Acute Encephalitis
WHAT’S KNOWN ON THIS SUBJECT: Encephalitis in children can cause significant neurologic sequelae, such as motor and cognitive impairment. Previous reported data are based mostly on questionnaires and clinical assessments.
WHAT THIS STUDY ADDS: Significant cognitive impairment, attention-deficit/hyperactivity disorder, and learning disabilities are common after childhood encephalitis. Even children who were considered fully recovered may be significantly affected. Identifiable pathogens, abnormal neuroimaging, and abnormal neurologic examination on discharge are risk factors of poor outcome.
abstract
OBJECTIVES: To examine the long-term motor and neurocognitive outcome of children with acute encephalitis and to look at possible prognostic factors.
METHODS:Children who were treated for acute encephalitis in 2000– 2010 were reevaluated. All children and their parents were interviewed by using structured questionnaires, and the children underwent full neurologic examinations, along with comprehensive neurocognitive, attention, and behavioral assessments.
RESULTS:Of the 47 children enrolled, 1 died and 29 had neurologic sequelae, including motor impairment, mental retardation, epilepsy, and attention and learning disorders. Children with encephalitis had a significantly higher prevalence of attention-deficit/hyperactivity disorder (50%) and learning disabilities (20%) compared with the reported rate (5%–10%) in the general population of Israel (P,.05) and lower IQ scores. Lower intelligence scores and significantly impaired attention and learning were found even in children who were considered fully recovered at the time of discharge. Risk factors for long-term severe neurologic sequelae were focal signs in the neurologic examination and abnormal neuroimaging on admission, confirmed infectious cause, and long hospital stay.
CONCLUSIONS:Encephalitis in children may be associated with signif-icant long-term neurologic sequelae. Significant cognitive impairment, attention-deficit/hyperactivity disorder, and learning disabilities are common, and even children who were considered fully recovered at discharge may be significantly affected. Neuropsychological testing should be recommended for survivors of childhood encephalitis.
Pediatrics2014;133:e546–e552
AUTHORS:Orli Michaeli, MD,aImad Kassis, MD,bYael
Shachor-Meyouhas, MD,bEli Shahar, MD,cand Sarit Ravid,
MDc
aDepartment of Pediatrics B,bPediatric Infectious Diseases Unit, andcPediatric Neurology Unit, Meyer Children’s Hospital, Rambam Health Care Campus, Haifa, Israel
KEY WORDS
attention-deficit, encephalitis, intelligence, sequelae
ABBREVIATIONS
ADHD—attention-deficit/hyperactivity disorder CI—confidence interval
CNS—central nervous system HSV—herpes simplex virus OR—odds ratio
Dr Michaeli conducted the initial analyses and drafted the initial manuscript; Dr Kassis conceptualized and designed the study, and reviewed and revised the manuscript; Dr Shachor-Meyouhas conceptualized the study, and reviewed and revised the manuscript; Dr Shahar designed the data collection questionnaires and reviewed and revised the manuscript; and Dr Ravid conceptualized and designed the study, conducted the initial analyses and examinations, and reviewed and revised the manuscript. All authors approved thefinal manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-3010
doi:10.1542/peds.2013-3010
Accepted for publication Dec 13, 2013
Address correspondence to Sarit Ravid, MD, Pediatric Neurology Unit, Meyer Children’s Hospital, Rambam Health Care Campus, Haifa 31096, Israel. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:No external funding.
