FROM ENGINEERING TO DENTISTRY: MANAGEMENT AND
APPLICATION OF TQM PRINCIPLES AND TOOLS AS A RESULT
LEVERAGE
ELIANA N. C. SILVA1; MARA T. SALLES1
1Professional Master in Management Systems
Laboratory of Technology, Business and Environment Management Fluminense Federal University
R. Passo da Pátria, 156/329-A, 24210-240-Niterói RJ, Brasil - (21) 2717-6390. e-mail: [email protected]; [email protected]
TQM is not new to industry and medicine. In dentistry, information on the topic is still insufficient. Our objective is to show tools that originate from industry, which are applied in dentistry with the intention of offering the Dental Surgeon conditions to improve performance in search of excellence in the practice.
1 - INTRODUCTION
Dentistry in the 20th century became more efficient due to great scientific and technological advances that revolutionized the practice of the professional DS (Dental Surgeon). Stating some of the inventions and techniques: the photoactive resins, which made esthetic restorations possible; micro-abrasion and laser for cavity tissue removal that can also be used for dental diagnosis and lightening; digital radiology with reduction of radiation and live image revelations on computer screens; the intra-oral camera, which, among other things, makes possible for the client/patient to accompany treatment at the time of performance.
Beyond all of this scientific and technological evolution, the challenge for the professional DS has been elevating considerably, these micro-entrepreneurs are increasingly under pressure: through globalization, which brought profound and irreversible changes in economics and in the behavior of people, through the market that demands reduction of costs and gains in efficiency, through the exasperated competition and the growing exigency of potential and final clients, and having these professionals, to find competitive differentials that guarantee long-term survival.
Nowadays, the importance of Quality, which initiated in the factory industry and is expanding, in large steps, and the service rendering sector, is no longer questionable, and it is this evidence that gives the spark in the actual competitive process in the dental segment, demanding that all are capacitated in tracing strategies and structured action plans in data and factual analysis, which will serve as a guide on the decisions on the resource and improved techniques application, to develop a system of modern management, that attends the needs and expectations of the client/patient and others.
This requires the identification of opportunities, the study of competition and market tendencies following a methodology. This is the reason why the introduction of TQM (Total Quality Management) techniques in a company, even if the company is a small service business like a dental office, is so important.
Total Quality Management in dentistry is equal to the sum of the technical quality of the professional plus the quality perceived by the client, through the knowledge and respect of their creed and values, seeking results with the strengthening of the existing credibility between the professional and the community. Credibility reached and sustained by continual learning and compromise with constant improvement.
That means that knowing everything about dentistry isn’t enough. For the professional, quality can have something to do with the technical-professional aspects, but for the client, quality has to do with their own level of personal satisfaction.
In the new competitive context, inside the dental segment, there is still little understanding of the true impact of a non-fundamental decision on information and focus analysis. The idea of working with management through the TQM concepts and tools is not disseminated.
2 - OBJECTIVE
The object of this article is to show some tools that originated from the factory industry, applied in day-to-day dentistry as information generating sources, that, combined with the implicit knowledge of the professional DS (dental surgeon) and assistant, and the interaction with the clients, will make possible the creation of knowledge, the incorporation to the rendered service, providing the Dental Surgeon and the learning organization with continuous improvement and innovation power, like in resources for performance sustaining and optimization in search of excellence in the practice.
3 –THEORETICAL ESTABLISHMENT
The dental office, even as a small service business, can be compared to a craft industry. The products for sale are the dental procedures that have the necessity of a logistic for the purchase of raw material and negotiation power with the supplier. The manager, besides updated techno-scientific abilities, should still create a competitive differential with the competitors, have professional competence to deal with client information, internal and external, resources and market, and knowledge of methodological practices that help in strategic decision making, through the analysis of information, statistical mapping, and raising of the processes/procedures, which will serve as a support augmenting the basis of knowledge. This article consists, mostly, in converting information into knowledge that makes possible the innovation in business administration to overcome the current challenges imposed to the practice of the dental profession and to maintain competitiveness. To create an environment where the innovating spirit and the undertaking becomes indispensable for a TQM-based strategy.
