TABLE OF CONTENTS Systematic Review
Abstract 3
Introduction 4
Methods 5
Results 7
Discussion 9
Conclusions 10
Appendices 12
References 17
Clinical Paper
Abstract 19
Introduction 20
Methods 21
Results 24
Discussion 25
Conclusions 27
References 28
Hepatic toxicity and Efavirenz use in Pregnant Women: A Systematic Review ABSTRACT
Introduction: Prevention of mother-to-child transmission (PMTCT) of HIV is essential in reducing HIV incidence and prevalence. In the past few years, many countries have moved to providing universal, lifelong antiretroviral therapy (ART) to all HIV-positive pregnant and breastfeeding women regardless of health status. Given the expansion of women initiating therapy while pregnant or breastfeeding, safety of these ART regimens must be ensured in this population. This review seeks to answer whether risk for hepatic toxicity secondary to efavirenz (EFV) use differs for pregnant/breastfeeding women, other groups of women, and men.
Methods: Studies published prior to March 22nd, 2017 were identified in PubMed and
EMBASE. ClinicalTrials.org and WHO ICTRP were searched for unpublished literature. Review included studies published in English that considered pregnant/breastfeeding women on EFV without known pre-existing liver disease and considered hepatic toxicity as an outcome. Relevant measures were collected from each study and risk of bias was assessed.
Results: Four studies were included after title, abstract, and full text review. Given the extremely low incidence of hepatic toxicity in pregnant individuals in each study, no robust comparisons were made for this specific adverse event in this population. Risk of bias for the proposed
question was unclear since sample sizes were so small and no study was designed to evaluate the specific outcome of hepatic toxicity.
starting ART while pregnant or breastfeeding, better characterization of their specific risks for adverse events is crucially important.
INTRODUCTION
Prevention of mother-to-child transmission (PMTCT) of HIV has been recognized as a cornerstone to successful national initiatives to reduce the burden of HIV. Recent spread and intensification of these programs has contributed to a reduction in incidence in infants by 50%.1 Additionally, the percentage of pregnant or breastfeeding women receiving antiretroviral therapy (ART) has increased from 50% to 77% since 2010.1
Prior to 2011, the international standard, as suggested by the World Health Organization (WHO), proposed two options for PMTCT for women not sick enough to qualify for ART. Option A includes maternal treatment with antenatal zidovudine and infant treatment with nevirapine during breastfeeding, while Option B employs maternal treatment throughout
pregnancy and breastfeeding.2 Since 2011, several countries have employed a strategy known as Option B+, an alternative providing universal, lifelong antiretroviral therapy (ART) to all HIV-positive pregnant and breastfeeding women regardless of health status in order to improve maternal health, employ treatment as prevention for reduction of adult transmission, and reduce vertical transmission.3
populations, potential for adverse effects during pregnancy must be better understood in the context of Option B+.4 Health risks and benefits of starting ART in healthier pregnant women have not been extensively studied in resource limited settings.5 Establishing the safety and effectiveness of currently recommended drug regimens for both mothers and infants is critical to ensuring this policy achieves the improvement in maternal health, reduction in adult
transmission, and reduction in mother-to-child transmission that it is intended to achieve without undue harm.
As established by the WHO, the primary regimen used for ART initiation in pregnant and breastfeeding women under Option B+ is efavirenz/tenofovir/lamivudine (EFV/TDF/3TC).6 While this regimen has many benefits over others, including not being limited to those with lower CD4 cell counts and potentially better adverse event profile, its safety in women initiating ART while pregnant or breastfeeding is less clear.6,7 While much research has been done
concerning the potential birth defects associated with EFV, including tracking with the Antiretroviral Pregnancy Registry, less is known about its effect on maternal health.8–13
We conducted a systematic review of efavirenz (EFV) and hepatic toxicity in pregnant and breastfeeding women, non-pregnant women, and men. Although we consider a range of possible drug regimens, each combination needed to include efavirenz. We aimed to describe (1) whether risk for hepatic toxicity secondary to efavirenz use differs across these sub-populations, and (2) whether initiating EFV-based ART prior to pregnancy compared to initiation while pregnant or breastfeeding was associated with a chance in incidence of hepatic toxicity.
A systematic protocol was used to search PubMed and EMBASE for studies published prior to March 22nd, 2017. ClinicalTrials.gov and the World Health Organization International Clinical Trials Registry Platform were also searched for unpublished and ongoing studies. Search terms were developed with the help of a librarian experienced with systematic reviews in order to identify studies that included HIV-positive pregnant patients treated with efavirenz and
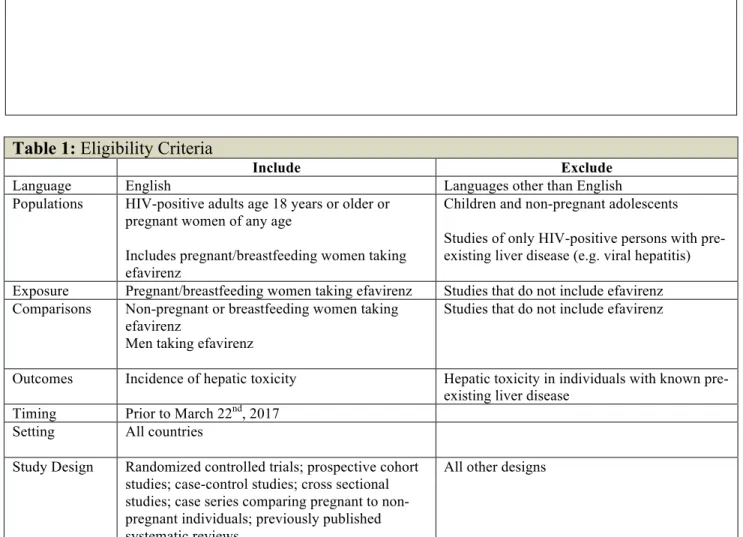
measurement of hepatic toxicity. Search strategy for each database is shown below in Figure 1. Inclusion and exclusion criteria were established for populations, interventions,
comparators, outcomes, and study designs (Table 1). Studies must be published in English. Studies had to include pregnant women. Interventions (drug regimens) were allowed to vary, but needed to include efavirenz. Comparisons could not include individuals with viral hepatitis or known pre-existing liver disease. Studies could include a variety of outcomes, but must include hepatic toxicity. Eligible study designs were randomized controlled trials, prospective or
retrospective cohort studies, case-control studies, cross sectional studies, systematic reviews, and large case series studies.
