ARTICLE
Randomized, Controlled Trial Comparing
Synchronized Intermittent Mandatory Ventilation
and Synchronized Intermittent Mandatory
Ventilation Plus Pressure Support in Preterm Infants
Zenaida C. Reyes, MD, Nelson Claure, PhD, Markus K. Tauscher, MD, Carmen D’Ugard, RRT, Silvia Vanbuskirk, RN, Eduardo Bancalari, MD
Division of Newborn Medicine, Department of Pediatrics, University of Miami, Miller School of Medicine, Miami, Florida
Financial Disclosure: Viasys Healthcare provided the ventilatory equipment used in this trial. The University of Miami and Drs Bancalari and Claure have a licensing agreement with Viasys Healthcare of a product not related to the ventilator used in this study. Viasys Healthcare provides financial support to an annual educational activity of the University of Miama Division of Newborn Medicine.
ABSTRACT
BACKGROUND.Prolonged mechanical ventilation is associated with lung injury in preterm infants. In these infants, weaning from synchronized intermittent man-datory ventilation may be delayed by their inability to cope with increased respi-ratory loads. The addition of pressure support to synchronized intermittent man-datory ventilation can offset these loads and may facilitate weaning.
OBJECTIVE.The purpose of this work was to compare synchronized intermittent mandatory ventilation and synchronized intermittent mandatory ventilation plus pressure support in weaning from mechanical ventilation and the duration of supplemental oxygen dependency in preterm infants with respiratory failure.
METHODS.Preterm infants weighing 500 to 1000 g at birth who required mechanical ventilation during the first postnatal week were randomly assigned to synchro-nized intermittent mandatory ventilation or synchrosynchro-nized intermittent mandatory ventilation plus pressure support. In both groups, weaning followed a set protocol during the first 28 days. Outcomes were assessed during the first 28 days and until discharge or death.
RESULTS.There were 107 infants enrolled (53 synchronized intermittent mandatory ventilation plus pressure support and 54 synchronized intermittent mandatory ventilation). Demographic and perinatal data, mortality, and morbidity did not differ between groups. During the first 28 days, infants in the synchronized intermittent mandatory ventilation plus pressure support group reached minimal ventilator settings and were extubated earlier than infants in the synchronized intermittent mandatory ventilation group. Total duration of mechanical ventila-tion, duration of oxygen dependency, and oxygen need at 36 weeks’ postmen-strual age alone or combined with death did not differ between groups. However, infants in synchronized intermittent mandatory ventilation plus pressure support within the 700- to 1000-g birth weight strata had a shorter oxygen dependency.
CONCLUSIONS.The results of this study suggest that the addition of pressure support as a supplement to synchronized intermittent mandatory ventilation during the first 28 days may play a role in reducing the duration of mechanical ventilation in extremely low birth-weight infants, and it may lead to a reduced oxygen depen-dency in the 700- to 1000-g birth weight strata.
www.pediatrics.org/cgi/doi/10.1542/ peds.2005-2923
doi:10.1542/peds.2005-2923
This work was presented in part at the meeting of the Society of Pediatric Research; May 1– 4, 2004; San Francisco, CA.
Key Words
mechanical ventilation, synchronized intermittent mandatory ventilation, pressure support, preterm infant, weaning, supplemental oxygen
Abbreviations
SIMV—synchronized intermittent mandatory ventilation PIP—peak inspiratory pressure PS—pressure support BW— birth weight
PIE—pulmonary interstitial emphysema HFOV— high-frequency oscillatory ventilation
PEEP—positive end-expiratory pressure FIO2—fraction of inspired oxygen SPO2—arterial oxygen saturation by pulse oximetry
VT—tidal volume
PaCO2—arterial carbon dioxide tension PMA—postmenstrual age IVH—intraventricular hemorrhage PDA—patent ductus arteriosus NEC—necrotizing enterocolitis ROP—retinopathy of prematurity A/C—assist/control
Accepted for publication May 23, 2006 Address correspondence to Eduardo Bancalari, MD, Division of Newborn Medicine, Department of Pediatrics, University of Miami Miller School of Medicine, PO Box 016960 R-131, Miami, FL 33101. E-mail: ebancalari@ miami.edu
D
