ARTICLE
Effects of Maternal Multimicronutrient
Supplementation on the Mental Development of
Infants in Rural Western China: Follow-up Evaluation
of a Double-Blind, Randomized, Controlled Trial
Qiang Li, MSca,b, Hong Yan, MSca, Lingxia Zeng, MSca, Yue Cheng, MSca, Weifeng Liang, MSca, Shaonong Dang, PhDa, Quanli Wang, MSca,
Ichiro Tsuji, MD, PhDb
aDivision of Epidemiology and Biostatistics, Department of Public Health, Xi’an Jiaotong University School of Medicine, Xi’an, China;bDivision of Epidemiology,
Department of Public Health and Forensic Medicine, Tohoku University Graduate School of Medicine, Sendai, Japan
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
Evidence shows that multimicronutrient supplementation during pregnancy can in-crease birth weights, prolong gestational periods, and dein-crease early infant mortality rates. However, the effects on the functional outcomes of infants remain unclear.
What This Study Adds
We found that multimicronutrient supplementation was associated with significant improvement in the MD of infants at 1 year of age, compared with folic acid only or folic acid plus iron supplementation.
ABSTRACT
OBJECTIVE.We investigated the benefits of maternal multimicronutrient
supplementa-tion during gestasupplementa-tion on the mental and psychomotor development of infants.
METHODS.In a double-blind, randomized, controlled trial, pregnant women (N⫽5828)
in 2 rural counties in western China were assigned randomly to receive multimicro-nutrient (5 minerals and 10 vitamins at levels approximating the recommended daily allowance), folic acid plus iron, or folic acid supplementation daily from⬃14 weeks of gestation until delivery. We assessed a subset of the newborns (N⫽1305) from the 3 supplementation groups by measuring their mental and psychomotor development with the Bayley Scales of Infant Development, at 3, 6, and 12 months of age. Multilevel analyses were used to compare the mental development and psychomotor development raw scores at 3, 6, and 12 months.
RESULTS.Multimicronutrient supplementation was associated with mean increases in
mental development raw scores for infants at 1 year of age of 1.00 and 1.22 points, compared with folic acid only and folic acid plus iron supplementation, respectively. However, supplementation did not increase significantly the psychomotor develop-ment raw scores up to 1 year of age.
CONCLUSION.Compared with iron and folic acid supplementation, the administration of
multimicronutrients to pregnant women improved the mental development of their children at 1 year of age.Pediatrics2009;123:e685–e692
M
ICRONUTRIENT MALNUTRITION ISwidespread and constitutes one of the main nutritional problems throughout the world.1 Micronutrient deficiencies are among the 10 leading contributors to the global burden of disease.2Currently,⬎2 billion of the world’s people are estimated to have deficiencies in key vitamins and minerals.3The majority
of the world’s people live in low-income countries, and they are typically deficient in ⬎1 micronutrient.
Pregnant women tend to have relatively greater requirements for most micronutrients, compared with the general population, and they are more susceptible to the harmful consequences of deficiencies,4which increases the risk of inadequate intake.
Commonly used, cost-effective strategies to ameliorate micronutrient deficiency are supplementation and forti-fication. Different micronutrients are provided to pregnant women around the world. However, multiple micronu-trients are required simultaneously when the diet is poor. With a view toward overcoming this problem, the United Nations Children’s Fund, the World Health Organization, and the United Nations University have formulated a combination of 5 minerals and 10 vitamins (at levels approximately equivalent to the recommended daily allowance) for pregnant women.5 Some trials have revealed benefits of this multimicronutrient, in terms of increasing birth weight and decreasing early infant mortality rates,6–10but the impact on the functional outcomes of infants is not
www.pediatrics.org/cgi/doi/10.1542/ peds.2008-3007
doi:10.1542/peds.2008-3007
This study has been registered as an International Standard Randomized Controlled Trial (no. ISRCTN08850194).
Key Words
multimicronutrients, dietary supplements, pregnancy, infants, Bayley Scales of Infant Development, randomized, controlled trial
Abbreviations
MD—mental development BSID—Bayley Scales of Infant Development
PD—psychomotor development CI— confidence interval
Accepted for publication Dec 22, 2008 Address correspondence to Hong Yan, MSc, Division of Epidemiology and Biostatistics, Department of Public Health, Xi’an Jiaotong University School of Medicine, 76 Yanta West Rd, Xi’an 710061, China. E-mail: xjtu㛭yh. [email protected]
clear. Therefore, we conducted this population-based, randomized, controlled trial to assess the effects of ma-ternal multimicronutrient supplementation on infant mental development (MD) and psychomotor develop-ment (PD).