One reviewer (RB) evaluated each title and abstract for eligibility against the criteria outlined above and reviewed all full-text articles that could not be excluded during abstract review to determine final eligibility. For studies meeting eligibility criteria, data were abstracted by one reviewer (RB) for further analysis. Quality assessment criteria for the internal validity of individual studies were drawn from the ROBINS-I tool by the Cochrane Bias Methods Group.14 Risk of bias was graded as high, medium, low, or uncertain.
measures considered included odds ratios, risk ratios, risk differences, and any measure of incidence. Search of grey literature using clinical trials registries was done to assess for selective reporting and possible publication bias.
RESULTS
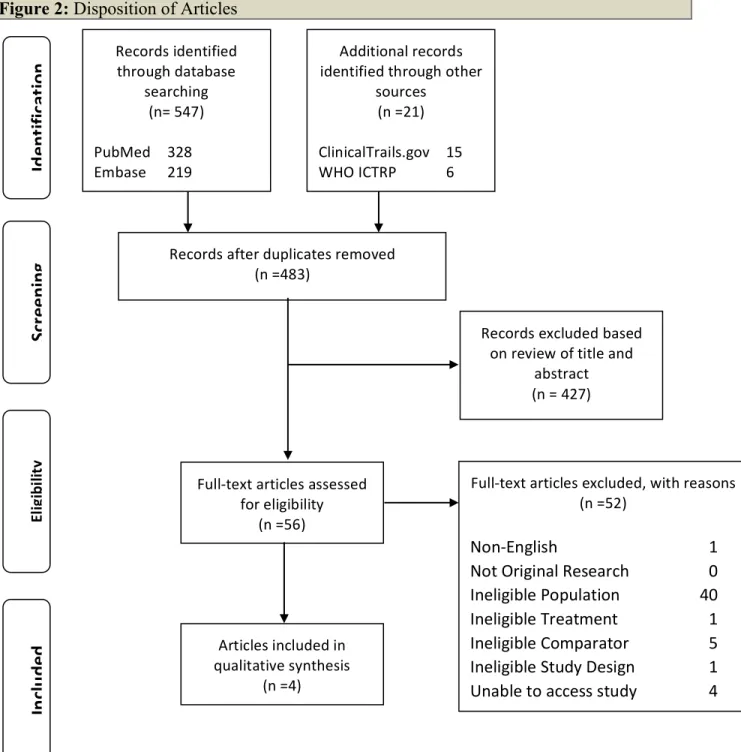
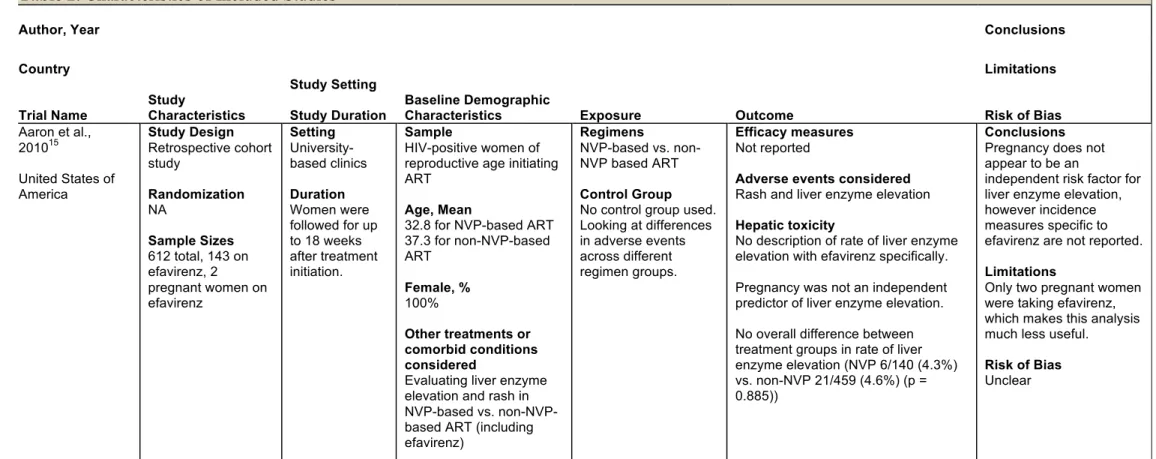
A total of 483 potentially relevant articles were included in initial review. After title and abstract review, 56 studies could not be excluded. After full-text review of these studies, four studies were found to meet all inclusion and exclusion criteria (Figure 2). Search for clinical trials yielded 21 results. All potentially relevant studies were either still recruiting or withdrawn prior to initiation, and thus were not included. Study characteristics and bias assessments are detailed in Table 2.
