Implications of the Transition
From Zapletal to GLI Reference
Values for Spirometry
Lena Raaijmakers, Bsc,a Annelies Zwitserloot, MD,a,b Peter Merkus, MD, PhD,a Monika Gappa, MD, PhDb
aDepartment of Respiratory Medicine and Allergy, Radboud University Nijmegen Medical Centre, Amalia Children’s Hospital, Nijmegen, Netherlands; and bDepartment of Paediatrics and Research Institute, Marien Hospital Wesel, Wesel, Germany
Ms Raaijmakers drafted the initial manuscript and carried out the initial analyses; Dr Zwitserloot conceptualized the study and reviewed and revised the manuscript; Drs Merkus and Gappa reviewed and revised the manuscript; and all authors approved the fi nal manuscript as submitted.
DOI: 10.1542/peds.2015-0033 Accepted for publication Aug 26, 2015 Address correspondence to Lena Raaijmakers, Radboud University Nijmegen Medical Centre, Department of Respiratory Medicine and Allergy, PO Box 9101 Nijmegen, 6500 HB, Netherlands. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2016 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no fi nancial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential confl icts of interest to disclose.
Asthma is characterized by chronic inflammation of the airways, resulting in bronchial hyperreactivity and variable airway obstruction.1 The
prevalence of asthma in Western Europe is 9.7% in children aged 6 to 7 years and 15.8% in children aged 13 to 14 years. Of these children, 12.6% and 15.2% are diagnosed with severe asthma, respectively.2
The diagnosis of asthma is based on a structured and thorough medical history, physical examination, and lung function testing. Usually, spirometry is performed, and reversibility with a significant improvement (>12%) of the forced expiratory volume in 1 second (FEV1) after bronchial dilatation is considered to be characteristic of asthma. The medical treatment of asthma is based on the treatment protocol devised by the Global Initiative for Asthma (GINA) and/or National Guidelines. Treatment of asthma follows a stepwise approach with short-acting
β-antagonists on demand for all grades of severity, and long-term controller medication according to severity and control, starting with low-dose inhaled corticosteroids, followed by a combination with long-acting β-antagonists and/or leukotriene antagonists. The severity of asthma, divided into the categories mild, moderate, and severe, can also be derived from these guidelines.3
Treatment of asthma is usually guided by asthma control, which may be controlled, partially controlled, and uncontrolled. The definition of uncontrolled asthma is the expression of ≥3 characteristics of partly controlled asthma (Table 1).2
For objective assessment of asthma control, normally spirometry is performed. Treatment is then adjusted according to asthma control.
Until now, results of lung function tests in Europe were mostly related to Zapletal reference values published in 1977.4 Recently, the Global Lung
abstract
The current standard for monitoring lung function in children with asthma is spirometry. In Europe, results of these lung function tests have been related to Zapletal reference values published in 1977. Recently, the Global Lung Function Initiative (GLI) published predicted values of spirometry for 5 ethnic groups, valid over an age range from 3 to 95 years. These reference values have been approved by many international lung societies, and the algorithms are increasingly being implemented globally. This report describes the consequences of the transition from Zapletal reference values to GLI reference values for 2 pediatric asthma patients, which include unexpected declines in lung function and the ability to take advantage of newly approved reimbursement for advanced therapy. The Zapletal and GLI reference values cannot be used interchangeably, and transition to the GLI values might lead to better treatment in the future.
CASE REPORT
PEDIATRICS Volume 137 , number 1 , January 2016 :e 20150033
To cite: Raaijmakers L, Zwitserloot A, Merkus P, et al. Implications of the Transition From Zapletal to GLI Reference Values for Spirometry. Pediatrics.
2016;137(1):e20150033
at Viet Nam:AAP Sponsored on August 29, 2020 www.aappublications.org/news
RAAIJMAKERS et al
Function Initiative (GLI) published predicted values of spirometry for 5 ethnic groups, valid over an age range from 3 to 95 years. These reference values have been approved by many international lung societies, and the algorithms are increasingly being implemented globally.5
We illustrate the potential clinical significance of the transition to the new reference values in clinical routine.