METHODS
Study Design and Population
The details of this double-blind, cluster-randomized, controlled trial have been described elsewhere.9Briefly, we conducted this trial in 2 poor rural counties in west-ern China. We used computer-generated random num-bers, stratified according to county and township, and randomly assigned villages to the 3 supplementation groups (daily folic acid, folic acid plus iron, or multimi-cronutrient supplements) before recruitment. Pregnant women in the same village received the same supple-ment tablets daily from enrollsupple-ment until delivery. Women in the folic acid supplement group received 400
g of folic acid per day, those in the folic acid plus iron supplement group received 400g of folic acid and 60 mg of iron per day, and those in the multimicronutrient supplement group received the following multimicronu-trients: 400 g of folic acid, 30 mg of iron, 5 g of vitamin D, 10 mg of vitamin E, 1.4 mg of thiamine, 1.4 mg of riboflavin, 18 mg of niacin, 1.9 mg of vitamin B6, 2.6g of vitamin B12, 70 mg of vitamin C, 800g retinol equivalents of vitamin A, 2.0 mg of copper, 65 g of selenium, 15 mg of zinc, and 150g of iodine per day. These amounts are consistent with the suggested com-position of multimicronutrient supplements for prenatal use, as recommended by the United Nations Children’s Fund, the World Health Organization, and the United Nations University.5The control group received folic acid only, because it is general practice in China to recom-mend folic acid supplements (400g per day) for preg-nant women. The 3 types of supplement tablets were indistinguishable from each other in both appearance and taste, were packaged in the same blister packs of 15 tablets each, and were marked with different expiration dates. The marked codes remained unknown to the in-vestigators and participants until the study was com-pleted. The tablets underwent composition analysis be-fore being distributed. The study was approved by the Committee for Science and Research at Xi’an Jiaotong University.
Eligibility and Surveillance of Pregnancy
Village doctors regularly visited all women of reproduc-tive age who were not already pregnant, menopausal, sterilized, or widowed, to identify new pregnancies (on the basis of a human chorionic gonadotropin urine test), and informed the women and their families about this program. When a newly pregnant woman was identi-fied, she received an initial prenatal care checkup at the township hospital or county hospital. Baseline informa-tion was collected and a written consent form was signed or fingerprinted (for illiterate women) at that time. The village doctor then distributed a 15-tablet pack to each enrolled pregnant woman, retrieving the used packs to
count the remaining tablets every 2 weeks (1 tablet should have been remaining if the patient was fully compliant). The women were instructed to consume 1 tablet every day, with no other vitamin or mineral sup-plements unless recommended by a study obstetrician. We organized regular meeting and supervision systems to maximize medication adherence.
Follow-up Monitoring and Data Collection
The pregnant women were monitored at ⱖ3 prenatal
care checkups in different stages of pregnancy. For hos-pital deliveries, obstetricians provided birth details and anthropometric data. For home deliveries, a field team visited the homes to collect the corresponding birth and anthropometric information for the newborns within 72 hours after delivery. A subgroup of singleton neonates (born between January 2004 and December 2004, the middle 1 year of the total 3.5 years of recruitment until January 2006) was included in the postnatal surveil-lance. Sample size calculations indicated that a mini-mum of 1200 infants (400 infants in each group) would be needed to detect a moderate difference of 1.2 (20% of SD) in the mean MD raw score, with 80% power and
␣⫽.05.
We assessed the MD and PD of this subgroup of infants until 1 year of age by using the Bayley Scales of Infant Development (BSID), which included items re-garding sensory/perceptual acuity, discrimination, mem-ory, early verbal communication, body control, coordi-nation of large muscles, fine manipulation skills, and
dynamic movement for different ages of ⬍42 months.
These scales have been translated into Chinese and lo-cally standardized to become culturally appropriate. The reliability and validity of these standardized scales have been shown to be satisfactory.11The BSID were admin-istered at the hospital or the child’s own home in a standardized manner, when the infant was not hungry, sleepy, or restless, by rigorously trained examiners who had demonstrated high levels of consistency with each other. The examiners, participating women, and re-searchers administering the interventions were all blinded successfully with respect to treatment group. It was intended that the infants would be assessed at 3, 6, and 12 months of age; however, because of logistic prob-lems, this schedule could not always be followed. If the infant was ill, was unavailable, or would not cooperate, then another assessment was arranged for a later date. The data were grouped for analysis around the sched-uled time points.
Statistical Analyses
We obtained information regarding the participating pregnant women, birth outcomes, and development of the infants in individual files and linked them with unique numbers. The data were checked manually for completeness at different times and were double-en-tered into a data management system. We subjected the data to range checks and logical checks for accuracy; in the case of any inconsistencies, recorders were sent back to the field within a few days. The primary analyses were based on intention to treat. Baseline characteristic of subjects were compared across treatment groups by us-ing analysis of variance or2tests. Because of the mul-tilevel structure of the data and the sampling method, a 4-level analysis was developed to compare the MD and PD raw scores, with county set to level 4, township to level 3, village to level 2, and individual to level 1. The multilevel model approach seems to be a good method for analyzing data with a hierarchical structure, and it can be applied in cluster sampling investigations.14 Anal-yses were conducted with SPSS 12 (SPSS, Chicago, IL). MLwiN 2.0 (Institute of Education, London, England) was used for the multilevel modeling.
Estimations of the mean differences and 95% confi-dence intervals (CIs) were made according to the cate-gories of supplementation and were adjusted for poten-tial confounding factors. All reported P values were 2-tailed, and values of⬍.05 were considered to be sta-tistically significant.
