Lara Balian
Adrienne Binder
Catherine Chao
Shannon Clancy
Sarah Mye
Asia-La’Rae Walker
In partnership with Cervical Cancer-Free North Carolina
Alexis Moore, MPH
Preceptor
Noel Brewer, PhD
Faculty Advisor
On our honor, we have neither given nor received any unauthorized aid on this assignment.
Improving North Carolina’s Capacity to Prevent
Cervical Cancer through Community Engagement,
a Needs Assessment, and Resource Strengthening
II. ABSTRACT
Background: In 2013, Cervical Cancer-Free North Carolina (CCFNC) identified the South Central and Northeast regions of North Carolina (NC) as disproportionately affected by cervical cancer based on epidemiological surveillance data. Women diagnosed with cervical cancer in NC are often minorities, older, recent immigrants, and/or of lower income. Cervical cancer cases also tend to occur in women who have below average screening rates and HPV vaccination uptake. To address this disparity, CCFNC works with a coalition of partners that deliver and promote cervical cancer prevention services. In 2012, CCFNC
developed nine evidenced-based recommendations that could improve cervical cancer prevention.As the CCFNC Capstone team, we worked with stakeholders, who provide cervical cancer prevention services, to identify barriers and encourage the adoption of one of the recommended strategies to increase screening rates and HPV vaccination in high-need regions of NC.
Methods: We attended the North Carolina Cervical Cancer Coalition Summit (State Summit) to gather information about the prevailing cervical cancer challenges and stakeholder attitudes towards strategies for improving prevention. We summarized and shared highlights from the event with attendees and coalition members. We then identified and recruited key informants (n=32) from the South Central and Northeast regions of NC using the list of coalition partners and participant referrals. We conducted semi-structured key informant interviews (KIIs) with healthcare providers and educators involved in women’s health and
immunization to identify challenges and opportunities to improve cervical cancer prevention services in their respective regions. Qualitative data informed the content of the Cervical Cancer Prevention: Strengthening Health Systems and Programs in South Central North Carolina regional meeting. Key informants, coalition members, and other cervical cancer prevention stakeholders attended the regional meeting and participated in community action planning to outline strategies and action steps to implement prioritized recommendations. Following the meeting, our team summarized participant strategies and action steps in the community action plan report, which we distributed to attendees of the meetings. We also updated the NC Cervical Cancer Resource Directory and established a process that can be replicated in the future using our phone survey and web form. Lastly, our team developed an online survey in Qualtrics and analyzed responses to determine
recommendations for making the Resource Directory more useful to practitioners and promotional strategies to increase use of the Resource Directory.
Results: Participants at the State Summit prioritized two evidence-based recommendations to improve cervical cancer prevention. KIIs identified challenges and opportunities to providing cervical cancer
prevention services. They also informed the format and focus of the regional meeting and contributed to its success. At the regional meeting, participants outlined specific strategies and action steps to implement evidence-based recommendations deemed feasible for their organizations. Additionally, our Capstone team identified several barriers that limit use of the Resource Directory, including inaccurate entries, poor Spanish translation, and text with an advanced reading level. Based on these findings and results from the NC Cervical Cancer Resource Directory Survey, the team updated the directory, established a process for revising the directory in the future, and developed specific recommendations for improving utility and awareness of the tool among healthcare professionals.
III. ACKNOWLEDGEMENTS
Our Capstone team graciously recognizes Alexis Moore, MPH, our wonderful preceptor who
selflessly stepped in to help guide us through our Capstone journey and consistently encouraged us to strive
for excellence. We thank our faculty advisor and Director of Cervical Cancer-Free North Carolina (CCFNC),
Noel Brewer, PhD, for his vision and guidance, as well as the passion he brings to addressing cervical cancer.
We also acknowledge Megan Hall, MPH, for providing insightful feedback, and the entire CCFNC staff for
supporting our Capstone efforts. We thank Kristina Felder, Research Assistant at CCFNC, for her valuable
contribution to our projects. Special thanks goes out to the Capstone Teaching Team, Meg Landfried, MPH,
Christine Brune, MPH, and Melissa Cox, MPH, for teaching us lifelong professional skills and for being a
consistent source of support, guidance, and feedback.
We extend a huge thank you to Suzanne Lea, PhD, Alice Richman, PhD, John Compagna, MD, and
Dianah Bradshaw, PhD, for their instrumental roles in the Cervical Cancer Prevention: Strengthening Health Systems
and Programs in South Central North Carolina regional meeting. We sincerely acknowledge all the clinicians, educators, stakeholders, community partners, and leaders across NC working to reduce the burden of cervical
cancer and eliminate the dramatic disparities that exist. We extend special warmth of gratitude to all South
Central and Northeast key informants for graciously sharing their time, insights, and wisdom in helping us
fulfill the goals of our Capstone project. We also thank Schatzi McCarthy, MAPA, for encouraging us to get
involved with cervical cancer initiatives and attracting us to this Capstone project.
All of your help made our Capstone project a fulfilling part of our lives. From the bottom of our
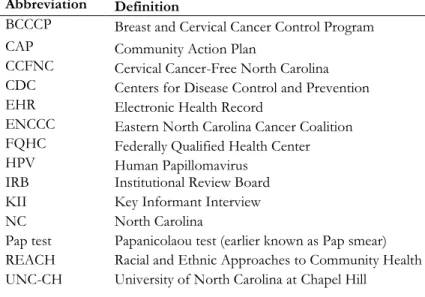
IV. ACRONYMS & PUBLIC HEALTH TERMS
Table 1: Acronyms and Public Health Terms
Abbreviation Definition
BCCCP Breast and Cervical Cancer Control Program
CAP Community Action Plan
CCFNC Cervical Cancer-Free North Carolina
CDC Centers for Disease Control and Prevention
EHR Electronic Health Record
ENCCC Eastern North Carolina Cancer Coalition
FQHC Federally Qualified Health Center
HPV Human Papillomavirus
IRB Institutional Review Board
KII Key Informant Interview
NC North Carolina