Encephalitis is the presence of an
in-flammatory process in the brain pa-renchyma associated with clinical evidence of brain dysfunction.1
Diag-nosis requires evidence of neurologic dysfunction and central nervous sys-tem (CNS) inflammation.2 Viruses are
the most frequently diagnosed infec-tious cause of encephalitis; bacteria, fungi, and parasites are less common.3,4
The frequency and distribution of viru-ses or other infectious agents causing encephalitis vary according to geo-graphical region. In Asia, the major identified cause of acute encephalitis is the Japanese encephalitis virus.5
Tick-borne encephalitis virus and enterovi-rus are common in the Western world.6,7
Data on long-term neurologic outcomes in children with encephalitis are limited and vary depending on the different geographic areas and endemic agents. In the majority of studies, data were determined by using clinical follow-up assessments at outpatient clinics8,9
and structured questionnaires10; only
a few studies used standardized cog-nitive and behavioral tests.11–13
Pre-viously reported neurologic sequelae include developmental delay, motor deficits, epilepsy, and learning and be-havioral problems.9,10,14
Information regarding prognostic fac-tors of acute encephalitis in children is sparse, and data vary between studies. Several factors have been suggested as indicative of poor outcome, such as young age,8,11 deteriorating
electroen-cephalography (EEG) findings,11 focal
neurologic signs at discharge,9 low
Glasgow Coma Scale score on admis-sion,8,15 and abnormal neuroimaging
results.9,15
The aim of the present study was to evaluate the long-term sequelae of acute encephalitis in children and to look for predictors of long-term mor-bidity. Although most previous studies were based on clinical assessments or questionnaires, this study is distinctive
because it provides an objective neu-rocognitive performance assessment. This information can help in offering guidance in anticipatory counseling, as well as emphasizing important aspects for future follow-up.
METHODS
Study Population
Medical records of children and ado-lescents, aged 1 month to 18 years, ad-mitted to Meyer Children’s Hospital in Haifa, Israel, during the years 2000 to 2010 with afinal diagnosis of acute en-cephalitis were reviewed. The hospital is the main tertiary center in the north of Israel and serves a population of 280 000 children. Inclusion criteria in-cluded: (1) at least 1 symptom or sign of cerebral dysfunction, such as al-tered mental status, motor or sensory deficits, or seizures; and (2) at least 1 of the following signs of inflammation: fever (.38°C), white blood cell count
.153103cells/mL, C-reactive protein level .10 mg/L, and cerebrospinal
fluid cell count .6 cells/mL. Children with meningoencephalitis, demyelina-ting disease, or any underlying neuro-logic, systemic, or metabolic disease were excluded from the study. All eli-gible patients were contacted, by letter and then by telephone, to ask whether they would be willing to be followed up.
Fifty-eight patients fulfilled the inclu-sion criteria. Of those, 1 died during the acute phase, 8 declined to be assessed, and 3 could not be located. There was no difference between those children re-garding age at onset, gender, and pre-senting symptoms.
Written informed consent was obtained from the parents during the follow-up meeting. The study was approved by the institutional review board.
Data Collection
A structured form was used to obtain data from patients’ hospital records
regarding presenting symptoms and signs, laboratory examinations, EEG and neuroimaging studies, and clinical
findings at discharge.
The causative organisms were
identi-fied according to serum virus antibody titers (West Nile virus, mycoplasma,
Coxiella burnetii, and Bartonella spe-cies), and cerebrospinal fluid poly-merase chain reaction (herpes simplex virus [HSV], herpesvirus 6, and en-terovirus).
Outcome at discharge was classified for all survivors as good, moderate, or poor. Good outcome was defined as having no neurologic sequelae. Mod-erate outcome was defined as having minor to moderate sequelae, including altered behavior or clinical signs not affecting functions. Poor outcome was defined as having severe neurologic se-quelae that impair everyday functions.
Clinical, Motor, and Neurocognitive Assessment
All the children were interviewed and underwent thorough neurologic ex-amination by a pediatric neurologist during the follow-up visit. A structured questionnaire was used to obtain infor-mation from parents regarding comor-bid illnesses, medications, behavioral problems, school performance, and ability to perform daily activities.
The Kaufman Brief Intelligence Test16
was used to assess intelligence. This standardized, individually adminis-tered test yields 3 scores: verbal, non-verbal, and the overall score, known as the IQ composite. The mean6SD age-based standard score for each test is 100 6 15. Scores lower than 2 SDs from the mean were considered as retardation. Scores between 1 and 2 SDs from the mean were considered as borderline intelligence.
The diagnosis of attention-deficit/ hyperactivity disorder (ADHD) was based on the criteria of theDiagnostic and
ogist, using the patient’s history, in-terviews with the parents and child, and examination during the visit. In addition, attention and behavior were measured by using the Conners’Parent Rating Scales–Revised.18
Long-term Outcome
The long-term outcome was classified for all survivors as good, moderate, or poor. Good outcome was defined as having no neurologic sequelae. Mod-erate outcome was defined as having moderate sequelae, including ADHD, learning disabilities, or seizures af-fecting function but compatible with independent living. Poor outcome was defined as having severe neurologic sequelae that impaired everyday func-tions, contrary to independent living.
