Multiple Courses of Antenatal Corticosteroids for
Preterm Birth Study: 2-Year Outcomes
WHAT’S KNOWN ON THIS SUBJECT: Recent trials of repeated courses of prenatal corticosteroid therapy showed some benefits but also raised concerns regarding potential harm. Long-term outcomes of these trials have shown no benefits in the neurodevelopmental status of the children.
WHAT THIS STUDY ADDS: This study was able to show that repeated courses of prenatal corticosteroid therapy did not contribute to improved outcomes. Although growth parameters at birth were significantly different with repeated courses, there was no significant difference at 2 years of age.
abstract
OBJECTIVE:The aim of this study was to determine the effects of re-peated courses of prenatal corticosteroid therapy versus placebo on death or neurologic impairment among the children enrolled in the Multiple Courses of Antenatal Corticosteroids for Preterm Birth Study, at 18 to 24 months of age.
METHODS:A total of 2305 infants were eligible for follow-up evaluation; 2104 infants (1069 in the prenatal corticosteroid therapy group and 1035 in the placebo group) were monitored. The primary outcome was death or neurologic impairment, defined as either cerebral palsy or cog-nitive delay, at 18 to 24 months of age. The secondary outcomes were measurements of growth (height, weight, and head circumference).
RESULTS:Children exposed to multiple courses of prenatal corticoste-roid therapy had similar rates of death or neurologic impairment, compared with children exposed to placebo (148 children [13.8%] vs 142 children [13.7%]; odds ratio: 1.001[95% confidence interval: 0.75– 1.30];P⫽.95). They had a mean weight of 11.94 kg, compared with 12.14 kg in the placebo group (P⫽.04), a mean height of 85.51 cm, compared with 85.46 cm (P⫽.87), and a mean head circumference of 48.18 cm, compared with 48.25 cm (P⫽.45).
CONCLUSIONS:Multiple courses of prenatal corticosteroid therapy, given every 14 days, did not increase or decrease the risk of death or neurologic impairment at 18 to 24 months of age, compared with a single course of prenatal corticosteroid therapy. Continued follow-up monitoring of these children is necessary to assess neurobehavioral function, school performance, and possible susceptibility to disease.
Pediatrics2010;126:e1045–e1055
AUTHORS:Elizabeth V. Asztalos, MD,aKellie E. Murphy, MD,bMary E. Hannah, MDCM,cAndrew R. Willan, PhD,d Stephen G. Matthews, PhD,e,f,gArne Ohlsson, MD,h Edmond N. Kelly, MB,hSaroj Saigal, MD,iSusan Ross, PhD,j Marie-France Delisle, MD,kKofi Amankwah, MD,lPatricia Guselle, MSc,mAmiram Gafni, DSc,nShoo K. Lee, MBBS,e,f,g B. Anthony Armson, MD,oRenee Sananes, PhD,pand Laura Tomat, MSc,mfor the Multiple Courses of Antenatal Corticosteroids for Preterm Birth Study Collaborative Group
Departments ofaNewborn and Developmental Paediatrics and cObstetrics and Gynaecology andmCentre for Mother, Infant, and Child Research, Sunnybrook Research Institute, Sunnybrook Health Sciences Centre, Departments ofbObstetrics and Gynaecology and hPaediatrics, Mount Sinai Hospital,dProgram in Child Health Evaluative Sciences, SickKids Research Institute, Dalla Lana School of Public Health, and Departments ofePhysiology,fObstetrics and Gynecology, andgMedicine, Faculty of Medicine, University of Toronto, Toronto, Canada;iDepartment of Pediatrics, McMaster University Medical Centre, andnDepartment of Clinical Epidemiology and Biostatistics, Centre for Health Economics and Policy Analysis, McMaster University, Hamilton, Canada; jDepartment of Obstetrics and Gynaecology, Faculty of Medicine, University of Calgary, Calgary, Canada;kDepartment of Obstetrics and Gynaecology, British Columbia Women’s Hospital, University of British Columbia, Vancouver, Canada;lDepartment of Gynecology-Obstetrics, Women’s and Children’s Hospital, State University of New York at Buffalo, Buffalo, New York;oDepartment of Obstetrics and Gynaecology, Izaak Walton Killan Health Centre, Dalhousie University, Halifax, Canada; andpDepartment of Psychology, Hospital for Sick Children, Toronto, Canada
KEY WORDS
prenatal corticosteroid therapy, repeated courses, neurodevelopmental outcomes
ABBREVIATIONS
MACS—Multiple Courses of Antenatal Corticosteroids for Preterm Birth Study
BSID-II—Bayley Scales of Infant Development II
This trial has been registered at www.clinicaltrials.gov (identifier NCT 00187382) and the International Standard Randomised Controlled Trial Number Register (identifier 2654148).
www.pediatrics.org/cgi/doi/10.1542/peds.2010-0857
doi:10.1542/peds.2010-0857
Accepted for publication Jul 23, 2010
Address correspondence to Elizabeth Vagi Asztalos, MD, Centre for Mother, Infant, and Child Research, Sunnybrook Health Sciences Centre, M4-233 2075 Bayview Ave Toronto, Ontario, M4N 3M5, Canada. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2010 by the American Academy of Pediatrics
Preterm birth continues to be a major health problem throughout the world.1 Infants born preterm are at increased risk of death and neonatal morbidities such as respiratory distress syn-drome, intraventricular hemorrhage,
and bronchopulmonary dysplasia,
which, in turn, increase the risk of abnormal neurodevelopmental out-comes in later life. The greatest benefit of a single course of prenatal cortico-steroid therapy is the acceleration of fetal lung maturity for women at high risk of preterm birth.2Since the early 1990s, it has been recommended that women who are between 24 and 34 weeks of gestation and at high risk of preterm birth receive a single course of prenatal corticosteroid therapy.3,4 However,⬃50% of women given a first course of prenatal corticosteroid ther-apy remain pregnant 7 to 14 days later; for these women, the question of whether repeated courses of prenatal corticosteroid therapy should be given has been raised.5The Multiple Courses of Antenatal Corticosteroids for Pre-term Birth Study (MACS) was a multi-center, international, randomized, double-blind, placebo-controlled trial with 1858 women who were at high risk of preterm birth and remained pregnant 14 to 21 days after an initial course of prenatal corticosteroid ther-apy. A course of prenatal corticoste-roid therapy was repeated every 14 days until week 33 or delivery, which-ever came first. The initial results, which were published previously,6 demonstrated no decrease in perina-tal or neonaperina-tal morperina-tality rates or neo-natal morbidity rates but indicated lower birth weights, smaller head circumferences, and shorter birth lengths with repeated courses of pre-natal corticosteroid therapy. Results of smaller trials of repeated courses of prenatal corticosteroid therapy sug-gested that repeated doses of prenatal corticosteroid therapy might be asso-ciated with reductions in the
occur-rence and severity of neonatal lung disease.7 Follow-up monitoring of the children in these trials is important, because studies of the use of postnatal corticosteroid therapy have shown that short-term benefits, in terms of less need for ventilatory support, can be offset by long-term problems, such as a higher risk of cerebral palsy.8The goal of the MACS 2-year follow-up study was to determine the effects of re-peated courses of prenatal corticoste-roid therapy versus placebo on death or neurologic impairment among chil-dren enrolled in the MACS at 18 to 24 months of age.