We considered the following variables as potential confounders in the multivariate adjusted analysis: in-fant’s age, gender, gestational age at birth, Apgar scores at 1 and 5 minutes, birth weight, and history of patho-logical jaundice and pneumonia, mother’s age at deliv-ery, BMI at enrollment, educational level, and occupa-tional class, number of supplement tablets consumed, father’s educational level and occupational class, and family’s socioeconomic status. Age-adjusted analyses were also conducted.
Interactions between micronutrient supplementation and confounders were tested through the addition of cross-product terms to the multivariate model. To min-imize the possibility of low supplementation, we re-peated the analyses after stratifying the data according to the number of supplement tablets consumed (⬍150 or
⬎150 tablets). Analyses stratified according to gender, gestational age, and mother’s age also were conducted.
RESULTS
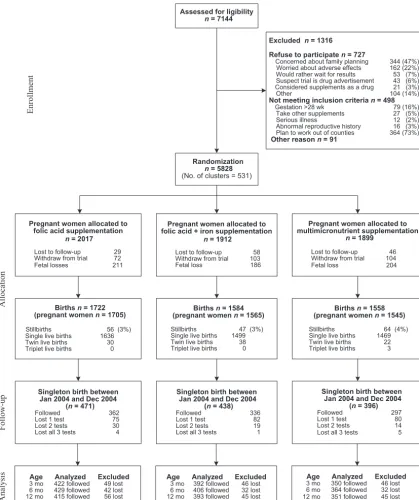
Figure 1 shows the profile of this trial. A total of 5828 pregnant women from 531 villages were enrolled in the study, and these women gave birth to 4864 children. A subgroup of 1305 newborns was monitored, including 471 infants of mothers who received folic acid supple-ments, 438 infants of mothers who received folic acid plus iron, and 396 infants of mothers who received multimicronutrients. Ten infants (0.8%) were lost to follow-up monitoring, 63 infants lacked 2 of the 3 as-sessments in the appropriate month, 237 infants lacked 1 assessment in the appropriate month, and 995 infants
(76%) were assessed on all 3 occasions at the appropri-ate ages.
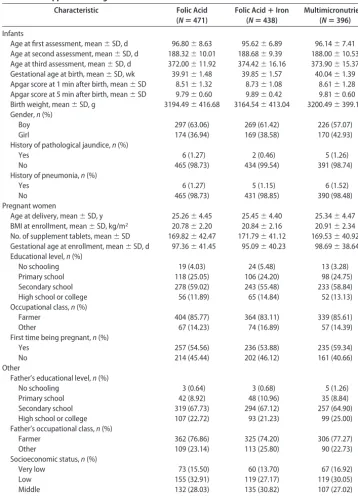
Table 1 shows the baseline characteristics of the preg-nant women and their infants. The values for mean gestational age of the fetus at enrollment, mean gesta-tional age at birth, mean age of the mother at delivery, mean BMI at enrollment, and mean birth weight of the child were similar. The mean numbers of supplement tablets consumed were also very similar, that is, 170 in the folic acid only group, 172 in the folic acid plus iron group, and 170 in the multimicronutrient group (P ⫽
.68, analysis of variance). The proportions for the edu-cational level and occupational classification of the par-ent, gender of the newborn, socioeconomic status (con-sidering the house type and property in the household as 2 proxy measures), and history of pathological jaundice or pneumonia were comparable. The mean Apgar scores of the infants at 1 and 5 minutes after birth were signif-icantly different among the 3 treatment groups, but the absolute differences were small. No important adverse event or side effect was reported for any of the treatment groups.
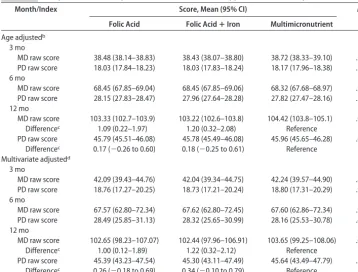
With adjustment for the children’s age, there was no significant difference in MD and PD raw scores among the different supplementation groups at 3 and 6 months of age. At 12 months of age, the mean MD raw scores were 104.42 points (95% CI: 103.8-105.1 points) for the multimicronutrient group, 103.22 points (95% CI: 102.6-103.8 points) for the folic acid plus iron group, and 103.33 points (95% CI: 102.7-103.9 points) for the folic acid only group (Table 2). Infants of mothers who received multimicronutrient supplementation had a higher mean MD raw score than did those in the other 2 groups. The increases in the MD raw scores were 1.09 points (95% CI: 0.22–1.97 points) and 1.20 points (95% CI: 0.32–2.08 points) in comparison with the folic acid only and folic acid plus iron groups, respectively. No significant increases in the PD raw scores at 12 months of age were found for the multimicronutrient group, com-pared with the folic acid and folic acid plus iron groups. The multivariate-adjusted results did not change sub-stantially when we included the potential confounders in the analysis (Table 2). Multimicronutrient supple-mentation was associated with a positive effect on chil-dren’s MD, increasing the mean MD raw score at 12 months by 1.22 points (95% CI: 0.32–2.12 points) in comparison with the folic acid plus iron group and by 1.00 points (95% CI: 0.12–1.89 points) in comparison with the folic acid only group (P⫽.02). The mean PD raw score at 12 months of age for the multimicronutri-ent supplemmultimicronutri-entation group was similar to those for the folic acid plus iron group and the folic acid only group, with mean differences of 0.34 points (95% CI:⫺0.10 to 0.79 points) and 0.26 points (95% CI: ⫺0.18 to 0.69 points), respectively.