Statistical Analysis
Data were summarized as proportions or means6SDs.x2analysis was used to test for qualitative variables, and Student’sttest was used for quantita-tive variables.
Multivariate analyses of the associa-tions between clinical presentation, pathogen, EEG and neuroimaging stud-ies, and long-term outcome were con-ducted by using logistic regressions with odds ratios (ORs) and 95% confi -dence intervals (CIs). Analyses for the total sample were adjusted for age and gender. For all comparisons and anal-yses, aPvalue of,.05 was used as the cutoff point of statistical significance.
RESULTS
A total of 46 patients (28 boys and 18 girls) were enrolled in our study. Mean age at disease onset was 564.88 years (range: 1–17 years), and mean time to follow-up was 5.863.08 years (range: 1–11 years).
The most common presenting symp-toms were fever (73%) and altered mental status (69%). Hemiparesis was found in 13 (28%) patients and ataxia in 6 (13%) patients. Eighteen (39%) patients had seizures.
An etiologic agent was identified in 23 (50%) patients. The most common pathogen was enterovirus (9 patients), followed by HSV (6 patients).
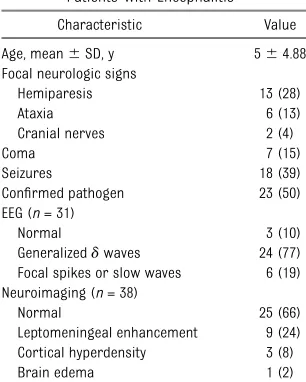
EEG was performed on 31 patients; re-sults were normal in only 3 (10%). Ab-normal results on neuroimaging studies were found in 39% of the patients (Table 1).
At discharge, neurologic examination was normal in 27 (58%) patients; 33% of patients showed focal motor deficits, and 15% of patients had various levels of cognitive impairment.
Long-term Motor and Cognitive Outcome
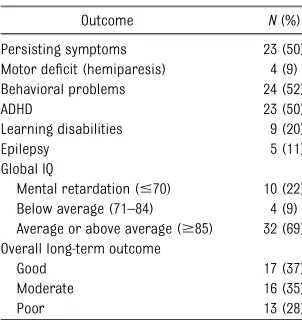
Persisting symptoms were reported by parents of 23 (50%) children. The most common residual symptoms were be-havioral problems (52%), recurrent
lepsy, which was intractable in 4 (80%).
Only 4 (9%) children had residual motor deficits. Those children suffered from spastic hemiparesis and were diag-nosed with herpes encephalitis. On the Kaufman Brief Intelligence Test, full-scale IQ .85 was found in only 69% of patients, compared with 84% in the general population, and 22% of patients had a full-scale IQ#70, com-pared with 2.2% in the general pop-ulation (Fig 1).
Twenty-three (50%) patients fulfilled the criteria for ADHD. This rate is signifi -cantly higher than the reported rate (5%–10%) in the general population of Israel19(P,.05). A substantial number
of patients had learning disorders (20%) compared with the reported rate (10%) in the general population of Israel20 (P, .05), and 8 (17%) were
placed in special education classes.
Overall, full recovery was found in only 17 (37%) patients. Moderate outcome was found in 35% of children, and 13 (28%) children suffered from poor outcome (Table 2).
Association Between Pathogen and Long-term Neurologic Outcome
Of 23 patients with verified pathogens, patients with HSV had the highest rate of neurologic sequelae, including signifi -cant motor deficit (66%), mental retar-dation (50%), ADHD (66%), and epilepsy (50%). However, patients with herpes encephalitis were not the only ones with an adversely affected prognosis. Of the 40 patients excluding those with HSV, ADHD was found in 18 (45%) patients and mental retardation in 7 (17%) (Table 3). Overall, having a
con-firmed etiologic agent was significantly associated with being at risk for poor long-term outcome (OR: 3.67 [95% CI: 1.1–15.68];P= .04).