ESPITE THE EMERGENCEof new modes of mechani-cal ventilation, the optimal ventilatory strategy that can provide adequate ventilation and minimize the risk of lung injury in premature infants with respiratory failure has not been identified. Synchronized intermit-tent mandatory ventilation (SIMV) is one of the most widely used modalities of respiratory support and has been found to reduce the duration of mechanical venti-lation compared with conventional intermittent manda-tory ventilation.1,2 SIMV weaning in preterm infants is achieved by a gradual reduction of the SIMV rate and peak inspiratory pressure (PIP) while the infants in-crease their spontaneous ventilation. This weaning pro-cess can be slowed by the inability of these infants to cope with the increased work of breathing because of the resistance of small endotracheal tubes, elevations in lung elastance and airway resistance induced by disease, in-creased dead space, and poor chest wall stability.3–10Pressure support (PS) assists every spontaneous breath by providing an inspiratory pressure boost aimed at reducing work of breathing.11–13PS has been shown to augment spontaneous ventilation in neonates with con-genital heart disease14and decrease the work of breath-ing in children durbreath-ing cardiac surgery.15
The short-term effects of combining SIMV and PS (SIMV⫹PS) in preterm infants were investigated previ-ously.16 The combined SIMV⫹PS maintained adequate ventilation and gas exchange while simultaneously pre-venting an increase in inspiratory effort during an acute reduction in SIMV rate. These findings support the use of PS as a supplement to SIMV to facilitate weaning from ventilatory support. This may be important in preterm infants in whom accelerated weaning and an exposure to lower SIMV rates may reduce the risk of lung injury. Therefore, it was hypothesized that SIMV⫹PS, com-pared with SIMV alone, will accelerate weaning from mechanical ventilation and minimize lung injury as in-dicated by a reduced oxygen dependency. The objective of the present study was to compare SIMV⫹PS to SIMV alone in a group of preterm infants with regard to ven-tilator weaning and need for supplemental oxygen.
METHODS
The study was conducted in the Newborn Intensive Care Unit of the University of Miami-Jackson Memorial Med-ical Center between September 2002 and November 2004. The study was reviewed and approved by the University of Miami Institutional Review Board for the Protection of Human Subjects in Research.
Study Population
All of the preterm infants with birth weights (BWs) between 500 and 1000 g who were appropriate for ges-tational age and required mechanical ventilation for⬎12 hours from the first day after birth until day 7 were considered eligible for the study. The exclusion criteria
included the presence of congenital anomalies, neuro-muscular disease, lung hypoplasia, congenital heart dis-ease, and hypotension requiring intravenous medica-tions. Infants were also excluded if they had pulmonary interstitial emphysema (PIE) or pneumothorax, if they required a previous course of ⬎24 hours of high-fquency oscillatory ventilation (HFOV), or if they re-ceived sedation or muscle relaxation. Infants were en-rolled after written informed consent was obtained from the parents or legal guardians.
Design and Randomization
It was estimated that 96 neonates surviving to day 28 needed to be enrolled to show a 30% difference in the duration of oxygen dependency between groups at an␣ of .05 with a power of 90%. After adjustment for center mortality rate in this population of preterm infants, it was estimated that enrollment of 108 infants was nec-essary.
Block randomization within 2 BW strata (500 – 699 and 700 –1000 g) was conducted to assign eligible infants to 1 of 2 modes of mechanical ventilation, SIMV or SIMV⫹PS, using sequential sealed opaque envelopes from a computer-generated randomization list. Caregiv-ers were not blinded to the assigned modality. Stratifi-cation was decided based on the differences in incidence of bronchopulmonary dysplasia and duration of me-chanical ventilation at different BWs.
Ventilatory Management
Mechanical ventilation for all of the infants was pro-vided using time-cycled, pressure-limited, flow-triggered neonatal ventilators (VIP Gold, Viasys Healthcare, Yorba Linda, CA). On randomization, ventilator settings for infants assigned to the SIMV⫹PS group were initially modified as follows: SIMV rate was decreased by 10 breaths per minute, and PS was added at 30% to 50% of the difference between PIP and positive end-expiratory pressure (PEEP) of the SIMV breaths. The initial decrease in rate in the SIMV⫹PS group was used to compensate for the added PS to minimize the increase in mean airway pressure and the risk of hyperventilation. Infants randomly assigned to the SIMV group remained on set-tings as determined by the clinical team.
difference and thereafter maintained at or decreased gradually below this level to a minimum of 30% as tolerated. Surfactant was administered following the center guidelines in both groups of infants as needed.
