ORIGINAL RESEARCH
Effects of a multimodal exercise program in pedal dexterity
and balance: study with Portuguese older adults
of different contexts
João Silva&Olga Vasconcelos&Paula Rodrigues&
Joana Carvalho
Received: 27 July 2012 / Accepted: 1 April 2013 / Published online: 25 April 2013 #European Group for Research into Elderly and Physical Activity (EGREPA) 2013
Abstract This study investigated the effects of a
multimod-al exercise program (MEP) on pedmultimod-al dexterity and bmultimod-alance in two groups of older adult participants (65–92 years of age) from a psychiatric hospital center (HC), a residential care home (RCH), and a daily living center (DLC). The experi-mental group (EG) trained three times per week for 12 months, and the control group (CG) maintained their normal activities. The Mini-Mental State Examination and the Modified Baecke Questionnaire, as well as the Pedal Dexterity and the Tinetti tests, were applied to all subjects before and after the experimental protocol. Furthermore, the foot preference was controlled using the Lateral Preference Questionnaire proposed by Coren [10]. In the EG, the re-sults from the Pedal Dexterity test showed that both males and females from the RCH and DLC improved their perfor-mances after the MEP. In the HC, the males slightly de-creased their performance with both feet, contrarily to females. Both males and females from the CG decreased their pedal dexterity performance, namely, with the non-preferred foot. Concerning the Tinetti test, the EG of both
males and females from the HC, the RCH (males were better than females regarding the gender factor), and the DLC improved their balance after the MEP. In the CG, no signif-icant effects or interactions were found for any of the con-text groups.
Keywords Aging . Multimodal exercise program . Pedal
dexterity . Balance
Introduction
Aging is characterized by a series of degenerative changes in the different systems of the organism at the anthropometric, muscular, articular, cardiovascular, pul-monary, and neural levels, with consequences including the decline of the functional abilities and changes in physiological functioning [1, 30, 49]. Mobility problems in older adults are generally associated with deficits in balance, musculoskeletal pain, gait disorders, and a de-cline in muscular strength of the lower limbs, which are also a factor of fall risk and loss of autonomy for the execution of daily life activities [27, 46].
Compared to the upper limbs, the age-related reduction of muscle strength and mass of the lower limbs is more evident [2, 21]. This fact is important since these muscle changes of the lower limbs have higher correlations with mobility, functionality, and everyday activities of the older adults [7]. Among other characteristics, pedal dexterity is especially important to facing unexpected situations in order to prevent a fall and subsequent fracture or immobilization. Besides a good dynamic balance, it is important that older adults are able to behave quickly and efficiently when faced with these conditions [24].
The authors declare that this manuscript has never been previously published and submitted simultaneously for publication elsewhere. In addition, its publication has been approved by all coauthors. J. Silva (*)
:
O. VasconcelosMotor Control and Learning Laboratory, CIFI2D, Faculty of Sport, University of Porto, Rua Dr. Plácido Costa 91,
4200-450 Porto, Portugal e-mail: [email protected] J. Carvalho
Research Center in Physical Activity, Health and Leisure, CIAFEL, Faculty of Sport, University of Porto, Porto, Portugal P. Rodrigues
Dexterity is the ability to solve (precisely, quickly, ratio-nally, and deftly) a motor task in an adequate way using, in general, the limbs and the body. In this context, flexibility, in relation to the changing environment, is an important char-acteristic [48].
Likewise, balance is the basis of all voluntary motor abilities in this population [22,33]. Problems with balance control as a result of compromised balance conditions will inevitably affect motor strategies because one cannot acti-vate muscle-response synergies with appropriate timing, force, and muscle-response organization [40]. So, the con-cept of balance is the ability to maintain the body in equi-librium [41]. If an old person has reduced levels of balance, he or she will become more dependent on others and ex-posed to a higher risk of fall and fractures [17]. The distinct movement patterns of postural recovery, also referred to as
“postural strategies,” function to preserve equilibrium fol-lowing external disruptions by restraining the center of mass within the base of support [41].
Several studies have shown the efficiency of physical exercise programs, not only in the reduction of the risk of fall [14, 17, 36], but also in the reduction of the fear of falling [36].
We point out that a consequence of the aging process leads to a decline in the interference of pedal dexterity with balance. These aspects affect many of the older adults' daily life activities; falls or accidents that often occur could be avoidable if the individuals maintained high levels of motor fitness [25,28].
Aging is a growing phenomenon in modern-day socie-ties. In fact, the number of older adults (normal or with mental health disorders) accessing rehabilitation and inter-mediate care services, either in hospitals or at home, is rising and will continue to increase [9].
However, there is not much information or enough sys-tematic investigation about pedal dexterity ability in the Portuguese population, so this subject needs to be further studied in order to better understand the effect of exercise on both abilities (dexterity and balance) in old males and fe-males in different living situations.
With this research, it was our intention to investigate older adults from a wide range of the population as a whole; that is, we sought to include older adults with mental health disorders (from a psychiatric hospital center [HC] and a residential care home [RCH]) and without mental health disorders (namely, from an RCH and a daily living center [DLC]).
