The Influence of Hospital Practices on Breastfeeding Among Non-Hispanic Black Women
Neha Verma
A thesis submitted to the faculty of the University of North Carolina at Chapel Hill
in partial fulfillment of the requirements for the degree of Bachelor of Science in
Public Health in the Gillings School of Global Public Health (Nutrition).
Chapel Hill 2015
Approved by:
____________________ Margaret Bentley, Advisor
____________________
Abstract
NEHA VERMA: The Influence of Hospital Practices on Breastfeeding Among Non-Hispanic Black Women (Under the direction of Margaret Bentley and Heather Wasser) The purpose of this study was to examine the influence of hospital practices on breastfeeding initiation and breastfeeding at hospital discharge among Non-Hispanic Black (NHB) women. Data was gathered as part of the Mothers and Others: Family-Based Obesity Prevention for Infants and Toddlers study, an ongoing randomized
controlled trial among 468 NHB women. The current study used preliminary data obtained from 99 women through survey
questionnaires. Data revealed a breastfeeding initiation rate of 88.9%, while the rate of breastfeeding at hospital discharge was determined to be 59.1%. While no hospital practices were significantly associated with breastfeeding initiation in bivariate analysis, pacifier use and rooming in were significantly associated with breastfeeding at
hospital discharge. Despite widespread recognition of the associated health benefits, breastfeeding rates in the United States remain suboptimal, with rates lowest among NHB women. Our preliminary data suggests the important influence the hospital setting may have on breastfeeding outcomes.
Table of Contents I.
Introduction... ...1
II.
Methods... ...3
III.
Results... ...7
IV.
Discussion... ...8
V.
Conclusion... ...11
VI.
Tables... ...12
I. Introduction
The benefits of breastfeeding for both the mother and child are widely recognized in the United States.1 Given the health benefits, the World Health Organization and the American Academy of Pediatrics recommend exclusive breastfeeding for the first six months of age.1, 2 However, according to the CDC, among infants born in 2011, 79.2% began breastfeeding, and only 53.2% breastfed exclusively for one month.3 Racial disparities exist within breastfeeding initiation and duration rates, and rates are typically lowest among Non-Hispanic Black (NHB) women. In 2011, NHB women had the lowest rates of breastfeeding initiation of any race at 61.6%, as compared to 81.1% and 83.8% for whites and Hispanics, respectively.3
Research has been conducted regarding the relationship between factors surrounding labor and delivery and breastfeeding, but results have been inconsistent. Some studies show an inverse relationship between cesarean delivery and breastfeeding outcomes,4, 5 while others show no association.6, 7 Similarly, some studies have found an inverse relationship between epidural analgesia and breastfeeding outcomes,8,9 while others show no association.10,11 Much of the previous research on this topic deals with the “Baby-Friendly”
Health Organization and the United Nations Children’s Fund. The initiative includes specific maternity care recommendations for promoting breastfeeding in hospitals: help mothers initiate breastfeeding within one hour of birth, show mothers how to
day. These recommendations have been consistently associated with positive breastfeeding outcomes.12, 13 When considering the influence of factors surrounding labor and delivery on breastfeeding, it is important to note that in addition to having their own individual effects, some of these factors have been found to intersect; for example, while in-hospital formula supplementation has been
negatively associated with breastfeeding outcomes, women who have caesarean births are more likely to receive formula from the
hospital.14
The purpose of this study is to examine the influence of hospital practices on breastfeeding initiation and breastfeeding at hospital discharge, specifically among NHB women. Despite racial disparities in breastfeeding rates, limited research has been done on this topic looking specifically at NHB women. In examining hospital practices, emphasis will be placed on type of delivery and presence of a doula during birth, as well as selected “Baby-Friendly” Hospital practices: timing of skin-to-skin contact, timing of breastfeeding initiation, pacifier use in the hospital, practicing “rooming in,” contact with a lactation consultant during the hospital stay, and receipt of free samples of formula or coupons for formula from the hospital.
II. Methods
Study Participants
The study population was drawn from Mothers and Others: Family-based Obesity Prevention for Infants and Toddlers, a randomized
controlled trial among 468 NHB women, their families, and their child caregivers to test the efficacy of a multi-component, tailored
intervention in promoting healthy weight gain patterns during infancy. Criteria for participation in the Mothers and Others study included NHB women with a singleton pregnancy; English-speaking; and less than 28 weeks pregnant. Exclusion criteria included
prematurity (gestation less than 36 weeks); newborn nursery, NICU, or maternity stay greater than 7 days; or diagnosis of a congenital anomaly or other condition that significantly affects feeding (e.g. Down’s syndrome, cleft lip or palate). Study participants were recruited from women seeking prenatal care through the Maternal Fetal Medicine Unit (MFMU) Network in the Piedmont area of North Carolina. The current study focused on a subset of mothers from Mothers and Others who had completed the baseline surveys,
collected at 26-30 weeks gestation, and neonatal surveys, collected at 2-4 weeks postpartum, by February 13, 2015. Analyses were
sample of women with complete data on all exposure and outcome variables (n= 99).