CASES
In our outpatient department, a 16-year-old boy with uncontrolled asthma according to GINA came in for a regular checkup. His treatment at the time consisted of a combination of formoterol and budesonide 9/320
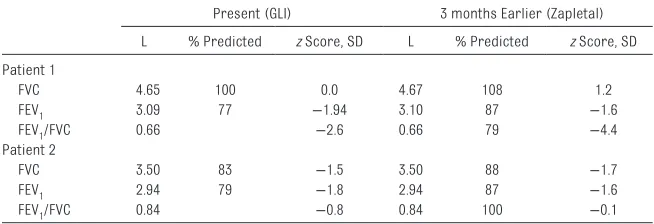
μg 1 dose twice a day, montelukast 10 mg once a day, and formoterol as needed. He had not experienced any symptoms in the weeks before the visit, apart from a mild cold 2 weeks earlier. As part of this routine visit, a spirometric lung function test was carried out. The results were as follows: forced vital capacity (FVC) of 4.65 L (100% predicted or z score 0.0 SD), FEV1 3.09 L (77% or –1.9 SD), and FEV1/FVC 0.66 (77% or –2.6 SD) using GLI reference values compared with a FVC of 109% (1.2 SD), FEV1 87% (–1.6 SD), and FEV1/FVC 79% (–4.4 SD) according to Zapletal reference values 3 months earlier (Table 2). The lung function values did not show any improvement after salbutamol 400 μg. Thus, the boy presented with significantly lower lung function, without an apparent cause or symptoms. The only
possibly related event was the recent cold, but we felt this was clinically not significant enough to explain the decline. It was decided to increase the dosage of the budesonide and formoterol from 1 to 2 doses twice a day. A follow-up appointment was planned. When reevaluating the test results, it was noticed that the latest lung function test had been expressed as % predicted according to GLI and the old test according to Zapletal.
A 14-year-old girl diagnosed with severe asthma had been visiting our outpatient department for years. Her therapy consisted of a fixed-dose combination of budesonide and formoterol 160/4.5 μg 2 doses twice a day, montelukast 10 mg once a day, and salbutamol as needed. She used the salbutamol ∼4 times per week. Despite her extensive therapy, she experienced many symptoms, consisting of nocturnal coughing, exercise intolerance, and asthma exacerbations requiring therapy with oral steroids. Additionally, her lung function showed an FVC of 3.52 L (88% or –1.7 SD), FEV1 2.95 L (87% or –1.6 SD), and FEV1/FVC 0.84 (100% or –0.1 SD) expressed according to Zapletal reference
values (Table 2). Because of the nature of her symptoms and the abnormal lung function, omalizumab as a step-up option was discussed. However, reimbursement depends on various criteria including level of lung function (FEV1 <80%). When relating the actual lung function to the reference values composed by GLI, FEV1 was 79% predicted, allowing prescription of omalizumab within predefined criteria.
On the basis of these 2 case descriptions, we conclude that the switch of reference values for spirometry from the GLI to Zapletal may have clinical consequences. However, to understand the effects the switch causes, the differences between GLI and Zapletal need to be specified.
DISCUSSION
A recent study has shown that significant differences exist in the predicted values of Zapletal and GLI, especially in age categories 6 to 8 and 14 to 18, in which the FEV1 and FVC % predicted expressed by using GLI data may be up to ∼15% and
∼20% lower, respectively.4 These
2
TABLE 1 GINA Criteria
Characteristics Controlled Partly Controlled Uncontrolled
Daytime symptoms None (twice or less/week) More than twice/week ≥3 features of partly controlled
asthma
Limitation in activities None Any
Nocturnal symptoms/awakening None Any
Need for reliever/rescue treatment None (twice or less/week) More than twice/week
Lung function (PEF or FEV1) Normal <80% predicted or personal best (if known)
PEF, peak expiratory fl ow.
TABLE 2 Lung Function Values
Present (GLI) 3 months Earlier (Zapletal) L % Predicted z Score, SD L % Predicted z Score, SD Patient 1
FVC 4.65 100 0.0 4.67 108 1.2
FEV1 3.09 77 −1.94 3.10 87 −1.6
FEV1/FVC 0.66 −2.6 0.66 79 −4.4
Patient 2
FVC 3.50 83 −1.5 3.50 88 −1.7
FEV1 2.94 79 −1.8 2.94 87 −1.6
FEV1/FVC 0.84 −0.8 0.84 100 −0.1
at Viet Nam:AAP Sponsored on August 29, 2020 www.aappublications.org/news
PEDIATRICS Volume 137 , number 1 , January 2016
differences can be partially explained by differences in the statistical approach between the Zapletal and GLI reference values. The algorithm by Zapletal et al includes gender and standing height of a patient only and was developed and approved for Caucasian children from 6 to 17 years old, almost 40 years ago.6 GLI
algorithms take height and age into account and are available according to gender and ethnicity for all ages, from 3 to 95 years.5 Furthermore, the
algorithm published by Zapletal was based on a small data set of 60 boys and 51 girls, whereas the GLI values have been based on measurements in 77 658 healthy nonsmokers from around the world, of which 15 264 persons were girls and 15 601 were boys between 2.5 and 18 years old.7
These aspects explain why use of Zapletal versus GLI reference data sets yields these differing results.