The aim of this investigation was to analyze the effects of a multimodal exercise program on the pedal dexterity and balance of older adults from different contexts. The follow-ing hypotheses were formulated a priori: (1) a multimodal exercise program improves pedal dexterity and balance and reduces the likelihood for falls in older adults from different
contexts, and (2) interventions targeted by a multimodal exercise program (over 12 months in older adults from different contexts) are effective in males and females.
Methods
Subjects
A convenience sample of 136 older adult participants from an HC, an RCH, and a DLC participated in this study. The eligible subject pool was restricted to older adults from both genders with the following characteristics: age ≥65 years, not engaged in any regular exercise training in the last year, older adults from an RCH and a DLC, lack of use of any medication known to affect balance and postural stability, and lack of any diagnosed or self-reported neurologic dis-orders or orthopedic medical conditions that contraindicate participation in exercise and testing. We point out that the older adults from the HC and the RCH (older adults with mental health disorders) were previously diagnosed with neurological deficits by neurologists and give authorization to participate in the study.
We try to compose the sample with an identical number of older adult participants in each context according to the gender and age. However, in some circumstances, this pro-ceeding was not possible, as was the case of HC and RCH (older adults with mental health disorders), contexts where the number of subjects in each group was different. The sample, in each context, was divided into two groups: an experimental group (EG) with practice of the multimodal exercise program and a control group (CG).
Before conducting the study, all participants received a complete explanation of the purpose, risks, and procedures of the investigation and provided their written informed consent. However, some older adults were excluded due to medical reasons, namely: in the EG, four males and two females from the HC, two males and two females from the RCH, and four males and two females from the DLC. In the CG, one male and one female from the RCH (mental health disorders), two males and three females from the RCH, and one female from the DLC. The characteristics of the partic-ipants of the study are shown in Table1.
Older adults from the EG were submitted to a multimodal exercise program for a period of 12 months, while those in the CG maintained their normal physical activity routine. All measurements and the multimodal exercise program were performed by the same evaluator together with teachers graduated from the University of Porto, Portugal. We emphasize that they were the evaluators prior and after training in both groups (EG and CG).
methods and procedures were approved by the Institutional Review Board.
Training protocol
The 12-month multimodal training protocol was held three times per week, and each session lasted about 60 min. All sessions were accompanied by appropriate music consid-ered relevant to the required activity and participants' age. A physical education instructor with specialization in older adults' training conducted the sessions. The exercise training was designed to promote the development of abilities, such as visuomotor coordination skills, flexibility, balance, strength, reaction time, speed of movements of the hands and feet, proprioceptive sensitivity, coincidence anticipa-tion, and visuomotor memory, as well as emotional and social aspects and awareness of the benefits of regular physical exercise.
Each training session included three main components: initial, a 10-min light warm-up and stretching exercises; fundamental, 45 min of light- to moderate-intensity exer-cises for the development of the abilities previously men-tioned, such as marching in place, stepping exercise at a speed of 40–60 beats per minute using a 15-cm-high bench, heel drops performed on a hard surface (a heel drop consists of raising the body weight onto the toes and then letting it drop to the floor, keeping the knees locked and hips extend-ed), muscular endurance exercises performed concentrically
and eccentrically involving the upper and lower limbs, strength training performed with elastic bands and dumb-bells, balance training with static and dynamic exercises (e.g., walking in a straight line, walking heel to toe, using additional resources, such as, balls, balloons, gymnastics parachutes and ribbons, hoops, ropes, and sticks), flexibility training involving the major muscle groups (quadriceps, back, and chest), and agility training (visuomotor coordina-tion) aimed at challenging hand–eye coordination, foot–eye coordination, dynamic balance, standing and leaning bal-ance, and psychomotor performance (coincidence anticipa-tion, proprioceptive sensitivity, visuomotor memory, and reaction time) including ball games, relay races, dance movements, and obstacle courses; and finally, 5 min of stretching. For the exercises in the second part of the ses-sion, for all the abilities mentioned above, the repetitions were increased from 8 to 15 and the number of sets in-creased to three.
Footedness assessment
The footedness assessment was evaluated by applying the Lateral Preference Questionnaire [10]. The older adults were asked to perform five motor tasks, which were associated with the five questions in the questionnaire. After register-ing the foot with which the subjects performed the activities, a ratio called the laterality quotient, using the following formula, was calculated:
LQ¼ðnumber of tasks with the right footnumber of tasks with the left footÞ
total number of tasks 100
The older adults were classified as right footed (value greater than zero) or left footed (value lower than zero) based on their score on this questionnaire, which identified 110 strong right footers (mean score of 92.84±11.39, where
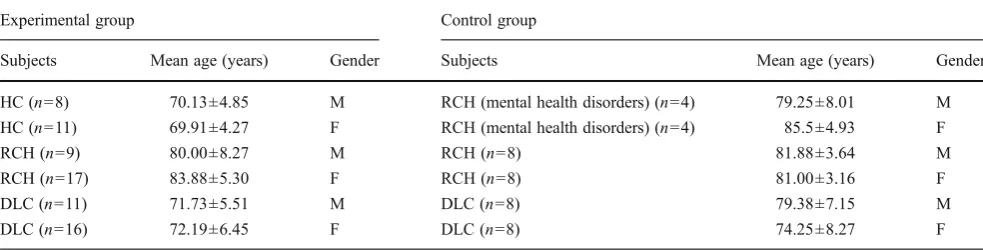
100 is maximal right footedness), and 2 strong left footers (mean score of −80.0 ± 0.0, where 100 is maximal left footedness). Both right footers' and left footers' data were included in our analysis, and according to their footedness, Table 1 Subject characteristics of experimental and control groups. Contexts, age and gender
Experimental group Control group
Subjects Mean age (years) Gender Subjects Mean age (years) Gender
HC (n=8) 70.13±4.85 M RCH (mental health disorders) (n=4) 79.25±8.01 M
HC (n=11) 69.91±4.27 F RCH (mental health disorders) (n=4) 85.5±4.93 F
RCH (n=9) 80.00±8.27 M RCH (n=8) 81.88±3.64 M
RCH (n=17) 83.88±5.30 F RCH (n=8) 81.00±3.16 F
DLC (n=11) 71.73±5.51 M DLC (n=8) 79.38±7.15 M
DLC (n=16) 72.19±6.45 F DLC (n=8) 74.25±8.27 F
HChospital center,RCHresidential care home,DLCdaily living center,RCHresidential care home: older adults with mental health disorders,M
the subjects used their preferred foot (PF) and their non-preferred foot (NPF) in the test. It is important to assess the non-preferred foot in order to appreciate—along with the preferred foot—its evolution from pre- to post-training and to observe if this evolution is similar when compared to the preferred foot.