TABLE 1 Initial Clinical Presentation, EEG, and Neuroimaging Studies in Patients With Encephalitis
Characteristic Value
Age, mean6SD, y 564.88 Focal neurologic signs
Hemiparesis 13 (28)
Ataxia 6 (13)
Cranial nerves 2 (4)
Coma 7 (15)
Seizures 18 (39)
Confirmed pathogen 23 (50) EEG (n= 31)
Normal 3 (10)
Generalizeddwaves 24 (77) Focal spikes or slow waves 6 (19) Neuroimaging (n= 38)
Normal 25 (66)
Leptomeningeal enhancement 9 (24) Cortical hyperdensity 3 (8) Brain edema 1 (2)
Association Between Clinical Presentation, EEG, and Neuroimaging Studies and Long-term Outcome
Predictors of poor long-term outcome are summarized in Table 4. The stron-gest predictors included long hospital stay (P = .004), abnormal neurologic examination results at discharge (P= .03), abnormal results on neuro-imaging studies (P = .04), and
con-firmed pathogen (P = .04). Although patients with seizures, abnormal neu-roimaging findings, and focal neuro-logic signs at presentation displayed a tendency toward increased risk for epilepsy, the number of patients was
too small to give reasonable inter-pretations.
Association Between Outcome at Hospital Discharge and Long-term Outcome
Figure 2 shows the distribution of out-come at hospital discharge and at the long-term follow-up visit. At hospital discharge, 27 (59%) patients had ap-parently made a full recovery, whereas 6 (13%) had moderate neurologic se-quelae and 13 (28%) had severe neu-rologic sequelae. Of the 13 children with severe sequelae, 6 improved (46%) and 3 (3%) fully recovered. Conversely, of the 27 children who were considered to have made a full re-covery at time of discharge, only 13 had a good long-term outcome. Four (15%) had mental retardation, 4 (15%) had learning disabilities, and 11 (41%) had ADHD.
DISCUSSION
The majorfindings of the present study are that encephalitis in children can lead to significant long-term neurologic sequelae, mainly reduced neurocog-nitive performance, behavioral prob-lems, ADHD, and learning disabilities. Overall, 50% of our patients suffered
from ADHD and 20% from learning disabilities. These values are signifi -cantly higher than the recent estimates of ADHD (5%–10%) and learning dis-ability (10%) rates in Israel (P,.05). Only 37% of the survivors had fully re-covered, and 28% of the children were left with severe neurologic disabilities that impaired everyday functions, such as motor deficits, mental retardation, and intractable seizures. Similar stud-ies that investigate the long-term out-come of encephalitis are sparse, and the results of long-term neurologic sequelae vary with geographic location and type of infectious pathogen. A similar incidence of severe neurologic sequelae was previously reported by Wang et al,9who found 25% significant
morbidity, such as epilepsy, mental re-tardation, and focal neurologic signs, in children who experienced acute en-cephalitis. In a study by Clarke et al,11
7 (35%) of 20 children who survived acute encephalitis experienced mod-erate to severe neurologic impairment. In contrast, an older study by Rautonen et al8found that only 6.7% of children
with encephalitis suffered from severe damage and 90.5% were cured with no or only minor sequelae. This study, however, included only clinical follow-up visits up to 6 months after discharge and may therefore have underesti-mated neurocognitive sequelae that could manifest at a later stage.
As noted earlier, the most common sequelae in our study was ADHD, which was found in 50% of patients. None of our patients was diagnosed with ADHD before the onset of disease, although most were too young at disease onset to manifest the characteristic clinical symptoms. Because all patients were healthy before the disease, we assumed the same incidence of the disorder in our study as in the general population. Although the association between ADHD and other brain insults, such as head trauma,21,22bacterial meningitis,23and FIGURE 1
Comparison of full-scale IQ of children with encephalitis versus the general population IQ.