This issue is illustrated in the first case described here in which a change in therapy was thought to be indicated on the basis of the spirometry result. Reevaluation showed that the apparent decline was attributable to the switch in GLI reference values rather than a true clinically relevant change. However, one may ask whether a proportion of patients have been undertreated over the past decades and whether this may result in a worse prognosis with regard to lung function later in life.
In contrast, the second case illustrates how changing reference values may have a positive effect on case management when patients fit the qualification criteria for prescribing omalizumab.
To prevent misinterpretation of individual patients’ lung function,
manufacturers should be required to show which set of reference values is used on the output. In addition, software should be able to convert historical data to new values when reference values are changed and should show z scores instead of percentage predicted. Clinical decisions regarding treatment are based on percentage predicted, whereas z scores would be a better choice for comparing volumes. The reason for this is that the scatter around predicted is not proportional to percentage predicted, leading to an age bias. In our cases, the outlying percentages predicted correspond to the outlying z scores, which both support our clinical decisions.
CONCLUSIONS
The switch from Zapletal to GLI reference values changes interpretation of lung function tests in a subgroup of patients. Predicted values of lung function are higher for a proportion of the youngest and oldest pediatric patients. The old and new reference values should not be used interchangeably. Switch to the GLI values may reduce undertreatment. How this may affect patient outcome in the long-term is an area for future research.
ABBREVIATIONS
FEV1: forced expiratory volume in 1 second
FVC: forced vital capacity GINA: Global Initiative for
Asthma
GLI: Global Lung Function Initiative
REFERENCES
1. International Union Against Tuberculosis and Lung Disease. The Global Asthma Report 2011. 2011. Available at: http://www. globalasthmanetwork.org/ publications/Global_Asthma_ Report_2011.pdf. Accessed December 17, 2014
2. Lai CKW, Beasley R, Crane J, Foliaki S, Shah J, Weiland S; International Study of Asthma and Allergies in Childhood Phase Three Study Group. Global variation in the prevalence and severity of asthma symptoms: phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax. 2009;64(6):476–483
3. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2014. Available at: http:// www.ginasthma.org/local/uploads/ fi les/GINA_Report_2014_Aug12.pdf. Accessed December 17, 2014
4. Quanjer PH, Weiner DJ. Interpretative consequences of adopting the Global Lungs 2012 reference equations for spirometry for children and adolescents. Pediatr Pulmonol. 2014;49(2):118–125
5. Quanjer PH, Stanojevic S, Cole TJ, ; ERS Global Lung Function Initiative. Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343
6. Zapletal A, Paul T, Samánek M. Signifi cance of contemporary methods of lung function testing for the detection of airway obstruction in children and adolescents [author’s transl] [in German]. Z Erkr Atmungsorgane. 1977;149(3):343–371
7. Quanjer PH, Hall GL, Stanojevic S, Cole TJ, Stocks J; Global Lungs Initiative. Age- and height-based prediction bias in spirometry reference equations. Eur Respir J. 2012;40(1):190–197
3 at Viet Nam:AAP Sponsored on August 29, 2020
DOI: 10.1542/peds.2015-0033 originally published online December 24, 2015;
2016;137;
Pediatrics
Lena Raaijmakers, Annelies Zwitserloot, Peter Merkus and Monika Gappa
Spirometry
Implications of the Transition From Zapletal to GLI Reference Values for
Services
Updated Information &
http://pediatrics.aappublications.org/content/137/1/e20150033
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/137/1/e20150033#BIBL
This article cites 5 articles, 3 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/asthma_subtopic
Asthma
http://www.aappublications.org/cgi/collection/pulmonology_sub
Pulmonology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
at Viet Nam:AAP Sponsored on August 29, 2020 www.aappublications.org/news
DOI: 10.1542/peds.2015-0033 originally published online December 24, 2015;
2016;137;
Pediatrics
Lena Raaijmakers, Annelies Zwitserloot, Peter Merkus and Monika Gappa
Spirometry
Implications of the Transition From Zapletal to GLI Reference Values for
http://pediatrics.aappublications.org/content/137/1/e20150033
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2016 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 29, 2020 www.aappublications.org/news