The decision to remove from mechanical ventilation was left to the discretion of the clinical team. All of the infants received caffeine before extubation and were maintained on nasal continuous positive airway pres-sure for ⱖ48 hours after extubation. Extubated infants who showed signs of respiratory deterioration including an increased oxygen requirement with FIO2 ⬎ 0.5 to maintain SPO2ⱖ88%, or a PaCO2ⱖ65 mm Hg and pH
ⱕ 7.25, or severe apneic episodes requiring bag-mask ventilation were returned to mechanical ventilation. Ventilatory support was resumed using the originally assigned mode, and ventilator management followed the above-mentioned protocol. Infants remained in the as-signed mode until day 28. Thereafter, ventilatory man-agement was left to the discretion of the clinical team, which was allowed to use either mode of ventilation. HFOV was used as rescue intervention only for infants who had PaCO2 ⬎70 mm Hg on 2 consecutive arterial blood gases despite an SIMV rate of 60 breaths per min, SPO2⬍88% on 1.0 FIO2, or for infants who developed PIE. General clinical management, as well as nursing care and monitoring were done according to the center routine protocol throughout the infant’s hospitalization.
Data Collection, Outcomes, and Data Analysis
Daily ventilatory parameters of PIP, PEEP, PS, SIMV rate, mean airway pressure, total respiratory rate, VTof SIMV breaths, SPO2, and FIO2 were documented. Data documentation included arterial or capillary blood gases obtained as per unit protocol or as dictated by the clinical condition. Infants were followed until hospital discharge or death.
Respiratory outcomes were assessed as those occur-ring from birth until day 28 while the study protocol was actively followed and those occurring from birth until discharge or death. Respiratory outcome parameters in-cluded: time to reach a level of minimal ventilator set-tings consisting of PIP ⱕ16 cm H2O, FIO2ⱕ0.30, PEEP
ⱕ5 cm H2O, and SIMV rateⱕ15 breaths per minute and remained on these settings for ⱖ48 hours (the clinical teams were not aware of the existence of this criterion or when an infant had met such criterion); time to first successful extubation (planned or inadvertent) defined as ⱖ48 hours without mechanical ventilation; age of final removal from mechanical ventilation; total cumu-lative duration of mechanical ventilation; ventilator re-quirement at day 28; total cumulative duration of sup-plemental oxygen; and oxygen requirement at day 28 and at 36 weeks’ postmenstrual age (PMA). A ventilator day was defined as any daily period of ⬎12 hours on conventional mechanical ventilation or HFOV. A sup-plemental oxygen day was defined as a daily
require-ment of FIO2⬎0.21 for⬎12 hours. In addition, infants were monitored for the occurrence of respiratory com-plications including pneumothorax and PIE. Morbidity assessment included intraventricular hemorrhage (IVH), patent ductus arteriosus (PDA), sepsis, necrotizing en-terocolitis (NEC), and retinopathy of prematurity (ROP). Data were analyzed on an intention-to-treat basis. Between-group comparisons of continuous variables were conducted using Student’s t test or the nonpara-metric Mann-Whitney rank-sum test for nonnormally distributed data. Categorical variables were compared by
2test or Fisher’s exact test as appropriate. Kaplan-Meier log-rank survival analysis was used to compare be-tween-group data involving the time required to reach the above-mentioned milestones. An overall significance level of 0.05 was used for all of the statistical compari-sons.
RESULTS
A total of 265 infants weighing between 500 and 1000 g at birth were admitted to the newborn intensive care unit during the trial. Of these, 125 infants were eligible for the study. A total of 107 infants were enrolled; 54 were randomly assigned to the SIMV group and 53 to SIMV⫹PS. Eighteen eligible infants were not enrolled: 16 for parental refusal and 2 for inability to get consent on time. A total of 140 infants were excluded from the study. Of these, 60 did not require mechanical ventila-tion during the screening period, 13 infants had congen-ital anomalies, 26 were intrauterine growth retarded, 9 had a recent history of pneumothorax or PIE, and 32 infants were hemodynamically unstable. Among the 140 infants excluded, there were 5 infants for whom consent was obtained but were recognized as ineligible shortly after randomization: 1 was diagnosed with PIE, 1 was inadvertently extubated, 1 developed intractable hypo-tension and died, and 2 infants were diagnosed with large ventricular septal defect with left heart overload. These 5 enrolled infants were randomly assigned, al-though they had met exclusion criteria during the inter-val between enrollment and randomization. They were not included in the analysis. The diagram of Fig 1 illus-trates the flow of participants from screening to study completion.
