Address for correspondence
Dr. Mohd Nurul Alam , Assistant Professor, Department of Dermatology and Venereology. Ibn Sina Medical College & Hospital, 1/1-B, Kallyanpur, Mirpur, Dhaka, Bangladesh. Email: [email protected]
Original Article
Association of plasma D-dimer concentration with
systemic sclerosis
Introduction
Systemic sclerosis (SSc) is a rare, multisystem disease, based on autoimmunological processes, vascular endothelial cell injury and an extensive activation of fibroblasts. It is characterized by a large individual variability in the extent of skin and organ involvement, as well as, in disease progression and prognosis. The skin, esophagus, lung, heart and kidneys are the most frequently
affected organs.1
Women are more frequently affected by SSc, with a female-to-male ratio between 3:1 up to 14:1. The age of disease onset ranges between 30 and 50 years. Male patients have earlier onset than female patients. Blacks with SSc are frequently younger than whites. Published data about incidence rate increased from 0.6 to 16 patients per million inhabitants, which is also true for the prevalence rates, which rose from 2 to 233 patients per million inhabitants per year, depending on methodological differences in case definition and ascertainment, as well as, the investigated time period.1
Hussain MA, Rahim MR*, Alam MN, Haque MR**
Department of Dermatology & Venereology, Ibn-Sina Medical College, Dhaka. * Department of Dermatology & Venereology, Rangpur Medical College, Rangpur ** Department of Transfusion Medicine, Ibn-Sina Medical College, Dhaka
Abstract
Objectives To establish the relationship between the level of plasma D-dimer concentration and systemic sclerosis.Methods This cross-sectional study was conducted in the department of dermatology and venereology, Ibn Sina Medical College & Hospital, Dhaka for one year. This study included 56 patients of systemic sclerosis. Systemic sclerosis was diagnosed by the panel of expert on the basis of history and American College of Rheumatology criteria. Statistical analysis of the results was obtained by using Windows based computer software devised with statistical package for social sciences (SPSS-20) (SPSS inc Chicago IL,USA).
Results The mean age of patients was 44.00 years. Majority were female (73.2%). Majority (76.8%) had diffuse cutaneous systemic sclerosis type. Higher level of plasma D-dimer was found in diffuse cutaneous systemic sclerosis than limited cutaneous systemic sclerosis, 538 mg/dl vs. 362 mg/dl (P<0.05).
Conclusion This study demonstrated that systemic sclerosis (SSc) patients with diffuse subset are characterized by increased plasma D-dimer values, reflecting a potential activation of both the hemostatic and fibrinolytic cascades, which might finally predispose these patients to thrombotic complications.
Key words
Patients with SSc are classified into two major subtypes depending on the extent of skin sclerosis – diffuse cutaneous systemic sclerosis (dcSSc) and limited cutaneous systemic sclerosis (lcSSc). Limited cutaneous systemic sclerosis is limited to the skin on the face, hands and feet. Diffuse cutaneous systemic sclerosis covers more of the skin, and is at risk of progressing to the visceral organs, including the kidneys, heart, lungs and gastrointestinal tract. Patients with lcSSc have a good prognosis, with 10-year survival of 75%, although <10% develop pulmonary arterial hypertension after 10 to 20 years. Patients with dcSSc have a 10-year survival of 55%. Death is most often from pulmonary, heart and kidney involvement although survival has greatly improved with effective treatment for kidney failure.2
Raynaud's phenomenon and microcirculatory abnormalities are well recognized features of SSc. Underlying abnormalities include endothelial dysfunction and hemorrheological abnormalities, similar to those seen in patients with macrovascular disease secondary to atherosclerosis. Atherosclerosis underlying cardiovascular mortality is the leading cause of death in developed countries.3
D-dimer is a fibrin degradation product (or FDP), a small protein fragment present in the blood after a blood clot is degraded by fibrinolysis. It is so named because it contains two crosslinked D fragments of the fibrin protein. It is an important test for patients with suspected thrombotic disorders. A negative result practically rules out thrombosis and a positive result can indicate thrombosis but does not rule out other potential causes. An increased D-dimer value in plasma is a reliable marker of a systemic prothrombotic state, likely superior to alternative fibrinolytic markers, and its measurement might be helpful in predicting or preventing thrombotic events.4 It also appears as
a strong, consistent predictor of cardiovascular events in the general population, in patients with cardiovascular disease and in other pathologies characterized by an increased risk of thrombosis. SSc patients are characterized by increased plasma D-dimer values reflecting a potential activation of both the coagulation and fibrinolytic pathways, which might finally predispose these patients to thrombotic complications. So this test thus aids to minimize thrombotic complications by adding antithrombotic agents at prothrombotic stage of systemic sclerosis.