Study Measures and Variables
Breastfeeding Outcomes
hospital practices affect breastfeeding. Breastfeeding initiation was defined as whether or not breastfeeding was attempted, while
breastfeeding at hospital discharge was defined as any continued breastfeeding at time of discharge from the hospital. These variables were measured by maternal self-report using items from the Infant Feeding Practices Study II (IFPS-II), a nationally representative longitudinal survey of pregnant women and new mothers conducted by the U.S. Food and Drug Administration. For breastfeeding
initiation, mothers were asked, “Did you ever breastfeed or try to breastfeed your baby?” (Yes/No). For breastfeeding at time of
discharge, mothers were asked, “When you left the hospital or birth center, how were you feeding your baby?”(Breastfeeding
Only/Formula Feeding Only/Both Breast and Formula Feeding).
Hospital Practices
The main independent variables included an array of hospital practices that have been previously shown to impact breastfeeding status or that are considered to be clinically important. These variables were also measured via maternal self-report using items from the IFPS-II: mode of delivery, presence of doula during delivery, pacifier use during hospital stay, provision of a gift pack containing formula or coupons for formula, breastfeeding within one hour of delivery, 24-hour rooming-in, any assistance with breastfeeding, and
assistance with breastfeeding from a certified lactation consultant. Mothers were asked: “How was your baby delivered?” (Vaginally and not induced/Vaginally and induced/A planned caesarean/An unplanned or emergency cesarean); “Other than the medical staff, who was with you during your labor? Please check all that apply.” (The baby’s
father/Your mother (baby’s maternal grandmother)/The baby’s
doula/No one other than medical staff); “While in the hospital or birth center, was your baby given a pacifier?” (Yes/No/Don’t Know); “Did you receive a gift pack or diaper bag from the hospital or birth
center? Include a gift pack from a childbirth class if you took the class at the hospital or birth center.” (Yes/No); “Were any of the following included in the gift pack? If you received more than one gift pack from the hospital or birth center, answer for all that you received. Please check all that apply.” (Infant formula/Coupon for infant
formula/Breastfeeding supplies (nursing pads, nipple cream, etc.); “About how long after your delivery did you breastfeed or try to breastfeed for the very first time?” (Less than 30 min/30 to 60 min/1 to 2 hours/3 to 6 hours/7 to 12 hours/13 to 24 hours/1 day/2
days/More than 2 days); “While you were in the hospital or birth center, did your baby stay in your room day and night, except for doctor visits, bathing, or other treatments?” (Yes, all the time/Yes, some nights but not all/No); “While you were in the hospital for delivery of this baby, did anyone help you with breastfeeding by showing you how or talking to you about breastfeeding?” (Yes/No); and “Who helped you with breastfeeding while in the hospital? Please check all that apply.” (Doctor/Midwife/Nurse/Lactation
consultant/Peer counselor/Family member(s)/Friend(s)/Breastfeeding support group member).
Covariates
Control variables included maternal age, maternal education, maternal relationship status, maternal smoking, maternal overweight/ obesity, maternal depressive symptoms, maternal breastfeeding intention scale score, infant birth weight, infant gender, and infant jaundice in the hospital.12
Statistical Analyses
Descriptive statistics were used to assess breastfeeding outcomes, hospital practices and important sample
characteristics/covariates. Bivariate analyses tested for associations between the outcome variables and each exposure and sample
characteristic. Student's t-tests were used for continuous variables and chi-squared or Fisher's exact tests were used for categorical variables. For each hospital practice found to be significantly
associated with a breastfeeding outcome in the bivariate analyses, a multivariable logistic regression model was run to test whether associations remained significant after controlling for important sample characteristics/covariates. Covariates were included if found to be significantly associated with the breastfeeding outcome at p<.10. Due to the limited sample size, statistical significance for outcome-exposure associations in the multivariable model was set at p<.10. Stata 12 (Stata Corp, College Station, TX) was used for all analyses.
III. Results
The study sample consisted of 99 Non-Hispanic Black women. Participants were fairly young, with a mean age of 25.1±5.1 (Table 1). Of the study population, 50.5% of mothers had received less than or equal to a high school education and 70.7% of mothers had a single or separated relationship status. A total of 9.2% of mothers were
smoking and 61.7% of mothers were overweight or obese.
