RESEARCH
Consumer and staff perspectives
of the implementation frequency and value
of recovery and wellbeing oriented practices
Keren E. Wolstencroft
1*, Frank P. Deane
2, Cara L. Jones
3, Adam Zimmermann
4and Merrilee Cox
5Abstract
Background: Despite advances in our understanding of what mental health systems and services can do to enhance recovery and wellbeing outcomes for people seeking support, there is limited evidence demonstrating that this body of work has translated successfully into mental health service practice. The Collaborative Recovery Model (CRM) is a practice framework that has been designed to support application of recovery and wellbeing oriented principles and practices within mental health service delivery. The aims of this study were to assess consumer and staff perceptions of implementation frequency during service engagement and the value of this approach for assisting recovery within a setting where the CRM approach had been adopted.
Methods: The setting was a large Australian community managed mental health organisation. The study involved a cross-sectional analysis of consumer (n= 116) and staff practitioner (n= 62) perspectives. A series of paired sam-ple t-tests assessed for differences between consumer and staff perceptions of the: (i) importance of key practice elements for assisting recovery, and the (ii) frequency that key practice elements are utilised during engagement sessions. Spearman’s r correlational analysis explored associations between importance, frequency and helpfulness of sessions.
Results: Key practice elements of the model were applied during service interactions at a high level and perceived by the majority of consumers and staff participants as being important or very important for assisting recovery. Significant moderate correlations were found between the extent that practice elements were valued and the level at which they were applied. Higher levels of implementation of CRM practices were associated with higher ratings of perceived session helpfulness. The strongest association was between ‘encouragement to set tasks to complete between support visits’ and perceived helpfulness.
Conclusions: Consumer and staff responses revealed that the key practice elements of the CRM were frequently implemented during service engagement interactions and were seen as valuable for assisting recovery. The level of agreement between raters suggests firstly, that the key practice elements were apparent and able to be rated as occurring, and secondly that the CRM approach is seen as responsive to consumer needs. The results have implica-tions for translating recovery and wellbeing oriented knowledge into mental health service practice.
Keywords: Recovery, Wellbeing, Mental health, Service, Practice, Implementation, Translation, Coaching, Training
© The Author(s) 2018. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creat iveco mmons .org/licen ses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creat iveco mmons .org/ publi cdoma in/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Open Access
*Correspondence: [email protected]
1 Neami National, Wollongong, NSW, Australia
Background
The activism, advocacy, and narrative based literature generated by people with a lived experience of mental illness and recovery has driven a transformational shift in how mental health and recovery is understood [1–4]. What has emerged is a wealth of valuable knowledge and guidance for what mental health systems and services can do to enhance recovery and wellbeing outcomes for people seeking support [5–10]. However, there is limited research evidence demonstrating that this substantial body of work has, and can be, translated successfully into mental health service practice [11].
Threaded throughout recovery and wellbeing ori-ented international research and policy literature are two compelling themes fundamental to mental health service practice transformation. Firstly, there is per-suasive evidence and argument for a shift in attention.
That is, mental health services need to broaden their scope of attention beyond illness and symptom allevia-tion, towards that of enhancing health and wellbeing [3,
12–17]. This requires engagement with complexity over reductionism [18], and deliberate attention to what might be possible for a person seeking support in terms of all that pertains to living well [19]. Secondly, there is well established evidence demonstrating the need for a shift in engagement style beyond traditional approaches and positional roles where a person accessing mental health services is seen as a passive recipient of clinical exper-tise [18, 20, 21]. This shift calls for practitioners to inter-act in a manner that is person centred and purposefully relational whilst utilising skills and therapeutic processes that are most likely to facilitate hope, self-empowerment and growth [22–26]. Coaching style practices and princi-ples of co-design have emerged as potential facilitators to support these shifts [27–29].
The strength of this knowledge is evident in the health policy missions and standards for mental health care provision in a growing number of countries [30]. How-ever, translating recovery-oriented policy principles and mandates successfully into mental health service systems and practice has proven to be a persistent challenge [31]. Whilst some of the challenges may be typical to imple-menting evidence based practice in human services in general [32], others are directly related to the nature of the shifts required by recovery and wellbeing oriented approaches [23]. For example, despite extensive efforts to define and translate a broader understanding of recov-ery into practice, it remains conceptually obscured and operationally entangled within the biomedical paradigm [12, 19, 33–37]. Leaders in the field point out that the shifts that are fundamental to recovery and wellbeing approaches require a ‘whole of service’ and systems ori-entation [8, 10, 38].
The development of conceptual frameworks and prac-tice models for services and practitioner staff to draw on represent a potentially valuable step in diminishing this knowledge to practice gap [31]. Training supplemented by ongoing learning opportunities such as coaching and supervision have been found to enhance the uptake of evidence based practice approaches [39, 40]. Further-more, implementation literature in the mental health field also indicates that the degree to which a practice innovation is, (i) championed at the leadership level, (ii) aligned with the values and service operations of an organisation, and (iii) perceived as valuable and relevant by staff and consumers; will influence its uptake and use [41–43].
Aside from well-designed learning and practice devel-opment opportunities, of critical importance to prac-titioner uptake is whether or not an approach is seen as responsive to consumer needs, strengths, personal characteristics and sociocultural context [44]. Posi-tive attitudes towards a practice approach not only increase the likelihood that a consumer will engage with the approach, but also that practitioners will facil-itate their use [45, 46]. At present little is known about the link between the value of recovery and wellbeing approaches and consumer perceptions of mental health care [25]. Thus exploring the connection between the value of an approach and its application is important to understanding the barriers and facilitators to successful implementation.
The Collaborative Recovery Model (CRM) is a person centred and strengths based coaching model [23]. The model translates recovery and wellbeing research and policy literature into overarching principles and key pro-cesses for mental health services and practitioner staff to implement [47]. The knowledge content and therapeu-tic structure are informed by lived experience recovery narrative and evidence based practice and positive psy-chological theories related to change, hope, growth and empowerment processes [4, 7, 48]. The principles and key practice elements are enacted within a coaching-style relationship wherein consumers engage in reflective life visioning and strategic planning processes that are founded on their own aspirations of recovery, wellbeing and/or a good life [23, 49]. The model was piloted and refined by university researchers [7, 42, 50] as part of a National Mental Health and Medical Research Council Strategic Partnership Grant in Mental Health and then adopted by a large Australian community managed men-tal health organisation as a framework to guide service practice in 2009.
health service practice, there is as yet limited literature demonstrating that services and practitioner staff are enacting these in everyday practice [11, 26, 31]. If men-tal health services are to give primacy to improving well-being outcomes for the people they provide support to, then new understandings of what supports people to move from illness to health requires evidence for their translatability to real world service settings and value to the people who use such services [14, 17, 51–53].
This paper presents findings from a large study aimed at exploring implementation fidelity to the Collaborative Recovery Model within an Australian community man-aged mental health organisation, Neami National. Imple-mentation fidelity refers to the extent to which a practice model is being delivered as intended by its designers [54]. Fidelity assessments can measure the presence and strength of an approach as it is used in daily practice, and are fundamental to knowing whether an approach has contributed to intended outcomes [55].