Population characteristics including BW, gestational age, gender, exposure to antenatal steroids and maternal chorioamnionitis, and surfactant treatment were not dif-ferent between the SIMV and SIMV⫹PS groups. At the time of random assignment, infants in both groups had comparable ages and were on similar ventilator settings (Table 1). Surfactant was administered therapeutically. Only 2 infants (1 per group) received surfactant after random assignment.
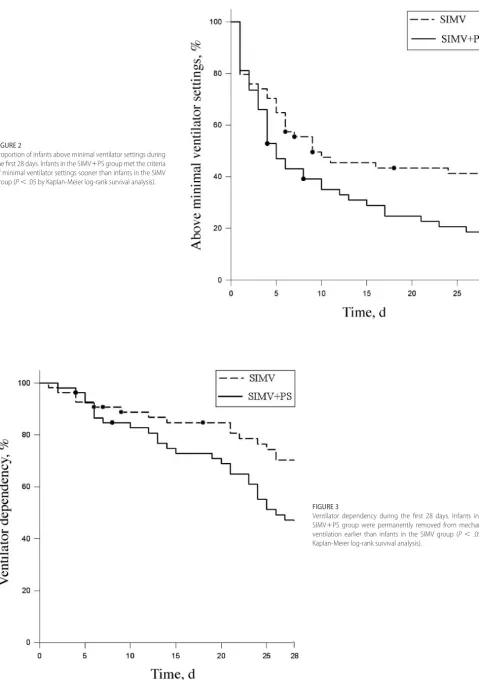
the SIMV⫹PS group reached the criteria of minimal ventilator settings earlier (Fig 2) and were permanently removed from mechanical ventilation sooner (Fig 3) than infants in the SIMV group.
When comparing the SIMV rates used to support infants during the first 28 days, the SIMV rates for in-fants in SIMV⫹PS were significantly lower than those for the SIMV group on days 4, 7, and 10 (Fig 4), whereas PaCO2levels did not differ between groups. Median PIP
and VTof SIMV breaths during the first 28 days did not differ between groups. PIP of the SIMV breaths were maintained within 15 and 18 cm H2O and VTwithin 4.6 and 7.0 mL/Kg (25th and 75th percentile) in both groups.
By design, ventilator rate was reduced immediately after random assignment by 10 breaths per minute in all of the infants in the SIMV⫹PS group. Weaning also occurred in the SIMV group, where 44% of the infants FIGURE 1
Flow of participants from screening to study completion.
TABLE 1 Population Characteristics
Characteristic All Infants BW 500–699 g BW 700–1000 g
SIMV (n⫽54)
SIMV⫹PS (n⫽53)
SIMV (n⫽23)
SIMV⫹PS (n⫽22)
SIMV (n⫽31)
SIMV⫹PS (n⫽31)
Birth weight, g 722⫾125 749⫾134 600⫾53 615⫾46 812⫾77 844⫾85
Gestational age, wk 25.0⫾1.4 25.4⫾1.3 24.0⫾1.0 24.5⫾1.0 25.8⫾1.0 26⫾1.1
Female gender 27 (50) 23 (43) 13 (56) 11 (50) 14 (45) 12 (39)
Antenatal steroids 49 (91) 47 (89) 19 (83) 20 (91) 30 (97) 27 (87)
Surfactant 38 (70) 42 (79) 19 (83) 17 (77) 19 (61) 25 (81)
Maternal chorioamnionitis 8 (15) 7 (13) 3 (13) 3 (14) 5 (16) 4 (13)
At randomization
Age, h 33⫾30 34⫾29 32⫾21 26⫾14 33⫾35 39⫾35
FIO2 0.25⫾0.06 0.28⫾0.09 0.27⫾0.06 0.26⫾0.06 0.24⫾0.06 0.30⫾0.11
SIMV rate, breaths per min 24⫾10 26⫾11 25⫾10 27⫾11 24⫾9 25⫾10
Mean airway pressure, cm H2O 6.4⫾1.1 6.5⫾1.3 6.3⫾1.1 6.4⫾1.1 6.4⫾1.0 6.6⫾1.4
FIGURE 3
Ventilator dependency during the first 28 days. Infants in the SIMV⫹PS group were permanently removed from mechanical ventilation earlier than infants in the SIMV group (P⬍.05 by Kaplan-Meier log-rank survival analysis).
FIGURE 2
in the SIMV group had a reduction in rate right after random assignment, and 55% were on a lower rate 12 hours later. Not every infant in the SIMV⫹PS group tolerated the initial weaning, and 24% of them were with a higher ventilator rate 12 hours after random assignment.