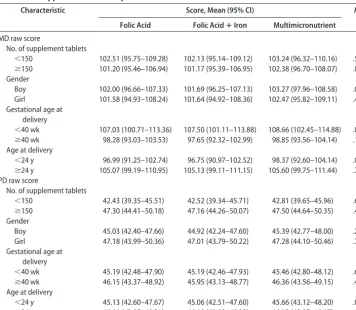
age, particularly for mothers who consumedⱖ150 tab-lets, male infants, and younger mothers (mother’s age at delivery of⬍24 years) (Table 3). No interaction between supplementation and corresponding confounders was noted when we performed additional analyses for inter-actional effects (data not shown).
DISCUSSION
In this population-based, double-blind, randomized, controlled trial conducted in rural western China, we found that maternal multimicronutrient
supplementa-tion improved MD in children at 1 year of age, compared with folic acid supplementation alone or folic acid plus iron supplementation, but did not affect PD significantly. The effects were robust, when adjusted for potential confounders or limited to stratified subcategories.
The multimicronutrient supplementation in our study was composed of 5 minerals and 10 vitamins and has been tested in several populations. The benefits of this maternal supplementation on mothers’ and chil-dren’s health were demonstrated previously, in terms of increased birth weight in randomized, controlled trials Assessed for ligibility
n = 7144
Excluded n = 1316
Refuse to participaten = 727
Concerned about family planning 344 (47%) Worried about adverse effects 162 (22%) Would rather wait for results 53 (7%) Suspect trial is drug advertisement 43 (6%) Considered supplements as a drug 21 (3%) ) % 4 1 ( 4 0 1 r e h t O
Not meeting inclusion criterian = 498
Gestation >28 wk 79 (16%) Take other supplements 27 (5%) ) % 2 ( 2 1 s s e n ll i s u o i r e S
Abnormal reproductive history 16 (3%) Plan to work out of counties 364 (73%)
Other reason n = 91
Randomization
n = 5828
(No. of clusters = 531)
Pregnant women allocated to folic acid supplementation
n = 2017
Lost to follow-up 29 Withdraw from trial 72 Fetal losses 211
Pregnant women allocated to folic acid + iron supplementation
n = 1912
Lost to follow-up 58 Withdraw from trial 103 Fetal loss 186
Pregnant women allocated to multimicronutrient supplementation
n = 1899
Lost to follow-up 46 Withdraw from trial 104 Fetal loss 204
Births n = 1722
(pregnant women n = 1705)
Stillbirths 56 (3%) Single live births 1636 Twin live births 30 Triplet live births 0
Births n = 1584
(pregnant women n = 1565)
Stillbirths 47 (3%) Single live births 1499 Twin live births 38 Triplet live births 0
Births n = 1558
(pregnant women n = 1545)
Stillbirths 64 (4%) Single live births 1469 Twin live births 22 Triplet live births 3
Singleton birth between Jan 2004 and Dec 2004
(n = 471)
Followed 362 Lost 1 test 75 Lost 2 tests 30 Lost all 3 tests 4
Singleton birth between Jan 2004 and Dec 2004
(n = 438)
Followed 336 Lost 1 test 82 Lost 2 tests 19 Lost all 3 tests 1
Singleton birth between Jan 2004 and Dec 2004
(n = 396)
Followed 297 Lost 1 test 80 Lost 2 tests 14 Lost all 3 tests 5
Enrollment Allocat ion Fo llo w-up An aly
sis Age Analyzed Excluded
3 mo 422 followed 49 lost 6 mo 429 followed 42 lost 12 mo 415 followed 56 lost
Age Analyzed Excluded
3 mo 392 followed 46 lost 6 mo 406 followed 32 lost 12 mo 393 followed 45 lost
Age Analyzed Excluded
3 mo 350 followed 46 lost 6 mo 364 followed 32 lost 12 mo 351 followed 45 lost
conducted in Guinea Bissau, Nepal, Zimbabwe, and Chi-na,6–9 prolonged gestational periods in Zimbabwe and China,8,9and reduced early infant mortality rates in In-donesia.10The positive effects persisted into childhood, with increases in both weight and body size at 2.5 years of age.15 In contrast, a study in Mexico failed to reveal benefits in either birth weight or length.16The only study related to infant cognitive development suggested small benefits of early food and multimicronutrient supple-mentation for 7-month-old infants of low-BMI mothers in Bangladesh.17 The present study has provided new
evidence for the benefits of micronutrient supplementa-tion with respect to infant mental and PD at 1 year of age.