The full study integrated multiple units of analysis— (1) the perceptions of consumers and practitioner staff regarding the importance of the model’s key practice ele-ments for assisting recovery and the frequency by which these are applied, (2) a file audit of consumer support plans to examine whether self-reports of practice appli-cation were consistent with documentary evidence, and, (3) the perceptions of staff across management and non-direct service delivery roles regarding policy and process transformations that have arisen as a result of an organi-sation wide systems approach to implementation of the model.
This paper focuses attention on the first unit of analysis and seeks to answer four questions:
1. Are the key practice elements within the CRM con-sidered important in assisting recovery?
2. To what extent are the key practice elements of the CRM applied during support engagement activities? 3. Is there any relationship between how the key
prac-tice elements of the CRM are valued and the fre-quency by which they are applied?
4. Is there any relationship between the frequency in which the key practice elements are implemented and consumer perceptions of helpfulness of support engagement sessions?
Methods
Design
The method was designed to assess the frequency by which the Collaborative Recovery Model was imple-mented, and its value for assisting recovery, from the viewpoints of consumers and staff receiving and
delivering support framed by this approach. A cross-sectional survey was conducted that assessed the paral-lel between consumer and practitioner staff perceptions. The study was reviewed and approved by University Human Research Ethics. The procedure outlines the pro-tocols implemented with respect to ethical considera-tions relevant to this study.
Procedure
The study was undertaken within an Australian com-munity managed mental health organisation. The organisation is one of the many community managed organisations (also referred to as non-government organ-isations or NGO’s) in Australia that provide support ser-vices to people living with and/or experiencing mental illness and distress. The Australian mental health service sector includes those delivered by government i.e. Pub-lic Health System; those delivered privately e.g. private psychiatrist; and those that are delivered by community managed organisations. Community-managed organi-sations are typically not for profit and deliver supports from a psychosocial framework of care. In Australia the majority of mental health service consumers access men-tal health support through the public and private sectors with approximately 3.1% of psychosocial mental health services expenditure spent in the NGO sector [56].
At the time of the study, the organisation provided sup-port to 3512 consumers and employed 607 staff from 36 service site locations ranging from inner-city and suburbs to regional and remote areas across five states of Aus-tralia. Seven sites were excluded from the study due to service parameters that required non-standard use of the CRM. This included short stay residential services and homelessness outreach services. A proportional random selection process was undertaken to select 12 sites from the remaining 29. Service site participation distribution across states included; Western Australia [1], Queens-land [1], South Australia [2], New South Wales [4] and Victoria [4]. Researchers with a lived experience of men-tal illness and recovery (otherwise named as consumer researchers) were employed in each state to undertake recruitment and data collection activities.
when research activities are undertaken with a consumer researcher [57, 58].
Names of ‘active’ consumers from the 12 sites were extracted from the organisational database, Carelink+, and a randomisation procedure was applied to sort consumer names in ascending order for invitation to participate. Active consumers are those who are cur-rently receiving support as opposed to those who have completed their service engagement or on a wait list to receive support. The extraction of consumer names and the randomisation procedure was undertaken by an employee from the study setting holding custodial responsibility for the collection, management, storage and transmission of all administrative data that is col-lected for service operations across the organisation. In this role the employee has responsibility to implement appropriate physical, technical and ethical safeguards to protect the confidentiality and integrity of organisational data. The funder and the researchers involved this pro-ject had no influence over the list creations and randomi-sation procedure other than providing the parameters related to length of time in service (minimum 3 months) and requirement for participants to be ‘active consumers’ as opposed to no longer receiving services or on a wait-ing list. Sorted lists were provided in Excel spreadsheets directly to consumer researchers and included consumer names, contact details, ID codes for later use and names of staff practitioners who were the key workers for each consumer. Consumer researchers requested site manag-ers advise them about any consummanag-ers currently in hospi-tal. Those names were also omitted from the lists.
Consumer researchers started at the top of the list to contact consumers by phone and invite participation. They introduced themselves to participants as having a lived experience of mental illness and recovery and being employed as a researcher by the service development department of the organisation. After introducing them-selves, they provided verbal information about the study and what participation would involve.
For consumers who indicated interest in knowing more, a meeting time and place was set for the consumer researcher and consumer to discuss the project more fully. Consumers were provided with full information (including written) about the study and what participa-tion would involve, invited to discuss and ask quesparticipa-tions, and offered time to consider and talk to significant oth-ers (e.g. family) about whether or not they would want to participate. Consumer participants were asked to relate back to the researchers their understanding of the nature of the study and what participation involved prior to pro-viding formal and signed consent. Researchers stopped recruitment once participation numbers reached 10 per site. In total 263 consumers were contacted about the
study and 116 (44%) agreed to participate and provided signed consent. One participant withdrew from the study due to a change in their circumstances.
Once a consumer had completed participation in the study, consumer researchers contacted staff members who were identified in the Excel spreadsheet as being the key worker for the participating consumer. After intro-ducing themselves and advising the staff member that a consumer they worked with was involved in the study they provided verbal information about the nature of the study and what participation would involve. If a staff member indicated interest they met with a consumer researcher and were provided with full study and par-ticipation information (including written) and offered time to consider their decision. All staff participants were taken through a formal information and consent process involving signed consent to participate.
Staff participants were the key workers holding pri-mary responsibility for the coordination and delivery of support to the consumer participants in this study. Key workers at this organisation may be responsible for a portfolio of between five and fifteen consumers. There was 65 staff identified on the Excel lists as being key workers to the 116 consumers who participated in the study. Two staff had left the organisation at the time of recruitment and one did not consent to participate. In total, 62 out of 63 staff members invited to participate did so. Staff participants completed separate measures for each consumer participant they were key worker for. As such, staff participants often completed measures in ref-erence to more than one consumer participant.
In all communications between researchers and par-ticipants the voluntary nature of participation was clearly communicated along with options for withdraw-ing consent. All participants were reminded that a deci-sion to not participate would have no impact on their relationship with the organisation of this study setting, on the service they receive (consumer participants) or their employment (staff participants). Participants were informed of protocols to protect participant confiden-tiality including the (1) designation of private rooms or option for alternative location of choice (e.g. private room in local library), (2) use of participant ID no. on all paper based and data-based data with only researcher access to the ID key, (3) all paper-based data stored in locked filing cabinets with only researcher access (4) signed consent forms stored separately to paper-based data responses.
participants. No service delivery staff member had access or knowledge of consumer participant responses. Like-wise no consumer participant had access or knowledge of staff member responses. Information about who did not consent to participate was only known to the consumer researchers involved in this study.
Measures
The Consumer Evaluation of CRM (CEO-CRM) and the Staff Evaluation of CRM (SEO-CRM) are matched self-report questionnaires, developed by university and consumer researchers [45] to assess consumer and staff perspectives on key aspects of support as informed by the Collaborative Recovery Model (CRM). The original version includes 15 items related to seven key practice elements of the model. A consumer review of the meas-ures found high levels of acceptance for use [45]. Reli-ability of the questionnaire was tested as part of previous study and was found to be acceptable (Cronbach’s alpha α = .78 for ‘importance’ items and α = .80 for ‘frequency’ items) [45].