Table 2 shows respiratory outcomes assessed during the first 28 days after birth. The proportion of infants requiring mechanical ventilation at day 28 was lower in the SIMV⫹PS group (47% vs 69%;P⬍.04). The dura-tion of mechanical ventiladura-tion and supplemental oxygen during the first 28 days and oxygen need at day 28 did not differ significantly between groups. Respiratory out-comes assessed during the first 28 days within each BW strata did not differ significantly between groups.
Table 3 shows the respiratory outcomes assessed from birth until discharge or death. The age when infants were permanently removed from mechanical ventilation and the total duration of mechanical ventilation did not differ significantly between groups. Although infants in SIMV⫹PS had a shorter median duration of supplemen-tal oxygen, and a smaller proportion of them required oxygen at 36 weeks’ PMA, these differences were not statistically significant. Similarly, the combined outcome of death or oxygen at 36 weeks’ PMA was not different. Most outcomes assessed from birth to discharge or death within each BW strata did not differ between groups. However, the SIMV⫹PS group had a shorter duration of oxygen dependency compared with the SIMV group within the 700- to 1000-g BW strata.
FIGURE 4
A, SIMV rate; B, PaCO2levels during the first 28 days after
birth. For infants who remained on conventional mechan-ical ventilation, the SIMV rate (median, 25th–75th percen-tile) was lower in the SIMV⫹PS group on days 4, 7, and 10 after birth, while levels of PaCO2did not differ between
groups.aP⬍.05 by Mann-Whitney rank-sum test.
TABLE 2 Respiratory Outcomes Assessed During the First 28 Days After Birth for All Infants and Within BW Strata
Variable All Infants BW 500–699g BW 700–1000 g
SIMV (n⫽54)
SIMV⫹PS (n⫽53)
P SIMV
(n⫽23)
SIMV⫹PS (n⫽22)
P SIMV
(n⫽31)
SIMV⫹PS (n⫽31)
P
Days on mechanical ventilation
25 (17–28) 20 (10–28) .175a 28 (27–28) 28 (23–28) .349a 20 (8–28) 12 (6–20) .132a
On mechanical ventilation at day 28 34 (69) 24 (47) .04b 18 (95) 15 (71) .095c 16 (53) 9 (30) .116b
Days on supplemental oxygen 25 (18–28) 23 (19–26) .355a 25 (22–27) 24 (22–26) .351a 23 (17–27) 22 (18–25) .52a
On supplemental oxygen at day 28 43 (88) 43 (86) .969b 19 (100) 18 (86) .233c 24 (80) 25 (86) .73c
Results are expressed as median (25th–75th percentile) orn(%) on infants alive at day 28. aMann-Whitney rank-sum test.
As the study protocol was followed until day 28, the clinical team subsequently determined the ventilatory modality. Among infants alive at day 28, 19 (39%) in the SIMV group and 12 (24%) in the SIMV⫹PS group were subsequently switched to the other modality. After day 28, infants required mechanical ventilation for a median (25th–75th percentile) duration of 26 (15– 44) and 13 (5–51) days in the SIMV and SIMV⫹PS group, respectively. The median (25th–75th percentile) venti-lator rate at extubation was 15 (15–15) in the SIMV group compared with 10 (10 –15) breaths per minute in the SIMV⫹PS group (P⬍.001).
Overall mortality and death before day 28 did not differ between groups. No infant developed pneumotho-rax, and the proportion of infants who developed PIE was not different between groups. HFOV was used as a rescue intervention in 23% of all infants. This was mainly indicated for persistent hypercapnia. The propor-tion of infants requiring HFOV did not differ between groups. The rates of other morbidities including sepsis, PDA, IVH grade III or higher, NEC, and ROP stage III or greater were not different between groups (Table 4).
The rate of endotracheal colonization was 76% and 81% in the SIMV and SIMV⫹PS groups, respectively. Systemic infections were diagnosed in 66% and 67% of the infants in the SIMV and SIMV⫹PS groups, respec-tively. Postnatal steroids were given to 11% and 6% of the infants in the SIMV and SIMV⫹PS groups, respec-tively.
DISCUSSION
The results of this randomized, controlled trial indicate that the use of PS in addition to SIMV during the first 28 days allowed for an earlier reduction in ventilatory sup-port and a shorter ventilator dependency compared with SIMV alone in a group of extremely low BW infants. This combined strategy also allowed maintenance of a lower SIMV frequency compared with SIMV alone dur-ing the first 10 days.