Given the extremely low incidence of hepatic toxicity in pregnant individuals in each study, no robust comparisons were made for this specific adverse event in this population. One study considered adverse events, including hepatic toxicity, in women taking nevirapine-based ART compared to non-nevirapine-based ART (including efavirenz).15 Only 2 pregnant women were taking efavirenz in this study, so no meaningful conclusions could be drawn. However, pregnancy was not an independent predictor of hepatic toxicity in the overall study population.15
of hepatic toxicity was noted in the study with no description of whether or not the participant was pregnant.16
A systematic review and meta-analysis found very little available evidence about efavirenz use and maternal outcomes, although the stated goal of the analysis was primarily to consider birth outcomes.17 They note that only 2 available studies of pregnant women taking efavirenz reported adverse events, and neither reported any hepatic toxicity.17–19 These studies were not included individually because they did not include non-pregnant comparison groups or the outcome of hepatic toxicity.
The final study included was a large case series looking at patterns of liver injury in South Africans taking efavirenz.20 Each of the 81 patients in this study had drug induced liver injury while on efavirenz; 18 (22%) of these were cases where ART was initiated while a woman was pregnant.20 The authors concluded that submassive necrosis of the liver among younger women with higher CD4 counts may be associated with beginning efavirenz-based ART.20
While there certainly are issues with bias associated with each study design, the most important finding is that the available sample size in each study was insufficient to confidently address the proposed questions. This result is not a surprise given that none of these studies sought to definitively describe the difference in incidence of hepatic toxicity between pregnant women and other populations taking efavirenz. The risk of bias for the question of interest in the first two studies included is unclear given the very small relevant population of pregnant women taking efavirenz; while each study certain has specific strengths and weakness, none are really relevant to the proposed question.15,16 The systematic review and meta-analysis was
hepatic toxicity as an adverse event for pregnant women taking efavirenz.17 The large case series has significant biases and limitations given its design; only examining patients with liver injury, with no description of overall incidence or comparison of incidence rates for different
populations (e.g. pregnant women compared to others), does not allow for strong conclusions to be drawn.20 The authors can say very little about possible associations without overall incidence measures. Their described possible risk factors for certain types of hepatic injury must be viewed in light of these significant limitations.
Since there is little to no available outcome data that compares pregnant women taking efavirenz to non-pregnant women or men, no confident conclusions can be drawn about the possible risk differential between these groups. Additionally, there is also not enough data to answer whether or not there is a difference in risk for hepatic toxicity in women initiating efavirenz-based ART prior to pregnancy compared to during pregnancy.
DISCUSSION
This review found little evidence of increased risk of hepatic toxicity in women initiating efavirenz-based ART while pregnant or breastfeeding. However, there was a paucity of literature addressing this question, and therefore no confident conclusions can be drawn.
For stakeholders involved in delivery of HIV treatment, including funders, ministries of health, non-governmental organizations, and others, the lack of evidence surrounding adverse events, specifically hepatic toxicity, in pregnant and breastfeeding women initiating ART should be concerning. Recent policies that have massively increased the number of pregnant and
outcomes and reduce mother-to-child transmission. However the ripple effects of such policies, including specific adverse events in pregnant women initiating ART, must be rigorously studied to ensure risks do not outweigh benefits.
The primary limitations of each of the studies included relate to sample size for populations relevant to this review. None of these studies sought to answer the question of difference in incidence of hepatic toxicity between groups, so this finding is to be expected. For the large case series, the study design presents numerous limitations, most importantly inability to assert meaningful association without overall incidence measures.20 While the search strategy was intended to maximize sensitivity and review all potentially relevant studies, there may have been gaps because of authors using a variety of key terms, MESH terms, and titles in describing their work. The search strategy may have also been limited by exclusion of non-English
language studies.
Bias of each study was considered, but is hardly meaningful since the sample sizes were so small and conclusions were so weak. Publication bias is unlikely in these studies since adverse events are a chief concern in large ART programs. Future studies related to prevention of
mother-to-child transmission and congenital anomalies should report on adverse events related to efavirenz use for mothers in addition to the other outcomes considered.
CONCLUSIONS
Given the large number of women starting ART while pregnant or breastfeeding under current WHO policies, better characterization of their specific risks for adverse events is crucially important.
III. Appendices !
Figure 1: Search Strategy!
PubMed: ((Efavirenz[tw] AND (Liver injur*[tw] OR hepatitis[tw] OR Hepatitides[tw] OR hepatic toxicity[tw]))) OR (Efavirenz[tw] AND adverse[tw] AND pregnan*[tw])
EMBASE: 'efavirenz'/exp/mj AND (“Liver injury”:de,ab,ti OR “Liver injuries”:de,ab,ti OR hepatitis:de,ab,ti OR Hepatitides:de,ab,ti OR “hepatic toxicity”:de,ab,ti)
Clinical Trials (clinicaltrials.gov; WHO ICTRP): efavirenz AND pregnancy
!
!