In preparation for this study, we consulted with three consumers, three staff and five consumer researchers to review the measures. Some small adjustments were made to the wording and sequence of the statements including a change in the Likert rating scale for ‘importance’ rat-ings. The option for ‘somewhat important’ was removed because it was considered too similar to ‘moderately important’. After additional consultation with the univer-sity researchers and developers of the CRM, two addi-tional practice elements were also added. These related to values clarification and strengths identification that were not in the original version but considered key prac-tice elements to the CRM. Supplementary files present the CEO-CRM and SEO-CRM measures (see Additional files 1, 2). Table 3 presents the nine key practice elements that form the basis of the modified CEO-CRM and SEO-CRM measures with items 5 and 7 being the additions. The modified CEO-CRM asks consumer participants to firstly provide responses in relation to how personally
important they perceive nine key CRM practice elements as assisting their recovery according to a 4-point Lik-ert scale; 0 = not important, 1 = moderately important, 2 = important, 3 = very important. The measure then asks consumer participants to rate the frequency in which the same nine key practice elements are applied during engagement sessions according to a 5-point Likert scale; 0 = never, 1 = occasionally, 2 = sometimes, 3 = usually, 4 = always. An engagement session is a time designated for a consumer and staff member to meet face to face for the consumer to receive mental health and wellbeing support. Table 1 presents the importance and frequency items. Following completion of importance and frequency
ratings consumer participants are asked to rate how help-ful the sessions with their key worker had been towards assisting their personal recovery process over the past 3 months according to a 4-point Likert scale; 0 = not at all helpful, 1 = moderately helpful, 2 = helpful, 3 = very helpful.
As a matched measure the modified SEO-CRM includes the same nine statements as the CEO-CRM and asks staff participants to refer to an individual con-sumer participant that they are key worker for in their responses. Staff are firstly asked to rate how important
they perceive the nine key practice elements of the CRM are for the individual consumer according to a 4-point Likert scale; 0 = not important, 1 = moderately impor-tant, 2 = important, 3 = very important. Secondly, staff are asked to rate how rate frequently they deliver the nine key practice elements of the CRM during engagement sessions. Upon completion of importance and frequency ratings staff are asked to rate how helpful they perceive the sessions have been towards assisting the consumer participants recovery process over the past 3 months according to a 4-point Likert scale; 0 = not at all helpful, 1 = moderately helpful, 2 = helpful, 3 = very helpful.
Data analysis
As this component was predominantly descriptive the main requirements were to seek a representative sample of consumers achieved through random selection. An estimate of sample size was based on previous research which identified between group differences on compo-nents of the CRM, using the measures used in the current study with a sample size of n of 92 [45]. A series of paired sample t-tests tested for differences between consumer and key worker perceptions of the: (i) importance of key CRM practice elements for assisting recovery, and the (ii) frequency that key CRM practice elements are utilised during engagement sessions. For these comparisons a Bonferroni adjusted p-value of .003 was used. Spearman’s
r correlational analysis was conducted to assess relation-ships between variables.
Results
Demographic profile of participants
Participants of the current study were active consumers (n= 116) and staff practitioners (n= 62) of an Austral-ian community managed mental health service. ‘Active consumers’ refers to consumers who were receiving sup-port at the time of the study as opposed to those who had completed their service engagement or were on a wait list to receive support. Participant demographics are pre-sented in Tables 1 and 2.
participants in this study. Out of the 62 staff participants, 61 had attended 3 day induction training in CRM, 54 had attended at least one CRM 6 month booster, and 48 had attended at least one CRM annual booster. The CRM training programme is intended to enhance and reinforce practitioner staff knowledge, skills and confidence to uti-lise the CRM therapeutic approach. Staff also engage in fortnightly coaching sessions which allow them to discuss consumer progress, and their own personal development within a CRM framework [39].
The importance of key practice elements of the CRM for assisting recovery
Table 3 provides consumer and staff participant mean importance ratings and standard deviation (SD) for each of the key practice elements. A paired t-test revealed that there was no significant difference between the total item means of consumer and staff ratings of importance.
Results indicated that the vast majority of consumer participants rated all key practice elements of the CRM as important in terms of assisting their recovery. The per-centage of consumer ratings in the important and very important range was 87% with a range of (76–91%) across elements. On average, they were rated by consumers as not important 4% of the time (range across elements 0–7%). Staff participant ratings of importance were simi-lar with the percentage of ratings in the important and very important range also being 87% with a range of (70– 96%) across elements.
Paired-sample t-test’s using Bonferroni adjusted alpha levels of .003 were conducted to compare consumer and staff perceptions of importance at the level of indi-vidual items. Results indicated no significant differ-ences between mean ratings of importance for eight out of the nine items. However ‘respect shown for right not to have to take key worker advice’ was regarded more highly by staff participants than consumer participants Table 1 Demographic profile of 116 consumer participants
Characteristics M SD Range
Age 42.9 years 11 years 20–69 years
Characteristics Frequency Percentage (%)
Gender
Female 52 45
Male 64 55
Primary diagnosis
Schizophrenia 48 41
Depression 23 20
Bipolar 16 14
Schizo-affective 13 11
Anxiety 3 3
Other 13 11
Length of time receiving support
Less than 1 year 12 10
1–2 years 53 46
2–3 years 30 26
3–4 years 12 10
5+ years 8 7
Missing 1 1
Language other than english
Yes 14 12
No 89 77
Missing 13 11
Indigenous status
Yes 7 6
No 109 94
Table 2 Demographic profile of 62 staff participants
a Other qualifications spread over seven fields with two or less participants per field
Characteristics M SD Range
Age 37 years 10.8 years 20–63 years
Length of time employed at study setting
2.46 years 2.56 years 1 month to 16 years
Characteristics Frequency Percentage (%)
Gender
Female 37 60
Male 25 40
Cultural and linguistic diversity
Yes 11 18
No 47 76
Missing 4 6
Highest level educational background
Postgraduate 15 24
Undergraduate 24 39
Diploma 20 32
Secondary school 3 5
Qualification field
Social work 10 16
Community welfare 15 24
Counselling 9 15
Psychology 9 15
Sociology 4 6
Othera 12 19
t (107) =− 4.46, p < .001, with a medium effect size, Cohen’s d = .59.
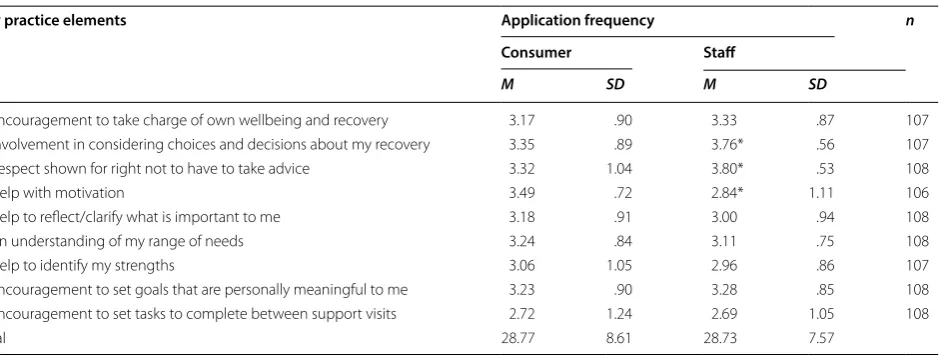
Application frequency of key practice elements of the CRM
Consumer and staff participant mean frequency ratings for each of the key practice elements are presented in Table 4. There were no significant differences between the total item means of consumer and staff ratings of applica-tion frequency. Consumer results showed that key CRM practice elements were perceived as being applied during
support engagement activities with their key worker either usually or always on average 79% of the time (range 62–91%). On average consumers rated the elements as never being applied 2% of the time (range 1–10%). Staff participants rated themselves as applying the key practice elements either usually or always on average 80% of the time (range 58–99%).
