. Two patients showed transient focal symptoms (aphasia and limb paresis), which disappeared during the first or
Table 1. Localization of malformations n = 32
Tabela 1.Umiejscowienie malformacji n = 32 Localization Number of patients (Umiejscowienie) (Liczba pacjentów) Left hemisphere 17
(Lewa półkula)
Right hemisphere 15 (Prawa półkula)
Parietal lobe 17
(Płat ciemieniowy)
Temporal lobe 14
(Płat skroniowy)
Occipital lobe 11
(Płat potyliczny)
Frontal lobe 10
(Płat czołowy)
Basal ganglia 1
(Jądra podstawy)
Cerebellum 1
(Móżdżek)
Table 2. Size of the nidus n = 32
Tabela 2. Rozmiar gniazda n = 32
Size Number of patients
(Rozmiar) (Liczba pacjentów)
< 30 mm 13
< 60 mm 16
> 60 mm 3
Table 3. Percentage value of obliteration of the nidus
Tabela 3.Stopień zamknięcia gniazda w procentach Lp. Patient Percentage of obliteration Number
(Pacjent) after last session of sesions (Stopień zamknięcia (Liczba gniazda po ostatniej sesji) sesji)
1 C.W. 100 1
2 K.C. 100 1
3 R.M. 100 1
4 K.S 90 2
5 D.M 50 1
6 W.W. 75 1
7 M.E. 33 1
8 N.E. 100 1
9 M.J. 95 1
10 C.S. 95 1
11 Z.B. 80 3
12 R.I. 50 3
13 K.B. 50 1
14 W.D. 90 2
15 W.T. 50 1
16 B.R. 75 1
17 S.H. 90 2
18 H.S. 50 1
19 P.B. 40 1
20 Z.G. 95 1
21 W.M. 30 2
22 M.B. 25 2
23 P.B. 33 1
24 K.I. 80 3
25 M.K. 25 1
26 K.E. 95 1
27 B.D. 35 1
28 W.T. 70 1
29 K.G. 90 1
30 P.I. 10 1
31 G.H. 15 1
32 K.E. 30 1
second day after the procedure (Table 4). Strong headaches appeared on the first and second day after embolization, subsiding afterwards. They occurred in 30 of the 32 patients (93.8%).
Discussion
Together with cavernomas, capillary teleang− iectasias, and venous anomalies (developmental venous malformations – DVMs), arteriovenous malformations belong to the group of intracranial vascular malformations. AVMs are further divided into brain malformations of the pia mater, i.e. pial arteriovenous malformations (the so−called angiomas), and malformations of the dura mater, or dural arteriovenous malformations (the so− called fistulas). In our material there were mainly cases of pia mater malformations (26 of the 32 cases), which are categorized according to the Spetzler and Martin Scale. The scale defines the degree of brain damage threat connected with sur− gical removal of the “angioma”. The main factors taken into consideration in this classification are the size of the AVM, its localization, and the type of venous drainage. Additionally, the risk of hem− orrhage from the AVM can be determined accord− ing to the Nataf Scale based on angiography, in which the risk estimation is based on the analysis of venous drainage and possible presence of an aneurysm accompanying the AVM.
The main aim of treating brain arteriovenous malformations is their complete exclusion from the blood circulation, and if that is impossible, a systematic partial reduction of their volume is essential. High morphological and angioarchitec− tural lability is the reason why treatment should be established individually.
With the rapid development of angiographic and catheter equipment, the importance of intravascular techniques in treating vascular mal− formations is consistently increasing. However, as the place of embolization in therapeutic process has not yet been established, different methods are used in different centers. In our center it was assumed that treating all AVMs without hemor− rhage or with a small hemorrhage (not requiring hematoma evacuation) starts with intracranial embolization (most frequently elective) and in the next stages, if necessary, surgical treatment and/or radiotherapy is ordered.