In a previous pilot study, a similar range of PS as the one used in the present trial was shown to unload the
respiratory pump and maintain spontaneous VTwithin a reference range during an acute reduction in SIMV rate in preterm infants with different stages of lung disease.16 In this study, PS was purposely maintained at a fraction of the SIMV pressure amplitude. This was done to avert exposure to higher peak pressures in the range of those of the SIMV breaths. Thus, in this trial, the combined use of SIMV and PS was not only intended to accelerate weaning but also to provide a more lung-protective ven-tilatory support by reducing exposure to the larger SIMV breaths.
The mechanisms by which PS can facilitate weaning are multiple. In addition to facilitating maintenance of a consistent spontaneous VT and better alveolar ventila-tion than during SIMV alone without the need for an increase in breathing effort, PS may attenuate the tho-racoabdominal asynchrony often observed in preterm infants. Because spontaneous minute ventilation de-pends on proper diaphragmatic function, PS may also avert diaphragm overexertion and fatigue because of the increased work of breathing that occurs during SIMV weaning. Also, a more consistent spontaneous breathing and reduced reliance on SIMV breaths can preserve di-aphragm conditioning and avert didi-aphragmatic
dysfunc-TABLE 4 Mortality, Morbidity, and Respiratory Complications
Variable SIMV (n⫽54),
n(%)
SIMV⫹PS (n⫽53),
n(%)
P
Mortality 7 (13) 6 (11) .971a
Death during first 28 d 5 (9) 2 (4) .449a
Pneumothorax 0 0
Pulmonary interstitial emphysemab 7 (14) 5 (10) .703a
HFOV need during first 28 d of lifeb 15 (30) 10 (20) .299a
PDA during first 28 d of lifeb 42 (86) 45 (88) .938a
Required PDA ligationb 16 (33) 12 (24) .428a
IVH grade III and IV 10 (19) 9 (17) .964a
NEC 5 (11) 7 (13) .733a
ROP stageⱖ3c 21 (45) 21 (45) .836a
a2test.
bOn infants alive at day 28. cOn infants alive at discharge.
TABLE 3 Respiratory Outcomes Assessed From Birth Until Discharge or Death for All Infants and Within Birth Weight Strata
Variable All Infants BW 500–699 g BW 700–1000 g
SIMV (n⫽54)
SIMV⫹PS (n⫽53)
P SIMV
(n⫽23)
SIMV⫹PS (n⫽22)
P SIMV
(n⫽31)
SIMV⫹PS (n⫽31)
P
Age at final extubation, d 44 (25–73) 35 (14–74) .91a 58 (39–110) 68 (35–110) .73a 29 (21–53) 24 (10–40) .366a
Days on mechanical ventilationb 34 (19–59) 22 (10–52) .18c 57 (34–81) 51 (25–85) .85c 25 (8–47) 15 (6–23) .118c
Days on supplemental oxygenb 72 (46–96) 49 (38–87) .11c 85 (55–138) 86 (56–140) .98c 58 (44–87) 41 (34–51) .034c
On oxygen at 36 weeks’ PMAd 23 (48) 16 (33) .21e 12 (63) 11 (58) 1.0e 11 (38) 5 (17) .142e
Results are expressed as median (25th to 75th percentile) orn(%). aLog-rank survival analysis.
tion as observed during prolonged ventilator dependen-cy.17
With the underlying assumption that the combined SIMV⫹PS would result in a more lung-protective ven-tilatory support, it was expected that the potential ben-eficial effects would be reflected in a reduced oxygen dependency. Although the duration of oxygen depen-dency and oxygen need at 36 weeks’ PMA were not lower in the SIMV⫹PS group, there was a significant reduction in oxygen dependency in SIMV⫹PS infants within the 700- to 1000-g BW strata. The observed benefit of SIMV⫹PS in the larger infants may have re-sulted from a more consistent respiratory drive and di-aphragmatic function compared with the smaller and more immature infants. This may have allowed PS, a patient-triggered modality, to function more effectively in assisting spontaneous inspiration.
In a randomized, controlled trial that compared vol-ume-targeted to pressure-limited ventilation in preterm infants,18PS was used in the weaning phase, which may have contributed to the faster weaning. Although those infants were more mature than the infants in the present study, those findings are in agreement with the present results.
Although PS can be used independently of SIMV, in this study the use of the combined SIMV⫹PS strategy was intended to provide a background level of minimum ventilation. This may be particularly important when used in preterm infants with unstable respiratory drive or insufficient breathing effort to trigger the ventilator adequately to maintain ventilation and gas exchange. Newer infant ventilators can provide a backup ventila-tory rate during PS ventilation, but the effects of such a strategy remain to be explored.