METHODS
Population
Women were enrolled in the MACS if they were between 25 and 32 weeks of gestation, remained pregnant 14 to 21 days after an initial course of prenatal corticosteroid (either betamethasone or dexamethasone) therapy, and con-tinued to be at high risk of preterm birth. Women were not eligible if they had a contraindication to corticoste-roid use, needed chronic treatment with these drugs, demonstrated evi-dence of chorioamnionitis, carried a fetus with a known lethal congenital anomaly, had received an initial course of prenatal corticosteroid ther-apy before 23 weeks of gestation, or had participated previously in the MACS. In multiple-fetus pregnancy, if a fetus was thought to have died prior to 13 weeks, that fetus was not consid-ered part of the pregnancy for the pur-poses of this study. Enrollment of these mothers took place between April 2001 and August 2006. The re-search ethics committees of all partici-pating centers approved the protocol, and women gave informed consent for the original study and for follow-up mon-itoring of the children before enrollment. All children of the enrolled women were included in the follow-up study.
Intervention
Randomization was performed by us-ing a centrally controlled, computer-ized, telephone randomization service at the data coordinating center, with stratification according to center and gestational age. Consenting women were assigned randomly to either the prenatal corticosteroid therapy group or the placebo treatment group. Women assigned to the prenatal corticosteroid therapy group received 2 doses of 12 mg of betamethasone administered intra-muscularly, 24 hours apart. Women as-signed to the placebo group received a similar-appearing injection. If the women continued to be at risk of pre-term birth after the initial course of the study drug, then courses were repeated every 2 weeks until 33 weeks of gestation or birth, whichever occurred first. For women who experienced preterm rup-ture of membranes, the recommenda-tion was that investigators would discon-tinue administration of the study medication at 32 weeks of gestation. All children who were alive at the time of the follow-up evaluation underwent stan-dardized neurologic assessments for de-termination of the presence of cerebral palsy and assessments with the Bayley Scales of Infant Development II (BSID-II)9 or other standardized tests for assess-ment of cognitive delays at 18 to 24 months of age.
Primary Outcomes for Follow-up Study
function was further classified by us-ing the criteria defined in the Gross Motor Function Classification Sys-tem.10A score of 0 was assigned if the child was able to walk independently, whereas scores of 3 to 5 (the highest score) indicated more-serious limita-tions of gross motor function.
Cognitive delays were defined as Mental Developmental Index scores of⬍70 (⬎2 SDs below the mean of 100) on the BSID-II or equivalent scores on another stan-dardized assessment. If a child could not be tested because of severe motor or de-velopmental delay, then the score was assumed to be⬍70. Personnel for the neurodevelopmental assessments in-cluded neonatologists, general pediatri-cians, developmental pediatripediatri-cians, and trained nurses who were experienced in performing neurodevelopmental exami-nations for follow-up programs, develop-ment assessdevelop-ment centers, and/or treat-ment centers for disabilities. The BSID-II was administered by individuals who had been trained specifically in adminis-tration of the test. Although follow-up evaluations were targeted for the ages of 18 to 24 months, efforts to conduct the assessments beyond 24 months were encouraged when necessary.
Other Outcomes
Anthropometric measurements (weight, height, and head circumference) were recorded and individual percentiles were computed in the data center, ac-cording to the corrected age at the time of assessment.11Information on general health, illnesses, and operations occur-ring after the primary hospitalization was recorded. In addition to the Mental Developmental Index, the Psychomotor Developmental Index and the Behavior Rat-ing Scale of the BSID-II were completed.
Statistical Analyses
The sample size for the MACS was calcu-lated to be 1900 women (950 per group). The power for the 2-year analysis was
calculated to be⬎90% for detection of an increase in the incidence of neuro-logic impairment from 5% to 9% (2-tailed
␣error of .05), if such an effect existed. This calculation was based on the as-sumption that the rate of cerebral palsy in the placebo group would be⬃5%.
The analysis was based on an
“intention-to-treat” approach. Descrip-tive statistics were used to check for any major dissimilarities in the study groups with respect to maternal de-mographic features, prognostic fac-tors, and other baseline information.
A logistic regression model, with ran-dom effect for multiple-fetus pregnan-cies to adjust for the dependence of ob-servations within the pregnancy, was used to calculate the adjusted odds ratio and 95% confidence intervals for com-parisons of the children in the 2 groups with respect to all outcomes. The level for declaring statistical significance for the primary outcome wasP⬍.05, using
a 2-tailed test, and that for all other out-comes wasP⬍.01.
Subgroup analyses were performed by including interaction terms for type of pregnancy (single versus multiple), ges-tational age at randomization, and pre-term prelabor rupture of membranes at randomization, for the primary outcome of the follow-up study. Although it was not planned a priori, the proportion of the primary outcome was calculated for the 2 treatment groups for infants born at ⱕ32 weeks of gestation and those born within 7 days after repeated study drug administration. The same sub-group analyses were performed for the primary neonatal outcome of the origi-nal MACS.6
RESULTS
Study Participants
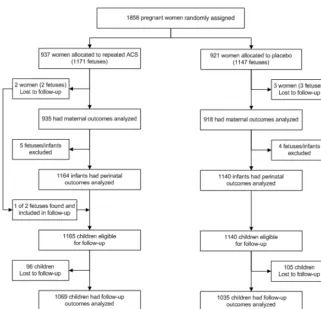
Figure 1 outlines the trial profile. In to-tal, 1858 women were enrolled in the MACS, with 2304 infants (1164 infants
FIGURE 1
in the prenatal corticosteroid therapy group and 1140 infants in the placebo group) contributing to the primary outcome initially reported.6One infant who was lost to follow-up monitoring for the primary report of the MACS was subsequently found. For the 2-year follow-up study, 201 additional infants (96 in the prenatal corticosteroid
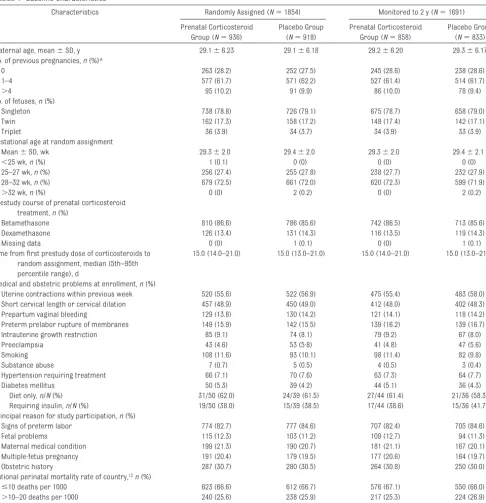
ther-apy group and 105 in the placebo group) were lost to follow-up monitor-ing, which left 2104 infants (91.3%) contributing to the primary outcome of the 2-year follow-up study, 1069 in the prenatal corticosteroid therapy group and 1035 in the placebo group. The baseline maternal characteristics were similar in the 2 groups (Table 1).