In most of the cases of this study only a part of the malformation was closed during one session, which is associated with a lower risk of evoking hemodynamic disturbance in the brain area involved by the AVM. During one session the application of a large amount of glue can cause
Table. 4.Complications
Tabela 4. Powikłania
Type Form Number of
(Rodzaj) (Forma) patients
(Liczba pacjentów) Focal ischemic lesions de novo 2
(Ogniskowe zmiany exacerbation 1 niedokrwienne)
Haemorrhage SAH 1
(Krwotok) haematoma 1
Transitory paresis 1
(Objawy przejściowe) aphasia 1
Ryc. 1. Small AVM in frontal lobe
Fig. 1.Mała malformacja w płacie czołowym
Ryc. 2. Medium AVM
considerable hemodynamic changes in the brain’s blood circulation, resulting in hemorrhage. It must be remembered that the intravascular polymeriza− tion of histoacrylic glue is an exothermic reaction. Application of larger amounts of glue could cause thermal brain damage [10].
In our center it is assumed that the optimal interval between embolization sessions is 2 to 6 months. A period of this length allows the brain to adjust to the new hemodynamic conditions and the potential “opening” of new pathological vessels, which can be embolized during subsequent ses− sions.
All these procedures were carried out under general anesthesia. Therefore, pre−embolization attempts with the application of barbiturates (amantyl, tiopental) [12] through a microcatheter under local anesthesia provoking neurological dysfunctions were not carried out in our center. In each case of embolization the portion of glue was applied superselectively, only to the pathological vessels. Consequently, the risk of glue reflux and embolization of healthy vessels was minimal. Furthermore, if a procedure lasts a few hours, deep anesthesia is much more comfortable for the patient [10].
According to the literature [1, 3], the most fre− quent clinical manifestation of AVM is intracranial hemorrhage (from 30 to 82%, depending on the source). In the material of the present study, most− ly non−bleeding malformations were embolized. Therefore, the main clinical manifestations in this material were strong headaches and seizures.
Analysis of the localization of the AVMs did not reveal any kind of dominance of any part of the brain lobes. Similarly to the other authors [1], the
majority of malformations analyzed in this study was localized supratentorially. In cases of AVMs with distinctly separated nidus, their volume ranged from 10 mm to 120 mm, but mostly they were not larger than 60 mm. One has to remember that some of the so−called angiomas and most fis− tulas do not have a distinct nidus.
Using embolization the authors managed to reduce (exclude from the blood circulatory sys− tem) the volume of the malformation’s nidus in about 64% of cases (Figs. 4, 5). In the case of multi−session procedures, the final result after the last session was considered. Analyzing the so− called small fistulas and angiomas, occlusion of 90–100% (mean: 93%) of the lesions was con−
Fig. 3.Large AVM
Ryc. 3. Duża malformacja
Fig. 4.Before embolization
Ryc. 4. Przed embolizacją
Fig. 5.After embolization
firmed. In the group of medium AVM (from 30 to 60 mm), the area of the nidus excluded from the blood circulatory system ranged from 30 to 95% (mean: 60%), and in nearly half of the cases there was a need for two or three sessions. The lowest effectiveness of embolization treatment was observed in the group with giant or large AVMs (over 60 mm); the largest reduction in area in this group of patients did not exceed 50% (mean: 33%). It should be emphasized, however, that in patients with medium and large AVM, further embolization sessions are planned which are sup− posed to further reduce the malformation size.
Among the 43 embolizations there were 5 ob− served complications (11.6%). In two cases these were hemorrhagic complications (confirmed in CT) and in the remaining three most probably ischemic ones (CT examination made after the embolization did not show bleeding, and neuro− logical examination indicated focal disturbances). Two patients showed transient neurological deficits (aphasia and limb paresis) which resolved within twenty−four hours after embolization. The etiology of those complications cannot be clearly determined, but according to some authors such symptoms result probably from the reaction after exogenic glue polymerization [10]. The most fre−
quent short−lived side effects after the procedure (within the first 48 hours) were strong headaches, which appeared in 30 of the 32 patients. It must be stressed that the percentage of serious complications (11.6%) did not differ from data other centers more experienced in intravascular treatment [13, 14].