Table 1: Eligibility Criteria
Include Exclude
Language English Languages other than English
Populations HIV-positive adults age 18 years or older or pregnant women of any age
Includes pregnant/breastfeeding women taking efavirenz
Children and non-pregnant adolescents Studies of only HIV-positive persons with pre-existing liver disease (e.g. viral hepatitis) Exposure Pregnant/breastfeeding women taking efavirenz Studies that do not include efavirenz Comparisons Non-pregnant or breastfeeding women taking
efavirenz
Men taking efavirenz
Studies that do not include efavirenz
Outcomes Incidence of hepatic toxicity Hepatic toxicity in individuals with known pre-existing liver disease
Timing Prior to March 22nd, 2017 Setting All countries
Study Design Randomized controlled trials; prospective cohort studies; case-control studies; cross sectional studies; case series comparing pregnant to non-pregnant individuals; previously published systematic reviews
All other designs
Figure 2: Disposition of Articles ! ! ! Records(identified( through(database( searching( (n=(547)( ( PubMed( 328( Embase( 219( ( Sc re eni ng ! In cl ude d! El ig ib ili ty ! Id ent ifi ca tio
!
Table 2. Characteristics of Included Studies
Author, Year Conclusions
Country Limitations
Trial Name Study Characteristics
Study Setting
Study Duration Baseline Demographic Characteristics Exposure Outcome Risk of Bias
Aaron et al., 201015
United States of America Study Design Retrospective cohort study Randomization NA Sample Sizes
612 total, 143 on efavirenz, 2 pregnant women on efavirenz Setting University-based clinics Duration Women were followed for up to 18 weeks after treatment initiation.
Sample
HIV-positive women of reproductive age initiating ART
Age, Mean
32.8 for NVP-based ART 37.3 for non-NVP-based ART
Female, %
100%
Other treatments or comorbid conditions considered
Evaluating liver enzyme elevation and rash in NVP-based vs. non-NVP-based ART (including efavirenz)
Regimens
NVP-based vs. non-NVP based ART
Control Group
No control group used. Looking at differences in adverse events across different regimen groups.
Efficacy measures
Not reported
Adverse events considered
Rash and liver enzyme elevation
Hepatic toxicity
No description of rate of liver enzyme elevation with efavirenz specifically.
Pregnancy was not an independent predictor of liver enzyme elevation.
No overall difference between treatment groups in rate of liver enzyme elevation (NVP 6/140 (4.3%) vs. non-NVP 21/459 (4.6%) (p = 0.885))
Conclusions
Pregnancy does not appear to be an
independent risk factor for liver enzyme elevation, however incidence measures specific to efavirenz are not reported.
Limitations
Only two pregnant women were taking efavirenz, which makes this analysis much less useful.
Risk of Bias
Danel et al., 200616 Abidjan, Cote d’Ivoire Study Design Prospective cohort study Randomization NA Sample Sizes 740 total, 7 pregnant women Setting 5 outpatient clinics in Abidjan Duration 6 months Sample HIV-positive adults initiating ART Age, Mean (IQR) 34 (29 - 40)
Female, % 74% Other
treatments/comorbid conditions considered No other ART regimens considered. Evaluate numerous other morbid conditions during first 6 months of ART. Split analysis based on HBV serology results. Regimens Zidovudine-lamivudine-efavirenz Control Group None Efficacy measures
CD4 count and HIV-1 viral load testing done at 3 and 6 months
Adverse events considered Recorded all causes of morbidity during 6-month period. Separately considered adverse events leading to treatment modification.
Hepatic toxicity
9 adverse events were attributable to efavirenz, including only 1 case of hepatic toxicity.
No description given of incidence of hepatic toxicity in 7 pregnant women.
Conclusions
Efavirenz does not seem to be associated with a high incidence of hepatic toxicity. No conclusions can be drawn about risk in pregnant women,
although none experienced hepatic toxicity in this study. Limitations
Very small sample of pregnant women for comparison. Risk of Bias Unclear
Ford et al., 201417 Multi-country systematic review and meta-analysis Study Design Systematic review and meta-analysis Randomization NA Sample Sizes 12 studies total, 2 reporting adverse events Setting Multi-country Duration Variable Sample
Pregnant women taking efavirenz
Age, Median range 28-33 Female, % 100% Other treatments/comorbid conditions considered Primary focus on congenital defects Regimens Efavirenz-based ART Control Group Variable Efficacy measures Not reported
Adverse events considered Congenital defects
Any reported adverse events Hepatic toxicity
No study noted any hepatic toxicity
Conclusions Limited reporting of adverse events gives little information to draw meaningful conclusions for potential increased risk associated with efavirenz use during pregnancy. Limitations
Only two studies reporting adverse events.
Sonderup et al., 201620 South Africa Study Design Case series Randomization NA Sample Sizes
81 total, 18 pregnant
Setting
South Africa (no further information given) Duration Unclear Sample HIV-positive patients taking efavirenz-containing first-line ART who experience drug induced liver injury (DILI)
Age, Median 34 Female, % 73% Other treatments/comorbid conditions considered Considered hepatitis serologies and immune reconstitution inflammatory syndrome. Regimens Efavirenz-containing first-line ART Control Group None Efficacy measures None
Adverse events considered
Drug induced liver injury Rash
Hepatic toxicity
Each of the 81 patients in this study had drug induced liver injury while on efavirenz; 18 of these were cases where ART was initiated while a woman was pregnant.
Conclusions
Submassive necrosis of the liver may be associated with younger women with higher CD4 counts beginning efavirenz-based ART
Limitations
Case series design greatly limits strength of conclusions.
Risk of Bias
References
1. Preventing mother-to-child transmission of HIV | UNAIDS.
http://www.unaids.org/en/resources/presscentre/featurestories/2016/october/201610 24_EMotherToChildT. Accessed March 8, 2017.