In regard to the Lateral Preference Questionnaire, addi-tional items were added to the Lateral Preference Inventory [11] that provided a measure of handedness, footedness, vision, and hearing. Coren et al.'s measure of lateral prefer-ence has demonstrated a 92 % concordance between self-reports and direct behavioral performance [10,11].
Cognitive function assessment
To assess the subjects' global cognitive function, the Mini-Mental State Examination (MMSE) [15] was applied. MMSE total score ranges from 0 to 30. According to this questionnaire, none of the participants had any cognitive impairment (RCH: mean score of 28.23±2.11; DLC: mean score of 27.53±2.43), except the older adults with mental health disorders of the experimental group and the control group, where the doctors confirmed pathologies like schizo-phrenia, dementia, and depression.
Daily physical activity assessment
In order to quantify and verify if there was any change in the daily activities of the sample during the research period, the Modified Baecke Questionnaire [4] was completed before and after training. This questionnaire has been shown to generate valid and reliable classification scores for activity in older subjects providing a domestic, a sport, and a leisure-time activity score. The sum of the different scores gives the total activity of the subject. The questionnaires were com-pleted by the same researcher during a personal interview. For ethical reasons, this questionnaire was not applied to all the older adults with mental health disorders of the experi-mental group and the control group.
Instruments
Tapping pedal test
The tapping pedal test, as an indicator of pedal dexterity, was adapted from the Human Performance Measurement/Basic Elements of Performance apparatus [26]. A chair, a wooden ruler (1 m length, 1 cm width, and 2 mm height) fixed to the floor at the midpoint between the subject's two feet in the longitudinal direction with two signalizing stickers (10 cm× 10 cm), and one chronometer were necessary. The participant sat on a chair, with the lower limbs at a right angle and slightly
distant, so that each heel was near each anterior leg of the chair (see Fig.1).
The evaluator set the chronometer to 10 s and had it count down. At the command of “ready… start” by the evaluator, each participant was instructed to tap alternately as quickly as possible in the lateral direction (did a sort of tap dance) using one foot at a time. In a period of 10 s, they tapped on the signalizing stickers (the width of the signal-izing stickers was 10 cm, and the distance between them was 45 cm) to avoid accuracy errors.
The subjects performed two trials for each foot. The results included the greatest number of taps done by each foot; therefore, this study only considered the better trial by each subject. Finally, the samples were counterbalanced; that is to say, half of the group began the tests with the PF, and the other half started with the NPF. Then, the contralat-eral foot was assessed. Following this procedure, we avoided the possibility of transfer of learning between feet. The same occurred with respect to the tests; subjects were counterbalanced according to the first test performed, with a time break between both tests.
The functional characteristics of footedness (e.g., the relationship between the preferred limb to execute a manip-ulative or mobilizing action, such as kicking a ball, and the other foot [non-preferred] that provides stabilizing support) have been studied in children [44] but not in older adults.
Tinetti test
Balance was evaluated using the Performance-Oriented As-sessment of Balance and Mobility, also known as the Tinetti test. This instrument was developed by Tinetti [45], and it assesses the predisposition for falls in older adults through the quantitative evaluation of a set of tasks related to balance and mobility that are performed by the subject after being explained by the investigator.
items include: (1) sitting balance; (2) rising from a chair; (3) immediate standing balance (first 3–5 s); (4) standing bal-ance; (5) with feet as close together as possible, the exam-iner pushes lightly with his palm on the subject's sternum three times (nudge); (6) eyes closed in the same position; (7) turning 360°; and (8) sitting down. Static balance is deter-mined by adding up to a maximum score of 16 points. The gait items include: (1) initiation of gait, (2) step length and height, (3) step symmetry and continuity, (4) path direction, (5) trunk sway, and (6) walking stance. This item adds up to a maximum score of 12 points. The total score ranges from 0 to 28 points. Lower scores indicate poorer performance.