Paired-sample t-test’s using Bonferroni adjusted alpha levels of .003 were conducted to compare consumer and staff participant ratings of application frequency at the Table 3 Means and standard deviations for importance ratings of key CRM practice elements
Importance scale: 0 = not at all important, 1 = moderately Important, 2 = important, 3 = very Important n for each item includes the number of paired responses obtained for each item
Total was mean of available items
* Significant difference Bonferroni adjustment p < .003
Key practice elements Importance
Consumer Staff
M SD M SD n
1. Encouragement to take charge of own wellbeing and recovery 2.35 .70 2.43 .75 109
2. Involvement in considering choices and decisions about my recovery 2.49 .62 2.66 .58 109
3. Respect shown for right not to have to take advice 2.22 .74 2.62* .61 108
4. Help with motivation 2.38 .70 2.26 .85 109
5. Help to reflect/clarify what is important to me 2.24 .79 2.42 .70 109
6. An understanding of my range of needs 2.55 .62 2.49 .69 109
7. Help to identify my strengths 2.18 .85 2.38 .74 109
8. Encouragement to set goals that are personally meaningful to me 2.42 .70 2.45 .73 109
9. Encouragement to set tasks to complete between support visits 1.96 .84 1.91 .89 107
Total 20.80 6.67 21.66 6.58
Table 4 Means and standard deviations for application frequency ratings of key CRM practice elements
Frequency scale: 0 = never, 1 = occasionally, 2 = sometimes, 3 = always n for each item includes the number of paired responses obtained for each item Total was mean of available items
*Significant difference Bonferroni adjustment p < .003
Key practice elements Application frequency n
Consumer Staff
M SD M SD
1. Encouragement to take charge of own wellbeing and recovery 3.17 .90 3.33 .87 107
2. Involvement in considering choices and decisions about my recovery 3.35 .89 3.76* .56 107
3. Respect shown for right not to have to take advice 3.32 1.04 3.80* .53 108
4. Help with motivation 3.49 .72 2.84* 1.11 106
5. Help to reflect/clarify what is important to me 3.18 .91 3.00 .94 108
6. An understanding of my range of needs 3.24 .84 3.11 .75 108
7. Help to identify my strengths 3.06 1.05 2.96 .86 107
8. Encouragement to set goals that are personally meaningful to me 3.23 .90 3.28 .85 108
9. Encouragement to set tasks to complete between support visits 2.72 1.24 2.69 1.05 108
individual item level. Results indicated no significant differences between consumer and staff mean ratings of application frequency for six out of the nine items. How-ever, there was a statistically significant difference for the ratings of application for three elements.
The key practice element ‘help with motivation’ was on average rated as being applied more often by consumers than staff rated themselves as applying it t (105) =− 4.94,
p < .00; with a substantial effect size, Cohen’s d = .69. The element ‘involvement in considering choices and deci-sions about my recovery’ was rated as being applied less often by consumers than staff rated themselves as applying it, t (106) =− 4.57, p < .00, with a medium effect size, Cohen’s d = .58; and ‘respect shown for right not to have to take practitioner advice’ was also rated as being applied less often by consumers, than staff rated themselves as applying it, t (107) =− 4.31, p < .00, with a medium effect size, Cohen’s d = .55.
Relationship between how key practice elements
of the CRM are valued and the frequency by which they are applied
Table 5 presents Spearman’s r correlations between con-sumer and staff ratings of overall importance and fre-quency. Significant moderate positive correlations were found between consumer importance and consumer application frequency ratings (r= .50) and between staff importance and staff frequency ratings (r = .49). Small but significant positive correlations were found between staff frequency ratings and consumer importance and frequency ratings (ranges = .20– .25).
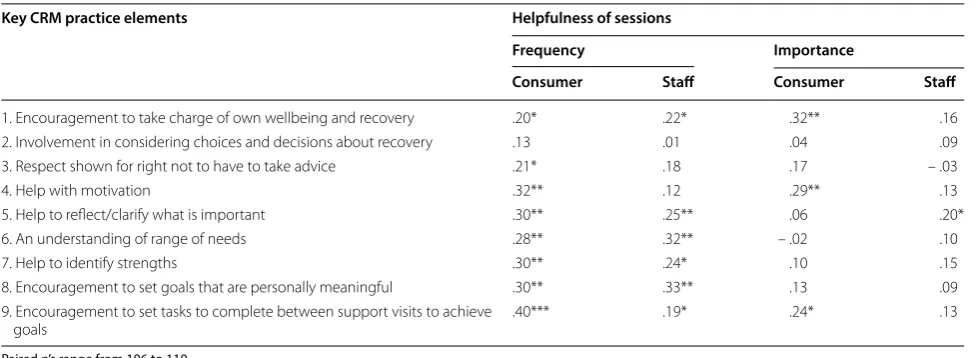
Relationships between the frequency that key practice elements are implemented and perceptions of helpfulness of sessions
Ninety-three percent (n= 103/111) of consumer partici-pants perceived sessions with their key worker as being helpful or very helpful (M= 2.52 out of 3, SD= .60) towards assisting their personal recovery, 5% as moderately helpful
(n= 6/111) and only 2% as not at all helpful (n= 2/111). Staff ratings were lower (M= 2.0, SD= .69) with 76% (n= 84/110) perceiving sessions as being helpful or very helpful and 24% (n= 26/110) as being moderately helpful.
A series of Spearman rank-order correlations found that perceptions of ‘helpfulness of sessions’ were posi-tively associated with CRM implementation frequency. Consumer helpfulness ratings were correlated with con-sumer importance and frequency ratings and staff help-fulness ratings were correlated with staff importance and frequency ratings. For consumers, higher implementa-tion frequency of eight of nine key practice elements showed significant (small to moderate) associations with higher perceptions of helpfulness of sessions. The strong-est association with helpfulness was for ‘encouragement to set tasks to complete between support visits’. For staff, significant albeit small associations were found between higher implementation of six of the nine key practice elements with higher perceptions of helpfulness. There was a greater proportion of items showing associations between application frequency and helpfulness, than that of importance and helpfulness. Table 6 presents the cor-relation coefficients between (1) importance of practice elements and helpfulness of sessions, and (2) implemen-tation frequency and helpfulness of sessions for consum-ers and staff.
Discussion
Importance
The Collaborative Recovery Model (CRM) promotes con-sumer and staff engagement with an individualised and holistic approach to recovery and wellbeing [23]. Results for the first question revealed that the key practice ele-ments of the CRM were valued at a high level by the majority of consumers (87%) and staff (87%) participants for supporting recovery. The results validate the design of the model as being responsive to consumer needs [44] and align with consumer narrative and recovery literature
Table 5 Spearman’s r correlations between consumer and staff participant importance, frequency and helpfulness ratings
Listwise n= 106
*p < .05 1-tailed **p < .01 1-tailed
Consumer
importance Consumer frequency Consumer helpfulness Staff importance Staff frequency
Consumer frequency .51** –
Consumer helpfulness .24** .39** –
Staff importance .17* .20* .05 –
Staff frequency 20* .25** .04 .49** –
calling for mental health services to move beyond symp-tom alleviation [4, 12, 15].