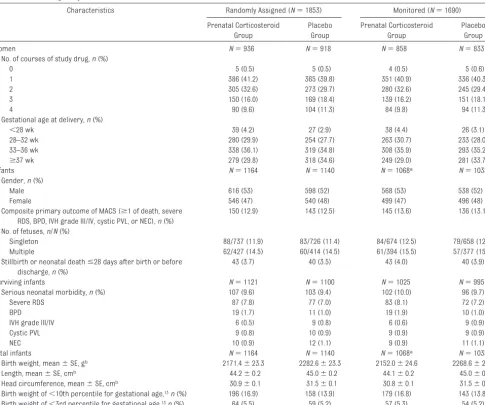
The early neonatal outcomes for the MACS for the infants included in the 2-year follow-up study are consistent with the results of the primary report (Table 2).
Follow-up Procedures
Of the surviving infants (N⫽2008), all underwent a neurodevelopmental
clin-TABLE 1 Baseline Characteristics
Characteristics Randomly Assigned (N⫽1854) Monitored to 2 y (N⫽1691)
Prenatal Corticosteroid Group (N⫽936)
Placebo Group (N⫽918)
Prenatal Corticosteroid Group (N⫽858)
Placebo Group (N⫽833)
Maternal age, mean⫾SD, y 29.1⫾6.23 29.1⫾6.18 29.2⫾6.20 29.3⫾6.17 No. of previous pregnancies,n(%)a
0 263 (28.2) 252 (27.5) 245 (28.6) 238 (28.6)
1–4 577 (61.7) 571 (62.2) 527 (61.4) 514 (61.7)
⬎4 95 (10.2) 91 (9.9) 86 (10.0) 78 (9.4)
No. of fetuses,n(%)
Singleton 738 (78.8) 726 (79.1) 675 (78.7) 658 (79.0)
Twin 162 (17.3) 158 (17.2) 149 (17.4) 142 (17.1)
Triplet 36 (3.9) 34 (3.7) 34 (3.9) 33 (3.9)
Gestational age at random assignment
Mean⫾SD, wk 29.3⫾2.0 29.4⫾2.0 29.3⫾2.0 29.4⫾2.1
⬍25 wk,n(%) 1 (0.1) 0 (0) 0 (0) 0 (0)
25–27 wk,n(%) 256 (27.4) 255 (27.8) 238 (27.7) 232 (27.9)
28–32 wk,n(%) 679 (72.5) 661 (72.0) 620 (72.3) 599 (71.9)
⬎32 wk,n(%) 0 (0) 2 (0.2) 0 (0) 2 (0.2)
Prestudy course of prenatal corticosteroid treatment,n(%)
Betamethasone 810 (86.6) 786 (85.6) 742 (86.5) 713 (85.6)
Dexamethasone 126 (13.4) 131 (14.3) 116 (13.5) 119 (14.3)
Missing data 0 (0) 1 (0.1) 0 (0) 1 (0.1)
Time from first prestudy dose of corticosteroids to random assignment, median (5th–95th percentile range), d
15.0 (14.0–21.0) 15.0 (13.0–21.0) 15.0 (14.0–21.0) 15.0 (13.0–21.0)
Medical and obstetric problems at enrollment,n(%)
Uterine contractions within previous week 520 (55.6) 522 (56.9) 475 (55.4) 483 (58.0) Short cervical length or cervical dilation 457 (48.9) 450 (49.0) 412 (48.0) 402 (48.3)
Prepartum vaginal bleeding 129 (13.8) 130 (14.2) 121 (14.1) 118 (14.2)
Preterm prelabor rupture of membranes 149 (15.9) 142 (15.5) 139 (16.2) 139 (16.7)
Intrauterine growth restriction 85 (9.1) 74 (8.1) 79 (9.2) 67 (8.0)
Preeclampsia 43 (4.6) 53 (5·8) 41 (4.8) 47 (5.6)
Smoking 108 (11.6) 93 (10.1) 98 (11.4) 82 (9.8)
Substance abuse 7 (0.7) 5 (0.5) 4 (0.5) 3 (0.4)
Hypertension requiring treatment 66 (7.1) 70 (7.6) 63 (7.3) 64 (7.7)
Diabetes mellitus 50 (5.3) 39 (4.2) 44 (5.1) 36 (4.3)
Diet only,n/N(%) 31/50 (62.0) 24/39 (61.5) 27/44 (61.4) 21/36 (58.3)
Requiring insulin,n/N(%) 19/50 (38.0) 15/39 (38.5) 17/44 (38.6) 15/36 (41.7) Principal reason for study participation,n(%)
Signs of preterm labor 774 (82.7) 777 (84.6) 707 (82.4) 705 (84.6)
Fetal problems 115 (12.3) 103 (11.2) 109 (12.7) 94 (11.3)
Maternal medical condition 199 (21.3) 190 (20.7) 181 (21.1) 167 (20.1)
Multiple-fetus pregnancy 191 (20.4) 179 (19.5) 177 (20.6) 164 (19.7)
Obstetric history 287 (30.7) 280 (30.5) 264 (30.8) 250 (30.0)
National perinatal mortality rate of country,12n(%)
ⱕ10 deaths per 1000 623 (66.6) 612 (66.7) 576 (67.1) 550 (66.0)
⬎10–20 deaths per 1000 240 (25.6) 238 (25.9) 217 (25.3) 224 (26.9)
⬎20 deaths per 1000 73 (7.8) 68 (7.4) 65 (7.6) 59 (7.1)
ical assessment for cerebral palsy and 1901 (94.7%) underwent a standard-ized cognitive assessment. Of those who underwent a standardized cogni-tive assessment, 1852 (97.4%) were as-sessed by using the BSID-II (Table 3).The corrected median age for the clinical assessment and the BSID-II was 22 months for both groups. If an-other standardized cognitive assess-ment was used, then the corrected me-dian age was 23 months.