Subjects that reach less than 19 points show high risk of fall, and those with scores between 19 and 24 points show moderate risk [40,45].
Statistical analysis
All data were analyzed with the Statistical Package for the Social Sciences (SPSS: version 19.0). They were checked for distribution, and the means and standard deviation were calculated. Descriptive statistics and tests for normality (Shapiro–Wilk test) were performed for all outcome vari-ables. To analyze the multimodal exercise program effect, a two-way ANOVA 2×2 (time, from pre- to post-training; gender, males and females) was used. This analysis was performed for the two groups (experimental group and the control group) and contexts (HC, RCH, DLC) separately and for each foot (PF and NPF). When ANOVA revealed significant interaction (time × gender), Bonferroni post hoc tests were performed to determine differences between the initial and the final values in each group. Statistical signif-icance was set atp≤0.05.
Results
Concerning the Modified Baecke Questionnaire data, and regardless of the exercise program, significant increases from pre- to post-training in the experimental group were found in the residential care home and the daily living center (p<0.001). The control group maintained the level of daily physical activities from pre- to post-training: residential care home (p=0.148) and daily living center (p=0.248).
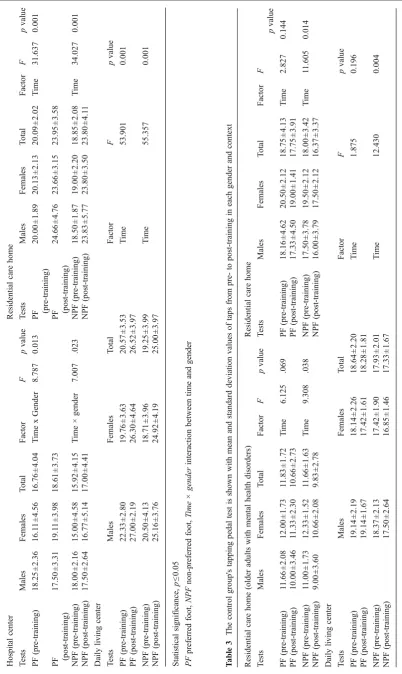
Tapping pedal test: pedal dexterity
Table2presents mean and standard deviation values of the tapping pedal test for the experimental group (males and females) of the hospital center, residential care home, and daily living center as a function of times of assessment and foot. In the experimental group of the hospital center, a significant main effect was found for the interaction
between time and gender with the PF [F1, 11=8.787; p=
0.013] and the NPF [F1, 11=7.007; p=0.023]. More
partic-ularly, males had slightly decreased performance with both feet from pre- to post-training (PF: from 18.25±2.36 taps to 17.50±3.31 taps and NPF: from 18.00±2.16 taps to 17.50± 2.64 taps), while females improved their performance with both feet from pre- to post-training (PF: from 16.11±4.56 taps to 19.11±3.98 taps and NPF: from 15.00±4.58 taps to 16.77 ± 5.14 taps). No other significant main effect was found.
In the residential care home, a significant main effect was found for time with the PF [F1, 19=31.637;p<0.001] and
the NPF [F1, 19=34.027; p<0.001]. Namely, there was a
significant improvement in performance from pre- to post-training (PF: from 20.09±2.02 taps to 23.95±3.58 taps and NPF: from 18.85±2.08 taps to 23.80±4.11 taps). No other significant main effect or interactions were found.
In the daily living center, a significant main effect was found for time with the PF [F1, 17=53.901;p<0.001] and
the NPF [F1, 18=55.357; p<0.001]. More precisely, there
was a significant improvement in performance from pre- to post-training (PF: from 20.57±3.53 taps to 26.52±3.97 taps and NPF: from 19.25±3.99 taps to 25.00±3.97 taps). No other significant main effect or interactions were found. Table 3 presents mean and standard deviation values for the control group's tapping pedal test (males and females) of the residential care home (older adults with mental health disorders), the residential care home, and the daily living center as a function of times of assessment and foot.
In the control group of the residential care home (older adults with mental health disorders), a significant main effect was found for time [F1, 4=9.308;p=0.038], only for
the NPF. More specifically, there was a significant decrease in performance from pre- (11.66±1.63 taps) to post-training (9.83±2.78 taps). No other significant main effect or in-teractions were found.
In the residential care home, a significant main effect was found for time [F1, 6=11.605;p=0.014], only for the NPF.
In particular, there was a significant decrease in performance from pre- (18.00 ±3.42 taps) to post-training (16.37 ±3.37 taps). No other significant main effect or interactions were found.
In the daily living center, a significant main effect was found for time with the NPF [F1, 13=12.430; p= 0.004].
More specifically, there was a significant decrease in per-formance from pre- (17.93 ± 2.01 taps) to post-training (17.33 ±1.67 taps). No other significant main effect or in-teractions were found.