Pap test Papanicolaou test (earlier known as Pap smear)
REACH Racial and Ethnic Approaches to Community Health
Table of Contents
II. ABSTRACT ... II III. ACKNOWLEDGEMENTS ... III IV. ACRONYMS & PUBLIC HEALTH TERMS ... I
VI. INTRODUCTION ... 2
THE CAPSTONE EXPERIENCE ... 2
CERVICAL CANCER-FREE NORTH CAROLINA ... 2
PROJECT OBJECTIVES AND DELIVERABLES ... 3
WE CATEGORIZED DELIVERABLES ONE THROUGH FOUR AS STAKEHOLDER ENGAGEMENT DESIGNED TO ACHIEVE THE FIRST OUTCOME OUTLINED ABOVE.DELIVERABLES FIVE AND SIX RELATE TO NC CERVICAL CANCER RESOURCE DIRECTORY UPDATES,IMPROVEMENTS, AND PROMOTION, WHICH TARGETED THE SECOND OUTCOME OF OUR PROJECT. ... 4
VII. BACKGROUND ... 4
EPIDEMIOLOGICAL ASSESSMENT ... 4
APPROACHES TO STAKEHOLDER ENGAGEMENT ... 5
KEY INFORMANT INTERVIEWS (KIIS) ... 6
CONVENING REGIONAL STAKEHOLDERS ... 7
COMMUNITY ACTION PLANS ... 8
OUR APPROACH ... 9
VIII. METHODS ... 9
ORGANIZATION ORIENTATION ... 9
STAKEHOLDER ENGAGEMENT –PHASE 1 ... 10
STAKEHOLDER ENGAGEMENT –PHASE II ... 11
NCCERVICAL CANCER RESOURCE DIRECTORY UPDATES,IMPROVEMENTS, AND PROMOTION ... 12
IX. RESULTS ... 13
ENGAGING WITH STAKEHOLDERS TO ENCOURAGE PARTICIPATION AND BUILD SUPPORT ... 13
PRIORITIZING AND ADOPTING EVIDENCED-BASED STRATEGIES TO IMPROVE CERVICAL CANCER PREVENTION ... 14
IMPROVING AND PROMOTING THE RESOURCE DIRECTORY TO INCREASE USE ... 14
X. DISCUSSION ... 15
IMPLICATIONS FOR CCFNC ... 15
IMPLICATIONS FOR CERVICAL CANCER PREVENTION ... 15
PROJECT LIMITATIONS ... 16
RECOMMENDED NEXT STEPS ... 16
CONSIDERATIONS FOR SUSTAINABILITY ... 17
PROFESSIONAL IMPACT ... 17
XI. CONCLUSION ... 18
XII. REFERENCES ... 19 XIII. APPENDIX A: LOGIC MODEL ... I XIV. APPENDIX B: CCFNC CAPSTONE DELIVERABLES ... II XV. APPENDIX C: KII PARTICIPANTS ... VII XVI. APPENDIX D: REGIONAL MEETING ATTENDANCE AND PARTICIPANT
VI. INTRODUCTION
The Capstone ExperienceThe purpose of this summary report is to provide an overview of our Capstone project with Cervical
Cancer-Free North Carolina (CCFNC). Capstone is a fieldwork requirement of the Master of Public Health
(MPH) program in the Department of Health Behavior at the Gillings School for Global Public Health at the
University of North Carolina at Chapel Hill (UNC-CH). Capstone provides second-year MPH students the
opportunity to partner with a community organization to gain practical fieldwork experience in public health
through the completion of projects requested by the partner organization. The report begins with an
explanation of the benefits of stakeholder engagement, specifically qualitative research and community action
planning for improving cervical cancer prevention efforts. The report then discusses the methods used to
produce Capstone deliverables for CCFNC, followed by a results section that highlights key findings from the
project. The discussion section notes project implications for CCFNC and stakeholders, including project
limitations, recommendations, and considerations for sustainability of the overall project.
Cervical Cancer-Free North Carolina
CCFNC is a statewide coalition of government and community partners working together to
decrease cervical cancer incidence rates in the state (McCarthy, 2013). CCFNC’s office is in the Gillings
School of Global Public Health at UNC-CH. The organization conducts projects to improve cervical cancer
prevention through health systems and behavior changes. Since many health agencies in North Carolina (NC)
have roles in cervical cancer prevention, CCFNC encourages strategies that promote collaboration across
organizations to improve Papanicolau (Pap) testing and Human Papillomavirus vaccination (HPV) rates.
In 2013, CCFNC released a report, Cervical Cancer Prevention in North Carolina: Strengthening Health
Programs and Systems, that identified 30 counties in the state that have a high-need for cervical cancer
prevention (Figure 1) (McCarthy, 2013). High-need was determined by cervical cancer incidence and
mortality, screening rates among low-income women, and HPV vaccination rates. The report also outlined
evidence-based recommendations and strategies for healthcare providers to improve cervical cancer
Figure 1: NC Counties with High Cervical Cancer Prevention Need (McCarthy, 2013)
In 2013, CCFNC requested a Capstone team to conduct qualitative research in some of the
high-need counties to better understand the challenges and opportunities that practitioners face in providing
cervical cancer prevention services. We, the CCFNC Capstone team, planned and conducted a regional
meeting in Fayetteville, NC based on information from the interviews. Meeting activities built upon
evidenced-based recommendations (hereinafter referred to as CCFNC’s recommendations) outlined in the
report by encouraging regional stakeholders to identify action steps that were feasible to tailor and implement
in their organizations to improve cervical cancer outcomes. In tandem with these efforts, our team updated
CCFNC’s online North Carolina Cervical Cancer Resource Directory, which contains information on
affordable cervical cancer screening locations throughout the state, and recommended strategies for
improving and promoting the Resource Directory.
Project Objectives and Deliverables
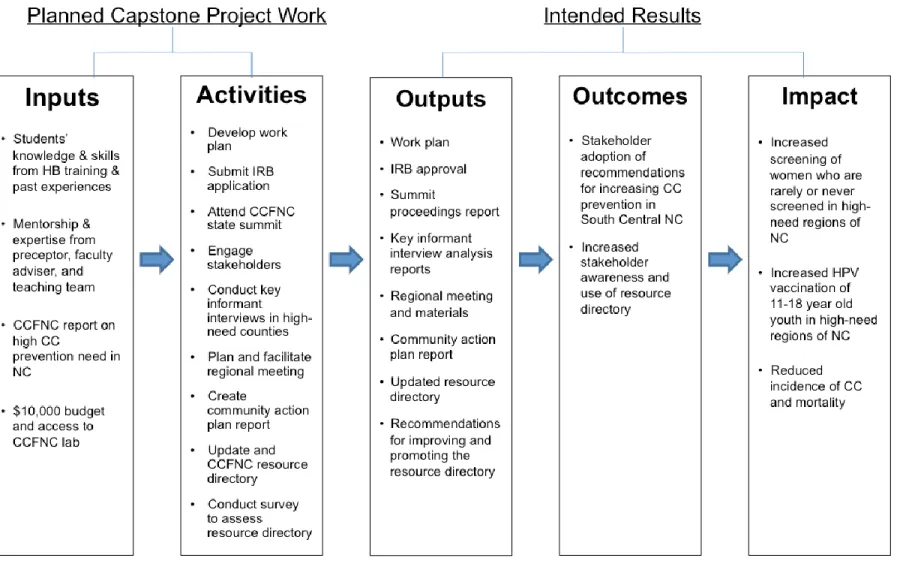
Our Capstone team identified two intended outcomes for the project: 1) stakeholder adoption of
recommendations for increasing cervical cancer prevention, and 2) increased stakeholder awareness and use
of the Resource Directory (see Appendix A). The long-term impact of our Capstone project is increased
cervical cancer screening of women who are rarely or never screening and increased HPV vaccination rates in
high-need counties in NC, both of which will contribute to a decreased incidence of cervical cancer and
1. State summit proceedings report: Summary of NC Cervical Cancer Coalition Summit
2. Key informant interviews (KIIs) with community stakeholders in NC counties with high-need for cervical cancer prevention and analysis report
3. Regional meeting in South Central NC
4. Community Action Plan (CAP) report for South Central region 5. Updated online NC Cervical Cancer Resource Directory
6.
NC Cervical Cancer Resource Directory Survey and Promotional Recommendations Report We categorized deliverables one through four as stakeholder engagement designed to achieve the firstoutcome outlined above. Deliverables five and six relate to NC Cervical Cancer Resource Directory Updates,
Improvements, and Promotion, which targeted the second outcome of our project.