TABLE 2 Long-term Motor and Cognitive Outcomes
Outcome N(%)
Persisting symptoms 23 (50) Motor deficit (hemiparesis) 4 (9) Behavioral problems 24 (52)
ADHD 23 (50)
Learning disabilities 9 (20)
Epilepsy 5 (11)
Global IQ
Mental retardation (#70) 10 (22) Below average (71–84) 4 (9) Average or above average ($85) 32 (69) Overall long-term outcome
Good 17 (37)
Moderate 16 (35)
Poor 13 (28)
brain tumor,24was previously reported,
little is known about its association with infectious encephalitis. Behavioral anom-alies similar to ADHD were first de-scribed as a complication of encephalitis
after the influenza epidemic of 1918.25
In their study on patients recovering from CNS infections due to enterovirus 71, Gau et al26 reported a 20%
in-cidence of ADHD, compared with 3% in
that relates to the core symptoms of ADHD.27 After tick-borne encephalitis,
children had lower scores than control subjects and relative impairment on several attention/concentration tests.13
Impaired memory function and reduced ability to concentrate was reported by Fowler et al14in children who survived
encephalitis. When assessed by using computerized cognitive tests, these children had slower reaction times but no differences in working memory com-pared with control subjects. This as-sociation is important, because ADHD symptoms may influence school per-formance as well as peer and family relationships. Early diagnosis of ADHD symptoms will allow early educational intervention and treatment if necessary.
Another importantfinding of our study was the significantly lower intelligence scores in children after acute enceph-alitis. A full-scale IQ of.85 was found in only 69% of patients, compared with 84% in the general population, whereas 22% of patients had a full-scale IQ of#70, compared with 2.2% in the general population. There is little information regarding cognitive func-tion after viral encephalitis in children. Similar significantly lower IQ evalua-tions were previously reported by Chang et al12in children who contracted
enterovirus 71 encephalitis. In con-trast, in a study from Germany, no significant difference was found in intelligence or neuropsychological eval-uations between children who experi-enced tick-borne encephalitis and control subjects.13
Lower intelligence scores and impaired attention and learning were found in our study even in children who were considered as fully recovered at the time of discharge. Of 27 children who were considered to have made a full recovery at the time of discharge, 4 Enterovirus 9 Mental retardation (3), ADHD (5), tic
disorder (3), sleep disturbances (2), learning disabilities (1), epilepsy (1)
7 (78)
HSV 6 Mental retardation (3), ADHD (4), motor deficit (4), tic disorder (3), sleep disturbances (3), epilepsy (3)
5 (83)
West Nile virus 3 ADHD (1), headaches (1) 1 (33)
Human herpesvirus 6 1 None 0 (0)
Mycoplasmapneumonia 1 ADHD (1), tic disorder (1) 1 (100) Coxiella burnetii 1 ADHD and learning disabilities (1), headaches
(1), sleep disturbances (1)
1 (100)
Bartonella henselae 1 None 0 (0)
Epstein-Barr virus 1 None 0 (0)
aPercentage of subjects with neurologic sequelae.
TABLE 4 Prevalence ORs for Poor Prognosis According to Clinical Presentation, EEG, and Neuroimaging Studies
Variable OR (95% CI) P
Female gender 0.49 (0.13–1.8) .39
Age at diagnosis 0.89 (0.75–1.05) .15 Focal neurologic signs at presentation 1.8 (0.5–6.32) .35 Coma at presentation 1.67 (0.37–7.6) .51 Admission to ICU 1.25 (0.33–4.73) .74
Seizures 2.33 (0.63–8.64) .2
Confirmed pathogen 3.67 (1.1–15.8) .04*
Abnormal EEG 2.75 (0.52–14.63) .24
Abnormal neuroimaging results 3.56 (0.91–13.94) .04* Abnormal neurologic examination results at discharge 3.11 (1.07–12.89) .03*
Hospital stay 1.18 (1.05–1.32) .004*
*P,.05.
FIGURE 2
(15%) had mental retardation, 11 (41%) had ADHD, and 4 (15%) had severe learning disability. A possible explana-tion for thesefindings is that cognitive recovery at discharge, especially in young children, is usually based on level of consciousness, awareness, and ori-entation. Neurocognitive parameters, such as memory, attention, or com-prehension, are not assessed, and fu-ture neuropsychological sequelae that interfere with intelligence and learning may thus be underestimated. In addi-tion, cognitive deficits at discharge may not be evident until the demands in-crease during school years. Similar late-onset cognitive sequelae were also seen in other studies.14,28,29
Epilepsy is a known sequelae of CNS infections. Furthermore, between 1% and 5% of epilepsy causes have been presumed to be due to CNS infections.30
Recurrent seizures, status epilepticus, and multifocal spikes on EEG were pre-viously reported as risk factors for postencephalitic epilepsy in children.31,32
In our study, 5 children (11%) developed long-term epilepsy; the condition was intractable in 4 children (80%). Seizures, abnormal neuroimaging findings, and focal neurologic signs at presentation displayed a tendency toward increased risk for epilepsy, but the number of patients was too small to make a mean-ingful interpretation.