There is evidence that different micronutrients play a role in children’s MD. Previous studies and reviews sug-gested that iodine deficiency is associated with poor development18 and iodine deficiency during pregnancy has negative effects on the developing fetus and MD of the offspring.19,20 Conversely, no effect of zinc supple-mentation alone, at daily doses of 25 mg and 30 mg, on children’s MD and PD has been found.21,22 Similarly,
TABLE 1 Baseline Characteristics of Pregnant Women and Their Offspring According to Maternal Supplement Assignment
Characteristic Folic Acid
(Nⴝ471)
Folic AcidⴙIron (Nⴝ438)
Multimicronutrient (Nⴝ396) Infants
Age at first assessment, mean⫾SD, d 96.80⫾8.63 95.62⫾6.89 96.14⫾7.41
Age at second assessment, mean⫾SD, d 188.32⫾10.01 188.68⫾9.39 188.00⫾10.53
Age at third assessment, mean⫾SD, d 372.00⫾11.92 374.42⫾16.16 373.90⫾15.37
Gestational age at birth, mean⫾SD, wk 39.91⫾1.48 39.85⫾1.57 40.04⫾1.39
Apgar score at 1 min after birth, mean⫾SD 8.51⫾1.32 8.73⫾1.08 8.61⫾1.28
Apgar score at 5 min after birth, mean⫾SD 9.79⫾0.60 9.89⫾0.42 9.81⫾0.60
Birth weight, mean⫾SD, g 3194.49⫾416.68 3164.54⫾413.04 3200.49⫾399.10
Gender,n(%)
Boy 297 (63.06) 269 (61.42) 226 (57.07)
Girl 174 (36.94) 169 (38.58) 170 (42.93)
History of pathological jaundice,n(%)
Yes 6 (1.27) 2 (0.46) 5 (1.26)
No 465 (98.73) 434 (99.54) 391 (98.74)
History of pneumonia,n(%)
Yes 6 (1.27) 5 (1.15) 6 (1.52)
No 465 (98.73) 431 (98.85) 390 (98.48)
Pregnant women
Age at delivery, mean⫾SD, y 25.26⫾4.45 25.45⫾4.40 25.34⫾4.47
BMI at enrollment, mean⫾SD, kg/m2 20.78⫾2.20 20.84⫾2.16 20.91⫾2.34
No. of supplement tablets, mean⫾SD 169.82⫾42.47 171.79⫾41.12 169.53⫾40.92
Gestational age at enrollment, mean⫾SD, d 97.36⫾41.45 95.09⫾40.23 98.69⫾38.64
Educational level,n(%)
No schooling 19 (4.03) 24 (5.48) 13 (3.28)
Primary school 118 (25.05) 106 (24.20) 98 (24.75)
Secondary school 278 (59.02) 243 (55.48) 233 (58.84)
High school or college 56 (11.89) 65 (14.84) 52 (13.13)
Occupational class,n(%)
Farmer 404 (85.77) 364 (83.11) 339 (85.61)
Other 67 (14.23) 74 (16.89) 57 (14.39)
First time being pregnant,n(%)
Yes 257 (54.56) 236 (53.88) 235 (59.34)
No 214 (45.44) 202 (46.12) 161 (40.66)
Other
Father’s educational level,n(%)
No schooling 3 (0.64) 3 (0.68) 5 (1.26)
Primary school 42 (8.92) 48 (10.96) 35 (8.84)
Secondary school 319 (67.73) 294 (67.12) 257 (64.90)
High school or college 107 (22.72) 93 (21.23) 99 (25.00)
Father’s occupational class,n(%)
Farmer 362 (76.86) 325 (74.20) 306 (77.27)
Other 109 (23.14) 113 (25.80) 90 (22.73)
Socioeconomic status,n(%)
Very low 73 (15.50) 60 (13.70) 67 (16.92)
Low 155 (32.91) 119 (27.17) 119 (30.05)
Middle 132 (28.03) 135 (30.82) 107 (27.02)
weekly supplementation with vitamin A in addition to iron during gestation was found to have no effect on MD or PD.23 However, there is evidence that multiple vita-mins administered together result in a significant
im-provement in PD.24 Multimicronutrient
supplementa-tion is hypothetically preferable to supplementasupplementa-tion with folic acid plus iron or folic acid alone; our results make an important contribution in support of this sup-position.
A long-term, follow-up study of a randomized, con-trolled trial from Australia involving 420 pregnant women who received 20 mg of iron daily from 20 weeks of gestation until delivery failed to demonstrate any significant benefits in the intelligence quotient and be-havior of their children at 4 years of age, compared with placebo treatment.25 This result was consistent with a previous systematic review of randomized, controlled trials, which concluded that iron supplementation im-proves MD scores modestly and has no convincing effect on the intelligence test scores or the PD scores of chil-dren⬍27 months of age.26Similarly, our results revealed that iron plus folic acid supplementation did not show additional benefits in MD and PD, compared with folic acid alone. Furthermore, the amount of iron used for the iron plus folic acid group was 60 mg, which was twice
that used for the multimicronutrient group. Our data thus provide additional evidence against an association between gestational iron supplementation and infant MD. No clear cause-effect relationship between iron de-ficiency and subsequent cognitive or behavioral perfor-mance has been demonstrated.27
Although our trial showed a statistically significant effect on infant MD, the degree of improvement was relatively small, representing a ⬃6-day advance in de-velopment at 1 year of age. Our findings and similar previous results17suggest that prenatal multimicronutri-ent supplemmultimicronutri-entation makes a relatively limited contri-bution to the MD and PD of infants.