2. Ciaranello AL, Perez F, Maruva M, et al. WHO 2010 Guidelines for Prevention of Mother-to-Child HIV Transmission in Zimbabwe: Modeling Clinical Outcomes in
Infants and Mothers. PLOS ONE. 2011;6(6):e20224.
doi:10.1371/journal.pone.0020224.
3. Ministry of Health Malawi. Clinical Management of HIV in Adults and Children: Malawi Integrated Guidelines for Providing Service in: Antenatal Care, Maternity Care, Under Five Clinics, Family Planning Clinics, Exposed Infant/Pre-ART clinics, ART clinics. 2011.
4. Grinsztejn B, Hosseinipour MC, Ribaudo HJ, et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: results
from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect Dis.
2014;14(4):281-290. doi:10.1016/S1473-3099(13)70692-3.
5. De Cock KM, El-Sadr WM. When to Start ART in Africa — An Urgent Research
Priority. N Engl J Med. 2013;368(10):886-889. doi:10.1056/NEJMp1300458.
6. UPdaTE Pr. Use of antiretroviral drugs for treating pregnant women and preventing
HIV infection in infants. WHO Geneva April. 2012.
http://www.who.int/entity/hiv/pub/pmtct_update.pdf. Accessed April 22, 2017.
7. Shapiro RL, Hughes MD, Ogwu A, et al. Antiretroviral regimens in pregnancy and
breast-feeding in Botswana. N Engl J Med. 2010;362(24):2282-2294.
doi:10.1056/NEJMoa0907736.
8. Bisio F, Nicco E, Calzi A, et al. Pregnancy outcomes following exposure to
efavirenz-based antiretroviral therapy in the Republic of Congo. New Microbiol.
2015;38(2):185-192.
9. Sibiude J, Mandelbrot L, Blanche S, et al. Association between prenatal exposure to antiretroviral therapy and birth defects: an analysis of the French perinatal cohort
study (ANRS CO1/CO11). PLoS Med. 2014;11(4):e1001635.
doi:10.1371/journal.pmed.1001635.
10. Phiri K, Hernandez-Diaz S, Dugan KB, et al. First trimester exposure to
antiretroviral therapy and risk of birth defects. Pediatr Infect Dis J.
2014;33(7):741-746. doi:10.1097/INF.0000000000000251.
11. Floridia M, Mastroiacovo P, Tamburrini E, et al. Birth defects in a national cohort
12. Ouattara EN, Anglaret X, Wong AY, et al. Projecting the clinical benefits and risks of using efavirenz-containing antiretroviral therapy regimens in women of
childbearing age. AIDS Lond Engl. 2012;26(5):625-634. doi:10.1097/QAD.0b013e328350fbfb.
13. For Health Care Providers. http://www.apregistry.com/HCP.aspx. Accessed May 16, 2017.
14. Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
doi:10.1136/bmj.i4919.
15. Aaron E, Kempf M-C, Criniti S, et al. Adverse Events in a Cohort of HIV Infected Pregnant and Pregnant Women Treated with Nevirapine versus
Non-Nevirapine Antiretroviral Medication. PLOS ONE. 2010;5(9):e12617. doi:10.1371/journal.pone.0012617.
16. Danel C, Moh R, Anzian A, et al. Tolerance and acceptability of an efavirenz-based regimen in 740 adults (predominantly women) in West Africa. J Acquir Immune Defic Syndr 1999. 2006;42(1):29-35. doi:10.1097/01.qai.0000219777.04927.50.
17. Ford N, Mofenson L, Shubber Z, et al. Safety of efavirenz in the first trimester of pregnancy: an updated systematic review and meta-analysis. AIDS Lond Engl. 2014;28 Suppl 2:S123-131. doi:10.1097/QAD.0000000000000231.
18. Areechokchai D, Bowonwatanuwong C, Phonrat B, Pitisuttithum P, Maek-A-Nantawat W. Pregnancy outcomes among HIV-infected women undergoing antiretroviral therapy. Open AIDS J. 2009;3:8-13.
doi:10.2174/1874613600903010008.
19. Cressey TR, Stek A, Capparelli E, et al. Efavirenz pharmacokinetics during the third trimester of pregnancy and postpartum. J Acquir Immune Defic Syndr 1999.
2012;59(3):245-252. doi:10.1097/QAI.0b013e31823ff052.
ABSTRACT
Introduction: Prevention of mother-to-child transmission (PMTCT) of HIV is essential
in reducing HIV incidence and prevalence. Many countries have moved to providing universal, lifelong antiretroviral therapy (ART) to all HIV-positive pregnant and breastfeeding women regardless of health status, necessitating adequate safety studies. Methods: We conducted a retrospective cohort study to compare risk of hepatic toxicity
secondary to initiation of EFV-based ART in a cohort of pregnant and breastfeeding women to risk in a cohort of non-pregnant/breastfeeding women and men. The main outcome of interest was development of hepatic toxicity in 6 months after treatment initiation (September 1, 2011 to August 31, 2016). Bivariable and multivariable analyses were conducted to assess differences across groups and ART regimen types.
Results: Pregnant and breastfeeding women group were younger and healthier overall.
Hepatic toxicity occurred in 41 (0.51%) out of 7,957 individuals in 6 months after starting ART. Bivariate comparisons revealed differences in comparisons of hepatic toxicity by group (p=0.01) and age category (p=0.04), with non-pregnant/breastfeeding women and older individuals having stronger associations. Multivariate comparisons showed no statistically significant difference in odds of developing hepatic toxicity for pregnant/breastfeeding women compared to men (OR=!0.47 (0.16, 1.39) or other women compared to men (OR=!1.49 (0.70, 3.19). Furthermore, no differences were seen when comparing EFV-based ART to non-EFV-based ART (OR=!0.99 (0.23, 4.19).