Primary Outcomes for 2-Year Follow-up Study
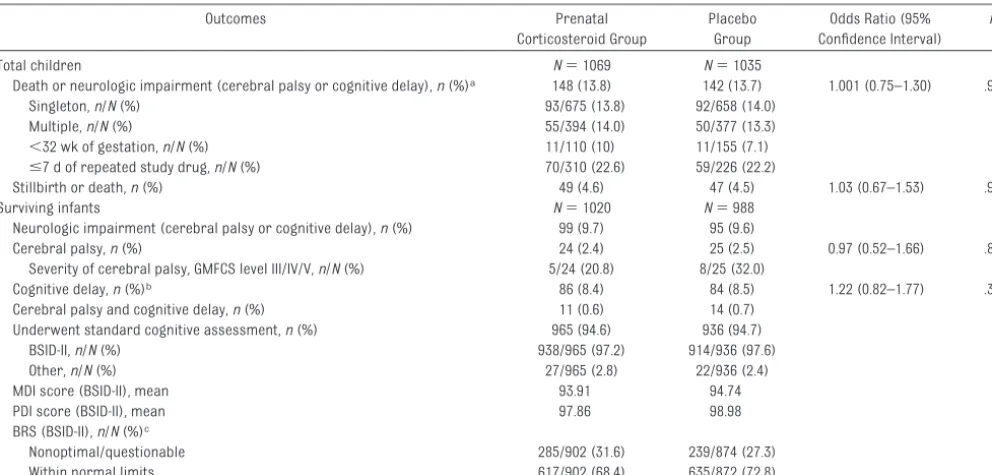
The results of the composite primary outcome and its components are shown in Table 3. There was no
statis-tically significant difference between the treatment groups in the risk of death or neurologic impairment at a corrected age of 18 to 24 months (148
[13.8%] of 1069 children in the prena-tal corticosteroid therapy group vs 142
[13.7%] of 1035 children in the placebo group; odds ratio: 1.001 [95% confi-dence interval: 0.75–1.30]; P ⫽ .95). Only 49 children (2.4%), 24 in the pre-natal corticosteroid therapy group and 25 in the placebo group, had cere-bral palsy. Most cases of cerecere-bral palsy were mild, with only 5 of 24 chil-dren in the prenatal corticosteroid therapy group and 8 of 25 children in the placebo group having gross motor function levels of III to V (Table 3). A TABLE 2 Initial Pregnancy and Neonatal Outcomes
Characteristics Randomly Assigned (N⫽1853) Monitored (N⫽1690)
Prenatal Corticosteroid Group
Placebo Group
Prenatal Corticosteroid Group
Placebo Group
Women N⫽936 N⫽918 N⫽858 N⫽833
No. of courses of study drug,n(%)
0 5 (0.5) 5 (0.5) 4 (0.5) 5 (0.6)
1 386 (41.2) 365 (39.8) 351 (40.9) 336 (40.3)
2 305 (32.6) 273 (29.7) 280 (32.6) 245 (29.4)
3 150 (16.0) 169 (18.4) 139 (16.2) 151 (18.1)
4 90 (9.6) 104 (11.3) 84 (9.8) 94 (11.3)
Gestational age at delivery,n(%)
⬍28 wk 39 (4.2) 27 (2.9) 38 (4.4) 26 (3.1)
28–32 wk 280 (29.9) 254 (27.7) 263 (30.7) 233 (28.0)
33–36 wk 338 (36.1) 319 (34.8) 308 (35.9) 293 (35.2)
ⱖ37 wk 279 (29.8) 318 (34.6) 249 (29.0) 281 (33.7)
Infants N⫽1164 N⫽1140 N⫽1068a N⫽1035
Gender,n(%)
Male 616 (53) 598 (52) 568 (53) 538 (52)
Female 546 (47) 540 (48) 499 (47) 496 (48)
Composite primary outcome of MACS (ⱖ1 of death, severe RDS, BPD, IVH grade III/IV, cystic PVL, or NEC),n(%)
150 (12.9) 143 (12.5) 145 (13.6) 136 (13.1)
No. of fetuses,n/N(%)
Singleton 88/737 (11.9) 83/726 (11.4) 84/674 (12.5) 79/658 (12.0)
Multiple 62/427 (14.5) 60/414 (14.5) 61/394 (15.5) 57/377 (15.1)
Stillbirth or neonatal deathⱕ28 days after birth or before discharge,n(%)
43 (3.7) 40 (3.5) 43 (4.0) 40 (3.9)
Surviving infants N⫽1121 N⫽1100 N⫽1025 N⫽995
Serious neonatal morbidity,n(%) 107 (9.6) 103 (9.4) 102 (10.0) 96 (9.7)
Severe RDS 87 (7.8) 77 (7.0) 83 (8.1) 72 (7.2)
BPD 19 (1.7) 11 (1.0) 19 (1.9) 10 (1.0)
IVH grade III/IV 6 (0.5) 9 (0.8) 6 (0.6) 9 (0.9)
Cystic PVL 9 (0.8) 10 (0.9) 9 (0.9) 9 (0.9)
NEC 10 (0.9) 12 (1.1) 9 (0.9) 11 (1.1)
Total infants N⫽1164 N⫽1140 N⫽1068a N⫽1035
Birth weight, mean⫾SE, gb 2171.4⫾23.3 2282.6⫾23.3 2152.0⫾24.6 2268.6⫾24.5
Length, mean⫾SE, cmb 44.2⫾0.2 45.0⫾0.2 44.1⫾0.2 45.0⫾0.2
Head circumference, mean⫾SE, cmb 30.9⫾0.1 31.5⫾0.1 30.8⫾0.1 31.5⫾0.1
Birth weight of⬍10th percentile for gestational age,13n(%) 196 (16.9) 158 (13.9) 179 (16.8) 143 (13.8)
Birth weight of⬍3rd percentile for gestational age,13n(%) 64 (5.5) 59 (5.2) 57 (5.3) 54 (5.2)
RDS indicates respiratory distress syndrome, defined as requiring assisted ventilation through an endotracheal tube and supplemental oxygen therapy, both within the first 24 hours of life and for a duration ofⱖ24 hours, and either a radiograph consistent with respiratory distress syndrome or surfactant given between the first 2 and 24 hours of life; BPD, bronchopulmonary dysplasia, defined as requiring supplemental oxygen therapy at a postnatal gestational age of 36 completed weeks and a radiograph consistent with bronchopulmonary dysplasia; IVH, intraventricular hemorrhage; PVL, periventricular leukomalacia, defined as periventricular cystic changes in the cranial white matter, excluding subependymal and choroid plexus cysts; NEC, necrotizing enterocolitis, defined as either perforation of the intestine, pneumatosis intestinalis, or air in the portal vein.
similar pattern was noted in the inci-dence of cognitive delays (8.4% in the prenatal corticosteroid therapy group, compared with 8.5% in the placebo group). The numbers of children with both cerebral palsy and cognitive de-lays were similar between the groups.
There were no significant interactions between treatment groups and the baseline variables of type of preg-nancy (single versus multiple), gesta-tional age at randomization, and pre-term prelabor rupture of membranes at randomization, which indicates that the proportions of the primary out-come were similar between the treat-ment groups for subgroups defined on the basis of these baseline variables. Rates of the primary outcome for the follow-up study were similar between groups for children who were born be-fore 32 weeks (11 [10%] of 110 chil-dren in the prenatal corticosteroid therapy group and 11 [7.1%] of 155 children in the placebo group) and for those born within 7 days after re-peated study drug administration (70
[22.6%] of 310 children in the prenatal corticosteroid therapy group and 59 [22.2%] of 266 children in the placebo group).
For children who were assessed with the BSID-II as the standardized mea-sure of cognition, the mean Mental De-velopmental Index scores were 93.91 and 94.74 and the Psychomotor Devel-opmental Index scores were 97.86 and 98.98 for the prenatal corticosteroid therapy and placebo groups, respec-tively. The Behavior Rating Scale re-sults were nonoptimal or questionable for 285 (31.6%) of 902 children in the prenatal corticosteroid therapy group and 239 (27.3%) of 874 children in the placebo group (Table 4).