Assist/control (A/C), a widely used ventilatory mo-dality in preterm infants, provides mechanical unloading to every spontaneous inspiration similarly to PS and a controlled backup ventilatory rate in the absence of spontaneous breathing. A/C weaning, like in PS, consists of a gradual reduction in PIP, which applies to both assist and control type of breaths. PIP levels during A/C could reach similar low levels as those of PS used in the present study. However, in the absence of spontaneous inspira-tory effort, the backup control breaths may not provide sufficient ventilation unless the backup rate is set at levels near the spontaneous breathing frequency. This differs from SIMV⫹PS as used in the present study where the PIP of SIMV breaths maintained sufficient VT in the absence of the spontaneous contribution at rela-tively low SIMV rates. Although this does not necessarily support the use of higher PIP for SIMV breaths, it sug-gests further investigation on the relevance of maintain-ing a minimum SIMV rate.
A trial of this nature is limited by the inability to blind the investigators and the clinical team; therefore, the existence of bias cannot be entirely ruled out. To
ame-liorate this, a weaning protocol was formulated and agreed by consensus between the investigators and clin-ical team. It can be argued that the initial reduction in ventilator rate in the SIMV⫹PS group after random as-signment could have lead to faster weaning. However, weaning also occurred in the SIMV group, suggesting absence of bias in the management of the ventilator rate during the postrandomization period. To detect bias, specific data were collected. More aggressive rate wean-ing in the SIMV⫹PS group or slower rate weaning in the SIMV group would have resulted in differences in ven-tilator rate or PaCO2levels. However, PaCO2levels were strikingly similar between groups, and ventilator rate differed only at days 4, 7, and 10. Most importantly, although the clinical team weaned both groups of in-fants using the same criteria, they were not aware of the criterion used to define minimal ventilatory support or when an infant had reached those settings.
In this study, the decision to extubate was left to the clinical team to minimize the influence of any existing bias in the research team, but the existence of bias in the timing of extubation cannot be entirely ruled out. A bias toward SIMV⫹PS is likely to have resulted in extubation from higher ventilator rates. However, the ventilator rate at the time of extubation was lower in the SIMV⫹PS group. Bias in the ventilator management is unlikely to have played a role in the total duration and final re-moval from supplemental oxygen, because for most in-fants the duration of oxygen exceeded the duration of ventilation, and the removal from oxygen occurred at a later time.
The study protocol was followed until day 28, and subsequently the clinical team determined the modality of ventilation. This study design was aimed at evaluating the use of a potentially gentler ventilatory strategy dur-ing the early postnatal period when lung protection may play a more important role. This is perhaps a limitation of the study, because one could speculate that more striking differences could have been obtained, particu-larly in the smaller BW strata, if the intervention had lasted longer. As a greater proportion of infants in the SIMV group were switched to the alternate experimental modality, this may have also attenuated the differences in respiratory outcome between the 2 groups.
Although the rate of surfactant administration did not differ between groups, it was higher in the SIMV⫹PS group, particularly within the 700- to 1000-g strata. In this center, surfactant is used only therapeutically, and the greater proportion of infants who required surfac-tant in the SIMV⫹PS group correlates with the higher mean FIO2at random assignment.
in this study represent most infants in that BW group who survive for at least the first 28 days and require mechanical ventilation and oxygen for a significant pe-riod of time. This is the group of infants who are at higher risk for lung injury and bronchopulmonary dys-plasia and could benefit most from prompt weaning of the ventilatory support.
CONCLUSIONS
The results of this study suggest that the addition of pressure support as a supplement to SIMV during the first 28 days may play a role in reducing the duration of mechanical ventilation in extremely low BW infants, and it may reduce oxygen dependency among infants in the 700- to 1000-g BW strata. These data underline the relevance of lung protective ventilatory strategies during the early course of mechanical ventilation in preterm infants. Given the multifactorial nature of lung injury in premature infants and its sequelae, these results need to be further confirmed.
ACKNOWLEDGMENTS
Support for this work was provided by the University of Miami Project NewBorn. Equipment was provided by Viasys Healthcare.
We thank the neonatologists, fellows, nurses, and respiratory therapists of the University of Miami/Jackson Memorial Medical Center NICU for their support. We thank Dr Tilo Gerhardt for thoughtful review of the manuscript. We are particularly grateful to the infants who participated in this trial and their parents or legal guardians for their trust.