According to JURAN, the new superiority in planning is a consequence, in part, of the process capacity quantification use, becoming imperious to adopt quantification as a tool for the competition in Quality planning (design for quality).
The Quality function is a planning methodology, which integrates tools and technologies to put the whole organization aiming client satisfaction and company demand. It follows a systematic sequence, in a way to transform the clients’ needs into requirements, which can be integrated to the service development process.
David Kearns (1992), affirms that Total Quality Management and it’s diverse tools are indispensable assistants for professionals, independent of the practice area, which seeks excellence in the practice and searches client satisfaction through a service that attends, or even overcomes, expectations. The TQM practice does not seek an objective in it’s own context. It should be constantly perfected through training and development of new practices that associate value to the business, generating competitive advantage.
To GARVIN, companies that learn, like, Honda, Corning, and General Electric, use construction blocks, where one of the five pillars is the use of simple statistic tools (Pareto graphs, correlations, histograms, cause and effect or Ishikawa diagrams) to organize data and extract inferences. It affirms that “the managers have known for a long time that what is not measurable is not manageable.”
According to SVEIBY, to the “knowledge organization” it is very important that there is an interaction between information (transferring knowledge in an indirect form, making data and facts explicit), and tradition (transferring knowledge in a direct form, from person to person, learning by practice), among explicit knowledge and tacit. Tradition must be used to transfer knowledge.
DAVENPORT and PRUSAK, affirm that, while the organizations interact with the environment, absorbing and transforming information into knowledge, they start to act with basis on these concepts, combined with experiences, values, and internal rules.
Through the study realized between the 28th of October and the 15th of November 2001- in the application of 80 questionnaires for dentistry professionals in the city of Niterói, in the state of Rio de Janeiro, with the objective to identify the level of TQM knowledge, application, and interest, it was verified that there is a gap of knowledge that makes this segment work with tools and methodologies that lead to structured decisions in data analysis in the internal and external environment possible. Of the 80 interviewed, 85% showed interest in obtaining more information on the methodology, also in learning and using the tools to optimize their work.
4 – APPLICATION IN DENTISTRY
The demonstration of the two TQM tools that can be very useful in dentistry is pertinent. They are:
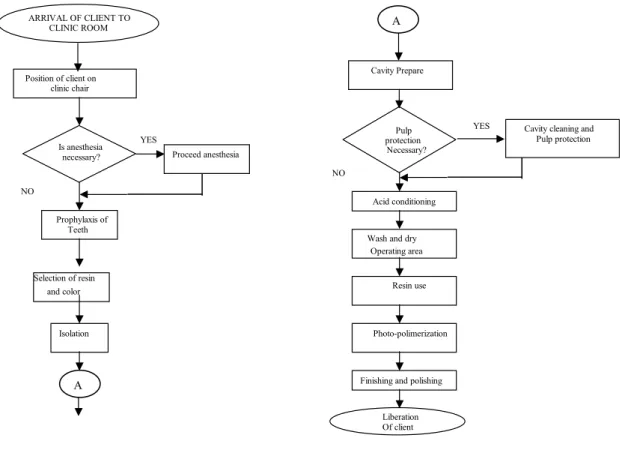
Flowchart - It is an illustrative summary of the various operations of a process, detailed in all of the involved steps. It may be better understood in Michael Brassard (1992).
In dentistry, the flowchart is an important tool for planning and also for perfecting processes, identifying the ideal current flow permitting critical analysis and alterations, also facilitating the visualization of the diverse linked steps, allowing to meet those that deserve greater attention, and still, facilitating the orientation/instruction of the professional assistant and other collaborators involved in the process.
In the day-to-day of the dentistry professional, the flowchart can be used for, for example, describing step-to-step the execution process of an esthetic restoration, from the client’s position on the clinic chair, to the final polishing of the restoration.
FIGURE 1 – Flowchart of Compound Resin Restoration Process
Cause and Effect or Ishikawa Diagram, is explained by Michael Brassard (1992) as a graphic technique that permits organizing information, identifying possible causes of a certain problem or effect, showing the principal causes of an action, leading to the final result.
In dentistry, it can be used with the finality of identifying the possible causes of a problem, obtaining better visualization of the cause and effect relation, diagnosing the causes that are originating an effect or problem. The causes can still be divided into sub-causes, facilitating the determination of specific actions for each one of them.