At the individual item level, results indicated no signifi-cant differences between consumer and staff perceptions of importance for eight out of the nine key practice ele-ments. However, for one item; ‘involvement in consider-ing choices and decisions about recovery’, it was found that although consumer ratings of importance for this were high (M = 2.49 out of 3) staff ratings were higher (M = 2.66 out of 3). Central to the concept of empower-ment is a person having the opportunity to voice their ideas, opinions and concerns [24]. This finding may indi-cate that when consumers experience this element as business as usual, they may not perceive its value at the same level as staff who receive CRM training which spe-cifically highlights the history of consumer disempower-ment and the crucial role of consumer involvedisempower-ment in decision making towards recovery and wellbeing.
Frequency
For the second question, the majority of consumers (79%) and staff (80%) rated the key practice elements as being applied during service interactions, as either usually or always. There was no significant difference between the total item means between consumers and staff. This rep-resents a substantial agreement between consumer and staff perceptions of application and suggests implemen-tation of the model is detectable and able to be rated as occurring. The model’s use of applied positive psychology constructs, such as cultivating a growth mindset and a focus on values and strengths, provides a framework for translation at the organisational, staff and consumer lev-els [23].
A component of the model that may have contributed to these results is the expanded use of the ‘parallel pro-cess’ [59]. Further to formal training and booster sessions staff practitioners engage in regular coaching, wherein they use exactly the same protocols that they are asked to use with consumers, for their own professional develop-ment or personal growth [39, 59]. Aside from developing skills and confidence to use the protocols in their work with consumers, staff are exposed to the tensions and rewards inherent to these processes [59]. There is also an implicitly normalising rationale to this process that con-firms that people with mental health difficulties are fun-damentally the same as anyone else; that is, everyone has strengths, values, needs and aspirations [23]. Research examining the translation of evidence-based practices, has found that providing staff with ongoing coaching in a practice approach promotes implementation [40]. In the current study, it is possible that providing training in the CRM that was supplemented with ongoing ‘parallel pro-cess’ coaching may have contributed to the level of imple-mentation [39].
Paired-sample t-test’s comparing consumer and staff application frequency ratings at the individual item level revealed no significant difference between consumer and staff perceptions of application frequency for six out of the nine elements. However, there was a dispar-ity between consumer and staff reports for the applica-tion of three elements. Firstly, ‘help with motivaapplica-tion’ was on average perceived by consumers as being applied more frequently during engagement interactions than staff rated themselves as applying it. For practitioners implementing the CRM approach, the ability to engage in discussions and activities that enhance and maintain Table 6 Correlation coefficients between importance and implementation of CRM practice elements with helpfulness of sessions
Paired n’s range from 106 to 110 * p < .05, **p < .01, ***p < .001
Key CRM practice elements Helpfulness of sessions
Frequency Importance
Consumer Staff Consumer Staff
1. Encouragement to take charge of own wellbeing and recovery .20* .22* .32** .16
2. Involvement in considering choices and decisions about recovery .13 .01 .04 .09
3. Respect shown for right not to have to take advice .21* .18 .17 – .03
4. Help with motivation .32** .12 .29** .13
5. Help to reflect/clarify what is important .30** .25** .06 .20*
6. An understanding of range of needs .28** .32** – .02 .10
7. Help to identify strengths .30** .24* .10 .15
8. Encouragement to set goals that are personally meaningful .30** .33** .13 .09
9. Encouragement to set tasks to complete between support visits to achieve
motivation, are supported through ongoing training. The content of training includes theoretical concepts emerg-ing from the recovery literature and align with knowl-edge from the positive psychology and wellbeing sciences pertaining to hope, change and growth [48]. Practitioner skill to utilise these concepts during engagement inter-actions is facilitated through development of coaching and motivational interviewing skills [23]. The dispar-ity in findings indicate that the application of ‘help with motivation’ may be experienced differently by consum-ers than staff. It is possible that staff predominantly per-ceive their application of this element as tied to the use of coaching and motivational interviewing skills, whereas consumer perceptions may be formed by a more global sense of ‘help with motivation’ that arises from all aspects of the interaction. This interpretation aligns with litera-ture and evidence for the value of the therapeutic alliance to consumer engagement and satisfaction with a practice approach [18, 25, 60].
The key practice elements ‘involvement in considering choices and decisions about my recovery’ and ‘respect shown for right not to have to take staff advice’ were rated on average by consumers as being applied less often than staff rated themselves as applying it. Although con-sumer application rating means for these items were high (M= 3.35 and M= 3.32 out of 4), staff ratings were signif-icantly higher (M= 3.76 and M= 3.80 out of 4). This dis-parity may indicate a bias on the part of practitioner staff ratings, which is common to practitioner self-reports of adherence to a practice approach [54]. However the find-ing that consumer ratfind-ings were also high suggests that both groups viewed these elements as being frequently applied.
Relationship between importance and frequency
For the third question, perceptions of importance of prac-tice elements of the CRM were related to the frequency that consumers and staff practitioners report such prac-tices are engaged in during support sessions. This find-ing is congruent with existfind-ing research that has found that positive attitudes about the value of an evidence base practice not only increase the likelihood that a consumer will engage in the approach, but also that practitioners will be more likely to implement an approach [44–46].
Relationship between importance, frequency, and helpfulness of sessions
Though the primary goal of this component of study was to assess the implementation and value of key prac-tice elements of the model, we found meaningful vari-ability when ratings of overall ‘helpfulness of sessions to assist recovery’ were added to the analysis. Initial analy-sis revealed that the majority (93%) of consumers rated
the sessions with staff practitioners as being helpful or very helpful towards assisting recovery. Staff perceptions about helpfulness of sessions were somewhat lower with 76% rating sessions at the helpful or very helpful level and 24% at the moderately helpful level.
Correlations revealed that perceptions of helpful-ness of sessions were related to the frequency that the key practice elements were applied, both at the indi-vidual item level and the total scale level. Higher ratings of CRM application were associated with higher levels of perceived helpfulness of sessions to assist recovery. The implementation of ‘encouragement to set tasks to complete between support visits to achieve own goals’ demonstrated the strongest association (r= .40) with consumer perceptions of helpfulness of sessions to assist recovery. This finding stands in contrast to other findings from this study where task setting was perceived as least important and the least frequently implemented element.