VII. BACKGROUND
Cervical cancer is the second most common cancer among women worldwide (Documet et al.,
2008). However, unlike other forms of cancer, the physical, emotional, and economic impact of cervical
cancer is mostly preventable with routine Pap tests and uptake of the complete human papillomavirus (HPV)
vaccination series (Denslow, Knop, Klaus, Brewer, Rao, & Smith, 2012). In order to reduce the incidence and
mortality of cervical cancer in North Carolina, CCFNC works with stakeholder groups that are crucial to the
delivery and promotion of cervical cancer prevention and screening measures. These stakeholders include
administrators, decision-makers, and healthcare providers at county health departments, hospitals, private
practices, and community clinics. Additionally, health educators, school nurses, and organizations that engage
in cervical cancer prevention advocacy are important stakeholders to CCFNC. Collectively, these stakeholders
provide Pap tests, administer the HPV vaccine, and educate individuals about the importance of these
prevention practices.
To assist with CCFNC’s work, our team has been charged with engaging these stakeholders to
identify barriers and opportunities to improving the provision of cervical cancer prevention and screening
services in high-need regions of NC. The following section summarizes the current literature discussing the
use of stakeholder engagement to reduce the incidence and mortality rates of cervical cancer.
Epidemiological Assessment
HPV, the most common sexually transmitted infection, causes nearly all cases of cervical cancer and
if left untreated can be fatal (Garner, 2003; CDC, 2014). In the United States, cervical cancer causes more
and 2007, there were 3,652 new cases of cervical cancer, or 8.2 cases per 100,000 women, and 1,208
associated deaths, or 2.6 cases per 100,000 women (Denslow et al., 2012). Cervical cancer affects adult
women at almost any age; in NC, the average age of diagnosis is 49 years old, with age at diagnosis ranging
from 19 to 98. Forty-five percent of cases occurred in 30-49 year olds, while more than half of mortality cases
occurred in women over the age of 50, as the risk of death increases with age (Denslow et al., 2012).
Minority, lower income, older, and recent immigrant women in NC have below average rates for
screening and HPV vaccine uptake, resulting in disproportionately higher cervical cancer incidences
(Documet et al., 2008). According to Denslow et al. (2012), Hispanic and Black women have higher incidence
rates (18.3 cases per 100,000 women and 10.6 cases per 100,000 women, respectively) than White women (7.3
cases per 100,000 women). Black women also have the highest mortality rate at 4.5 deaths per 100,000
women, which is greater than both the rates of non-Hispanic White and Hispanic women combined.
Minority status is associated with factors such as the lack of economic security and insurance coverage, which
in turn can result in lower utilization of cervical cancer prevention and screening services (Denslow et al.,
2012).
In addition to race, Denslow et al. (2012) found that cervical cancer burden varies by county in NC,
such that counties with lower economic prosperity have higher incidence and mortality rates than higher
income counties. This finding aligns with previous research demonstrating the association between poverty
and adverse health behaviors, in that the lower the income, the lower the rate of cancer screening (NC Center
for Health Statistics, 2008). The high-need counties are primarily located in the South Central and Northeast
regions of NC, as well as in the Western part of the state (Denslow et al., 2012). Engaging stakeholders in
counties with high cervical cancer prevention need to adopt evidence-based recommendations can improve
prevention efforts and reduce cervical cancer cases.
Approaches to Stakeholder Engagement
Involving stakeholders in cervical cancer prevention efforts is beneficial in multiple ways, due in part
to their knowledge of community culture, and may result in the improved sustainability of programs by
specific barriers to care that underserved populations face. Their support and buy-in is crucial to the
implementation of evidenced-based recommendations proposed by outside organizations. According to the
National Cancer Institute, stakeholder collaboration can help improve the continuity of care of cervical
cancer services, decrease health system fragmentation, and facilitate a more efficient use of resources (Texas
Department of State Health Services, 2006). There is also a strong theoretical basis for facilitating
collaboration among organizations. One example is the Interorganizational Relations (IOR) Theory, which
presumes that “collaboration among community organizations leads to a more comprehensive, coordinated
approach to a complex issue than can be achieved by one organization” (Butterfoss, Kegler, & Francisco,
2008, p. 346). Collaboration with stakeholders can be accomplished through the processes of conducting
KIIs, hosting regional meetings, and developing CAPs. The decision to engage stakeholders through KIIs
and the development of CAPs is based on recommendations from the Diffusion of Innovations Theory
(Rogers, 2003). Given that the overall goal of our project is to promote the adoption of evidenced-based
strategies for increasing cervical cancer screening and HPV vaccination, the diffusion of innovations theory
offers a useful framework for understanding how organizations adopt new practices. The theory proposes
that organizations will adopt innovations at different stages and that properties of the innovation such as
relative advantage, compatibility, trialability, observability, and complexity influence this rate. Stakeholder
engagement helped our team assess the compatibility of cervical cancer prevention strategies with these
organizations and highlight their relative advantage.
Key Informant Interviews (KIIs)
KIIs are an important component for building stakeholder engagement in multiple regions, both
domestically and internationally, and are essential in reaching target populations (Allen et al., 2010). KIIs also
provide insight into stakeholders’, community members’, and clinicians’ perspectives of how community
structures impact the uptake of cervical cancer screenings and HPV vaccinations in underserved women and
hard to reach populations. In the literature, KIIs are used to involve stakeholders, increase buy-in, and gather
information needed to make decisions and recommendations about cervical cancer prevention services that
Katz et al. (2007) and Documet et al. (2008) conducted interviews regarding Pap tests in 17 Ohio
Appalachia counties and eight Western Pennsylvania counties. The populations in these counties are
demographically similar to NC’s underserved female population. To examine the social, economic, and
healthcare environments that affect cervical cancer screening, researchers in both studies conducted KIIs
with residents, providers, and stakeholders using semi-structured interview guides. Study results revealed that
most of the women had limited knowledge of cervical cancer, limited access to healthcare services, and did
not receive recommended Pap test (Katz et al., 2007; Documet et al., 2008). These studies were effective in
increasing community engagement through KIIs, which helped inform strategies to increase recruiting and
retention methods for cervical cancer screening among target populations.
Although there is limited domestic research about the implementation and evaluation of HPV
vaccine programs, international data indicates that KIIs are effective in engaging the community and
stakeholders in creating HPV vaccination programs and policies. Leask et al. (2009) conducted 24
semi-structured KIIs with program managers and primary care providers to evaluate the early implementation of
Australia’s national HPV vaccination programs for females, ages 12-26 years old. A study in Uganda by
Katahoire et al. (2008) provided another example of how KIIs were successfully used for community
engagement surrounding HPV vaccine uptake. This study’s ultimate objective was to generate evidence for
governmental decision-making and operational planning for the introduction of HPV vaccine in the country.
Similar to the cervical cancer screening studies discussed previously, the information obtained from KIIs
revealed that HPV vaccination perspectives were effective in developing large stakeholder colloquiums and
building community engagement across regions regarding cervical cancer, which in turn can facilitate
collaborative efforts to implement evidence-based strategies to increase cervical cancer prevention services
(Katahoire et al., 2008; Leask et al., 2009).
Convening Regional Stakeholders
In addition to gaining insight on stakeholder perspectives through KIIs, an emerging method for
promoting engagement is the convening of regional stakeholders through meetings and symposiums. Sherris
Asia that drew representatives from 20 nations. The conference conveyed the importance of cervical cancer
as a public health issue and improved cooperation among gynecological oncologists in the region (Sherris et
al., 2005). Furthermore, in 2011 the World Health Organization (WHO) hosted a regional meeting on cervical
cancer prevention in Europe; deliverables of the meeting included an overview of lessons learned on HPV
vaccination from countries that were early adopters and outlined future priorities for prevention (WHO
Regional Office for Europe, 2011). Domestically, the Texas Department of State Health Services and the
Texas Cancer Council worked with various stakeholders, including nurses, health educators, and researchers,
to develop the Texas Cervical Cancer Strategic Plan (Texas Department of State Health Services, 2006).