Example of a Flowchart in the Restoration Process with compound resin according to the adaptation of the operational tactic of Baratieri/Cols (1991) ARRIVAL OF CLIENT TO CLINIC ROOM Position of client on clinic chair Is anesthesia necessary? YES Proceed anesthesia NO Prophylaxis of Teeth Selection of resin and color Isolation Cavity Prepare Pulp protection Necessary?
YES Cavity cleaning and Pulp protection
NO
Acid conditioning
Wash and dry Operating area
Resin use
Photo-polimerization
Finishing and polishing
Liberation Of client
A
FIGURE 2 – Cause and Effect or Ishikawa Diagram. For the identification of possible causes of non-conformity levels in Anterior Esthetic Restorations type class V. 5 – PRACTICAL APPLICATION
The first initial case of TQM concept, tool, and application use began originally in a small organization – a private dental office in the State of Rio de Janeiro, Brazil.
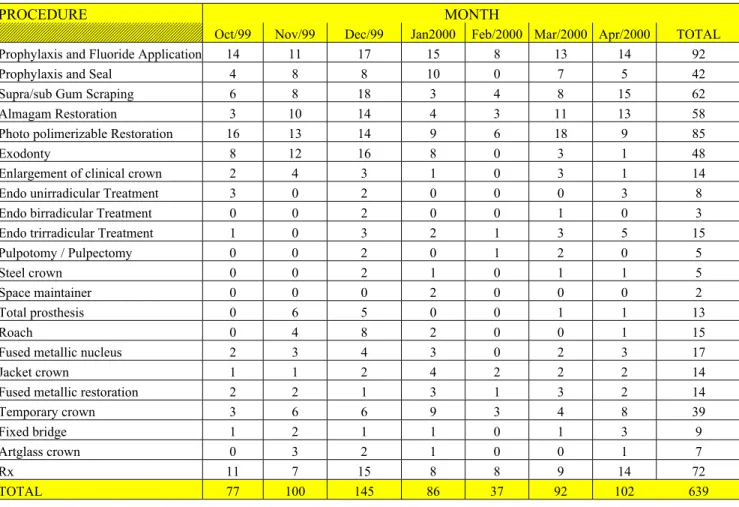
The data or sampling (frequency of dental procedure occurrences) were collected in a period of 7 months, from October 1999 to April 2000, to map dental procedures and factual analyses, with the goal to promote better distribution of grants spent on maintenance and acquisition of consumption materials, facilitating logistics, and consequentially raising the negotiation power with the suppliers.
The procedures were calibrated monthly with the help of a verification sheet adapted for the organization in question. With basis on the information in the verification sheet, from October to April, it was possible to construct a table, according to the proposed objectives, named the TABLE OF PROCEDURES PER PERIOD, where the processes/procedures are shown.
Inadequate resin because of Technical information insufficiency
Irregular resin package
Inadquate Lamps for office
illumination Absence of Natural illumination Change of Supplier and manufacturer
Not enough artificial Illumination to make Up absence of natural illumination
Reflector with inadquate lamp Inadquate illumination Compound Resin Color unstaisfactory nas restaurações estéticas de dentes s ant riores do tipo CLASSE V Photopolimerization Uncalibrated Photo polimizer Less light than
recomended o In application
Resin Tempurature
Distance and direction of light Source to the resin surface
Visual fat igue
Necessity to Recycle Selection of color
W ith dental element dehydrated Failure in selection of Restoration material Dental Surgeon Unsatisfactory color in the anterior esthetic tooth restorations class V
TABLE 1 – Table of Procedures per Period FREQUENCY OF DENTAL PROCEDURES
PROCEDURE MONTH
Oct/99 Nov/99 Dec/99 Jan2000 Feb/2000 Mar/2000 Apr/2000 TOTAL
Prophylaxis and Fluoride Application 14 11 17 15 8 13 14 92
Prophylaxis and Seal 4 8 8 10 0 7 5 42
Supra/sub Gum Scraping 6 8 18 3 4 8 15 62
Almagam Restoration 3 10 14 4 3 11 13 58
Photo polimerizable Restoration 16 13 14 9 6 18 9 85
Exodonty 8 12 16 8 0 3 1 48
Enlargement of clinical crown 2 4 3 1 0 3 1 14
Endo unirradicular Treatment 3 0 2 0 0 0 3 8
Endo birradicular Treatment 0 0 2 0 0 1 0 3
Endo trirradicular Treatment 1 0 3 2 1 3 5 15
Pulpotomy / Pulpectomy 0 0 2 0 1 2 0 5
Steel crown 0 0 2 1 0 1 1 5
Space maintainer 0 0 0 2 0 0 0 2
Total prosthesis 0 6 5 0 0 1 1 13
Roach 0 4 8 2 0 0 1 15
Fused metallic nucleus 2 3 4 3 0 2 3 17