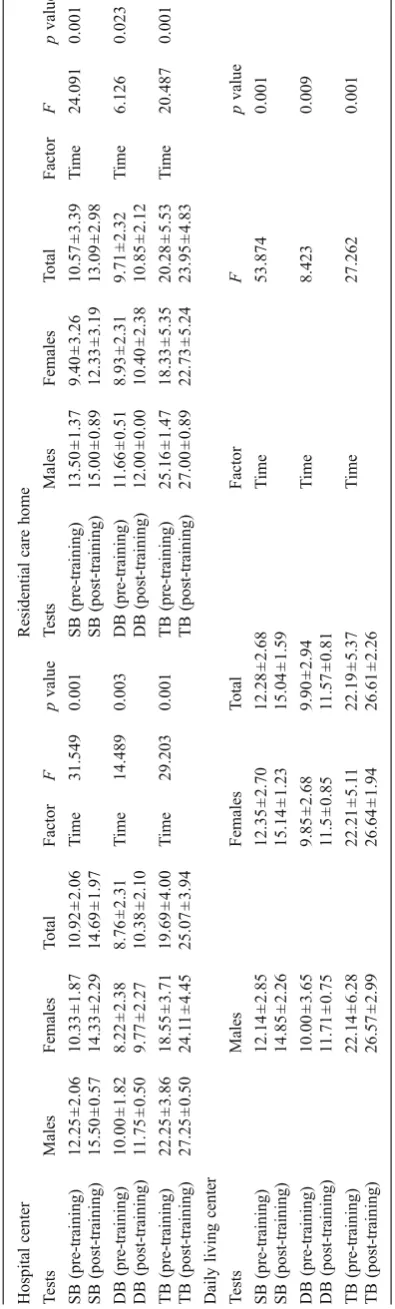
Tinetti test: balance
of the hospital center, the residential care home, and the daily living center as a function of times of assessment. In the experimental group of the hospital center, the time factor was significant for the static balance (SB) [F1, 11=31.549;p
< 0.001], the dynamic balance (DB) [F1, 11= 14.489; p=
0.003], and the total balance (TB) [F1, 11= 29.203; p<
0.001]. From pre- to post-training, all of the older adults in the sample had a significant improvement of performance in the SB (from 10.92±2.06 to 14.69±1.97 points), DB (from 8.76±2.31 to 10.38±2.10 points) and TB (from 19.69±4.00 to 25.07±3.94 points). No other significant main effect or interactions were found. In the hospital center, after the physical exercise program, the older adults presented a low risk of fall (25.07 ±3.94 points), but at the beginning, they showed a moderate risk of fall (19.69 ±4.00 points) as mea-sured by the Tinetti test [45].
In the residential care home, the time factor was signifi-cant for the SB [F1, 19=24.091;p<0.001], the DB [F1, 19=
6.126;p=0.023], and the TB [F1, 19=20.487;p<0.001]. We
found that from pre- to post-training, all the older adults in the sample experienced a significant improvement of per-formance in SB (from 10.57±3.39 to 13.09±2.98 points), DB (from 9.71±2.32 to 10.85±2.12 points), and TB (from 20.28±5.53 to 23.95±4.83 points). The gender factor was also significant for the SB [F1, 19=6.823;p=0.017], the DB
[F1, 19=5.691; p=0.028], and the TB [F1, 19=6.930; p=
0.016]. Males obtained a better performance in all of the three tests: SB (14.25 ± 1.18 points), DB (11.83 ± 0.25 points), and TB (26.08±1.18 points). In comparison, fe-males performed the tests as follows: SB (10.86 ± 3.23 points), DB (9.66 ± 4.69 points), and TB (20.53 ± 5.29 points). We verified that after the exercise program, females were at a threshold that indicated a moderate risk of fall (22.73 ±5.24 points), but at the beginning, they showed a high risk of fall (18.33 ±5.35 points). On the other hand, males showed a low risk of fall in the pre- (25.16 ±1.47 points) and post-training (27.00 ±.89 points), as measured by the Tinetti test [45].
In the daily living center, the time factor was significant for SB [F1, 19=53.874; p<0.001], DB [F1, 19=8.423; p=
0.009], and TB [F1, 19=27.262;p<0.001]. More
specifical-ly, from pre- to post-training, all the older adults in the sample showed a significant improvement of performance in SB (from 12.28±2.68 to 15.04±1.59 points), DB (from 9.90±2.94 to 11.57±0.81 points), and TB (from 22.19±5.37 to 26.61±2.26 points). No other significant main effect or interactions were found.
In the daily living center, after the exercise program, the older adults had a low risk of fall (26.61 ±2.26 points), but at the beginning, they presented a moderate risk of fall (22.19 ±5.37 points). In the control group, no significant main effect or interactions were found for any of the context groups or variables, from pre- to post-training.
Discussion
The purpose of this study was to investigate the effects of a multimodal exercise program on pedal dexterity and balance by comparing older adults from different contexts. In the tapping pedal test, the results showed that for the time factor, both genders of the experimental group from the residential care home and the daily living center improved their perfor-mance significantly with both feet (preferred foot and non-preferred foot). In the hospital center, a significant main effect was found for the interaction between time and gen-der, namely males slightly decreased their performance while females improved theirs with both feet (preferred foot and non-preferred foot). In the control group, a significant main effect was found for time in all contexts; that is, both genders decreased their performance with the non-preferred foot.
It should be noted that in our study, all the older adults without mental pathologies of the experimental group (from the residential care home and the daily living center) im-proved their pedal dexterity with both feet through regular physical exercise. In other words, our results are in accor-dance with previous studies, which claim that the pedal dexterity of older adults can be improved through the prac-tice of regular physical exercise [23,32]. On the other hand, low levels of physical activity and weakness of the lower limbs have been identified as risk factors for functional status decline and falls [20,28].