Encouragement to set tasks refers to a process whereby staff and consumers collaborate to break down a goal into individual actions and strategies for a consumer to com-plete between support contacts. The actions and their associated goals are then reviewed at follow-up engage-ment sessions. The process is informed by research on health behaviour change and therapeutic homework; and functions to improve self-management, self-mon-itoring and self-efficacy [48]. Task setting activities in this study were rated as least important but the correla-tions between how frequently this activity was engaged in had the highest correlation with session helpfulness. It is unlikely that respondents were aware of the relation-ship between task setting frequency and perceptions of helpfulness. Had they been, it is possible that respond-ents might have rated its importance higher. Regardless of perceptions of value, the strength of association found in this study adds to findings in previous studies that task setting is positively related to improved outcomes [61]. There is need for services to highlight the importance of these action planning components and to increase atten-tion to implementaatten-tion of this component.
positive therapeutic alliance as being central to a service practice, staff may not link the experience of receiving support framed in this manner to ‘help with motivation’. For people accessing mental health services, the connec-tion, support and safety of a trusting relationship with a practitioner who is personally invested in them and dem-onstrates respectful curiosity can act as a stepping stone for recovery [25]. In this study, consumer reports indicate that staff appear to deliver components of CRM that help with motivation at a high level, yet staff may underesti-mate the source and value of this experience to people who use the service.
Strengths and limitations
The focus of this study is important in terms of advanc-ing knowledge and evidence for the translation of recov-ery and wellbeing oriented approaches into mental health service practice. The use of matched measures to exam-ine consumer and staff perspectives provide comparison points to substantiate findings. A clear limitation of this study is that it utilised a measure with relatively limited psychometric testing. Whilst preliminary reliability and face validity has been found, further testing is required [45] and therefore results should be interpreted with caution. Furthermore, the measure used in the current study was designed to balance existing validity with what was reasonably practical to use in a mental health set-ting. The measure may not have captured the full extent or the complexity of CRM principles and practices. This may limit the effectiveness of the measure to provide a comprehensive evaluation of implementation and value [54]. A common limitation of self-report measures is the potential for bias. For this study, the use of matched measures and the involvement of consumer researchers was included to minimise bias.
In total 116 consumers and 62 staff participated in this study. However, sample sizes ranged from 106 to 111 due to missing data and represent a percentage loss of between 4.3 and 8.6%. Three consumer participants did not have ‘matched data’ due to one staff member declin-ing to participate and two bedeclin-ing unavailable to participate having left employment at the study setting. Additional missing data may be the result of data entry error or items not responded to by participants. As such, this may have had an effect on the results.
The study was descriptive and correlational so causal explanations cannot be made. Implementation litera-ture has demonstrated that a complex variety of factors, at different levels, interact and contribute to whether or a not mental health practice approach is translated into service delivery practice [32]. Given the extensive evidence for translational challenges the developers and researchers sought to firstly assess the feasibility of
implementation within one setting. This study provides an indication that the key practice elements of the model were detected as being implemented by consumers and staff. There is a need to extend this enquiry by explor-ing whether or not the same results would be achieved in other settings. In particular, it is important to know whether settings that are more traditionally clinically oriented are able to obtain similar results. Furthermore, without a comparison cohort it is impossible to deter-mine whether the results would be any different to that in any other service setting context where the CRM has not been implemented. However, prior research using equivalent measures have demonstrated differences in perceptions of those receiving CRM framed support and those not receiving CRM [45]. What the current study adds, are staff perspectives to further verify these find-ings and extended this to an organisation that has been implementing CRM and associated coaching programs over 5+ years.
The response rate (44%) for consumer participation in this study was relatively low and may impact on the reli-ability of the results. There is a chance that consumers who chose to participate were those more satisfied with the service. However steps were taken in the recruit-ment procedure to limit such bias, which may also have impacted the response rates. Firstly, recruitment for this study was undertaken by consumer researchers without any previous relationship with the consumers contacted for potential participation. Recruitment rates may have been higher if consumers had been recruited by staff practitioners with whom they had existing relationships. However, in order to minimise perceptions of coercion and limit bias the study involved consumer researchers to invite participants. Secondly, recruitment to participate in mental health research is often influenced by clinician decision making as to whether a person is deemed suit-able (in terms of situational and mental health readiness). In this study we sought to limit clinician decision mak-ing and optimise consumer choice for optmak-ing in or out of participation [62]. Given the time and commitment involved in participation there is the potential that con-sumers with more obstacles may have chosen not to par-ticipate. By offering a financial incentive at recruitment, consumer participants may have been more willing to overcome obstacles to participate and/or may have been more willing to believe that their participation would be of value.
Implications for mental health services field
worked closely with real world mental health service set-tings and consumers to develop and refine the model for use in everyday practice [7, 23, 63]. This involved devel-opment and testing of methods and processes to improve practitioner uptake and sustainability of practice over time [31, 39, 42, 45, 63, 64]. Complementing this work, at the service practice level; organisational readiness for change, leadership practices, and adoption of the model as a ‘whole of organisation; systems, policies and practice approach’, may have contributed to the perceptions of high implementation reflected in the results of this study.
Conclusions
Translating recovery-oriented knowledge into mental health service systems and practice has proven to be a persistent challenge [32]. Assessing implementation can provide critical knowledge to address research to prac-tice gaps and inform translation pracprac-tices [65]. This paper presents a unit of analysis within a wider study aimed at assessing fidelity to the Collaborative Recovery Model within an Australian community managed mental health organisation. Perceptions of consumers and staff were examined regarding the value and implementation of key practice elements that are considered to reflect the mod-el’s theoretical underpinnings and therapeutic structure.
Findings revealed that the key practice elements were perceived as being applied during service interactions at a high level and perceived by consumers and staff as being valuable for assisting recovery. There was a substantial level of agreement between consumer and staff percep-tions of value and application frequency indicating vis-ibility and positive engagement with the CRM approach in the study context. Congruent with existing research, higher perceptions of value were found to be associated with higher levels of implementation, strengthening the proposition that positive attitudes about the value of an approach can increase the likelihood of consumer engagement and staff uptake [44–46]. Variability between consumer and staff perceptions found at the individual item level highlighted areas for attention that can impact on the helpfulness of sessions to assist with recovery.
By combining recovery knowledge and policy with practices known to enhance mental health and wellbe-ing, along with a coaching orientation and organisa-tional change principles, the CRM framework may offer a practical solution for mental health services to trans-late recovery policy into practice [48]. Further attention to the complementary nature of recovery knowledge and positive psychology and wellbeing approaches may serve to advance a whole of systems orientation to practices shown to enhance mental health and wellbeing.
Additional files
Additional file 1. CEO-CRM Consumer Evaluation of CRM. Additional file 2. SEO-CRM Staff Evaluation of CRM.
Abbreviations
CRM: Collaborative Recovery Model; CEO-CRM: Consumer Evaluation of CRM; SEO-CRM: Staff Evaluation of CRM; ID: identification.
Authors’ contributions
AZ, MC, KW and FD contributed to the conceptualisation and design of this study. AZ recruited and trained the lived experience researchers and sup-ported them to engage with service sites. AZ and KW assisted with implemen-tation of research activities in the study context. FD guided and undertook the statistical analysis and interpretation. KW assisted with interpretation. CJ contributed to data analysis and interpretation. All authors contributed to the manuscript. All authors read and approved the final manuscript.
Author details
1 Neami National, Wollongong, NSW, Australia. 2 Illawarra Institute for Mental
Health, School of Psychology, University of Wollongong, Wollongong, NSW, Australia. 3 School of Psychology, University of Wollongong, Wollongong, NSW,
Australia. 4 KPMG Australia Services Pty Ltd., Melbourne, Australia. 5 Mental
Health Association of Central Australia, Alice Springs, NT, Australia.