Conclusions: Our findings suggest that there is no additional concern for hepatic toxicity
INTRODUCTION
Prevention of mother-to-child transmission (PMTCT) of HIV has been recognized
as a cornerstone to successful national initiatives to reduce the burden of HIV. Recent
spread and intensification of these programs has contributed to a reduction in incidence in
infants by 50%.1 Additionally, the percentage of pregnant or breastfeeding women
receiving antiretroviral therapy (ART) has increased from 50% to 77% since 2010.1
Prior to 2011, the international standard, as suggested by the World Health
Organization (WHO), proposed two options for PMTCT for women not sick enough to
qualify for ART. Option A includes maternal treatment with antenatal zidovudine and
infant treatment with nevirapine during breastfeeding, while Option B employs maternal
treatment throughout pregnancy and breastfeeding.2 Since 2011, several countries have
employed a strategy known as Option B+, an alternative providing universal, lifelong
ART to all HIV-positive pregnant and breastfeeding women regardless of health status in
order to improve maternal health, employ treatment as prevention for reduction of adult
transmission, and reduce vertical transmission.3
Given the expansion of women initiating therapy while pregnant or breastfeeding,
safety of ART regimens used in such programs must be ensured in this population.
However, safetyof the prevailing ART regimens used during pregnancy has not been
rigorously studied in women initiating therapy while pregnant, since very few previous
trials have included this sub-population of women. While studies have demonstrated
strong benefits to early initiation of treatment in other populations, potential for adverse
effects during pregnancy must be better understood in the context of Option B+.4 Health
studied in resource limited settings.5 Establishing the safety and effectiveness of currently recommended drug regimens for both mothers and infants is critical to ensuring this
policy achieves the improvement in maternal health, reduction in adult transmission, and
reduction in mother-to-child transmission that it is intended to achieve without undue
harm.
As established by the WHO, the primary regimen used for ART initiation in
pregnant and breastfeeding women under Option B+ is efavirenz/tenofovir/lamivudine
(EFV/TDF/3TC).6 While this regimen has many benefits over others, including not being limited to those with lower CD4 cell counts and potentially better adverse event profile,
its safety in women initiating ART while pregnant or breastfeeding is less clear.6,7 While much research has been done concerning the potential birth defects associated with EFV,
including tracking with the Antiretroviral Pregnancy Registry, less is known about its
effect on maternal health during pregnancy and the postpartum period.8–13
We conducted a retrospective cohort study to compare risk of hepatic toxicity
secondary to initiation of EFV-based ART in a cohort of pregnant and breastfeeding
women to risk in a larger cohort of non-pregnant/breastfeeding women and men. We also
compare risk of hepatic toxicity in those taking EFV-based compared to non-EFV-based
ART.
METHODS
Design and Setting
This study was a retrospective analysis of data collected from a cohort of pregnant
women and men, all of whom were treated at a large HIV treatment facility run by the
Ministry of Health (Martin Preuss Centre) in Lilongwe, Malawi.
Subjects
All adult individuals initiating ART from September 1, 2011 until August 31,
2016 according to electronic medical record (EMR) data were considered. Inclusion
criteria for the cohort of pregnant or breastfeeding women included age ≥16 years and
HIV positive by 2 rapid tests approved by Malawi Ministry of Health. Exclusion criteria
included age <16 years or HIV negative. No other laboratory measures were used for
exclusion, but ART selection was modified on an individual basis based on Malawi HIV
guidelines.
Eligibility criteria for the cohort of non-pregnant/breastfeeding women and men
included age ≥16, HIV positive according to electronic medical record data, eligible for
ART based on WHO stage 3/4 or low CD4 count, and available ART regimen data.
Approval was received from both the National Health Sciences Research Committee of
Malawi (NHSRC) and the Biomedical Institutional Review Board of the University of
North Carolina at Chapel Hill.
Data collection
Data collection relevant to this analysis, not to the overall cohort study, is
described here. In the pregnant and breastfeeding women cohort, all women received
opt-out HIV testing during their first antenatal visit according to Malawi Ministry of Health
received ART education, counseling, a baseline CD4 count, and was encouraged to start
same-day first-line TDF/3TC/EFV. Mothers were seen monthly for 6 months after the
first antenatal visit and then quarterly for the duration of the study in accordance with
recommendations from the Malawi HIV program.
Group status was considered the main exposure variable; it included
pregnant/breastfeeding female, WHO stage 3/4 or low CD4 non-pregnant/breastfeeding
female, or WHO stage 3/4 or low CD4 male. The main outcome of interest was
development of hepatic toxicity (Yes, No, or Unknown) after treatment initiation. Hepatic
toxicity was primarily a clinical diagnosis; diagnosis was made by clinical suspicion
based on factors including new onset jaundice with right upper quadrant pain, drug
substitution from EFV to NVP, ATZ/r, or stopping EFV. Individuals who were
categorized as “Yes” or “Unknown” for the outcome were considered jointly as cases of
hepatic toxicity to reflect the clinical suspicion underlying the outcome. Importantly,
there was no laboratory confirmation of hepatotoxicity. Other data collected regarding
treatment and health status included age, weight, WHO clinical stage, tuberculosis (TB)
treatment, and ART regimen.
Data analysis
Univariable analyses were performed to compare health and demographic factors
for pregnant/breastfeeding women, non-pregnant/breastfeeding women, and men
initiating ART. Group data was missing for 0.4% of individuals.