REFERENCES
1. Bernstein G, Mannino F, Heldt G, et al. Randomized multi-center trial comparing synchronized and conventional inter-mittent mandatory ventilation in neonates.J Pediatr.1996;128: 453– 463
2. Chen JY, Ling UP, Chen JH. Comparison of synchronized and conventional intermittent mandatory ventilation in neonates.
Acta Pediatr Jpn.1997;39:578 –583
3. Roze JC, Liet JM, Gournay V, Debillon T, Gaultier C. Oxygen cost of breathing and weaning process in newborn infants.Eur Respir J.1997;10:2583–2585
4. LeSouef PN, England SJ, Bryan AC. Total resistance of the respiratory system in preterm infants with and without an endotracheal tube.J Pediatr.1984;104:108 –111
5. Oca MJ, Becker MA, Dechert RE, Donn S. Relation of neonatal endotracheal tube size and airway resistance.Respir Care.2002; 47:994 –997
6. Heldt GP, Mcllroy MB. Distorsion of chest wall and work of diaphragm in preterm infant.J Appl Physiol.1987;62:164 –169 7. Kiciman NM, Andre´asson B, Bernstein G, et al. Thoracoab-dominal motion in newborns during ventilation delivered by endotracheal tube or nasal prongs.Pediatr Pulmonol.1998;25: 175–181
8. Carlo WA, Martin RJ, Versteegh FGA, Goldman MD, Robert-son SS, Fanaroff AA. The effect of respiratory distress syndrome on chest wall movements and respiratory pauses in preterm infants.Am Rev Respir Dis.1982;126:103–107
9. Deoras KS, Greenspan JS, Wolfson MR, Keklikian E, Shaffer TH, Allen JL. Effects of inspiratory resistive loading on chest wall motion and ventilation: differences between preterm and full-term infants.Pediatr Res.1992;32:589 –594
10. Numa AH, Newth CJ. Anatomic dead space in infants and children.J Appl Physiol.1996;80:1485–1489
11. Dekel B, Segal E, Perel A. Pressure support ventilation.Arch Int Med.1996;156:369 –373
12. Brochard L, Rua F, Lorina H, Lemaire F, Harf A. Inspiratory pressure support compensates for the additional work of breathing caused by the endotracheal tube. Anesthesiology.
1991;75:739 –745
13. Brochard L, Harf A, Lorino H, Lemaire F. Inspiratory pressure support prevents diaphragmatic fatigue during weaning from mechanical ventilation.Am Rev Respir Dis.1989;139:513–521 14. Tokioka H, Kinjo M, Hirakawa M. The effectiveness of pressure
support ventilation for mechanical ventilatory support in chil-dren.Anesthesiology.1993;78:880 – 884
15. Tokioka H, Nahano O, Ohta Y, Hirakawa M. Pressure support ventilation augments spontaneous breathing with improved thoracoabdominal synchrony in neonates with congenital heart disease.Anesth Analg.1997;85:789 –793
16. Osorio W, Claure N, D’Ugard C, Athavale K, Bancalari E. Effects of pressure support during an acute reduction of syn-chronized intermittent mandatory ventilation in preterm in-fants.J Perinat.2005;25:412– 416
17. Knisely AS, Leal SM, Singer DB. Abnormalities of diaphrag-matic muscle in neonates with ventilated lungs.J Pediatr.1988; 113:1074 –1077
DOI: 10.1542/peds.2005-2923
2006;118;1409
Pediatrics
Vanbuskirk and Eduardo Bancalari
Zenaida C. Reyes, Nelson Claure, Markus K. Tauscher, Carmen D'Ugard, Silvia
Support in Preterm Infants
Ventilation and Synchronized Intermittent Mandatory Ventilation Plus Pressure
Randomized, Controlled Trial Comparing Synchronized Intermittent Mandatory
Services
Updated Information &
http://pediatrics.aappublications.org/content/118/4/1409 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/118/4/1409#BIBL This article cites 18 articles, 2 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neonatology_sub Neonatology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2005-2923
2006;118;1409
Pediatrics
Vanbuskirk and Eduardo Bancalari
Zenaida C. Reyes, Nelson Claure, Markus K. Tauscher, Carmen D'Ugard, Silvia
Support in Preterm Infants
Ventilation and Synchronized Intermittent Mandatory Ventilation Plus Pressure
Randomized, Controlled Trial Comparing Synchronized Intermittent Mandatory
http://pediatrics.aappublications.org/content/118/4/1409
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.