Several meetings, both in-person and via teleconference, facilitated this effort. Additionally, one of the
specific objectives listed in the Texas Cervical Cancer Strategic Plan was to increase the number of regional
and local cancer networks, to be achieved in part through engaging stakeholders to develop regional/local
coalitions. While the previous examples do not include measurable outcomes, we believe that convening
regional stakeholders can contribute to a growing commitment to improving cervical cancer prevention in
their area through the promotion of inter-organizational collaboration.
Community Action Plans
Similar to the Texas Cervical Cancer Strategic Plan, the development of a CAP is a localized
approach for identifying objectives and results from stakeholder engagement. Creating a relevant CAP is
facilitated by the stakeholder knowledge and inter-organizational collaboration gained from KIIs and regional
meetings, respectively. Several programs designed to address cervical cancer have employed this strategy. For
example, the Centers for Disease Control and Prevention’s (CDC) Racial and Ethnic Approaches to
Community Health (REACH) initiative includes a goal of reducing breast and cervical cancer disparities
(Fouad et al., 2004). The Alabama REACH 2010 Project, designed to reduce disparities between African
American and White women, involved three sequential stages: coalition building, community needs
assessment, and the development of a CAP. The coalition used information from the community needs
assessment to inform the development of individual, community systems, and change agent level objectives
utilized similar methods to inform the development of its own CAP (Bigby, Ko, Johnson, David, & Ferrer,
2003).
A final example of community action planning is from 2000-2004 in Santa Clara County, California
among Vietnamese American women (Nguyen et al., 2006). Based on input from coalition members,
including the Vietnamese Physician Association of Northern California and the Santa Clara County Public
Health Department, the Vietnamese REACH for Health Initiative Coalition developed a six-component CAP
to increase Pap testing. Using Harris County, Texas as a comparison group, the quasi-experimental, pre-post
evaluation design revealed that although Pap test rates were comparable between the counties initially, Santa
Clara County experienced a significant increase in rates after the CAP activities were implemented (77.5% to
84.2%, p<0.001). This increase was not seen in the comparison group (73.9% to 70.6%, p=NS) (Nguyen et
al., 2006).
Our Approach
Based on the aforementioned evidence, our team used KIIs, regional meetings, and CAPs as ways to
engage and collaborate with stakeholders. The literature suggests that these methods are effective at
addressing and reducing cervical cancer disparities in vulnerable female populations similar to those in NC.
These methods align with CCFNC’s mission to improve cervical cancer screening rates and HPV vaccination
coverage in high-need counties of NC.
VIII. METHODS
Organization OrientationIn order to complete six deliverables for CCFNC, our team relied on several methodologies and
skills. First, our team held several meetings with mentors to become better oriented to CCFNC and its
mission, as well as to prepare for the State Summit that occurred in September 2013. During these meetings,
mentors provided a context for Capstone deliverables and detailed information on CCFNC’s purpose and
stakeholders. In addition, Dr. Jennifer Smith, an epidemiological expert in HPV and cervical cancer, provided
a presentation regarding cervical cancer pathology and HPV vaccine to our team to further our understanding
of this issue. Finally, we read the CCFNC report, Cervical Cancer Prevention in North Carolina: Strengthening Health
regions in the state and recommended evidence-based actions for strengthening health programs, both of
which helped to inform our team’s work. Stakeholder engagement also informed our team’s work: in phase 1
we engaged with stakeholders to better understand their perspectives, while in phase 2 we focused on guiding
stakeholders through an action-planning framework.
Stakeholder Engagement – Phase 1
Following this orientation to CCFNC, our team prepared for the State Summit and created a note
taker form to summarize discussions at the meeting and a key informant interview guide to test at the
meeting. The note taker form helped organize field notes and allowed us to identify major themes discussed
by participants. We documented these findings in the Summary of NC Cervical Cancer Coalition Summit, which
highlighted recommendations prioritized by participants at the meeting and discussions surrounding the
recommendations. CCFNC disseminated the document through direct email to summit attendees, coalition
partners, an announcement in the monthly newsletter, and a posting to the CCFNC website.
After completing the pilot test and subsequent modifications to the KII guide, our team submitted
an application to the Institutional Review Board (IRB) and was approved to conduct KIIs. We identified and
recruited key informants (n=32) from the South Central and Northeast regions of the state by contacting
CCFNC stakeholders in high-need regions and asking informants for referrals. Our team contacted members
of the NC Cervical Cancer Coalition and other community members referred to us by interview participants,
via email and phone, to request participation in a 30-minute phone interview. Between October 2013 and
January 2014, our team conducted a total of 25 interviews with 32 individuals in South Central and Northeast
NC (see Appendix B and C). All interviews were conducted over the phone in pairs, with one Capstone
member leading the interview while the second took field notes. After completing all interviews in both
regions, we summarized interview notes and developed topical and sub-topical codes to categorize themes.
We analyzed the qualitative data using Atlas.ti software, first coding one interview together to ensure that we
agreed on what content applied to each code. We drafted two internal analysis reports (one per region) to
document major themes, challenges, and solutions identified from these interviews. The reports informed
Stakeholder Engagement – Phase II
Event planning for the regional meeting also overlapped with the KIIs. First, our team and mentors
selected Fayetteville, in the South Central region of NC, and Rocky Mount, in the Northeast region, as
meeting locations because of their centrality, concentrated populations, and availability of venues. After
choosing these locations, team members identified, contacted, and visited potential venue locations. During
this time, mentors and team members became concerned with the feasibility of implementing two regional
meetings because of time constraints. After a discussion with the mentors, the meeting in South Central was
prioritized because of the area’s larger population, and it was decided that the meeting in the Northeast region
would be postponed. Once the meeting venue and date were finalized, our team developed an email
invitation and distribution list using the North Carolina Institute for Public Health (NCIPH) to handle the
online registration for the event.
Occurring simultaneously with event planning, content planning for the event involved several
meetings with mentors to develop the meeting agenda, to recruit and coordinate moderators and speakers,
and to create materials that facilitate the breakout session activities. These activities were informed by
CCFNC’s recommendations on how to prevent cervical cancer in NC and by information gathered from the
KIIs (McCarthy, 2013). Our team researched models for developing community action plans (CAPs) and
adapted the materials to facilitate community action planning activities for the breakout sessions from the
Community Tool Box from the University of Kansas (Community Tool Box, 2013). Specifically, we created
seven handouts for the meeting: an agenda, two recommendations handouts for the breakout sessions, a CAP
worksheet, an educational resources handout, a speaker bio sheet, and an evaluation form. Our team also
developed two presentations for the regional meeting. One presentation provided background information
on cervical cancer data specific to the South Central region, including relevant findings from the KIIs, while
the other shared the prioritized recommendations from the State Summit so that attendees would be familiar
with the recommendations prior to the breakout session. Finally, a map of the South Central region was
created to illustrate hospitals, cancer centers, Breast and Cervical Cancer Control Program (BCCCP) counties,
During the regional meeting, a total of 41 participants from 19 organizations shared innovative ideas
through small and large group discussions, which facilitated the development of action plans. The meeting’s
breakout sessions, which focused on cervical cancer screening and HPV vaccination, provided attendees the
opportunity to think through the action steps necessary for strategy implementation (e.g. who needs to be
involved, approval process, timeframe). One moderator per breakout session facilitated the group discussion,
highlighting various strategies for achieving the selected CCFNC recommendations (McCarthy, 2013).