Our study had several strengths. It was a randomized, controlled trial, our subjects were recruited from the general population, our sample size was appropriate, and we achieved a high retention rate.
Our study also had certain limitations. First, the ran-domization method we used was based on villages rather than individual women, which might have introduced a larger random error. However, we included a large num-ber of villages (N ⫽ 531) and the average number of subjects in each village was small, which minimized the potential for random error. Randomization was per-formed with approximately equal distribution, to ensure
TABLE 2 Comparison of Developmental Scores in Different Supplementation Groups
Month/Index Score, Mean (95% CI) Pa
Folic Acid Folic AcidⴙIron Multimicronutrient Age adjustedb
3 mo
MD raw score 38.48 (38.14–38.83) 38.43 (38.07–38.80) 38.72 (38.33–39.10) .54
PD raw score 18.03 (17.84–18.23) 18.03 (17.83–18.24) 18.17 (17.96–18.38) .57
6 mo
MD raw score 68.45 (67.85–69.04) 68.45 (67.85–69.06) 68.32 (67.68–68.97) .95
PD raw score 28.15 (27.83–28.47) 27.96 (27.64–28.28) 27.82 (27.47–28.16) .37
12 mo
MD raw score 103.33 (102.7–103.9) 103.22 (102.6–103.8) 104.42 (103.8–105.1) .01
Differencec 1.09 (0.22–1.97) 1.20 (0.32–2.08) Reference
PD raw score 45.79 (45.51–46.08) 45.78 (45.49–46.08) 45.96 (45.65–46.28) .65
Differencec 0.17 (⫺0.26 to 0.60) 0.18 (⫺0.25 to 0.61) Reference
Multivariate adjustedd 3 mo
MD raw score 42.09 (39.43–44.76) 42.04 (39.34–44.75) 42.24 (39.57–44.90) .81
PD raw score 18.76 (17.27–20.25) 18.73 (17.21–20.24) 18.80 (17.31–20.29) .91
6 mo
MD raw score 67.57 (62.80–72.34) 67.62 (62.80–72.45) 67.60 (62.86–72.34) .99
PD raw score 28.49 (25.85–31.13) 28.32 (25.65–30.99) 28.16 (25.53–30.78) .44
12 mo
MD raw score 102.65 (98.23–107.07) 102.44 (97.96–106.91) 103.65 (99.25–108.06) .02
Differencec 1.00 (0.12–1.89) 1.22 (0.32–2.12) Reference
PD raw score 45.39 (43.23–47.54) 45.30 (43.11–47.49) 45.64 (43.49–47.79) .29
Differencec 0.26 (⫺0.18 to 0.69) 0.34 (⫺0.10 to 0.79) Reference
aMultilevel models were used to compare the differences between supplementation groups, with county set to level 4, township to level
3, village to level 2, and individual to level 1.
bMean, 95% CI, andPvalues were adjusted according to the infant’s age in days (calculated as the difference between the date of
measurement and the date of the first day of the last menstrual period).
cDifference of the mean raw score compared with that in the multimicronutrient supplementation group.
dMean, 95% CI, andPvalues were adjusted according to the infant’s age in days, gender, gestational age at birth, Apgar scores at 1 and
balance across the groups, and a multilevel model was used to accommodate the cluster sampling method. Sec-ond, the design of this study did not enable us to identify which micronutrient (or combination of a few) made the major contribution to the beneficial effect observed, be-cause all of the nutrients were contained within the same tablet. Third, we did not include all possible con-founding variables (such as smoking, alcohol use, and energy consumption) in our analysis, mainly because of the very small numbers of smokers and drinkers among women and the low levels of cigarette and alcohol use by women in the study region. Randomization and our large sample size likely resulted in balancing of these confounders across the groups. Finally, the follow-up period was relatively short and the predictive relation-ship between BSID scores at 1 year and long-term MD was relatively poor, which may limit the implications of our findings.
CONCLUSIONS
This large, population-based, randomized, controlled trial indicated a positive effect on the MD of children at 1 year of age as a consequence of maternal
multimicro-nutrient supplementation. Additional long-term studies are needed to evaluate the effect of this multimicronu-trient formula.
ACKNOWLEDGMENTS
This work was supported by a grant from the National Natural Science Foundation of China (grant 30300287) and a grant from the United Nations Children’s Fund (grant YH101-H12/03). Neither of the funding sources had any role in the study design; in the collection, anal-ysis, and interpretation of data; in the writing of the report; or in the decision to submit the manuscript for publication.
We are indebted to Dr Liu Xiaohong for training and supervising the testers and to Lin Dongtao for editing the manuscript. We also thank all of our supervisors for their tremendous efforts in maintain the quality of our data.