Other Outcomes
The mean height, weight, and head cir-cumference for children who were
ex-posed to repeated courses of prenatal corticosteroid therapy were not signif-icantly different from those for chil-dren who were exposed to a single
course (Table 4). Children in the prena-tal corticosteroid therapy group had a mean weight of 11.94 kg, compared with 12.14 kg in the placebo group
(P⫽.04); mean heights were 85.46 cm for the prenatal corticosteroid therapy group and 85.51 cm for the placebo group (P⫽.87), and mean head cir-cumferences were 48.18 cm for the prenatal corticosteroid therapy group
TABLE 4 Growth Measurements
Mean Difference, Mean (95% Confidence Interval)
P
Prenatal Corticosteroid Group (N⫽1020)
Placebo Group (N⫽988)
Height, cm 85.46 85.51 ⫺0.04846 (⫺0.6162 to 0.5271) .87 Weight, kg 11.94 12.14 ⫺0.1934 (⫺0.3812 to 0.0057) .04 Head circumference, cm 48.18 48.25 ⫺0.0723 (⫺0.2589 to 0.1156) .45
Values are adjusted. TABLE 3 Primary Outcomes for Follow-up Period
Outcomes Prenatal
Corticosteroid Group
Placebo Group
Odds Ratio (95% Confidence Interval)
P
Total children N⫽1069 N⫽1035
Death or neurologic impairment (cerebral palsy or cognitive delay),n(%)a 148 (13.8) 142 (13.7) 1.001 (0.75–1.30) .95
Singleton,n/N(%) 93/675 (13.8) 92/658 (14.0)
Multiple,n/N(%) 55/394 (14.0) 50/377 (13.3)
⬍32 wk of gestation,n/N(%) 11/110 (10) 11/155 (7.1)
ⱕ7 d of repeated study drug,n/N(%) 70/310 (22.6) 59/226 (22.2)
Stillbirth or death,n(%) 49 (4.6) 47 (4.5) 1.03 (0.67–1.53) .97
Surviving infants N⫽1020 N⫽988
Neurologic impairment (cerebral palsy or cognitive delay),n(%) 99 (9.7) 95 (9.6)
Cerebral palsy,n(%) 24 (2.4) 25 (2.5) 0.97 (0.52–1.66) .82
Severity of cerebral palsy, GMFCS level III/IV/V,n/N(%) 5/24 (20.8) 8/25 (32.0)
Cognitive delay,n(%)b 86 (8.4) 84 (8.5) 1.22 (0.82–1.77) .35
Cerebral palsy and cognitive delay,n(%) 11 (0.6) 14 (0.7) Underwent standard cognitive assessment,n(%) 965 (94.6) 936 (94.7)
BSID-II,n/N(%) 938/965 (97.2) 914/936 (97.6)
Other,n/N(%) 27/965 (2.8) 22/936 (2.4)
MDI score (BSID-II), mean 93.91 94.74
PDI score (BSID-II), mean 97.86 98.98
BRS (BSID-II),n/N(%)c
Nonoptimal/questionable 285/902 (31.6) 239/874 (27.3)
Within normal limits 617/902 (68.4) 635/872 (72.8)
MDI indicates Mental Developmental Index; PDI, Psychomotor Developmental Index; BRS, Behavior Rating Scale; GMFCS, Gross Motor Functional Classification System.
aComposite outcome.
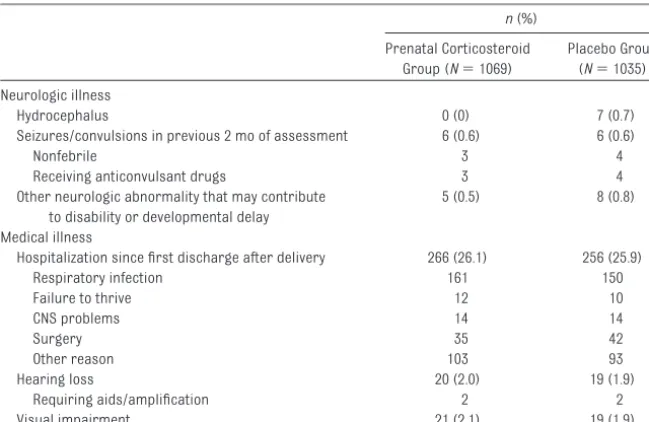
and 48.25 cm for the placebo group (P⫽.45). Rates of readmission to the hospital and reports of other health is-sues are presented in Table 5.
DISCUSSION
Earlier trials of repeated courses of prenatal corticosteroid therapy found some evidence for short-term benefits with respect to the risk of neonatal re-spiratory disease.7,14 The MACS re-ported that multiple courses of prena-tal corticosteroid therapy, given every 14 days, were associated with no neo-natal benefits and reduced size at birth, compared with a single course of prenatal corticosteroid therapy.6 Therefore, the evidence for short-term neonatal benefits is mixed. This follow-up study of children in the MACS found no significant difference in sur-vival rates or the presence of neuro-logic impairment at 18 to 24 months of age with multiple courses of prenatal corticosteroid therapy.
On the basis of the initial results of the MACS, repeated courses of prenatal corticosteroid therapy are not recom-mended. However, for clinicians rec-ommending repeated courses of pre-natal corticosteroid therapy as part of
routine care, on the basis of earlier tri-als showing short-term benefits, the main issue is the need for confidence that the increased exposure to ste-roids is not associated with long-term harm, because most randomized con-trolled trials are underpowered to as-sess long-term benefits. At the initia-tion of this trial in 2001, there was limited information regarding the long-term effects of exposure to multi-ple courses of prenatal corticosteroid therapy.15 However, the earlier trials with multiple courses of prenatal cor-ticosteroid therapy have now reported 2-year outcomes.16–18 All reported no significant differences in rates of death or major neurodevelopmental difficulties at 2 years of age. One study did note a nonsignificant increase in cerebral palsy in the group exposed to more courses of prenatal corticoste-roid therapy, but this was not ob-served in the other studies.17The fact that our study is able to report no sig-nificant increase in rates of death or major neurologic impairment at 2 years of age is reassuring. Caution must be exercised, however, because measurements at 2 years of age have limited predictive abilities and are only
moderately correlated with develop-mental outcomes at later ages.19
Animal studies suggested that re-peated exposure to prenatal cortico-steroid therapy might have neurologic
consequences. Investigators who fo-cused on brain development noted a decrease in growth of all brain struc-tures, including a reduced number of
neurons and degeneration of neurons in the hippocampus with exposure to prenatal corticosteroid therapy.20,21 Within the developing brain, the limbic system (in particular, the
hippocam-pus) is sensitive to both endogenous and exogenous glucocorticoids. The hippocampus has a myriad of func-tions that support cognition, memory, and behavior. There has been some
suggestion that repeated courses of prenatal corticosteroid therapy may result in adverse behavior changes in children. French et al22noted, in a
co-hort study of children at 3 and 6 years of age, that increasing courses of pre-natal corticosteroid therapy were as-sociated with a lower risk of cerebral palsy, with no differences in
intellec-tual ability, all disabilities, and median IQ scores. Behavioral abnormalities in-creased with additional courses of corticosteroids, however, with aggres-sive, destructive, and hyperkinetic
be-havior among infants who receivedⱖ3 courses. Crowther et al16 did not ob-serve an increase in aggressive behav-ior but did note that a slightly greater
proportion of children who were ex-posed to repeated courses of prenatal corticosteroid therapy had scores for attention problems. We did not ob-serve a difference in behavior between
the 2 groups by using the Behavior Rat-ing Scales; however, this assessment is less sensitive than the Child Behav-ior Checklist and reflects only the ob-servation of the assessor during the
assessment of the child.9,23 In both studies, the children were young, and TABLE 5 Neurologic and Medical Illnesses
n(%)
Prenatal Corticosteroid Group (N⫽1069)
Placebo Group (N⫽1035)
Neurologic illness
Hydrocephalus 0 (0) 7 (0.7)
Seizures/convulsions in previous 2 mo of assessment 6 (0.6) 6 (0.6)
Nonfebrile 3 4
Receiving anticonvulsant drugs 3 4
Other neurologic abnormality that may contribute to disability or developmental delay
5 (0.5) 8 (0.8)
Medical illness
Hospitalization since first discharge after delivery 266 (26.1) 256 (25.9)
Respiratory infection 161 150
Failure to thrive 12 10
CNS problems 14 14
Surgery 35 42
Other reason 103 93
Hearing loss 20 (2.0) 19 (1.9)
Requiring aids/amplification 2 2
Visual impairment 21 (2.1) 19 (1.9)
it is possible that behavior changes are not as evident in younger children.