Acknowledgements
This study was made possible through the support and cooperation of service development and direct support staff across the community managed mental health organisation that was the setting for this study. We would also like to acknowledge the input of consumers and lived experience researchers into the design of data collection protocols and measures used in this study.
Competing interests
At the time that this research was conducted KW, AZ and MC were all employed by Neami National which funded this study. FD was employed by the University of Wollongong which provided an exclusive license for Neami National to deliver training in CRM. There is no competing interests between MC and AZ’s current employment and completion of the study. KW is cur-rently employed by Neami National. All analyses reported in this paper were undertaken by FD and CJ independently.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available to comply with University of Wollongong Ethics policy but are available from the corresponding author on reasonable request and HREC application. The measures used in this study are included in the Additional files 1 and 2.
Consent for publication
All participants provided informed consent for publication. No individual patient data is published in this manuscript.
Ethics approval and consent to participate
This research was granted human research ethics approval by the University of Wollongong Human Research Ethics Committee—Reference Number HE13/335. All participants involved in this study provided informed consent to participate.
Funding
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in pub-lished maps and institutional affiliations.
Received: 18 April 2018 Accepted: 15 October 2018
References
1. Piat M, Sabetti J. The development of a recovery-oriented mental health system in Canada: what the experience of commonwealth countries tells us. Can J Community Ment Health. 2009;28(2):17–33.
2. Slade M, Amering M, Oades L. Recovery: an international perspective. Epidemiol Psichiatr Soc. 2008;17(2):128–37.
3. Amering M, Schmolke M. Recovery in mental health: reshaping scientific and clinical responsibilities. Herrman H, editor. Hoboken: Wiley-Blackwell; 2009.
4. Andresen R, Oades L, Caputi P. The experience of recovery from schizophrenia: towards an empirically validated stage model. Aust N Z J Psychiatry. 2003;37:586–94.
5. Le Boutillier C, Leamy M, Bird VJ, Davidson L, Willams J, Slade M. What does recovery mean in practice? A qualitative analysis of international recovery-oriented practice guidance. Psychiatr Serv. 2011;62(12):1470–6. 6. Farkas M, Gagne C, Anthony W, Chamberlin J. Implementing recovery
oriented evidence based programs: identifying the critical dimensions. Community Ment Health J. 2005;41(2):18.
7. Oades LG, Deane FP, Crowe TP, Lambert WG, Kavanagh D, Lloyd C. Col-laborative recovery: an integrative model for working with individuals who experience chronic and recurring mental illness. Aust Psychiatry. 2005;13(3):279–84.
8. Slade M, Amering M, Farkas M, Hamilton B, O’Hagan M, Panther G, et al. Uses and abuses of recovery: implementing recovery-oriented practices in mental health systems. World Psychiatry. 2014;13(1):12–20.
9. Shepherd G, Boardman J, Slade M. Making recovery a reality. Sainsbury Centre for Mental Health. 2007. https ://www.centr eform ental healt h.org. uk/sites /defau lt/files /2018-09/Makin g%20rec overy %20a%20rea lity%20 pol icy%20pap er.pdf. Accessed 8 Aug 2017.
10. Oades L, Mossman L. The science of wellbeing and positive recovery. In: Slade M, Oades LG, Jarden A, editors. Wellbeing, recovery and mental health. Cambridge: Cambridge University Press; 2017. p. 7–23. 11. Piat M, Sofouli E, Sabetti J, Lambrou A, Chodos H, Briand C, et al. Protocol
for mixed studies systematic review on the implementation of the recov-ery approach in mental health services. BMJ Open. 2017;7(8):1–7. 12. Morera T, Pratt D, Bucci S. Staff views about psychosocial aspects of
recovery in psychosis: a systematic review. Psychol Psychother Theor Res Pract. 2017;90(1):1–24.
13. Resnick SG, Rosenheck RA. Recovery and positive psychology: parallel themes and potential synergies. Psychiatr Serv. 2006;57(1):120–2. 14. Keyes CL. Promoting and protecting mental health as flourishing: a
com-plementary strategy for improving national mental health. Am Psychol. 2007;62(2):95–108.
15. Clark S, Oades LG, Crowe TP. Recovery in mental health: a movement towards well-being and meaning in contrast to an avoidance of symp-toms. Psychiatr Rehabil J. 2012;35(4):297–304.
16. Linley PA, Joseph S, Harrington S, Wood AM. Positive psychology: past, present, and (possible) future. J Posit Psychol. 2006;1(1):3–16.
17. Slade M. Mental illness and well-being: the central importance of positive psychology and recovery approaches. BMC Health Serv Res. 2010;10:26. 18. Bracken P, Thomas P, Timimi S, Asen E, Behr G, Beuster C. Psychiatry
beyond the current paradigm. Br J Psychiatry. 2012;201:430–4. 19. Slade M, Oades L, Jarden A. Why wellbeing and recovery? In: Slade M,
Oades LG, Jarden A, editors. Wellbeing, recovery and mental health. Cambridge: Cambridge University Press; 2017. p. 1–6.
20. Jacob S, Munro I, Taylor BJ, Griffiths D. Mental health recovery: a review of the peer-reviewed published literature. Collegian. 2017;24(1):53–61. 21. Deegan PE. Spirit breaking: when the helping professions hurt. Humanist
Psychol. 1990;18(3):301–13.
22. Mancini AD. Self-determination theory: a framework for the recovery paradigm. Adv Psychiatr Treat. 2008;14(5):358–65.
23. Oades L, Crowe T, Nguyen M. Leadership coaching transforming mental health systems from the inside out: the Collaborative Recovery Model as person-centred strengths based coaching psychology. Int Coach Psychol Rev. 2009;4(1):25–36.
24. Baumann A. Statement on the meaning of empowerment of mental health service users and carers. In: Health W-EPPoUEiM, editor. Copenha-gen: WHO Regional Office for Europe; 2010.
25. O’Keeffe D, Sheridan A, Kelly A, Doyle R, Madigan K, Lawlor E, et al. ‘Recov-ery’ in the real world: service user experiences of mental health service use and recommendations for change 20 years on from a first episode psychosis. Administration and policy in mental health and mental health services research. 2018.
26. Leamy M, Bird V, Boutillier C, Williams J, Slade M. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis. Br J Psychiatry. 2011;199:445–52.
27. Bora R, Leaning S, Moores A, Roberts G. Life coaching for mental health recovery: the emerging practice of recovery coaching. Adv Psychiatr Treat. 2010;16(6):459–67.
28. Oades L, Anderson J. Recovery in Australia: marshalling strengths and living values. Int Rev Psychiatry. 2012;24(1):5–10.
29. Fairhurst K, Weavell W. Co-designing mental health services—providers, consumers and carers working together. New Paradigm. 2011;54:5. 30. Ellison ML, Belanger LK, Niles BL, Evans LC, Bauer MS. Explication and
definition of mental health recovery: a systematic review. Adm Policy Ment Health. 2018;45(1):91–102.