Participants recorded their strategies, action steps, and notes from the discussion on the handouts developed
by our team, most of which were then collected by us to inform the CAP Report.
The strategies and actions steps documented in the breakout session handouts were compiled into
the CAP Report, which served as a collaborative plan to help reduce cervical cancer in South Central NC. We
then drafted and finalized the report based on these worksheets, discussions that occurred at the regional
meeting, and feedback from the mentor and teaching team. CCFNC emailed the CAP Report to regional
meeting attendees to enable them to see the strategies that other stakeholders in their region identified as
feasible.
NC Cervical Cancer Resource Directory Updates, Improvements, and Promotion
Concurrent to stakeholder engagement, our team also updated the NC Cervical Cancer Resource
Directory. In collaboration with mentors, we determined what additional information would be helpful for
providers and women using the Resource Directory. Additional items included what languages the clinic
offered translation services for and whether clinic exam tables could accommodate women who were
overweight/obese, as such services may facilitate the screening of women rarely or never screened. Our team
then developed a phone survey and began calling each clinic listed in the directory. Additional information
was collected for approximately 30 clinics. We created a spreadsheet to document the information gained
from each conversation. Before each call, any information that was obtained from the clinic websites was
recorded in the spreadsheet and verified by phone. Our team also converted the phone survey into a
Qualtrics survey for clinics that preferred to answer the questions electronically. We completed edits to the
While conducting KIIs and updating the Resource Directory, our team conducted formative research
for the Promotional Recommendations Report by developing an online survey in Qualtrics. First, our team
determined two objectives for the questionnaire: 1) to develop recommendations for making the Resource
Directory more useful to practitioners, and 2) to determine promotional strategies that could be used to
increase use of the Resource Directory. After our team and mentors provided feedback on multiple iterations
of the questionnaire, we emailed the survey to healthcare professionals (n=357) throughout NC with an
incentive to enter a drawing to win a $25 Amazon gift card.
For the Promotional Recommendations Report, we reviewed and analyzed the results of the
Qualtrics survey to develop strategies to increase awareness and use of the Resource Directory, based on
survey respondents’ suggestions. A total of 59 participants from 43 counties in NC, representing health
departments, primary care clinics, hospitals, insurance companies, academia, non-profit, and local and state
government agencies completed the Resource Directory survey. Using these data, we developed eight
promotional recommendations for CCFNC, some of which included email campaigns, social media messages,
Resource Directory promotion through links on partner organizations’ websites, and search engine
optimization. This report was finalized after feedback from the mentors and submitted to CCFNC for
internal use.
IX. RESULTS
The overall goals of this project were to: 1) promote and encourage the adoption of CCFNC’s
evidenced-based recommendations for increasing cervical cancer screening and HPV vaccine uptake rates and
2) to increase awareness and use of the NC Cervical Cancer Resource Directory. These outcomes will
decrease the incidence and mortality rates of cervical cancer in NC by increasing the number of people who
are screened and vaccinated. In the following section, we describe key findings across our project deliverables.
Engaging with Stakeholders to Encourage Participation and Build Support
Consistent and regular stakeholder engagement throughout the course of the project was essential to
foster stakeholder buy-in and inform project deliverables. Stakeholder engagement through KIIs and written
challenges to providing cervical cancer prevention services included physician reluctance to recommend the
vaccine and health organizations’ limited capacity (e.g. funding, time, staff, equipment). Despite these
challenges, participants noted opportunities to improve cervical cancer prevention that included:a)
strengthening partnerships, b) using technology such as electronic medical records, c) providing additional
training and resources for staff, and d) increasing awareness of cervical cancer prevention services through
local media promotion and health education. These findings informed subsequent deliverables (regional
meeting and CAP Report).
Prioritizing and Adopting Evidenced-Based Strategies to Improve Cervical Cancer Prevention
At the statewide cervical cancer summit, participants prioritized two of CCFNC’s recommendations
to improve cervical cancer prevention: 1) encourage providers to recommend HPV vaccine and 2) improve
recruitment of women who are rarely or never screened. Months later at the regional meeting, participants
outlined specific strategies and action steps to implement these recommendations. For example, some
attendees of the meeting identified the strategy of using Electronic Health Records (EHRs) to: 1) remind
physicians to discuss HPV vaccination with patients or their parents or 2) identify rarely or never screened
women with the action step of programming alerts. Activities at the regional meeting provided stakeholders
with a framework for creating sustainable change within their organization. Assessing the actual
implementation of these strategies is beyond the scope of this project. Overwhelmingly, participants were
very satisfied with the regional meeting and agreed that the event succeeded in meeting the outlined
objectives (see Appendix D).
Improving and Promoting the Resource Directory to Increase Use
Our team identified a number of challenges that limit the use of the Resource Directory, namely
inaccurate listings, poor Spanish translation, and complicated language. Addressing these issues and revising
the layout has the potential to increase the usefulness of the tool. Recommendations for promoting the tool,
based on user suggestions and CCFNC resource considerations, include circulating information about the
directory through partner health and non-health organizations’ newsletters and listervs, using search engine
have the potential to increase awareness and use of the Resource Directory among healthcare professionals
and women seeking free or low-cost screening services.
X. DISCUSSION
Implications for CCFNCOur Capstone project built upon CCFNC’s recommendations to improve cervical cancer prevention
by facilitating efforts to implement these recommendations. More specifically, our team assisted in the
planning and execution of a regional meeting that can be replicated in other regions of the state. CCFNC can
use the format, worksheets, and activities developed by our team to plan future CAP meetings in other
high-need regions of the state, such as the Northeast and the West. Similarly, our interview guide and KII analysis
reports provide a framework for CCFNC to conduct similar research in other areas of the state. Procedures
and materials for updating the Resource Directory can be used periodically to verify the accuracy of records
in the directory going forward. Furthermore, the Resource Directory survey results and the Promotional
Recommendations Report identify areas for CCFNC to increase the functionality of the Resource Directory
and expand awareness and use of the Resource Directory through different promotional strategies.
Implications for Cervical Cancer Prevention
Our Capstone project contributed to a deeper understanding of the resources, challenges, and
opportunities to providing cervical cancer prevention services in the South Central and Northeast regions of
North Carolina. While the results of our Capstone project are not generalizable, our methods of stakeholder
engagement can be used in other regions to facilitate system-level changes. The regional meeting and CAP
Report encouraged local organizations working in cervical cancer to strategically implement the CCFNC
recommendations that align with their organizations’ goals and objectives by identifying feasible action steps
given their existing resources. If organizations implement intended action steps with fidelity, we expect that
screening and HPV vaccination rates will increase. The regional meeting was also an opportunity for
attendees to meet new colleagues involved in cervical cancer prevention work and identify potential
partnerships with other organizations serving the same community. In addition, our recommendations to
Project Limitations
Our KIIs were crucial in planning the regional meeting to develop a CAP that is relevant to the
interests and needs regarding cervical cancer prevention in South Central NC. Continued stakeholder
engagement through additional interviews, in-person meetings, and county visits would have improved our
Capstone project. Supplementary interviews with key stakeholders and greater representation from different
types of healthcare professionals (e.g. health directors) would have enhanced our understanding of the
structural barriers to cervical cancer prevention. In our interviews, three of the eight high-need counties in the
South Central region and five of the 12 counties in the Northeast region were not represented in our
research. Broader representation from high-need counties would have contributed to an even deeper
understanding of local organizations’ resources, challenges, capacity, and opportunities to providing cervical
cancer prevention services. The breadth of our Capstone project meant we did not have enough time to build
relationships with key stakeholders or community leaders prior to the regional meeting. We also did not have
time to follow-up with South Central stakeholders with a second meeting or conference call, which could
have allowed for greater collaboration between organizations and enhanced the potential for sustainable
action by continuing the momentum generated at the regional meeting.