Our earlier report showed a significant difference in body size at birth be-tween the 2 groups.6This was not ob-served at 18 to 24 months of age. Al-though the children in the prenatal corticosteroid therapy group were slightly smaller (by 200 g), the effect was less significant than that noted at birth. This may suggest a transient ef-fect of repeated courses of prenatal corticosteroid therapy on growth and may indicate that children can com-pensate and “catch up” in the first 2 years of life. Whether this has any clin-ically important effect on size and gen-eral health in later childhood and adult life is not clear.24Human epidemiolog-ical studies suggest that catch-up growth may contribute to health is-sues in later life.24,25
Over the past decade, there has been intense work in the field of develop-mental origins of health and disease. It is now solidly established that stimuli experienced during critical periods of prenatal and postnatal development can influence developmental pathways and induce permanent changes in metabolism, cellular function, and chronic disease susceptibility.26 The term “metabolic imprinting” has been used to describe the adaptive changes that occur during periods of sensitiv-ity. Recent studies indicated that a number of permanent changes in physiologic function that result from modification of the perinatal environ-ment are mediated through epigenetic processes.27,28 Furthermore, it has been suggested that exposure of the fetus to increased levels of glucocorti-coids (endogenous and exogenous) may lead to modification of the fetal epigenome, which in turn leads to per-manent alterations in the expression of affected genes and their associated function.29,30 It also has been deter-mined that the effects of an altered
fe-tal environment may not manifest until later childhood, adolescence, or adult-hood. In the current study, children were monitored only to 2 years of age; however, this group is currently being monitored to 5 years, at which time a more-sophisticated analysis of neuro-development can be undertaken.
CONCLUSIONS
Multiple courses of prenatal cortico-steroid therapy, given every 14 days, do not increase or decrease the risk of death or neurologic impairment at 18 to 24 months of age, compared with a single course of prenatal corticoste-roid therapy. In our opinion, however, repeated courses of prenatal cortico-steroid therapy are not recommended for routine use, because of a lack of conclusive evidence of either short- or long-term benefits. There continues to be concern regarding the possibility of long-term harm, given the effects of re-peated courses on size and head circumference at birth. Continued follow-up monitoring of these children is necessary to answer questions re-garding neurobehavioral function and possible susceptibility to metabolic and cardiovascular disease.
ACKNOWLEDGMENTS
The MACS, including the follow-up phase, was funded by the Canadian Institutes of Health Research (grant 38142), which had no role in study design, manage-ment, data collection, analysis, or data interpretation. The Canadian Institutes of Health Research had no role in the writing of the manuscript or in the deci-sion to submit for publication.
The MACS Collaborative Group was as follows: Steering Committee: K. E. Mur-phy, K. Amankwah, B. A. A. Armson, E. V. Asztalos, M-F. Delisle, A. Gafni, P. Guselle, M. E. Hannah, E. N. Kelly, S. K. Lee, S. G. Matthews, A. Ohlsson, S. Ross, J. Rovet, S. Saigal, R. Sananes, I. Schmid, I. Schweitzer, L. Tomat, A. R.
Materno Infantil, Goiania (4 subjects recruited): Luiza Emylce Pela Rosado Schmaltz, Goianice Ribeiro de Souza Georgia Bueno; Maternidade Escola da Universidade Federal de Rio de Janeiro (Federal University of Rio de Janeiro), Rio de Janeiro (5 subjects recruited): Renato Augusto Moreira de Sa, Rita Guerios Bornia, Denise Sterit Morsch, Maria Amelia Sayeg Campos Porto; Canada: Royal Alexandra Hospital, Edmonton (46 subjects recruited): Nestor N. Demianczuk, Elizabeth Pen-tinnen, Jacqui Mackoway, Leonora Hendson, Jill Tomlinson; Dr Everett Chalmers Regional Hospital, Frederic-ton (7 subjects recruited): Kimberly Butt, Kathryn Hay, R. Krishnaswamy, Karen Ward; IWK Health Centre, Halifax (36 subjects recruited): B. Anthony Armson, Michael Vincer, Victoria Allen, Cora Fanning; North Bay General Hos-pital, North Bay (17 subjects
recruit-ed): Ramesh Kulkarni, Joanne
Laplante, Rhonda Scarfoni; Regina General Hospital, Regina (26 subjects recruited): George D. Carson, Suzanne Williams, Sandy Holfeld, Leanne Fon-taine, Jodie Bigalky; Royal University Hospital, Saskatoon (26 subjects re-cruited): Olufemi Olatunbosun, April Henry, Linda Erker, Neil Wonko, Janna Haughian, Shirley Dalton; Centre Hos-pitalier Universitaire de Sherbrooke (University Hospital Centre of Sher-brooke) Fleurimont, Sherbrooke (25
subjects recruited): Jean-Marie
Moutquin, Daniel Blouin, Suzanne Koc-sis Bédard, Emanuela Ferretti; Mount Sinai Hospital, Toronto (89 subjects re-cruited): Kellie Murphy, Arne Ohlsson, Edmond Kelly, Anne Jordan, Jodi Sha-piro, Renee Sananes, Laura Cooper, Alda Fernandes-Penny; Sunnybrook Health Sciences Centre, Toronto (20 subjects recruited): Elizabeth Asztalos, Denise Hohn, Maralyn Lacy; Children’s and Women’s Health Centre of British Columbia, Vancouver (22 subjects re-cruited): Marie-France Delisle, Anne