The overall rate of breastfeeding initiation among the study sample was 88.9% (Table 1). Sample characteristics significantly associated with breastfeeding initiation were a higher level of maternal
education and a higher maternal breastfeeding intention scale score at baseline (26-30 weeks pregnancy). No hospital practices were significantly associated with breastfeeding initiation.
The overall rate of breastfeeding at hospital discharge was 59.1% (Table 1). Sample characteristics significantly associated with breastfeeding at hospital discharge were higher maternal age, a married or domestic partnership relationship status, presence of maternal depressive symptoms*, higher maternal breastfeeding
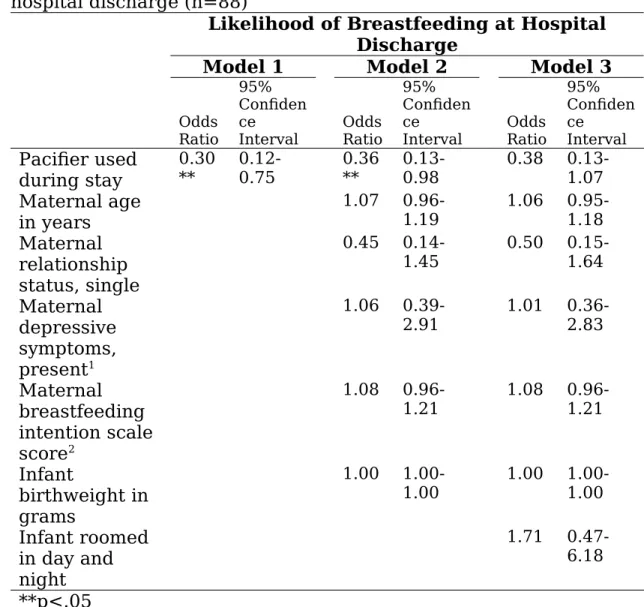
Mother-infant pairs given a pacifier in the hospital were 20.0% less likely to be breastfeeding at hospital discharge (Table 1). Pacifier use
IV. Discussion
This study examined the influence of hospital practices on breastfeeding initiation and breastfeeding at hospital discharge among NHB women.
At 88.9%, our sample had a higher rate of breastfeeding initiation than North Carolina’s Non-Hispanic Black breastfeeding initiation rate of 77.2% and the national Non-Hispanic Black average of 79.2%. 15 While studies often do not make a distinction between breastfeeding initiation and breastfeeding at hospital discharge because of the short period of time between the two, we documented that a large
proportion of women who had initiated breastfeeding in the hospital were no longer breastfeeding at the time of hospital discharge, illustrating the important influence of the hospital setting on breastfeeding outcomes. While 88.9% of women in our sample initiated breastfeeding, only 59.1% were still breastfeeding at the time of hospital discharge. These findings suggest that perhaps the period of time women spend in the hospital after delivery is a critical window for influencing breastfeeding outcomes. The Surgeon
discharge was 59.1%, but this may be due to a confluence of factors in our sample that have been shown to be negatively associated with breastfeeding, namely race/ethnicity, low education level and a single relationship status.
Sample characteristics significantly associated with breastfeeding initiation were a higher level of maternal education and a higher maternal breastfeeding intention scale score at baseline (26-30 weeks pregnancy). For breastfeeding at hospital discharge, significant
presence of maternal depressive symptoms*, higher maternal breastfeeding intention scale score, and lower infant birth weight. These findings are similar to those of Hauck et al, 6 who found that lower maternal education levels and younger maternal age are
associated with early breastfeeding cessation. They are also similar to those of Parry et al, 14 who found that higher infant birth weight is associated with in-hospital formula supplementation. Perhaps this is because infants of higher birth weight are perceived as having higher calorie needs, and mothers worry that breast milk alone will not be sufficient.