Recommended Next Steps
Our team recommends that CCFNC support the Eastern North Carolina Cancer Coalition
(ENCCC) in hosting a regional meeting in the Northeast region that focuses on community action planning
to implement CCFNC’s recommendations to improve cervical cancer prevention. CCFNC can use meeting
materials developed by our team to create a CAP toolkit that can be disseminated to organizations or
coalitions interested in developing CAPs for this purpose. We also suggest that CCFNC regularly update the
Resource Directory and implement our recommendations to improve the Resource Directory website. After
these improvement recommendations are implemented, we suggest that CCFNC or partner organizations
implement feasible strategies to promote the directory, as listed in our Promotional Recommendations
Report. We recommend that CCFNC also evaluate the reach of the promotional strategies that it implements
Considerations for Sustainability
An important consideration throughout this project was that CCFNC was in its last year of funding
and had been scaling down its operations throughout our Capstone work. The Resource Directory will
continue to provide clinics and women with information about where to obtain affordable screening services.
Should CCFNC use the procedures our team developed for updating the directory regularly, it will ensure
that this resource remains a useful tool. In addition, the CAP Report provided stakeholders with tools to
discuss and identify new strategies for cervical cancer prevention. Furthermore, the regional meeting
generated momentum among local partners, such as the ENCCC, to engage with CCFNC in planning future
regional meetings for cervical cancer prevention. Please see Appendix B for recommendations for
sustainability by deliverable.
Professional Impact
Our team gained knowledge about cervical cancer, including the epidemiology, barriers, and
opportunities impacting provider efforts to prevent cervical cancer in NC. As we executed our Capstone
project, we gained many skills throughout the year that will be useful in our future public health work. The
KIIs improved our qualitative data collection and analysis skills. In organizing the regional meeting, we
improved skills related to: event planning, facilitating interactive breakout sessions, creating and delivering
effective presentations, and stakeholder engagement. We gained experience in questionnaire design and
analysis through the development of the Qualtrics survey that informed the Promotional Recommendations
Report. Through updating the online Resource Directory, we learned how to use WordPress, a web content
management tool. The project also afforded several opportunities to improve our report writing skills for
both internal and external documents.
As the scope of our deliverables and timelines changed, we learned that communication, flexibility,
and adaptability are crucial to a project’s success. A main challenge for us at the beginning of the year was
adapting to changes in organizational and project leadership. We learned how to accommodate different
management styles and advocate for clarity around project goals and expectations. Our ability to
communicate effectively as a team and to establish individual strengths, work styles, preferences, and
strengthened our ability to communicate with CCFNC and stakeholders, which was key to managing a project
that had several moving pieces at once.
XI. CONCLUSION
Over the past year, we have been charged with engaging stakeholders and developing tools and
resources through a variety of means in order to improve the state's healthcare capacity to provide cervical
cancer prevention services and reduce the disease's overall incidence and mortality rates in high burden
regions of NC. As evident in the literature, collaborating with stakeholders is key to quality improvement and
the facilitation of such services. Conducting KIIs, convening regional meetings, and developing CAPs are
effective in fostering discussion and action steps to reaching cervical cancer prevention goals. CCFNC used
these methods to gain a thorough understanding of the regional cervical cancer prevention landscape and
bring stakeholders together. Lastly, with the updates to the Resource Directory and the development of the
Promotional Recommendations Report, we expect that more providers, patients, and community members
will access important information related to cervical cancer prevention services.
We hope that through our various efforts we make an impact on cervical cancer by helping to
increase the capacity of our stakeholder groups to provide cervical cancer prevention services. Only together
XII. REFERENCES
American Cancer Society. (2011). Cancer facts and figures. No. 500811.
www.cancer.org/acs/.../acspc-029771.pdf. Published in 2011. Accessed October 2013.
Agurto, I., Arrossi, S., White, S., Coffey, P., Dzuba, I., Bingham, A., Bradley, J., & Lewis, R. (2005).
Involving the community in cervical cancer prevention programs. International Journal of Gynecology and
Obstetrics, 89, S38—S45. doi:10.1016/j.ijgo.2005.01.015
Allen, M. L., Culhane‐Pera, K. A., Pergament, S. L., & Call, K. T. (2010). Facilitating research faculty
participation in CBPR: development of a model based on key informant interviews. Clinical and
translational science, 3(5), 233-238.
Bigby, J., Ko, L.K., Johnson, N., David, M. M. A., & Ferrer, B. (2003). A community approach to
addressing excess breast and cervical cancer mortality among women of African descent in Boston.
Public Health Reports, 118, 338-347.
Butterfoss, F.D., Kegler, M.C., & Fransisco, V. T. (2008). Mobilizing organizations for health promotion:
Theories of organizational change. In Glanz, K., Rimer, B. K., & Viswanath, K. (Eds.), Health behavior
and health education: Theory, research, and practice. San Francisco: Jossey-Bass.
Centers for Disease Control and Prevention. (2014). Genital HPV infection – fact sheet. Retrieved from
http://www.cdc.gov/std/hpv/stdfact-hpv.htm
Community Tool Box (2013). Developing an action plan. Retrieved from
http://ctb.ku.edu/en/table-of-contents/structure/strategic-planning/develop-action-plans/main
Denslow, S.A., Knop, G., Klaus, C., Brewer, N.T., Rao, C., & Smith, J.S. (2012). Burden of invasive
cervical cancer in North Carolina. Preventive Medicine, 54, 270-276.
Documet, P., Green, H., Adams, J., Weil, L., Stockdale, J., Hyseni, Y. (2008) Perspectives of African
American, Amish, Appalachian and Latina Women on Breast and Cervical Cancer Screening:
Implications for Cultural Competence. Journal of Health Care Poor Underserved, 19(1), 56-74. doi:
Fouad, M. N., Nagy, M. C., Johnson, R.E., Wynn, T. A., Partridge, E. E., & Dignan, M. (2004). The
development of a community action plan to reduce breast and cervical cancer disparities between
Garner, E. I. (2003). Cervical cancer: Disparities in screening, treatment, and survival. Cancer
Epidemiology, Biomarkers & Prevention,12, 242-274s.
Katahoire, R. A., Jitta, J., Kivumbi, G., Murokora, D., Arube, W. J., Siu, G., Arinaitwe, L., Bingham, A.,
Mugisha, E., Tsu, V. (2008) An assessment of the readiness for introduction of the HPV vaccine in
Uganda. African Journal of Reproductive Health. 12 ( 3),
Katz, M. L. (2007). Key Informants' Perspectives Prior to Beginning a Cervical Cancer Study in Ohio
Appalachia. Qualitative Health Research., 17 (1), 131-141.