Potential risk factors for a poor neu-rologic outcome in our study were identifiable pathogens, abnormal im-aging, abnormal neurologic examina-tion at discharge, and longer hospital stay. The cause of encephalitis was found in 50% of our patients. Thisfi nd-ing is consistent with previous studies, in which an etiologic diagnosis was made in 31% to 75% of cases.9–11,14,15
The most common pathogens in our study were enterovirus, HSV, and West Nile virus. Children with HSV encephalitis had the worst outcome. One patient died, and 5 of 6 survivors had severe
neuro-logic sequelae. These results are in line with other recent studies that found a high incidence of neurologic sequelae in children with HSV encephalitis33–35;
these sequelae were probably second-ary to cortical necrosis and infarction. However, all agents, even those pre-viously considered benign, such as en-terovirus,9,14 caused major neurologic
sequelae. Some 78% of our patients with enterovirus encephalitis experienced long-term neurologic sequelae, such as mental retardation (33%) and ADHD (55%). Enterovirus 71, a distinctive spe-cies of enterovirus that is common in the Asia-Pacific region but not in our region, has also been reported as being asso-ciated with ADHD and reduced cognitive functioning.12,26
Several studies, as well as our study, have shown the predictive value of ab-normal neuroimaging on both short-term7,36and long-term9,10,37outcomes of
childhood encephalitis. Thisfinding may be explained by irreversible parenchy-mal damage. Severe brain lesions may also cause focal neurologic signs and correlate with abnormal neurologic examinations at discharge, which in-dependently was found to be a predictor for long-term neurologic sequelae.9
Long hospital stay was also associated with poor prognosis in the present study and most likely reflects the se-verity of the disease. Other factors that reflect severity of disease, such as low Glasgow Coma Scale score on admis-sion,15,28,37 deep coma,28 and ICU
ad-mission,14 were previously found as
poor prognostic factors in other stud-ies (although not in the present study). Several authors have suggested that young age is associated with a poor long-term prognosis in children with encephalitis.8,11,38 We did not observe
this correlation in our study.
Although the strength of our study is the clinical examination and neuro-psychological evaluations of the pa-tients, it did have several limitations. As
a retrospective study, it is limited by the quality of information regarding symp-toms and signs, laboratory evaluation, and treatment during admission avail-able in hospital charts. Furthermore, because medications were not given according to a standardized protocol, the impact of certain treatments, such as steroids and intravenous immuno-globulin, could not be assessed. Simi-larly, because the diagnostic methods for causative organisms and antibodies for autoimmune encephalitis have evolved during the last decade, higher rates of causative organisms might be found if those children were being evaluated today. Nevertheless, the cause of encephalitis was found in 50% of our patients, which is consistent with pre-vious studies.9–11,14,15 In addition, the
study was also limited by the highly variable follow-up period. However, be-cause attention and cognitive deficits mayfirst be evident years after disease onset, their prevalence could be even higher. Another limitation of our study is the lack of a control group. Because all patients were healthy before the dis-ease, we compared the incidence of cognitive impartment, learning dis-abilities, and ADHD with the incidence of the general population, but it is not fully controlled for age and socioeconomic status.
CONCLUSIONS
Encephalitis in children may be asso-ciated with significant long-term neu-rologic sequelae. Significant cognitive impairment, ADHD, and learning dis-abilities are common, and even children who were considered fully recovered at discharge may be significantly affected. Neuropsychological testing should be recommended for survivors of child-hood encephalitis. Patients with iden-tifiable pathogens, abnormal imaging, abnormal neurologic examinations on discharge, and long hospital stay have an increased risk of a poor outcome.
fectious Diseases Society of America. The management of encephalitis: clinical prac-tice guidelines by the Infectious Diseases Society of America.Clin Infect Dis. 2008;47 (3):303–327
2. Glaser CA, Honarmand S, Anderson LJ, et al. Beyond viruses: clinical profiles and etiologies associated with encephalitis.