31. Williams VC, Deane FP, Oades LG, Crowe TP, Ciarrochi J, Andresen R. Enhancing recovery orientation within mental health services: expanding the utility of values. J Ment Health Train Educ Pract. 2016;11(1):23–32. 32. Tansella M, Thornicroft G. Implementation science: understanding the
translation of evidence into practice. Br J Psychiatry. 2009;195:283–5. 33. Le Boutillier C, Chevalier A, Lawrence V, Leamy M, Bird V, Macpherson R,
et al. Staff understanding of recovery-orientated mental health practice: a systematic review and narrative synthesis. Implement Sci. 2015;10(1):87. 34. Davidson L, Roe D. Recovery from versus recovery in serious mental
illness: one strategy for lessening confusion plaguing recovery. J Ment Health. 2007;16(4):459–70.
35. Shanks V, Williams J, Leamy M, Bird VJ, Le Boutillier C, Slade M. Measures of personal recovery. Psychiatr Serv. 2013;64(10):974–80.
36. Burgess P, Pirkis J, Coombes T, Rosen A. Assessing the value of existing recovery measures for routine use in Australian mental health services. Aust N Z J Psychiatry. 2011;45(4):267–80.
37. Davidson L, O’Connell MJ, Tondora J, Lawless M, Evans AC. Recovery in serious mental illness: a new wine or just a new bottle? Prof Psychol Res Pract. 2005;36(5):480–7.
38. Bellack AS, Drapalski AMY. Issues and developments on the consumer recovery construct. World Psychiatry. 2012;11(3):156–60.
39. Deane F, Andresen R, Crowe T, Oades L, Ciarrochi J, Williams V. A compari-son of two coaching approaches to enhance implementation of a recov-ery-oriented service model. Adm Policy Ment Health. 2013;41(5):660–7. 40. Kretlow AG, Bartholomew CC. Using coaching to improve the fidelity of
evidence-based practices: a review of studies. Teach Educ Spec Educ. 2010;33(4):279–99.
41. Aarons GA, Hurlburt M, Horwitz SM. Advancing a conceptual model of evidence-based practice implementation in public service sectors. Adm Policy Ment Health. 2011;38(1):4–23.
42. Deane FP, Crowe TP, King R, Kavanagh DJ, Oades LG. Challenges in implementing evidence-based practice into mental health services. Aust Health Rev. 2006;30(3):305–9.
43. Gilburt H, Slade M, Bird VJ, Oduola S, Craig T. Promoting recovery-oriented practice in mental health services: a quasi-experimental mixed-methods study. BMC Psychiatry. 2013;13:167.
44. Prendergast ML. Issues in defining and applying evidence-based prac-tices criteria for treatment of criminal-justice involved clients. J Psychoac-tive Drugs. 2011;43(Suppl 7):10–8.
45. Marshall S, Oades L, Crowe T. Mental health consumers’ perceptions of receiving recovery-focused services. J Eval Clin Pract. 2009;15(4):654–9. 46. Pagoto SL, Spring B, Coups EJ, Mulvaney S, Coutu M-F, Ozakinci G. Barriers
and facilitators of evidence-based practice perceived by behavioral sci-ence health professionals. J Clin Psychol. 2007;63(7):695–705. 47. Oades L, Deane F, Crowe T. The Collaborative Recovery Model: positive
•fast, convenient online submission
•
thorough peer review by experienced researchers in your field
• rapid publication on acceptance
• support for research data, including large and complex data types
•
gold Open Access which fosters wider collaboration and increased citations maximum visibility for your research: over 100M website views per year
•
At BMC, research is always in progress.
Learn more biomedcentral.com/submissions
Ready to submit your research? Choose BMC and benefit from:
in enduring mental illness. In: Boniwell I, David S, editors. Oxford hand-book of happiness. Oxford: Oxford University Press; 2013. p. 1050–66. 48. Oades LG, Deane FP, Crowe TP. Collaborative Recovery Model: from
mental health recovery to wellbeing. In: Slade M, Oades L, Jarden A, editors. Wellbeing, recovery and mental health. Cambridge: Cambridge University Press; 2017. p. 99.
49. Oades L, Crowe T, Deane F. Life Journey Enhancement Tools (LifeJET). Illawarra Institute for Mental Health Research Online - University of Wol-longong. 2008. https ://ro.uow.edu.au/cgi/viewc onten t.cgi?refer er=https ://www.googl e.com.au/&https redir =1&artic le=1140&conte xt=hbspa pers. Accessed 13 Dec 2017.
50. Crowe T, Deane F, Oades L, Caputi P, Morland K. Effectiveness of a collabo-rative recovery training program in Australia in promoting positive views about recovery. Psychiatr Serv. 2006;57(10):1497–500.
51. Piat M, Briand C, Bates E, Labonté L. Recovery communities of practice: an innovative strategy for mental health system transformation. Psychiatr Serv. 2016;67(1):10–2.
52. Slade M, Williams J, Bird V, Leamy M, Le Boutillier C. Recovery grows up. J Ment Health. 2012;21(2):99–104.
53. Roberts G, Boardman J. Becoming a recovery-oriented practitioner. Adv Psychiatr Treat. 2014;20(1):37–47.
54. Mowbray C. Fidelity criteria: development, measurement, and validation. Am J Eval. 2003;24(3):315–40.
55. Breitenstein SM, Gross D, Garvey CA, Hill C, Fogg L, Resnick B. Imple-mentation fidelity in community-based interventions. Res Nurs Health. 2010;33(2):164–73.
56. Department of Health and Aging. National Mental Health Report 2013: tracking progress of mental health reform in Australia 1993–2011. Can-berra: Commonwealth of Australia; 2013.
57. Hancock N, Bundy A, Tamsett S, McMahon M. Participation of mental health consumers in research: training addressed and reliability assessed. Aust Occup Ther J. 2012;59(3):218–24.
58. Oades LG, Law J, Marshall SL. Development of a consumer constructed scale to evaluate mental health service provision. J Eval Clin Pract. 2011;17(6):1102–7.
59. Crowe TP, Deane LG, Ciarrochi J, Williams VC. Parallel processes in clinical supervision: implications for coaching mental health practitioners. Int J Evid Based Coach Ment Health Pract. 2011;9(2):56–66.
60. Deane F, Crowe T. Building and maintaining a recovery focused thera-peutic relationship. In: King R, Loyd C, Meehan T, editors. Handbook of psychosocial rehabilitation. Victoria: Blackwell Publishing Ltd; 2007. p. 57–70.
61. Kelly PJ, Deane FP. Relationship between therapeutic homework and clinical outcomes for individuals with severe mental illness. Aust N Z J Psychiatry. 2009;43:968–75.
62. Pinfold V, Cotney J, Hamilton S, Weeks C, Corker E, Evans-Lacko S, et al. Improving recruitment to healthcare research studies: clinician judgements explored for opting mental health service users out of the time to change viewpoint survey. J Ment Health. 2017. https ://doi. org/10.1080/09638 237.2017.13405 98.
63. Marshall S, Oades L, Crowe T. Australian mental health consumers’ contri-butions to the evaluation and improvement of recovery-oriented service provision. Isr J Psychiatry Relat Sci. 2010;47(3):198–205.
64. Uppal S, Oades LG, Crowe TP, Deane FP. Barriers to transfer of collabora-tive recovery training into Australian mental health services: implica-tions for the development of evidence-based services. J Eval Clin Pract. 2010;16(3):451–5.