Bivariable analyses included Fisher’s exact testing for hepatic toxicity by group
categories), by ART regimen type (EFV-based vs. non-EFV-based), and by TB treatment
(Yes vs. No). One-way ANOVA testing with pairwise comparisons using Bonferroni’s
correction were used to evaluate for differences in weight by group. Differences in these
tests were assessed at an alpha level of 0.05. Spearman’s correlation was used to evaluate
for co-linearity with a cut-off set at an absolute value of 0.3 or greater for rho value for
all possible covariates to be used in etiologic modeling.
Multivariable analyses included logistic regression models of risk for developing
hepatic toxicity across the 3 group categories and for ART regimen types, both using an
etiologic modeling approach. Covariates considered in the full models included age,
weight, WHO stage, and TB treatment. The initial model was reduced using a change in
estimate approach for etiologic modeling; however confounders deemed clinically
relevant were retained, even if the change in estimate was minimal.
This study had a power level of 98% to detect an odds ratio of 1.2 times the odds
of developing hepatic toxicity with a sample size of 7,989 at an alpha level of 0.05.
Statistical analysis was performed using Stata/SE 14.1 (StataCorp, Inc., College Station,
TX).
RESULTS
The study population (7,957 individuals) was predominantly individuals 20-40
years old on EFV-based ART. Notable between group differences were that the pregnant
and breastfeeding women group was younger, had more individuals on EFV-based ART,
The outcome of interest, development of hepatic toxicity after initiation of ART, occurred in only 41 individuals (0.51%).
Bivariate comparisons yielded statistically significant differences in comparisons of hepatic toxicity by group (p=0.01) and age category (p=0.04), but not by ART regimen type or TB treatment (Table 2). There were also statistically significant differences in initial weight across each of the groups, although this likely reflected the large sample size and not clinical relevance since absolute differences were small.
Multivariate comparisons using logistic regression with etiologic modeling and possible confounders showed no statistically significant difference in odds of developing hepatic toxicity for pregnant/breastfeeding women compared to men (OR=!0.47 (0.16, 1.39) or other women compared to men (OR=!1.49 (0.70, 3.19) (Table 3).
Furthermore, no differences were seen when comparing EFV-based ART to non-EFV-based ART (OR=!0.99 (0.23, 4.19) using the same etiologic modeling approach with logistic regression analysis (Table 4).
DISCUSSION
Given these findings, we do not recommend any changes be made to current
recommendations for ART regimens for this population. With the initial success of the
Option B+ program in Malawi and other countries, the number of pregnant/breastfeeding
women initiating ART will likely continue to grow. In our context,
pregnant/breastfeeding women initiating therapy represent 25% of all Malawians
beginning therapy. Continued study of adverse events associated with ART initiation in
pregnant/breastfeeding women is needed to accurately characterize their risk, minimize
harms, and optimize ART regimens for this group.
Our results are consistent with previous study findings concerning the risk of
hepatitis with EFV-based ART.6,7 However, most other studies have compared
EFV-based to Nevirapine-EFV-based ART with respect to adverse events, including hepatic
toxicity. No other available study has sought to compare risk associated with EFV-based
ART across women initiating therapy while pregnant/breastfeeding, non-pregnant
women, and men.
Our study had several noteworthy limitations. Under current clinical guidelines in
Malawi, hepatic toxicity in someone on ART is a clinical diagnosis that does not require
laboratory confirmation, thus true incidence of drug-induced hepatitis is difficult to
assess. Our analysis is based on this routine collection of clinical data, possibly
weakening the strength of our findings. Our data should be viewed as a preliminary
indication of EFV-based regimen safety in pregnant and breastfeeding women initiating
ART, but further prospective study of hepatic toxicity and other adverse events with
laboratory confirmation remains important. Additionally, given the relatively small
increased concern for pregnant/breastfeeding women. We also did not have data on past
liver disease for our patients and were unable to consider this as a possible confounder.
Other possible sources of bias include “healthy woman bias”, wherein women
who are healthy enough to become pregnant are the ones seen in care, creating an
unrepresentatively healthy pool of pregnant women with apparent increased incidence in
pregnant subjects. This bias is less likely since we did not see increased risk in
non-pregnant individual. Prevalent user bias is also a concern since we may have missed some
cases of hepatic toxicity in those who were lost to follow-up. These individuals may have
experienced adverse events, but never presented to care for their toxicity because they
either recovered or were lost to follow up.
CONCLUSION
Our findings suggest that there is no additional concern for hepatic toxicity in
pregnant/breastfeeding women initiating EFV-based ART. Based on our findings, we do
not suggest any changes to current treatment guidelines or practice patterns in Malawi.
Given the still growing number of pregnant/breastfeeding women initiating ART,
continued study of adverse events associated with ART initiation in this sub-population
REFERENCES
1. Preventing mother-to-child transmission of HIV | UNAIDS.
http://www.unaids.org/en/resources/presscentre/featurestories/2016/october/201610 24_EMotherToChildT. Accessed March 8, 2017.
2. Ciaranello AL, Perez F, Maruva M, et al. WHO 2010 Guidelines for Prevention of Mother-to-Child HIV Transmission in Zimbabwe: Modeling Clinical Outcomes in
Infants and Mothers. PLOS ONE. 2011;6(6):e20224.
doi:10.1371/journal.pone.0020224.