Literature emphasizes that an active lifestyle, complemented by regular physical exercise programs, can make an old person capable of performing daily tasks, providing meaningful im-provement at the physical level [3,42,51].
Furthermore, the muscular structure of the lower limbs presents a strong relation with the mobility and functionality of the older adults [7]. It is evident that the training of balance and muscular strength (especially directed to the lower limbs) can improve the physical function and the functional mobility (e.g., walking speed, transferences, climbing stairs, and standing up from the position of sitting down) and reduce the risk of fall [17, 28, 39].
As mentioned above, the males of the experimental group from the hospital center slightly decreased their performance with both feet from pre- to post-training. This means that the effect of the multimodal exercise program was not enough to improve this ability. Addi-tional studies are necessary to elucidate the effects (with respect to this ability) of exercise on men with mental health disorders. In this way, the risk of injury—namely falls and fractures—is even greater among adults with impaired cognitive functioning [6, 29]. Additionally, it is important to recall that due to their impaired motor and mental function, adults with dementia have an
increased risk of falling, and those who do fall run the risk of further injuries [31].
On the other hand, the females of the experimental group from the hospital center improved their performance with both feet from pre- to post-training. These results are in agreement with other studies that have shown that structured exercise training leads to an increase in physical fitness and function in daily life in adults diagnosed with dementia [18,
19]. Likewise, exercise in old age is increasingly recognized as an important tool to postpone disability and improve function [6, 38]. Carmeli, Zinger-Vaknina, Morad, and Merrick [8] reported identical results to ours, with females improving their pedal dexterity, that is, an improvement in balance and muscle strength as the result of the applied exercise program.
Furthermore, findings have shown that adults who are generally active have a smaller risk of developing dementia than those who take part in fewer activities. Whether the activity is energy intensive or not plays a minimal role in this context [34]. Even in the oldest subjects (over 85 years), there are indications that regular physical activity protects against the development of dementia [43].
Exercise for adults diagnosed with dementia can yield physiological, psychological, and emotional effects. There is no basis for assuming that the volume and intensity of exercise components, such as muscle strength, flexibility, and balance, act differently in comparison to adults without dementia. When considering the impact of exercise on cog-nition and emotion, there is little knowledge regarding the amount and type of activity conducive to better results. Studies in the field of motor learning [37] indicate that the most important factors for learning are an adequate volume of practice together with a perceived meaningful and moti-vating task. However, considering our results, we think that additional studies are necessary to elucidate the effects of exercise on adults diagnosed with mental health disorders.
In our study, a pedal dexterity decrease was verified for the non-preferred foot in the control group (from the resi-dential care home [older adults with mental health disor-ders], the residential care home, and the daily living center) for both genders, from pre- to post-training. In this sense, our results may suggest that the effect of aging is most visible in subjects who prefer the left foot. Nevertheless, further studies are necessary to confirm this hypothesis.
females were at a threshold that indicates a moderate risk of fall when, at the beginning, they exhibited a high risk. Other-wise, males showed a low risk. For the daily living center, the older adults displayed a low risk of fall after the training, when at the beginning it was moderate.
In summary, in the experimental group, all participants in this study improved their performance from pre- to post-training. Our results showed that the benefits of the multi-modal exercise program are numerous, namely in balance, leading to a decrease of the fall risk [17, 35]. As some studies also confer (e.g., [12, 13]), it is expected that the older adults from our sample will be more autonomous when performing activities like sitting down, taking a bath, crossing a street, or cleaning a window.
Studies have shown that improvements in the proprio-ception and standing balance control of older adults may be specific to the type of physical training undertaken [47,50]. It is important to mention that in our 12-month exercise program, we applied some Tai Chi exercises. One activity that has shown a strong relationship with the proprioceptive ability is the traditional Chinese exercise of Tai Chi, which involves slow movements and continuous monitoring of the body position. Tai Chi has been associated with increased joint position sense [47] and a way to enable older adults to feel their joint motion [50].
In the control group, no significant main effect or in-teractions were found in any of the context groups. These data are not in agreement with the study developed by Demura et al. [13], who find that with aging, balance de-clines especially after 80 years of age. Supported by these results, the authors suggest that the induced alterations through aging have influences on balance [16]. The loss of motor function is a common consequence of old age, and it is associated with adverse health consequences [5,12].
The major limitation of our study was the difficulty of finding a sufficient number of older adults with mental health disorders who could perform a 1-year program of regular exercise. A key strength of our study is that, to our knowledge, there is not much information or systematic research on this subject (in the Portuguese population). So we believe that our results can contribute to a better under-standing of the effect of exercise in the pedal dexterity and balance in old males and females from different contexts.
As a conclusion, we confirmed our previous hypothesis, noting that from pre- to post-training: (1) in the hospital center, males slightly decreased their performance with both feet while females improved theirs; (2) in the residential care home and the daily living center, the older adults improved their performance significantly with both feet. Furthermore, in the Tinetti test, the older adults from the hospital center, the residential care home (gender factor: males better than females), and the daily living center improved their balance. Finally, we believe that Portuguese society should pay
special attention to multimodal exercise programs for older adults because they seem to improve some important motor and functional abilities, such as pedal dexterity and balance, contributing in this way to an increase of the autonomy and a better quality of life for the older population.