REFERENCES
1. Allen LH. Interventions for micronutrient deficiency control in developing countries: past, present and future.J Nutr.2003; 133(11 suppl 2):3875S–3878S
2. World Health Organization.The World Health Report 2001:
Re-TABLE 3 Stratified Analysis of Developmental Scores at 12 Months of Age in Different Supplementation Groups
Characteristic Score, Mean (95% CI) Pa
Folic Acid Folic AcidⴙIron Multimicronutrient MD raw score
No. of supplement tablets
⬍150 102.51 (95.75–109.28) 102.13 (95.14–109.12) 103.24 (96.32–110.16) .50
ⱖ150 101.20 (95.46–106.94) 101.17 (95.39–106.95) 102.38 (96.70–108.07) .04
Gender
Boy 102.00 (96.66–107.33) 101.69 (96.25–107.13) 103.27 (97.96–108.58) .02
Girl 101.58 (94.93–108.24) 101.64 (94.92–108.36) 102.47 (95.82–109.11) .44
Gestational age at delivery
⬍40 wk 107.03 (100.71–113.36) 107.50 (101.11–113.88) 108.66 (102.45–114.88) .06
ⱖ40 wk 98.28 (93.03–103.53) 97.65 (92.32–102.99) 98.85 (93.56–104.14) .17
Age at delivery
⬍24 y 96.99 (91.25–102.74) 96.75 (90.97–102.52) 98.37 (92.60–104.14) .02
ⱖ24 y 105.07 (99.19–110.95) 105.13 (99.11–111.15) 105.60 (99.75–111.44) .73
PD raw score
No. of supplement tablets
⬍150 42.43 (39.35–45.51) 42.52 (39.34–45.71) 42.81 (39.65–45.96) .65
ⱖ150 47.30 (44.41–50.18) 47.16 (44.26–50.07) 47.50 (44.64–50.35) .47
Gender
Boy 45.03 (42.40–47.66) 44.92 (42.24–47.60) 45.39 (42.77–48.00) .26
Girl 47.18 (43.99–50.36) 47.01 (43.79–50.22) 47.28 (44.10–50.46) .75
Gestational age at delivery
⬍40 wk 45.19 (42.48–47.90) 45.19 (42.46–47.93) 45.46 (42.80–48.12) .60
ⱖ40 wk 46.15 (43.37–48.92) 45.95 (43.13–48.77) 46.36 (43.56–49.15) .48
Age at delivery
⬍24 y 45.13 (42.60–47.67) 45.06 (42.51–47.60) 45.66 (43.12–48.20) .05
ⱖ24 y 46.14 (43.07–49.21) 46.18 (43.03–49.32) 46.12 (43.07–49.17) .99
Mean, 95% CI, andPvalues were adjusted according to the infant’s age in days, gender, gestational age at birth, Apgar scores at 1 and 5 minutes after birth, birth weight, history of pathological jaundice, and history of pneumonia, mother’s age at delivery, BMI at enrollment, educational level, and occupational class, number of supplement tablets consumed, father’s educational level and occupational class, and family socioeconomic status.
aMultilevel models were used to compare the differences between supplementation groups, with county set to level 4, township to level
ducing Risks, Promoting Healthy Life. Geneva, Switzerland: World Health Organization; 2001
3. World Health Organization; World Food Programme; United Nations Children’s Fund.Preventing and Controlling Micronutrient Deficiencies in Populations Affected by an Emergency. Geneva, Switzerland: World Health Organization; 2007
4. Ladipo OA. Nutrition in pregnancy: mineral and vitamin sup-plements.Am J Clin Nutr.2000;72(1 suppl):280S–290S 5. United Nations Children’s Fund; World Health Organization;
United Nations University.Composition of a Multi-Micronutrient Supplement to Be Used in Pilot Programmes Among Pregnant Women in Developing Countries. New York, NY: United Nations Chil-dren’s Fund; 1999
6. Kaestel P, Michaelsen KF, Aaby P, Friis H. Effects of prenatal multimicronutrient supplements on birth weight and perinatal mortality: a randomised, controlled trial in Guinea-Bissau.Eur J Clin Nutr.2005;59(9):1081–1089
7. Osrin D, Vaidya A, Shrestha Y, et al. Effects of antenatal mul-tiple micronutrient supplementation on birthweight and ges-tational duration in Nepal: double-blind, randomised con-trolled trial.Lancet.2005;365(9463):955–962
8. Friis H, Gomo E, Nyazema N, et al. Effect of multimicronutrient supplementation on gestational length and birth size: a ran-domized, placebo-controlled, double-blind effectiveness trial in Zimbabwe.Am J Clin Nutr.2004;80(1):178 –184
9. Zeng L, Cheng Y, Dang S, et al. Impact of micronutrient sup-plementation during pregnancy on birth weight, duration of gestation, and perinatal mortality in rural western China: dou-ble blind cluster randomised controlled trial.BMJ.2008;337: a2001
10. Shankar AH, Jahari AB, Sebayang SK, et al. Effect of maternal multiple micronutrient supplementation on fetal loss and in-fant death in Indonesia: a double-blind cluster-randomised trial.Lancet.2008;371(9608):215–227
11. Huang H, Tao SD, Zhang YW, et al. Standardization of Bayley Scales of Infant Development in Shanghai.Chin J Child Health. 1993;1(3):158 –160