Synnes, Vesna Popovska, Shelly
Soanes, Agnes Sauter; St Boniface Gen-eral Hospital, Winnipeg (28 subjects re-cruited): Michael E. Helewa, Doris Kenny-Lodewyks, Diane Moddemann, Naomi Granke, Karen Penner; Chile: Hospital Dr Sotero del Rio, Puente Alto (92 subjects recruited): Ricardo Go-mez, Karla Silva Neculman, Juan An-dres Ortiz Castro, Manuel Schepeler Solari, Mario Alfredo Carstens Rojas; Hospital Clinico San Borja Arriaran, Santiago (23 subjects recruited): Jorge Figueroa Poblete, Patricia
Ur-rutia Gonzalez, Monica Troncoso
Schifferli, Lilian Saez Aguilera; Univer-sidad Catolica, Santiago (33 subjects recruited): Cristian Belmar, Rosario Moore, Claudio Vera, Javier Kattan; China: Peace Maternity, Shanghai (4 subjects recruited): Qi Feng Su, Wei Gu, Zhi Wei Liu; Colombia: Universidad del Norte, Barranquilla (6 subjects re-cruited): Martha Marrugo Flores, Car-los Malabet Santoro, Jaime Galindo López; Cemiya, Cali (85 subjects re-cruited): Edgar Ivan Ortiz, Javier Torres, Adriana Rodriguez Sanchez; Denmark: Aarhus University Hospital, Aarhus (35 subjects recruited): Lone Hvidman, Anne Mouritzen, Jennifer Vikre-Jørgensen, Marianne B. Chris-tiansen; Germany: Charite Universita-tsmedizin Berlin (CUB) Benjamin Franklin, Berlin (16 subjects recruited): Hartmut Hopp, Andreas Nonnenma-cher; Helios Klinikum, Erfurt (13 sub-jects recruited): Udo B. Hoyme, Hans-Jorg Bittrich, Britta Oletzky; Hannover Medical School, Hannover (1 subject recruited): Bettina Hollwitz, Katrin Oehler, Frank Dressler; University of Saarland, Homburg/Saar (5 subjects recruited): Juliane Meng-Hentschel; Universitatsklinikum Leipzig, Leipzig (5 subjects recruited): Renaldo Faber, Holger Stepan, Ferdinand Pulzer; Uni-versity Hospital Geissen and Marburg, Marburg (14 subjects recruited): Maritta Kuhnert, Susanne Stiller; Tech-nical University Munchen, Munich (3 subjects recruited): Bettina Kuschel,
K. T. M. Schneider, Andrea Zimmer-mann; Klinikum Nurnberg Sud, Nurn-berg (35 subjects recruited): Michael Krause, Jana Korausova; St Hedwig Hospital, Regensburg (7 subjects re-cruited): Birgit Seelbach-Goebel, Andreas Falkert; Dr Horst-Schmidt-Kliniken, Wiesbaden (5 subjects re-cruited): Karin Mueller, Hana Voss; Hungary: University of Debrecen, Deb-recen (45 subjects recruited): Tamas Major, Zoárd Krasznai, Tünde Bartha, Edit Polonkai, Judit Zsadányi; Israel: Haemek Medical Center, Afula (58 sub-jects recruited): Zohar Nachum, Clari Felszer; Soroka Medical Center, Beer
Sheva (15 subjects recruited):
Hospital Research, Lodz (66 subjects recruited): Jan Wilczynski, Michael Krekora, Marcin Kesiak, Ewa Gulczyn´-ska; University School of Medical Sci-ences, Poznan (108 subjects recruit-ed): Grzegorz H Breborowicz, Mateusz Madejczyk, Joanna Rozycka, Agnieszka Montgomery, Marta Szymankiewicz; Russia: Research Institute, Ivanovo (3 subjects recruited): Nadezhda Bor-zova, Lubov V. Posiseeva; Research Centre of Obstetrics, Gynecology, and Perinatology, Moscow (15 subjects re-cruited): Zulfiya S. Khodzhaeva, Ekat-erina M. Vikhlyaeva, Natalya V. Greben-nikova, Elena N. Baibarina; Spain: Hospital Clinic-University of Barcelona, Barcelona (21 subjects recruited): Montse Palacio, Francesc Botet, Teresa Cobo, Sonia Pisa, Dolors Salvia; Switzerland: University Women’s Hos-pital, Basel (14 subjects recruited):
Irene Hösli, Wolfgang Holzgreve, Cora A. Voekt; Centre Hospitalier Universita-ire (University Hospital Centre) Vau-dois, Lausanne (9 subjects recruited):
Margarita Forcada-Guex, Adrian
Moessinger, Myriam Bickle-Graz; Uni-versity Hospital, Zurich (4 subjects re-cruited): Ernst Beinder, Ursula von Mandach, Jean-Claude Fauchere; Neth-erlands: Atrium Medical Center, Heer-len (1 subject recruited): Frans J. M. E. Roumen, J. B. G. Wynands; Academisch Ziekenhuis Maastricht, Maastricht (8 subjects recruited): Antonio W. D. Gavilanes; United Kingdom: Diana, Princess of Wales Hospital, Grimsby (4 subjects recruited): Ibrahim I. Bolaji, Pauline Adiotomre; Queen Elizabeth Hospital, King’s Lynn (2 subjects re-cruited): Hamed Al-Taher, Hayley Bar-nes, Susan Rubin; Royal Free Hospital, London (2 subjects recruited): Rezan
Abdul-Kadir, Claudia Chi, Vivienne Van Someren; Montefiore Medical Center, Bronx (27 subjects recruited): Setul Pardanani, Michael Bebbington, Cyn-thia Chazotte; University of Illinois Med-ical Center at Chicago, Chicago (7 sub-jects recruited): Sarah Kilpatrick, Jessica L. Drahos; Baystate Health Sys-tem, Springfield (2 subjects recruited):
Fadi Bsat, Jennie Fleming, Alison Lee, Despina Hoffman; Data Safety Monitor-ing Board: M. Bracken (chair), P. Crow-ley, L. DuCrow-ley, R. Erenkranz, K. Thorpe.
We thank all of the participants in the MACS trial, the members of the Data Safety Monitoring Board for their guid-ance throughout the trial, and all of the staff members at the Centre for Mother, Infant, and Child Research (To-ronto, Canada) for their hard work and dedication.