Acknowledgments Funding/support: This research was funded by the Portuguese Foundation of Science and Technology, grant PTDC/ DES/108780/2008-FCOMP-01-0124-FEDER-009606. The first author was awarded grants from the Portuguese Foundation of Science and Technology (SFRH/BD/40196/2007). We wish to thank the elderly who participated in this study. We also thank all the staff of theConde de FerreiraHospital Center in Porto, whose generous and skillful help made this work possible.
Disclosures
Conflict of interest Guido Schröder, Andreas Knauerhase, Günther Kundt and Hans-Christof Schober declare that they have no conflict of interest.
Informed consent For studies with human subjects All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
Animal studies Not applicable.
References
1. Akgün KM, Crothers K, Pisani M (2012) Epidemiology and man-agement of common pulmonary diseases in older persons. J Gerontol A: Biol Sci Med Sci 67A(3):276–291
2. American College of Sports Medicine ACSM (2003) Diretrizes do ACSM para os testes de esforço e sua prescrição (6 th ed. ed.) [Guidelines of ACSM for effort testing and prescription]. Editora Guanabara, Rio de Janeiro-RJ
3. Aoyagi Y, Shephard RJ (2010) Habitual physical activity and health in the elderly: The Nakanojo Study. Geriatr Gerontol Int 10(Suppl 1):S236–S243
4. Baecke JAH, Burema J, Frijters JER (1982) A short questionnaire for the measurement of habitual physical activity in epidemiolog-ical studies. Am J Clin Nutr 36:936–942
5. Buchman AS, Wilson RS, Bienias JL, Bennett DA (2009) Change in frailty and risk of death in older persons. Exp Aging Res 35(1):61–82 6. Cameron ID, Murray GR, Gillespie LD, Robertson MC, Hill KD, Cumming RG, Kerse N (2010) Interventions for preventing falls in older people in nursing care facilities and hospitals. Cochrane Database Syst Rev 20(1)
7. Carmeli E, Reznick AZ, Coleman R, Carmeli V (2000) Muscle strength and mass of lower extremities in relation to functional abilities in elderly adults. Gerontology 46(5):249–257
8. Carmeli E, Zinger-Vaknina T, Morad M, Merrick J (2005) Can physical training have an effect on well-being in adults with mild intellectual disability? Mech Ageing Dev 126(2):299–304 9. Comas-Herrera A, Wittenberg R, Martin Knapp LP, MRC-CFAS
10. Coren S (1993) The Lateral Preference Inventory for measurement of handedness, footedness, eyedness and earedness: norms for young adults. Bull Psychotomic Soc 31(1):1–3
11. Coren S, Porac C, Duncan P (1979) A behaviorally validated self report inventory, to assess four types of lateral preferences. J Clin Neuropsychol 1:55–64
12. Delmonico MJ, Harris TB, Lee JS, Visser M, Nevitt M, Kritchevsky SB, Tylavsky FA, Newman AB (2007) Alternative definitions of sarcopenia, lower extremity performance, and func-tional impairment with aging in older men and women. J Am Geriatr Soc 55(5):769–774
13. Demura S, Minami M, Nagasawa Y, Tada N, Matsuzawa J, Sato S (2003) Physical-fitness declines in older Japanese adults. J Aging Phys Act 11(1):112–122
14. DeVito CA, Morgan RO, Duque M, Abdel-Moty E, Virnig BA (2003) Physical performance effects of low-intensity exercise among clinically defined high-risk elders. Gerontology 49(3):146–154 15. Folstein MF, Robins LN, Helzer JE (1983) The mini-mental state
examination. Arch Gen Psychiatry 40(7):812. doi:10.1001/ archpsyc.1983.01790060110016
16. Gauchard G, Jeandel C, Perrin P (2001) Physical and sporting activities improve vestibular afferent usage and balance in elderly human subjects. Gerontology 47(5):263–270
17. Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson LM, Lamb SE (2012) Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev 12(9)
18. Hauer K, Schwenk M, Zieschang T, Essig M, Becker C, Oster P (2012) Physical training improves motor performance in people with dementia: a randomized controlled trial. J Am Geriatr Soc 60(1):8–15 19. Heyn P, Abreu BC, Ottenbacher KJ (2004) The effects of exercise training on elderly persons with cognitive impairment and demen-tia: a meta-analysis. Arch Phys Med Rehabil 85(10):1694–1704 20. Hirvensalo M, Rantanen T, Heikkinen E (2000) Mobility
difficul-ties and physical activity as predictors of mortality and loss of independence in the community-living older population. J Am Geriatr Soc 48(5):493–498
21. Hunter GR, McCarthy JP, Bamman MM (2004) Effects of resis-tance training on older adults. Sports Med 34(5):329–348 22. Huxham FE, Goldie PA, Patla AE (2001) Theoretical
consider-ations in balance assessment. Aust J Physiother 47(2):89–100 23. Jacobson BH, Thompson B, Wallace T, Brown L, Rial C
(2011) Independent static balance training contributes to in-creased stability and functional capacity in community-dwelling elderly people: a randomized controlled trial. Clin Rehabil 25(6):549–556