Clin Infect Dis. 2006;43(12):1565–1577 3. Kolski H, Ford-Jones EL, Richardson S, et al.
Etiology of acute childhood encephalitis at The Hospital for Sick Children, Toronto, 1994-1995.Clin Infect Dis. 1998;26(2):398– 409
4. Cizman M, Jazbec J. Etiology of acute en-cephalitis in childhood in Slovenia.Pediatr Infect Dis J. 1993;12(11):903–908 5. Solomon T, Dung NM, Kneen R,
Gains-borough M, Vaughn DW, Khanh VT. Japa-nese encephalitis. J Neurol Neurosurg Psychiatry. 2000;68(4):405–415
6. Koskiniemi M, Korppi M, Mustonen K, et al. Epidemiology of encephalitis in children. A prospective multicentre study. Eur J Pediatr. 1997;156(7):541–545
7. Fowler A, Stödberg T, Eriksson M, Wickström R. Childhood encephalitis in Sweden: etiol-ogy, clinical presentation and outcome.Eur J Paediatr Neurol. 2008;12(6):484–490 8. Rautonen J, Koskiniemi M, Vaheri A.
Prog-nostic factors in childhood acute encepha-litis.Pediatr Infect Dis J. 1991;10(6):441–446 9. Wang IJ, Lee PI, Huang LM, Chen CJ, Chen CL, Lee WT. The correlation between neurologi-cal evaluations and neurologineurologi-cal outcome in acute encephalitis: a hospital-based study.
Eur J Paediatr Neurol. 2007;11(2):63–69 10. Ilias A, Galanakis E, Raissaki M, Kalmanti M.
Childhood encephalitis in Crete, Greece.J Child Neurol. 2006;21(10):910–912 11. Clarke M, Newton RW, Klapper PE, Sutcliffe
H, Laing I, Wallace G. Childhood encepha-lopathy: viruses, immune response, and outcome.Dev Med Child Neurol. 2006;48(4): 294–300
12. Chang LY, Huang LM, Gau SS, et al. Neuro-development and cognition in children af-ter enaf-terovirus 71 infection.N Engl J Med. 2007;356(12):1226–1234
13. Schmolck H, Maritz E, Kletzin I, Korinthenberg R. Neurologic, neuropsychologic, and elec-troencephalographicfindings after European tick-borne encephalitis in children. J Child Neurol. 2005;20(6):500–508
14. Fowler A, Stödberg T, Eriksson M, Wickström R. Long-term outcomes of acute encephalitis
able at: www.pediatrics.org/cgi/content/full/ 126/4/e828
15. Aygün AD, Kabakus¸ N, Celik I, et al. Long-term neurological outcome of acute en-cephalitis.J Trop Pediatr. 2001;47(4):243– 247
16. Kaufman AS, O’Neal MR, Avant AH, Long SW. Introduction to the Kaufman Accessory Battery for Children (K-ABC) for pediatric neuroclinicians. J Child Neurol. 1987;2(1): 3–16
17. American Psychiatric Association. Diag-nostic and Statistical Manual of Mental Disorders. Fourth Edition (DSM-IV). Wash-ington, DC: American Psychiatric Associa-tion; 1994
18. Conners C.Conners’Rating Scale–Revised: Technical Manual. Tonawanda, NY: Multi-Health Systems Publishing; 1997
19. Barak Y. Attention deficit-hyperactivity disor-der. Available at: www.health.gov.il/Subjects/ KidsAndMatures/child_development/Documents/ ADHD-Barak.doc. Accessed August 22, 2013 20. Margalit M. The committee for examination
of extraction ability of students with learning disabilities. Ministry of Health, Is-rael, 1997. Available at: http://makom-m.cet. ac.il/pages/item.asp?s=6&id=200&defid= -1&page=5&item=288. Accessed August 22, 2013
21. Max JE, Lansing AE, Koele SL, et al. Attention deficit hyperactivity disorder in children and adolescents following traumatic brain injury. Dev Neuropsychol. 2004;25(1–2): 159–177
22. Levin H, Hanten G, Max J, et al. Symptoms of attention-deficit/hyperactivity disorder fol-lowing traumatic brain injury in children.J Dev Behav Pediatr. 2007;28(2):108–118 23. Wait JW, Stanton L, Schoeman JF.