Methods
It was a cross-sectional study carried out Department of Dermatology & Venereology, Ibn Sina Medical College & Hospital, Dhaka. Patients with positive serological test of
systemic sclerosis. History and clinical
examination findings were recorded. SSc was diagnosed by the panel of expert on the basis of history and American College of Rheumatology (ACR) criteria. Then diagnosis was confirmed by ANA, Anti-scl70, anti-centromere antibody and skin biopsy for histopathology test. The respondents were studied by measuring plasma D-dimer test. Then level of plasma D-dimer was determined at different stages of severity of SSc and finally levels of plasma D-dimer were correlated with the severity of disease.
Skin biopsy samples were taken from the skin lesion (up to dermis) of systemic sclerosis patients. The incision was elliptical in shape. Sample were merged in 10% formalin for histopathology. 2 ml of blood was drawn from the patient of SSc and tested at biochemistry department of Ibn Sina Medical College by indirect immunofluorescence on Hep-2 cell and ELISA. After an overnight fast, 2.7 ml blood was collected in a siliconized vacuum tube
anticoagulant agent). Samples were gently mixed and centrifuged for 10 min at 500C. Plasma were separated and stored in aliquots at -700C until measurement. Plasma D-dimer was
measured by automated enzyme linked
immunosorbent assay with fluorescent detection. This test was carried out by automated coagulation analyzer Sysmex CA-5000 series. Normal level of plasma D-dimer is <0.55 mg/L. More than normal level of plasma D-dimer indicates that there were chance of thrombosis in future.
Results
Table 1 shows the age and sex distribution of study population i.e. 56 patients. The mean age
of patients was 44.00±11.78 years. There were
41 female (73.2%) and 15 (26.8%) male patients.
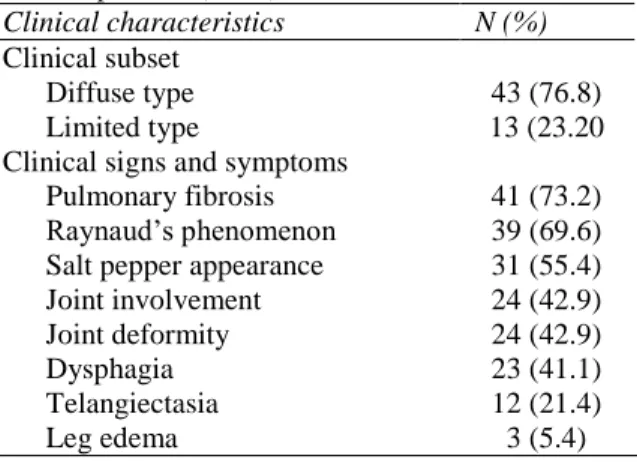
Regarding type of systemic sclerosis, there were 43 (76.8%) patients suffering from dcSSc and 13 (23.2) had lcSSc. Frequency of different cutaneous and systemic features is depicted in
Table 2. Pulmonary (73.2%), joints (42.9%) and gastrointestinal tract (41.1%) were the more frequently affected internal organs.
Although plasma D-dimer levels were elevated both dcSSc and lcSSc (Table 3), the higher level of plasma D-dimer was found in dcSSc than in lcSSc, 538 mg/dl vs. 362 mg/dl (P<0.05).
Discussion
D-dimer (a breakdown product of cross-linked fibrin) has been reported to be a marker of systemic prothrombotic state in patients with cardiovascular diseases.5-7 Meta analysis of prospective studies have shown that plasma levels of D-dimer were independent predictors of increased risk of coronary heart disease, stroke, peripheral arterial disease, as well as,
Table 1 Distribution of the systemic sclerosis patients by age (n=56).
Clinical characteristics N (%) Age (years)
20-30 6 (10.7)
31-40 11 (19.6)
41-50 23 (41.1)
51-60 9 (16.1)
> 60 7 (12.5)
Sex
Female 41 (73.2)
Male 15 (26.8)
Table 2 Clinical characteristics among systemic sclerosis patients (n=56).
Clinical characteristics N (%) Clinical subset
Diffuse type 43 (76.8)
Limited type 13 (23.20
Clinical signs and symptoms
Pulmonary fibrosis 41 (73.2) Raynaud’s phenomenon 39 (69.6) Salt pepper appearance 31 (55.4)
Joint involvement 24 (42.9)
Joint deformity 24 (42.9)
Dysphagia 23 (41.1)
Telangiectasia 12 (21.4)
Leg edema 3 (5.4)
Table 3 Comparison of mean plasma D-dimer
concentration (mg/L) with the subset of patients of systemic sclerosis.