24. Kauranen K (1999) Human motor performance and physiotherapy. Effect of strapping, hot and cold pack treatments and muscle strength training. University of Oulu, Finland
25. Kim S, Lockhart T (2012) Lower limb control and mobility fol-lowing exercise training. J Neuroeng Rehabil 9:15
26. Kondraske GV (1991) HPM/BEP manual. Human Performance Measurement, Inc, Arlington
27. Lihavainen K, Sipilä S, Rantanen T, Sihvonen S, Sulkava R, Hartikainen S (2010) Contribution of musculoskeletal pain to postural balance in community-dwelling people aged 75 years and older. J Gerontol A: Biol Sci Med Sci 65A(9):990–996 28. Liu-Ambrose T, Khan KM, Eng JJ, Janssen PA, Lord SR, McKay
HA (2004) Resistance and agility training reduce fall risk in women aged 75 to 85 with low bone mass: a 6- month randomized, controlled trial. J Am Geriatr Soc 52(5):657–665
29. Maggio D, Ercolani S, Andreani S, Ruggiero C, Mariani E, Mangialasche F, Palmari N, Mecocci P (2010) Emotional and psychological distress of persons involved in the care of patients with Alzheimer disease predicts falls and fractures in their care recipients. Dement Geriatr Cogn Disord 30(1):33–38
30. Mobasheri A (2011) Applications of proteomics to osteoarthritis, a musculoskeletal disease characterized by aging. Front Physiol 2:108 31. Muir SW, Gopaul K, Montero Odasso MM (2012) The role of cognitive impairment in fall risk among older adults: a systematic review and meta-analysis. Age Ageing 41(3):299–308
32. Nagai K, Inoue T, Yamada Y, Tateuchi H, Ikezoe T, Ichihashi N, Tsuboyama T (2011) Effects of toe and ankle training in older people: a cross-over study. Geriatr Gerontol Int 11(3):246–255 33. Nitz JC, Choy NL (2004) The efficacy of a specific balance-strategy
training programme for preventing falls among older people: a pilot randomized controlled trial. Age Ageing 33(1):52–58
34. Podewils LJ, Guallar E, Kuller LH, Fried LP, Lopez OL, Carlson M, Lyketsos CG (2005) Physical activity, APOE genotype, and dementia risk: findings from the Cardiovascular Health Cognition Study. Am J Epidemiol 161(7):639–651
35. Sato D, Kaneda K, Wakabayashi H, Shimoyama Y, Baba Y, Nomura T (2011) Comparison of once and twice weekly water exercise on various bodily functions in community-dwelling frail elderly requir-ing nursrequir-ing care. Arch Gerontol Geriatr 52(3):331–335
36. Schleicher MM, Wedam L, Wu G (2012) Review of Tai Chi as an effective exercise on falls prevention in elderly. Res Sports Med 20(1):37–58
37. Schmidt RA, Lee TD (2011) Motor control and learning. A be-havioral emphasis, 5th edn. Human Kinetics, Champaign 38. Schnelle JF, Alessi CA, Simmons SF, Al-Samarrai NR, Beck JC,
Ouslander JG (2002) Translating clinical research into practice: a randomized controlled trial of exercise and incontinence care with nursing home residents. J Am Geriatr Soc 50(9):1476–1483 39. Shumway-Cook A, Gruber W, Baldwin M, Liao S (1997) The
effect of multidimensional exercises on balance, mobility, and fall risk in community-dwelling older adults. Phys Ther 77(1):46–57 40. Shumway-Cook A, Woollacott MH (2007) Motor control—
translating research into clinical practice, 3rd edn. Lippincott Williams & Wilkins, Philadelphia
41. Shumway-Cook A, Woollacott MH (2007) Motor control: theory and practical applications, 3rd edn. Lippincott Williams & Wilkins, Baltimore
42. Sorace P (2010) Exercise recommendations for the frail popula-tion. In: Churilla JR, Sorace P (eds) American College of Sports Medicine, Certified News, vol 20. vol 1. Indianapolis, pp 3–4 43. Sumic A, Michael YL, Carlson NE, Howieson DB, Kaye JA
(2007) Physical activity and the risk of dementia in oldest old. J Aging Health 19(2):242–259
44. Teixeira MC, Teixeira LA (2008) Leg preference and interlateral performance asymmetry in soccer player children. Dev Psychobiol 50(8):799–806
45. Tinetti ME (1986) Performance-oriented assessment of mobility problems in elderly patients. J Am Geriatr Soc 34(2):119–126 46. Tinetti ME (2003) Clinical practice. Preventing falls in elderly
persons. N Engl J Med 348(1):42–49
47. Tsang W, Hui-Chan C (2004) Effects of exercise on joint sense and balance in elderly men: Tai Chi versus golf. Med Sci Sports Exerc 36(4):658–667
48. Turvey MT, Carello C (1996) Dynamics of Bernstein's level of synergies. In: Latash ML, Turvey MT (eds) Dexterity and its development. Lawrence Erlbaum, Mahwah
49. Woolf AD, Pfleger B (2003) Burden of major musculoskeletal conditions. Bull World Health Organ 81(9):646–656
50. Xu D, Hong Y, Li J, Chan K (2004) Effect of tai chi exercise on proprioception of ankle and knee joints in old people. Br J Sports Med 38(1):50–54