REFERENCES
1. World Health Organization. The World Health Report 2005: Make Every Mother and Child Count. Geneva, Switzerland: World Health Organization; 2005. Available at: www.who.int/whr/2005/en/index.html. Ac-cessed March 1, 2010
2. Roberts D, Dalziel S. Antenatal corticoste-roids for accelerating fetal lung maturation for women at risk of preterm birth. Co-chrane Database Syst Rev. 2006;(3): CD004454
3. National Institute of Child Health and Human Development, Office of Medical Applications of Research.Report of the Consensus Develop-ment Conference on the Effect of Corticoste-roids for Fetal Maturation on Perinatal Out-comes. Bethesda, MD: National Institutes of Health; 1994. NIH publication V01.95–3784. Available at: www.nichd.nih.gov/publications/ pubs/corticosteroids/Corticosteroids. htmlXXX. Accessed September 30, 2005
4. Crane J, Armson A, Brunner M, et al. Ante-natal corticosteroid therapy for fetal matu-ration.J Obstet Gynaecol Can. 2003;25(1): 45–52
5. McLaughlin KJ, Crowther CA, Walker N, Har-ding JE. Effects of a single course of corti-costeroids given more than 7 days before birth: a systematic review.Aust N Z J Obstet Gynaecol. 2003;43(2):101–106
6. Murphy KE, Hannah ME, Willan AR, et al. Mul-tiple Courses of Antenatal Corticosteroids
for Preterm Birth (MACS): a randomised controlled trial. Lancet. 2008;372(9656): 2143–2151
7. Crowther C, Harding J. Repeat doses of pre-natal corticosteroids for women at risk of preterm birth for preventing neonatal re-spiratory disease.Cochrane Database Syst Rev. 2007;(3):CD003935
8. Halliday HL, Ehrenkranz RA, Doyle LW. Early (⬍8 days) postnatal corticosteroids for preventing chronic lung disease in preterm infants.Cochrane Database Syst Rev. 2009; (1):CD001146
9. Bayley N.Bayley Scales of Infant Develop-ment. 2nd ed. San Antonio, TX: Psychological Corp; 1993
10. Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reli-ability of a system to classify gross motor function in children with cerebral palsy.Dev Med Child Neurol. 1997;39(4):214 –223
11. World Health Organization. WHO child growth standards. Available at: www.who. int./childgrowth/standards/en/index.html. Accessed March 15, 2009
12. World Health Organization. Neonatal and Perinatal Mortality Country, Regional and Global Estimates. Geneva, Switzerland: World Health Organization; 2000. Available at: www.who.int/making_pregnancy_ safer/publications/neonatal.pdf. Accessed March 1, 2007
13. Kramer MS, Platt RW, Wen SW, et al. A new and improved population-based Canadian reference for birth weight for gestational age. Pediatrics. 2001;108(2). Available at: www.pediatrics.org/cgi/content/full/108/ 2/e35
14. McEvoy C, Bowling S, Williamson R, et al. The effect of a single remote course versus weekly courses of antenatal corticoste-roids on functional residual capacity in pre-term infants: a randomized trial.Pediatrics. 2002;110(2):280 –284
15. French NP, Hagan R, Evans SF, Godfrey M, N e w n h a m J P . R e p e a t e d a n t e n a t a l corticosteroids: size at birth and subse-quent development.Am J Obstet Gynecol. 1999;180(1):114 –121
16. Crowther CA, Doyle LW, Haslam RR, et al. Out-comes at 2 years of age after repeat doses of antenatal corticosteroids.N Engl J Med. 2007;357(12):1170 –1189
17. Wapner RJ, Sorokin Y, Mele L, et al. Long-term outcomes after repeat doses of ante-natal corticosteroids.N Engl J Med. 2007; 357(12):1190 –1198
18. Peltoniemi OM, Kari MA, Lano A, et al. Two-year follow-up of a randomised trial with repeated antenatal bethamethasone.Arch Dis Child Fetal Neonatal Ed. 2009;94(6): F402–F406
Infant Development for cognitive function of extremely low birth weight children at school age. Pediatrics. 2005;116(2): 333–341
20. Huang WL, Beazley LD, Quinlivan JA, Evans SF, Newnham JP, Dunlop SA. Effect of corti-costeroids on brain growth in fetal sheep. Obstet Gynecol. 1999;94(2):213–218
21. Uno H, Lohmiller L, Thieme C, et al. Brain damage induced by prenatal exposure to dexamethasone in fetal rhesus macaques, part I: hippocampus.Brain Res Dev Brain Res. 1990;53(2):157–167
22. French NP, Hagan R, Evans SF, Mullan A, N e w n h a m J P . R e p e a t e d a n t e n a t a l corticosteroids: effects on cerebral palsy
and childhood behavior.Am J Obstet Gy-necol. 2004;190(3):588 –595
23. Achenbach System of Empirically Based As-sessment. Child Behavior Checklist/11⁄
2–5.
Available at: www.aseba.org/index.htmlXXX. Accessed March 1, 2005
24. Barker DJP. The origins of the developmen-tal origins theory.J Intern Med. 2007;261(5): 412– 417
25. Waterland RA, Michaels KB. Epigenetic epide-miology of the developmental origins hypoth-esis.Annu Rev Nutr. 2007;27:363–388 26. Unterberger A, Andrews SD, Weaver IC, Szyf
M. DNA methyltransferase 1 knockdown ac-tivates a replication stress checkpoint.Mol CellBiol. 2006;26(20):7575–7586
27. Szyf M. Early life, the epigenome and human health.Acta Paediatr. 2009;98(7):1082–1084
28. Unterberger A, Szyf M, Nathanielsz PW, Cox LA. Organ and gestational age effects of ma-ternal nutrient restriction on global methyl-ation in fetal baboons.J Med Primatol. 2009; 38(4):219 –227
29. Kapoor A, Petropolous S, Matthews SG. Fetal programming of hypothalamic-pituitary-adrenal (HPA) axis function and behaviour by synthetic glucocorticoids.Brain Res Rev. 2008;57(2):586 –595
DOI: 10.1542/peds.2010-0857 originally published online October 18, 2010;
2010;126;e1045
Pediatrics
Antenatal Corticosteroids for Preterm Birth Study Collaborative Group
B. Anthony Armson, Renee Sananes, Laura Tomat and for the Multiple Courses of
Marie-France Delisle, Kofi Amankwah, Patricia Guselle, Amiram Gafni, Shoo K. Lee,
Stephen G. Matthews, Arne Ohlsson, Edmond N. Kelly, Saroj Saigal, Susan Ross,
Elizabeth V. Asztalos, Kellie E. Murphy, Mary E. Hannah, Andrew R. Willan,
Outcomes
Multiple Courses of Antenatal Corticosteroids for Preterm Birth Study: 2-Year
Services
Updated Information &
http://pediatrics.aappublications.org/content/126/5/e1045 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/126/5/e1045#BIBL This article cites 20 articles, 5 of which you can access for free at:
Subspecialty Collections
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior
Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2010-0857 originally published online October 18, 2010;
2010;126;e1045
Pediatrics
Antenatal Corticosteroids for Preterm Birth Study Collaborative Group
B. Anthony Armson, Renee Sananes, Laura Tomat and for the Multiple Courses of
Marie-France Delisle, Kofi Amankwah, Patricia Guselle, Amiram Gafni, Shoo K. Lee,
Stephen G. Matthews, Arne Ohlsson, Edmond N. Kelly, Saroj Saigal, Susan Ross,
Elizabeth V. Asztalos, Kellie E. Murphy, Mary E. Hannah, Andrew R. Willan,
http://pediatrics.aappublications.org/content/126/5/e1045
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.