12. Bayley N.The Bayley Scales of Infant Development. New York, NY: Psychological Corp; 1969
13. Bayley N.Bayley Scales of Infant Development. 2nd ed. San An-tonio, TX: Psychological Corp; 1993
14. Brazy JE, Eckerman CO, Oehler JM, Goldstein RF, O’Rand AM. Nursery Neurobiologic Risk Score: important factor in predicting outcome in very low birth weight infants.J Pediatr. 1991;118(5):783–792
15. Osrin D, Vaidya A, Shrestha Y, et al. Effects of antenatal mul-tiple micronutrient supplementation on children’s weight and size at 2 years of age in Nepal: follow-up of a double-blind randomised controlled trial.Lancet.2008;371(9611):492– 499 16. Ramakrishnan U, Gonzalez-Cossio T, Neufeld LM, Rivera J,
Martorell R. Multiple micronutrient supplementation during pregnancy does not lead to greater infant birth size than does iron-only supplementation: a randomized controlled trial in a semirural community in Mexico.Am J Clin Nutr.2003;77(3): 720 –725
17. Tofail F, Persson LA, El Arifeen S, et al. Effects of prenatal food and micronutrient supplementation on infant development: a randomized trial from the Maternal and Infant Nutrition In-terventions, Matlab (MINIMat) study.Am J Clin Nutr.2008; 87(3):704 –711
18. Grantham-McGregor SM, Ani CC. The role of micronutrients in psychomotor and cognitive development.Br Med Bull.1999; 55(3):511–527
19. Black MM. Micronutrient deficiencies and cognitive function-ing.J Nutr.2003;133(11 suppl 2):3927S–3931S
20. Zimmermann M, Delange F. Iodine supplementation of preg-nant women in Europe: a review and recommendations.Eur J Clin Nutr.2004;58(7):979 –984
21. Hamadani JD, Fuchs GJ, Osendarp SJ, Huda SN, Grantham-McGregor SM. Zinc supplementation during pregnancy and effects on mental development and behaviour of infants: a follow-up study.Lancet.2002;360(9329):290 –294
22. Tamura T, Goldenberg RL, Ramey SL, Nelson KG, Chapman VR. Effect of zinc supplementation of pregnant women on the mental and psychomotor development of their children at 5 y of age.Am J Clin Nutr.2003;77(6):1512–1516
23. Schmidt MK, Muslimatun S, West CE, Schultink W, Hautvast JG. Mental and psychomotor development in Indonesian in-fants of mothers supplemented with vitamin A in addition to iron during pregnancy.Br J Nutr.2004;91(2):279 –286 24. McGrath N, Bellinger D, Robins J, Msamanga GI, Tronick E,
Fawzi WW. Effect of maternal multivitamin supplementation on the mental and psychomotor development of children who are born to HIV-1–infected mothers in Tanzania. Pediatrics. 2006;117(2). Available at: www.pediatrics.org/cgi/content/ full/117/2/e216
25. Zhou SJ, Gibson RA, Crowther CA, Baghurst P, Makrides M. Effect of iron supplementation during pregnancy on the intel-ligence quotient and behavior of children at 4 y of age: long-term follow-up of a randomized controlled trial.Am J Clin Nutr. 2006;83(5):1112–1117
26. Sachdev H, Gera T, Nestel P. Effect of iron supplementation on mental and motor development in children: systematic review of randomised controlled trials.Public Health Nutr.2005;8(2): 117–132
DOI: 10.1542/peds.2008-3007
2009;123;e685
Pediatrics
Quanli Wang and Ichiro Tsuji
Qiang Li, Hong Yan, Lingxia Zeng, Yue Cheng, Weifeng Liang, Shaonong Dang,
Double-Blind, Randomized, Controlled Trial
Development of Infants in Rural Western China: Follow-up Evaluation of a
Effects of Maternal Multimicronutrient Supplementation on the Mental
Services
Updated Information &
http://pediatrics.aappublications.org/content/123/4/e685 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/123/4/e685#BIBL This article cites 21 articles, 10 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/therapeutics_sub Therapeutics
http://www.aappublications.org/cgi/collection/pharmacology_sub Pharmacology
http://www.aappublications.org/cgi/collection/nutrition_sub Nutrition
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2008-3007
2009;123;e685
Pediatrics
Quanli Wang and Ichiro Tsuji
Qiang Li, Hong Yan, Lingxia Zeng, Yue Cheng, Weifeng Liang, Shaonong Dang,
Double-Blind, Randomized, Controlled Trial
Development of Infants in Rural Western China: Follow-up Evaluation of a
Effects of Maternal Multimicronutrient Supplementation on the Mental
http://pediatrics.aappublications.org/content/123/4/e685
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.