3. Ministry of Health Malawi. Clinical Management of HIV in Adults and Children: Malawi Integrated Guidelines for Providing Service in: Antenatal Care, Maternity Care, Under Five Clinics, Family Planning Clinics, Exposed Infant/Pre-ART clinics, ART clinics. 2011.
4. Grinsztejn B, Hosseinipour MC, Ribaudo HJ, et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: results
from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect Dis.
2014;14(4):281-290. doi:10.1016/S1473-3099(13)70692-3.
5. De Cock KM, El-Sadr WM. When to Start ART in Africa — An Urgent Research
Priority. N Engl J Med. 2013;368(10):886-889. doi:10.1056/NEJMp1300458.
6. UPdaTE Pr. Use of antiretroviral drugs for treating pregnant women and preventing
HIV infection in infants. WHO Geneva April. 2012.
http://www.who.int/entity/hiv/pub/pmtct_update.pdf. Accessed April 22, 2017.
7. Shapiro RL, Hughes MD, Ogwu A, et al. Antiretroviral regimens in pregnancy and
breast-feeding in Botswana. N Engl J Med. 2010;362(24):2282-2294.
doi:10.1056/NEJMoa0907736.
8. Bisio F, Nicco E, Calzi A, et al. Pregnancy outcomes following exposure to
efavirenz-based antiretroviral therapy in the Republic of Congo. New Microbiol.
2015;38(2):185-192.
9. Sibiude J, Mandelbrot L, Blanche S, et al. Association between prenatal exposure to antiretroviral therapy and birth defects: an analysis of the French perinatal cohort
study (ANRS CO1/CO11). PLoS Med. 2014;11(4):e1001635.
doi:10.1371/journal.pmed.1001635.
10. Phiri K, Hernandez-Diaz S, Dugan KB, et al. First trimester exposure to
antiretroviral therapy and risk of birth defects. Pediatr Infect Dis J.
2014;33(7):741-746. doi:10.1097/INF.0000000000000251.
11. Floridia M, Mastroiacovo P, Tamburrini E, et al. Birth defects in a national cohort
of pregnant women with HIV infection in Italy, 2001-2011. BJOG Int J Obstet
12. Ouattara EN, Anglaret X, Wong AY, et al. Projecting the clinical benefits and risks of using efavirenz-containing antiretroviral therapy regimens in women of
childbearing age. AIDS Lond Engl. 2012;26(5):625-634. doi:10.1097/QAD.0b013e328350fbfb.
TABLES
Table&1:&Group&Characteristics&
&& Preg/BF&Women&(n=3,437)& Other&Women&(n=2,173)& Men&(n=2,347)&
Characteristic&& !! !! !!
Age!(%)! !! !! !!
16*19! 11.1! 4.3! 2.1!
20*29! 60.0! 40.1! 20.7!
30*39! 27.7! 36.4! 46.8!
40*49! 1.1! 13.2! 21.0!
50*59! 0.0! 4.3! 6.4!
60!or!older! 0.0! 1.1! 2.2!
EFV*containing!regimen!(%)! 99.7! 89.8! 91.9!
WHO!Stage!(%)! !! !! !!
1! 97.8! 32.8! 18.8!
2! 2.1! 16.6! 19.2!
3! 0.0! 34.5! 41.2!
4! 0.1! 11.9! 18.3!
Current!TB!treatment! 0.6! 9.3! 18.2!
Mean!weight!(SD)!(kg)! 60.0!(10.0)! 55.2!(11.3)! 56.8!(9.0)! *Missing!group!data!for!0.40%!
Table!2.!Bivariable!comparisons!for!hepatic!toxicity!and!relevant!clinical!or! demographic!factors!
Comparison& Percent& PFvalue&
Hepatic!toxicity! && &&
!!!!by!Group! !! !!
Preg/BF!Women! 0.29!
0.02! Other!Women! 0.83!
Men! 0.55!
!!!!by!Age!category! !! !!
16*19! 0.57!
0.04! 20*29! 0.67!
30*39! 0.39! 40*49! 0.12!
50*59! 0!
60!or!older! 2.67!
!!!!by!ART!regimen! !! !!
EFV*based! 0.52!
0.59! non*EFV*based! 0.44!
!!!!by!TB!treatment! !! !!
Yes! 0.31! 0.34!
No! 0.53!
!! !! !!
Weight! Mean& PFvalue&
!!!!by!Group! !! !!
Preg/BF!Women! 60!
<0.01! Other!Women! 55.2!
Table&3.&Comparison&of&risk&of&hepatic&toxicity&across&group&categories&
Model!
Pregnant/Breastfeeding!
women!vs.!men! Other!women!vs.!men!!
OR!(95%!Confidence!
interval)! OR!(95%!Confidence!interval)!
Unadjusted!! 0.52!(0.23,!1.20)! 1.50!(0.73,!3.07)!
Fully!adjusted! 0.47!(0.16,!1.40)! 1.51!(0.71,!3.24)!
Final!model*!! 0.47!(0.16,!1.39)! 1.49!(0.70,!3.19)!
*Model!controls!for!age,!WHO!stage,!and!TB!treatment!
!
Table&4.&Comparison&of&risk&of&hepatic&toxicity&by&exposure&to&EFV&
Model!
EFV*based!vs.!non*EFV* based!ART! OR!(95%!Confidence!
interval)!
Unadjusted!! 1.17!(0.28,!4.86)!
Fully!adjusted! 0.98!(0.23,!4.16)!
Final!model*!! 0.99!(0.23,!4.19)!
*Model!controls!for!age,!group!status,!WHO!stage,!and!TB! treatment!