We did not find that any hospital practices were significantly associated with breastfeeding initiation, while hospital practices significantly associated with breastfeeding at hospital discharge were lack of pacifier use in the hospital and 24-hour rooming in. Perhaps hospital practices affect breastfeeding at hospital discharge more significantly than breastfeeding initiation because hospital practices have the most potential to influence women in the short period
between delivery and discharge from the hospital. These findings are similar to those of DiGirolamo et al,12 who found that lack of pacifier use in the hospital and 24-hour rooming in were both associated with longer breastfeeding duration, with pacifier use being more
consistently associated than 24-hour rooming in. These findings are also similar to those of Butler et al,4 who found that lack of
rooming in was associated with early breastfeeding cessation. In general, these findings add to a growing body of research12, 13 supporting the maternity care recommendations outlined by the “Baby-Friendly” Hospital Initiative in promoting breastfeeding in the hospital, specifically lack of pacifier use and 24-hour rooming in. When considering this, it is also important to note that at UNC, which is designated a “Baby-Friendly Hospital,” the rate of breastfeeding initiation was 13.9% higher than that of Wake Med, which is not designated a “Baby-Friendly” Hospital. Similarly, the rate of
As an observational study, this investigation allowed us to
simultaneously consider a wide variety of sample characteristics and hospital practices and how they relate to breastfeeding outcomes. At the same time, this study did have some limitations. A major limitation of this preliminary study is the small sample size, which reduces power to detect significant differences. These important analyses will be repeated at the end of the study period. Additionally, data on hospital practices was collected by maternal self-report, and a mother’s perception of her experiences in the hospital may be different from the actual services received.12
V. Conclusion
Our study adds to the growing literature on the important influence of the hospital setting on breastfeeding outcomes. The period of time between delivery and discharge from the hospital may be a critical window for continued breastfeeding and may be influenced by hospital practices. Our results suggest that the “Baby-Friendly” Initiative’s recommendations for lack of pacifier use in the hospital and 24-hour rooming in are positively associated with breastfeeding at hospital discharge. Future studies should assess whether a similar pattern of results is found with one-week and one-month
VI. Tables
Table 1. Sample characteristics and bivariate associations with breastfeeding initiation and breastfeeding at hospital discharge. Sample
Characteristic Total Sample (n=99)
Breastfeeding
Initiation Breastfeeding at Discharge
% (n) or mean±S D Yes 88.9% (n=88) No 11.1% (n=11) Yes 59.1% (n=52) No 40.9% (n=36) Treatment group Intervention
Control 55.6 (55) 44.4 (44)
90.9
86.4 9.113.6 54.065.8 46.034.2
Maternal variables
Maternal age 25.1±5.
1 25.4 22.8 26.2*** 24.2
Maternal education High school Some college 50 (50.5) 49 (49.5) 82.0***
95.9 18.04.1 61.057.5 39.042.6
Maternal relationship status Single/separated Married/partnership 70 (70.7) 29 (29.3) 87.1
93.1 12.96.9 52.5***74.1 47.525.9
Maternal smoking Yes
No 9 (9.2)89
(90.8)
77.8
89.9 22.210.1 42.960.0 57.140.0 Maternal overweight/obesity <25 25 36 (38.3) 58 (61.7) 91.7
Sample
Characteristic Total Sample (n=99)
Breastfeeding
Initiation Breastfeeding at Discharge
% (n) or mean±S D Yes 88.9% (n=88) No 11.1% (n=11) Yes 59.1% (n=52) No 40.9% (n=36) Maternal depressive symptoms <16 CES-D 16 CES-D
65 (66.3) 33 (33.7)
89.2
87.9 10.812.1 58.6***62.1 41.437.9
Maternal breastfeeding
intention scale score (0-16)
9.4±4.8 10.0* 4.3 10.8*** 8.9
Infant variables Infant birth weight,
grams 3306.2±463.4 3299.8 3358.1 3215.9** 3420.8 Infant gender
Female
Male 51.0 (50) 49.0 (48)
92.0
85.4 8.014.6 60.958.5 39.141.5
Infant jaundice in hospital Yes No 22 (22.5) 76 (77.6) 95.6
88.2 4.611.8 61.958.2 38.141.8
Delivery hospital UNC
Wake 20 (20.2)
79 (79.8)
100.0
86.1 0.013.9 75.054.4 25.045.6
Hospital variables Delivery mode
Vaginal
C-section 78 (80.4) 19 (19.6)