Tubercu-losis meningitis and attention deficit hy-peractivity disorder in children. J Trop Pediatr. 2002;48(5):294–299
24. Ris MD, Noll RB. Long-term neurobehavioral outcome in pediatric brain-tumor patients: review and methodological critique.J Clin Exp Neuropsychol. 1994;16(1):21–42 25. Millichap JG. Etiologic classification of
attention-deficit/hyperactivity disorder. Pe-diatrics. 2008;121(2). Available at: www.pe-diatrics.org/cgi/content/full/121/2/e358 26. Gau SS, Chang LY, Huang LM, Fan TY, Wu YY,
Lin TY. Attention-deficit/hyperactivity-related symptoms among children with enterovi-rus 71 infection of the central nervous sys-tem. Pediatrics. 2008;122(2). Available at:
e452
27. Arensten AF. Fundamentals of attention-deficit/ hyperactivity disorder: circuits and pathways.
J Clin Psychiatry. 2006;67(suppl 8):7–12 28. Ooi MH, Lewthwaite P, Lai BF, et al. The
epidemiology, clinical features, and long-term prognosis of Japanese encephalitis in central Sarawak, Malaysia, 1997-2005.
Clin Infect Dis. 2008;47(4):458–468 29. Sejvar JJ. The long-term outcomes of
hu-man West Nile virus infection. Clin Infect Dis. 2007;44(12):1617–1624
30. Ohtsuka Y, Yoshinaga H, Kobayashi K, et al. Predictors and underlying causes of med-ically intractable localization-related epi-lepsy in childhood.Pediatr Neurol. 2001;24 (3):209–213
31. Annegers JF, Hauser WA, Beghi E, Nicolosi A, Kurland LT. The risk of unprovoked seizures after encephalitis and meningitis. Neurol-ogy. 1988;38(9):1407–1410
32. Chen YJ, Fang PC, Chow JC. Clinical char-acteristics and prognostic factors of post-encephalitic epilepsy in children. J Child Neurol. 2006;21(12):1047–1051
33. Ward KN, Ohrling A, Bryant NJ, Bowley JS, Ross EM, Verity CM. Herpes simplex serious neurological disease in young children: in-cidence and long-term outcome.Arch Dis Child. 2012;97(2):162–165
34. Lahat E, Barr J, Barkai G, Paret G, Brand N, Barzilai A. Long term neurological outcome of herpes encephalitis.Arch Dis Child. 1999; 80(1):69–71
35. Elbers JM, Bitnun A, Richardson SE, et al. A 12-year prospective study of childhood herpes simplex encephalitis: is there a broader spectrum of disease?Pediatrics. 2007;119(2). Available at: www.pediatrics. org/cgi/content/full/119/2/e399
36. Klein SK, Hom DL, Anderson MR, Latrizza AT, Toltzis P. Predictive factors of short-term neurologic outcome in children with en-cephalitis.Pediatr Neurol. 1994;11(4):308–312 37. DuBray K, Anglemyer A, LaBeaud AD, et al. Epidemiology, outcomes and predictors of recovery in childhood encephalitis: a hos-pital-based study.Pediatr Infect Dis J. 2013; 32(8):839–844
DOI: 10.1542/peds.2013-3010 originally published online February 17, 2014;
2014;133;e546
Pediatrics
Orli Michaeli, Imad Kassis, Yael Shachor-Meyouhas, Eli Shahar and Sarit Ravid
Long-term Motor and Cognitive Outcome of Acute Encephalitis
Services
Updated Information &
http://pediatrics.aappublications.org/content/133/3/e546 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/133/3/e546#BIBL This article cites 33 articles, 6 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/neurologic_disorders_
Neurologic Disorders
http://www.aappublications.org/cgi/collection/neurology_sub
Neurology
rning_disorders_sub
http://www.aappublications.org/cgi/collection/cognition:language:lea
Cognition/Language/Learning Disorders
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior
Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2013-3010 originally published online February 17, 2014;
http://pediatrics.aappublications.org/content/133/3/e546
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.