Leask, J., Jackson, C., Trevena, L., McCaffery, K., Brotherton, J. (2009). Implementation of the
Australian HPV vaccination program for adult women: Qualitative key informant interviews. Vaccine,
27(40), 5505, 5505-5512
McCarthy, S. H. (2013). Cervical cancer prevention in North Carolina: Strengthening health programs and
systems. Retrieved from
http://www.cervicalcancerfreecoalition.org/wp-content/uploads/Cervical-Cancer-Prevention-in-NC-Strengthening-Health-Programs-and-Syste....pdf
North Carolina Center for Health Statistics. (2008). Cancer in North Carolina. 2008 Report:
Cancer and income with a special report on cancer, income, and racial differences.
http://ucrf.unc.edu/publications/cancer_report_2008.pdf.
Nguyen, T., McPhee, S., Bui-Tong, N., Luong, T., Ha-Iaconis, T., Nguyen, T., Lam,
H. (2006). Community-based participatory research increases cervical cancer screening among
Vietnamese-Americans. Journal of Health Care for the Poor and Underserved, 17, 31–54. DOI:
10.1353/hpu.2006.0078
Rogers, M. (2003). Knowledge, technological catch-up and economic growth. Edward Elgar Publishing.
Texas Department of State Health Services (2006). Texas Cervical Cancer Strategic Plan. Retrieved from
https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&ved=0CCoQ
FjAA&url=http%3A%2F%2Fwww.dshs.state.tx.us%2Fbcccs%2FPDF%2Fcervical-cancer-strategic-plan.pdf&ei=PZVwUs6THNPHsASYu4C4Bw&usg=AFQjCNETO2Rz_M3SAgbtXmKf0bWehnZ
TYg&sig2=ZxJqgDRpfKNDqf06JKmHJQ
(2005). Advocating for cervical cancer prevention. International Journal of Gynecology and Obstetrics, 89,
S46—S54. doi:10.1016/j.ijgo.2005.01.010
WHO Regional Office for Europe (September 12, 2011). Scope and purpose. Retrieved from
http://www.euro.who.int/__data/assets/pdf_file/0018/152235/Cancer_mtg_scope_and_purpose.p
XIII. APPENDIX A: LOGIC MODEL
Figure 1: CCFNC Capstone Logic Model
XIV. APPENDIX B: CCFNC Capstone Deliverables
Deliverable 1: Statewide Summit Meeting Materials & Summary of Proceedings
Format: Meeting minutes, 3-4 page report, and 1 page executive summary.
Purpose: To engage and support NC coalition partners and community stakeholder groups (e.g.
NC County Health Directors) in considering enhanced strategic and sustainable action against cervical cancer that is consistent with their organizations’ public health mission and easily integrated into their current program operations.
Intended Audience(s): NC County Health Directors and other health department employees, immunization
staff, pharmaceutical companies’ representatives, medical professionals, CCFNC coalition members, and health educators throughout the state.
Activities: 1. Review CCFNC’s status and policy report on the state of cervical cancer
prevention in North Carolina
2. Develop note taking form for summit proceedings
a. Review note taking forms from other conferences
b. Draft note taking form for summit
c. Finalize note taking form
3. Attend the statewide summit, take notes on proceedings
4. Write summary of statewide summit proceedings to inform participants and
community stakeholders of meeting recommendations, action steps, and key commitments
a. Compile meeting notes
b. Draft summary of proceedings
c. Finalize summary of proceedings
Recommendations for
CCFNC: Continue to disseminate Summit Proceedings Report to stakeholders Post the report on the Cervical Cancer-Free Coalition website Reference and distribute report whenever representatives attend an event
Deliverable 2. Key Informant Interviews (KIIs) with Community Stakeholders in Areas of NC with a High Cervical Cancer Prevention Need (Northeast & South Central Regions)
Format: (1) 6-8 question Interview guide; (2) 30-60 interviews by phone or in-person; (3)
Compiled interview case notes report to inform regional meetings; (4) 1-2 page report outlining the key themes from interviews per high-need region
Purpose: To identify needs, resources, capacity (e.g. funding, staff, organizational capacity, current
services offered), and barriers (e.g. transportation, language barriers, insurance status) to providing cervical cancer prevention services for organizations and individuals in high-need regions.
Intended Audience(s): NC County Health Directors and other health department employees, immunization
Activities: 1. Submit IRB-exemption application for KIIs
2. Develop KII guide
a. Draft research and interview questions for ~30-45 minute interviews b. Pilot interview guide at Statewide Summit Meeting
c. Revise interview guide d. Finalize interview guide 3. Identify and recruit KII participants
a. Use existing CCFNC directory of community stakeholders to compile
a list of interview informants to be recruited (purposive and snowball sampling)
b. Consult with mentor team to identify additional key thought leaders in the field
c. Contact key informants via email and phone to participate in interviews
d. Schedule interviews with key informants
4. Conduct 30-60 (or until saturation) KIIs (both phone and in-person) in pairs using case notes method
5. Analyze KII findings and write a 1-2 page KII report of analysis per region a. Review case notes regular to identify emerging themes and new
questions to ask respondents
b. Develop codebook of topical and overarching themes
c. Code interview notes and create summaries
d. Draft a 1-2 page KII report (summary of themes and issues) for South Central Region
e. Draft a 1-2 page KII report (summary of themes and issues) for Northeast Region
f. Submit final KII reports for South Central and Northeast regions Recommendations for
CCFNC: Use the report to inform future regional meetings in the South Central or Northeast regions
Use the report to inform or identify areas for additional research in high-need regions
Deliverable 3: Updated Online Resource Directory
Format: Web-based resource directory
Purpose: To update this online directory so that it accurately reflects the latest community partner
and clinic information, as well as up-to-date cervical cancer screening guidelines around HPV co-testing.
Intended Audience(s): Medical and social service providers, as well as women ages 25-70 who are rarely
screened for cervical cancer (more than 3 years since the last pap smear), uninsured or under-insured women ages 21-70 in need of information about and locations for pap smears, and uninsured or under-insured adolescents aged 11-18 years of age who have not completed HPV dose administration in North Carolina.
Activities: 1. Update online Resource Directory
a. Create spreadsheet to track changes made to the directory. b. Update clinic information on spreadsheet
i. Create phone survey
ii. Call clinics to confirm information and inquire about transportation, accommodations for obese women, translation services, etc. iii. Adapt phone survey into a Qualtrics survey to be sent to clinics that
prefer to communicate information electronically iv. Distribute survey to those clinics that request it
2. Add material about new cervical cancer screening guidelines that include HPV co-testing
site with the new screening guidelines
b. Propose the language and location of a link from the screening page to another webpage to explain the new guidelines
c. Finalize website language and send to CCFNC
Recommendations: Use developed process to update Resource Directory annually
Review and update content on website annually
Deliverable 4. South Central Regional Meeting
Format: Meeting in a high-need region of the state (Fayetteville, NC), electronic invitations for
meeting, meeting agenda, Excel list of attendees, and narrative synthesis of meeting proceedings with action steps. 25-40 people attending the regional meeting (3-4 hours)
Purpose: Work with community stakeholders to create a community action plan to facilitate the
implementation of recommendations listed in the Cervical Cancer Prevention in North Carolina: Strengthening Health Programs and Systems report.
Intended Audience(s): NC County Health Directors and other health department employees, immunization
staff, medical professionals, CCFNC coalition members, and health educators from South Central region.