87.2
Sample
Characteristic Total Sample (n=99)
Breastfeeding
Initiation Breastfeeding at Discharge
% (n) or mean±S D Yes 88.9% (n=88) No 11.1% (n=11) Yes 59.1% (n=52) No 40.9% (n=36) Doula present at
birth Yes No 7 (7.1) 92 (92.9) 100.0
88.0 0.012.0 57.159.3 42.940.7 Pacifier in hospital
Yes
No 33 (33.3)
66 (66.7)
90.9
87.9 9.112.1 40.0*69.0 60.031.0
Gift pack with formula Yes No 8 (8.1) 91 (91.9) 87.5
89.0 12.511.0 57.159.3 42.940.7 Breastfed within 1
hour of birth Yes No 45 (51.1) 43 (48.9) -- --62.2
55.8 37.844.2
Roomed-in Yes
No 71 (81.6)
16 (18.4)
--
--63.4***
37.5 36.662.5
Help with breastfeeding Yes No 75 (85.2) 13 (14.8) -- --58.7
61.5 41.338.5
Help with breastfeeding from LC Yes No 59 (67.1) 29 (32.9) -- --59.3
58.6 40.741.4
Table 2. Results of logistic regression models testing the association between pacifier use in the hospital and breastfeeding status at
hospital discharge (n=88)
Likelihood of Breastfeeding at Hospital Discharge
Model 1 Model 2 Model 3
Odds Ratio
95% Confiden ce
Interval OddsRatio
95% Confiden ce
Interval OddsRatio
95% Confiden ce Interval Pacifier used during stay 0.30 ** 0.12-0.75 0.36 ** 0.13-0.98 0.38 0.13-1.07 Maternal age in years 1.07 0.96-1.19 1.06 0.95-1.18 Maternal relationship status, single 0.45 0.14-1.45 0.50 0.15-1.64 Maternal depressive symptoms, present1 1.06 0.39-2.91 1.01 0.36-2.83 Maternal breastfeeding intention scale score2 1.08 0.96-1.21 1.08 0.96-1.21 Infant birthweight in grams 1.00 1.00-1.00 1.00 1.00-1.00 Infant roomed in day and night
1.71
0.47-6.18
**p<.05
1Presence of depressive symptoms defined as a score of 16 or higher on the Center for Epidemiological Studies Depression Scale (CES-D)
2Infant Feeding Intention (IFI) scale score ranges from 0 (no intention to breastfeed) to 16 (very strong intentions to fully breastfeed for 6 months).
References
1. American Academy of Pediatrics, Work Group on Breastfeeding. Breastfeeding and the
use of human milk. Pediatrics 1997;100:1035–1039.
2. World Health Organization. Global Strategy for Infant and Young Child Feeding. Geneva,
Switzerland: World Health Organization; 2003.
3. Centers for Disease Control and Prevention. Breastfeeding Among U.S. Children Born
2001-2011. CDC National Immunization Survey. 2014.
4. Butler S, Williams M, Tukuitonga C, Paterson J. Factors associated with not breastfeeding
exclusively among mothers of a cohort of Pacific infants in New Zealand. N Z Med J
2004;117:U908.
5. Perez-Rios, Naydi, Gilberto Ramos-Valencia and Ana Patricia Ortiz. Cesarean Delivery as
a Barrier for Breastfeeding Initiation: The Puerto Rican Experience. Journal of Human Lactation 2008;24.3;293-302.
6. Hauck YL, Fenwick J, Dhaliwal SS, Butt J. A western Australian survey of breastfeeding
initiation, prevalence and early cessation patterns. Matern Child Health J 2011;15:260–8.
7. Patel RR, Liebling RE, Murphy DJ. Effect of operative delivery in the second stage of
labor on breastfeeding success. Birth 2003;30:255–60.
8. Baumgarder DJ, Muehl P, Fischer M, Pribbenow B. Effect of labor epidural anesthesia on
breast-feeding of healthy full-term newborns delivered vaginally. J Am Board Fam Pract. 2003;16:7-13.
9. Ransjo-Arvidson AB, Matthiesen AS, Lilja G, Nissen E, Widstrom AM, Uvnas-Moberg K.
Maternal analgesia during labor disturbs new- born behavior: effects on breastfeeding, temperature, and crying. Birth. 2001;28:5-12.
10. Chang, Z. M. Epidural Analgesia During Labor and Delivery: Effects on the Initiation
and Continuation of Effective Breastfeeding. Journal of Human Lactation 2005;21.3;305-14.
11. Halpern SH, Levine T, Wilson DB, MacDonell J, Katsiris SE, Leighton BL. Effect of
labor analgesia on breastfeeding success. Birth. 1999;26:83-88. 12. DiGirolamo AM, Grummer-Strawn LM, Fein SB. Effect of
Maternity-Care Practices on
Breastfeeding. Pediatrics 2008;122.2;543-49.
13. Rosenberg KD, Stull JD, Adler MR, Kasehagen LJ, Crivelli-Kovach A. Impact of
Hospital Policies on Breastfeeding Outcomes. Breastfeeding Medicine 2008;3.2;110-16.
In-Hospital Formula Supplementation for Healthy Breastfeeding Newborns. Journal of
Human Lactation 2013;29.4;527-536.
15. Centers for Disease Control and Prevention. United States 2014 Breastfeeding Report Card.
July 2014.
16. U.S. Department of Health and Human Services. Maternal, Infant, and Child Health.
Healthy People 2020.