Subset of systemic sclerosis
Level of plasma D-dimer in mg/L (mean±SD)
P Value Diffuse cutaneous
systemic sclerosis 538±45.65
0.001 Limited cutaneous
systemic sclerosis 362±36.39
cardiovascular death.8-13
higher D-dimer levels as compared to patients with inactive disease (p=0.27). No correlation was observed between plasma D-dimer concentration and age, sex, according to proposed by Medsger et al.15
The pathogenesis of the endothelial injury in SSc is as yet elusive and most biochemical evidence is often inconclusive or controversial. Although endothelial cell apoptosis and impaired angiogenesis have received major attention among the mechanisms involved in the characteristic vascular dysfunction. Recent studies provide clear evidence of a significant activation of the coagulation cascade, resulting in a procoagulant state that might finally raise the relative risk of thrombotic events in these patients. In SSc the peculiar vascular lesions and fibrosis are claimed to impair endothelial function, as suggested by impairment of fibrinolysis and activation of the coagulation pathway. The following loss of the balance between fibrinolysis and coagulation might finally contribute to vessel engulfment with fibrin and breakdown of vessel patency, symptomatic of a tendency to the development of thrombotic complications in this particular autoimmune disorder.4 D-dimer is the heterogeneous class of end stage degradation products that directly reflect the level of lysed cross-linked fibrin, occurring in vivo with a wide range of molecular weights. Therefore, D-dimer is a well recognized marker of a systemic prothrombotic state5,9 and appears as a strong, consistent predictor of cardiovascular events in the general population, in patients with cardiovascular diseases and in other pathologies characterized by an increased risk of thrombosis.10,12 Accordingly, D-dimer measurement could be reliably used as an initial screening test in patients with clinically suspected thrombosis, as its high negative predictive value enables to validly rule out tendency of SSc patients so far.13 At variance
with previous investigations2-4 increased plasma D-dimer values, reflecting a potential activation of both the coagulation and fibrinolytic pathways.
Conclusion
This study shows increased D-dimer values in SSc patients. The significant correlation suggests that SSc patients, especially those with diffuse subset, display a hypercoagulable state, which might finally predispose this peculiar subset of patients to the development of thrombotic complications.
References
1. Moinzadeh P, Denton Christopher P, Krieg T, Black Carol M. Scleroderma. Fitzpatrick’s Dermatology in General Medicine, 8th edn. Philadelphia: McGraw-Hill; 2012. P. 120-140.
2. Viswanath V, Meghana M Phiske MM, Vinay V GopalaniVV. Systemic Sclerosis: Current Concepts in Pathogenesis and Therapeutic Aspects of Dermatological Manifestations. Indian J Dermatol. 2013;58:255-68.
3. Ho M, Veale D, Eastmond C, Nuki G, Belch J. Macrovascular disease and systemic sclerosis. Ann Rheum Dis. 2000;59;39-43. 4. Prisco D, Antonucci E, Marcucci R.
D-dimer in the year 2000, Current data and new perspectives. Ann Ital Med Int. 2000;l15:267-72.
5. Falanga V, Kruskal JB, Franks JJ. Fibrin and fibrinogen-related antigens in systemic sclerosis (scleroderma). J Am Acad Dermatol. 1991;25:771-5.
6. Lippi G, Volpe A, Caramaschi P, Salvagno GL, Montagnana M, Guidi GC. Plasma D-dimer concentration in patients with systemic sclerosis. Thromb J. 2006;4:2. 7. Maeda M, Kachi H, Mori S. Plasma levels
of molecular markers of blood coagulation and fibrinolysis in progressive systemic sclerosis (PSS). J Dermatol Sci. 1996;11:223-7.
peripheral arterial occlusive disease. Eur Heart J. 2002;23:1309-16.
9. Lowe GDO. Can haematological tests predict cardiovascular risk? The 2005 Kettle Lecture. Br J Haematol. 2006;133:232-50. 10. Morange PE, Bickel C, Nicaud V, Schnabel
R, Rupprecht HJ, Peetz D et al. Haemostatic factors and the risk of cardiovascular death in patients with coronary disease: the AtheroGene study. Arterioscler Thromb Vasc Biol. 2006;26:2793-9.
11. Nylaende M, Kroese A, Stranden E, Morken B, Sandbaek G, Lindahl AK et al. Prothrombotic activity is associated with the anatomical as well as the functional severity of peripheral arterial occlusive disease. Thromb Haemost. 2006;95:702-7.
12. Rudnicka AR, Rumley A, Lowe GD, Strachan DP. Diurnal, seasonal, and blood-processing patterns in levels of circulating fibrinogen, fibrin D-dimer, C-reactive protein, tissue plasminogen activator, and
von Willebrand factor in a 45-year-old population. Circulation. 2007;115 :996-1003.
13. Tzoulaki I, Murray GD, Price JF, Smith FB, Lee AJ, Rumley A et al. Hemostatic factors, inflammatory markers, and progressive peripheral atherosclerosis. The Edinburgh Artery Study. Am J Epidemiol. 2006;163:334-41.
14. Valentini G, Della Rossa A, Bombardieri S, Bencivelli W, Silman AJ, D'Angelo S et al. European multicentre study to define disease activity criteria for systemic sclerosis. II. Identification of disease activity variables and development of preliminary activity indexes. Ann Rheum Dis. 2001;60:592-8. 15. Medsger TA Jr, Bombardieri S, Czirjak L,