Activities: 1. Plan regional meeting logistics
a. In consultation with preceptor and key informants, identify meeting dates and locations
i. Create a mileage and driving chart for potential regional meeting areas and locations
b. Develop final budget for regional meeting and send to preceptor for review
c. Secure meeting logistics
i. Identify and contact potential venue locations availability, capability, and prices
ii. Visit potential venues to assess space
iii. Coordinate with venue contact to develop Event order
iv. Finalize and sign event order and submit to UNC accounting for payment
d. Coordinate with North Carolina Institute for Public Health (NCIPH) to handle registration
i. Draft and finalize scope of work for registration tasks and submit to NCIPH
ii. Submit registration materials (Names, email addresses of invitees, invitation text) to NCIPH
2. Develop regional meeting materials
a. Draft meeting materials for the regional meeting, including:
i. Meeting agenda outline
Identify and confirm speakers
ii. CCFNC recommendation handout
iii. Community action plan template/worksheets
iv. Map showing counties with BCCCP, Medicaid providers,
hospitals, and cancer centers from South Central Region
v. Speaker bios
vi. Meeting evaluation form
b. Finalize meeting materials and submit to NCIPH and create meeting
folders for attendees
3. Convene South Central Regional Meeting
a. Present factual information about cervical cancer in South Central region from KIIs and CCFNC research and solicit feedback from attendees on how to strengthen community resources
and sustainable activities that could be implemented within their organizations
c. Present information about new Breast and Cervical Cancer Control
Program (BCCCP) guidelines
d. Identify action steps that stakeholders can build into their current program plans using a minimal investment of financial or staff resources
e. Take meeting notes
Recommendations for
CCFNC: Identify a partner organization such as the Eastern North Carolina Cancer Coalition and encourage them to organize a regional meeting in the Northeast region
Share meeting materials to facilitate future meetings in different locations
Deliverable 5. South Central Region Community Action Plan (CAP) Report
Format: NarrativeReport (1 page executive summary + 3 page discussion, combined with
deliverable 4)
Purpose: 1. To summarize meeting proceedings and action steps to implement cervical
cancer prevention strategies
2. To make appropriate recommendations for stakeholder action and next steps
Intended Audience(s): Attendees of the regional meeting and CCFNC
Activities: 1. Create an outline for the CAP Report
a. Draft outline
b. Discuss in working meeting with mentors
c. Finalize outline
2. Write CAP Report
a. Send first draft to mentors
b. Incorporate mentor feedback and send second draft to mentors
c. Submit final CAP report to CCFNC for dissemination
Recommendations for
CCFNC: Follow-up with attendees via email; invite them to share their thoughts about the CAP report and progress in implementing strategies and actions steps
Include attendees’ responses in CCFNC newsletter
Deliverable 6. NC Cervical Cancer Resource Directory Promotional Recommendations Report
Format: Internal document (1-2 pages) outlining recommendations for objectives, target
audience, activities, and timeline.
Purpose: To recommend strategies to improve, widely disseminate, and encourage usage of the
NC Cervical Cancer Resource Directory
Intended Audience(s): CCFNC
Activities: 1. Conduct formative research for communication and outreach
a. Design 5-10 minute online survey to assess awareness of resource directory, improvements that can be made, and promotional strategies (e.g., media outlet identification)
b. Create and test Qualtrics survey
c. Disseminate survey to CCFNC coalition members and other
stakeholder groups
d. Send reminder email about survey
e. Close survey
2. Write Communication and Outreach Recommendations Report
a. Review and analyze results from survey to help inform communication and outreach recommendations and to inform updates to the resource directory
b. Outline communication and recommendations report
send to mentors
d. Incorporate feedback from mentors and finalize report 3. Finalize and submit communication and outreach recommendations report Recommendations for
CCFNC: Implement website improvements from the report Select and implement at least one method for promoting the Resource
Directory from the report
Consider how to evaluate the effectiveness and reach of promotion method(s)
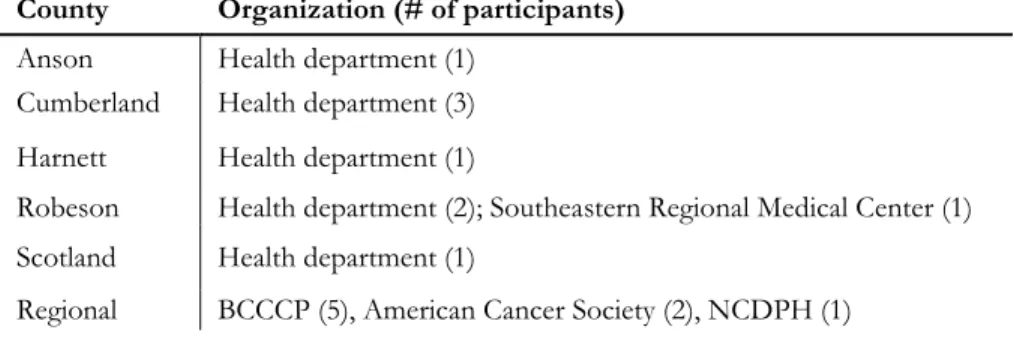
XV. APPENDIX C: KII Participants
Table 2: South Central KII Participants by County
County Organization (# of participants)
Anson Health department (1)
Cumberland Health department (3)
Harnett Health department (1)
Robeson Health department (2); Southeastern Regional Medical Center (1)
Scotland Health department (1)
Regional BCCCP (5), American Cancer Society (2), NCDPH (1)
Table 3: Northeast KII Participants by County
County Organization (# of participants)
Edgecombe Health Department (2)
Halifax Gregory B. Davis Foundation (3); Rural Health Group (1)
Martin- Tyrell-
Washington Health Department (2)
Nash Health Department (2)
Pitt Pitt Public Health Center (1); East Carolina University (1)
Warren Health Department (2)
XVI. APPENDIX D: Regional Meeting Attendance and Participant Evaluation
Table 4: South Central Regional Meeting Attendance by Organization
Organization Number Organization Number
Cumberland Co Health Dept 10 Robeson Co Health Dept 2
American Cancer Society 3 Wade Family Medical Center 2
Carolina Collaborative Community Care 2 Beaufort Co Health Dept 1
DHHS DPH 2 Cape Fear Valley Health System 1
East Carolina University 2 Community Care for Sandhills 1
Harnett Co Health Dept 2 Duplin Co Health Dept 1
Merck & Co Inc 2 Robeson Co Health Dept 1
NC BCCCP 2 Robeson Health Care Corporation 1
North Carolina Central University 2 WAMC Adolescent Clinic 1
Planned Parenthood of Central NC 2 Womack Army Medical Center 1
Table 5: South Central Regional Meeting Attendance by County
County Number
Beaufort 1
Cumberland 20
Duplin 1
Durham 2
Harnett 3
Pitt 2
Robeson 4
Scotland 1
Wake 3
Non-county 4
Table 6: Participant Satisfaction with Regional Meeting (n=36)
satisfied Not Somewhat satisfied Satisfied satisfied Very N/A
Handling of registration 0 0 3 33 0
Meeting rooms 0 6 13 17 0
Presentation: CC in SC NC 0 1 7 28 0
Presentation: Evidenced Based Action 0 1 8 27 0
Breakout sessions 0 0 5 31 0
Networking opportunities 0 0 5 29 2
Packet materials 0 0 10 25 1
Table 7: Participant Assessment of Meeting Utility (n=31)
Strongly disagree Disagree Agree Strongly agree
I'm glad we met in person 0 1 6 24
This meeting changed the way I think about cervical cancer
prevention 0 2 17 12
This meeting will help me improve my organization's approach to