Keeping in mind that the experience of the authors during the first embolizations was not very great, and that most patients were disqualified by neurologists from surgical treatment, the number of complications was relatively small, which pro− vides encouragement for further application of the method.
The authors conclude that intravascular embolization of AVMs should be an initial method of treating most malformations. The most frequent side effects of embolization are strong headaches. Neurological symptoms caused by intracranial hemorrhage or by ischemia are relatively rare. Most malformations require multi−session embolization followed by microsurgery or/and radiotherapy. Due to the small number of compli− cations and the continuous development of intravascular techniques, it seems that emboliza− tion could become a leading method in treating arteriovenous brain malformations, especially small and medium−sized ones.
References
[1] Al−Shahi R, Warlow C:A systematic review of the frequency and prognosis of arteriovenous malformations of the brain in adults. Brain 2000, 10, 1900–1926.
[2] McCormick WF: Classification, pathology, and natural history of angiomas of the central nervous system. Weekly Update Neurol Neurosurg 1978, 14, 2–7.
[3] Mohr J: Arteriovenous Malformations of the Brain in Adults. The Arteriovenous Malformation Study Group. N Engl J Med 1999, 340, 1812–1818.
[4] Al−Shahi R, Bhattacharya JJ, Currie DG, Papanastassiou V, Ritchie V, Roberts RC, Sellar RJ, Warlow CP:
Scottish Intracranial Vascular Malformation Study (SIVMS): evaluation of methods, ICD−10 coding, and poten− tial sources of bias in a prospective, population−based cohort. Stroke 2003, 34, 1156–1162.
[5] Bury A, Bartosz S, Dziki M, Gutkowski K:Olbrzymi naczyniak tętniczo−żylny mózgu u 68−letniego mężczyzny z migrenowymi bólami głowy – opis przypadku. Neurol Neurochir Pol 2005, 39, 6, 514–519.
[6] Berman MF, Sciacca RR, Pile−Spellman J, Stapf C, Connolly ES Jr, Mohr JP, Young WL:The epidemiolo− gy of brain arteriovenous malformations. Neurosurgery 2000, 47, 389–396.
[7] Halim A, Claiborne S, Singh W, McCulloch C, Bennett J, Achrol A, Sidney S, Young W:Longitudinal Risk of Intracranial Hemorrhage in Patients with Arteriovenous Malformation of the Brain Within a defined Population. Stroke 2004, 35, 1697–1702.
[8] Michael J, Tolbert B, Marshall E: Targeting Cerebral Arteriovenous Malformations for Minimally Invasive Therapy. Neurosurgery 2006, 59, 178–183.
[9] Bernd B, Killer S, Monika B, Al−Schameri, Abdul R, Ritter L, Agic R, Krenn M: Therapy of Brain Arteriovenous Malformations: Multimodality Treatment from a Balanced Standpoint. Neurosurgery 2006, 59 148–157.
[10] Intracranial Vascular Malformations and Aneurysms. Ed.: Forsting M. Springer, Berlin 2004, 66–77.
[11] Nataf F, Meder JF, Merienne L, Roux FX, Merland JJ, Chodkiewicz JP: Therapeutic strategy for cerebral arteriovenous malformations. Proposal for classification of individual hemorrhagic risk. Neurochirurgie 1998, 44, 83–93.
[12] Kordecki K, Janica J, Lewszuk A, Kubas B, Kochanowicz J, Kądziołka B, Ząbek M: Endovascular treatment of cerebral arteriovenous malformations. Pol J Radiol 2006, 71, 26–31.
[13] Ledezma CJ, Hoh BL, Carter BS, Pryor JC, Putman CM, Ogilvy CS: Complications of cerebral arteriove− nous malformation embolization: multivariate analysis of predictive factors. Neurosurgery 2006, 58, 602–611.
Address for correspondence:
Marek SąsiadekDepartment of General Radiology,
Interventional Radiology and Neuroradiology ul. Skłodowskiej−Curie 68
50−369 Wroclaw Poland
Tel.: +48 71 784 26 66
E−mail: [email protected]
Conflict of interest: None declared