Jacket crown 1 1 2 4 2 2 2 14
Fused metallic restoration 2 2 1 3 1 3 2 14
Temporary crown 3 6 6 9 3 4 8 39
Fixed bridge 1 2 1 1 0 1 3 9
Artglass crown 0 3 2 1 0 0 1 7
Rx 11 7 15 8 8 9 14 72
TOTAL 77 100 145 86 37 92 102 639
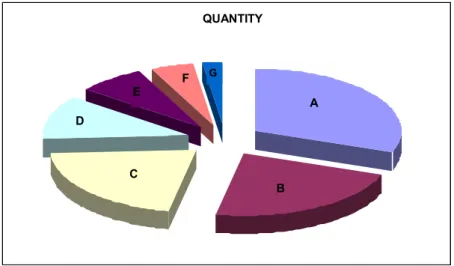
Table 2 presents the dental procedures, grouped and divided by codes from A to G, according to the practice area and organizational interest, permitting graphic representation.
TABLE 2 – Procedure Grouping by Codes
Code A Prevention Procedures Code B Restoring Procedures Code C Prosthetic Procedures Code D Radiological Procedures Code E Surgical Procedures Code F Endodontical Procedures Code G Individualized Surgical Procedures
Figure 3 graphically represents the distribution of the procedures.
FIGURE 3 – Graphic representation of the distribution of procedures
In figure 4 is used the Pareto diagram to identify the dental processes/procedures responsible for consumer behavior.
FIGURE 4 – Pareto Diagram
The diagram above shows, in decreasing order, that the code A, B, and C procedures are responsible for 74.18% of the consumer behavior.
QUANTITY B C D E F G A OBS.: A+B+C = 74.18% 11.27 7.51 4.85 2.19 22.38 21.13 30.67 0 50 100 150 200 250 A B C D E F G CODE Q U A N T I T Y 0.0 5.0 10.0 15.0 20.0 25.0 30.0 35.0 P E R C E N T A G E
6 – CONCLUSION AND SUGGESTIONS
According to the quality plan, by JURAN, we have parted from a goal, identifying the clients’ needs, followed by developing the service characteristics and procedure conformity, inside the quality standards, according to the budget planning. Lastly, establishing the procedure control following a systematic sequence in a way to transform the clients’ needs into requirements and these becoming an integrated part of the final service.
With basis on the mapping and analyses of facts and data (frequency of dental procedure occurrences), it was possible to prioritize with coherence and aligned to the budget proposal, the acquisition of consumption material (raw material) for the organization following a quality standard and service conformity.
In this article, the tacit knowledge of the professional Dental Surgeon orientated for procedure, based on the belief of external resource (TQM tools and methods application) use, combined with ability and experience, proceeding in social network, inside a culture that values learning and knowledge, was the answer to a more economic and balanced budget proposal, in a way to make the organization more competitive attending the clients’ exigencies and needs, inside a pre-established standard of quality and conformity.
The following described steps made possible a real experience, besides realizing interactive improvements to reach higher quality levels:
• Process identification and mapping – communicating and measuring;
• Participation, mobilization, and initiative development – people;
• Consolidation – operational integration;
• TQM monitoring and adjustments.
It is important to emphasize that the professional DS can use TQM tools to accompany processes, such as:
• Procedures – quantity produced, differentiation, performance, number of re-work (repetition), and motive;
• Client data – in relation to the preferences of time and service environment (with or without music, TV, etc.), of the materials used in treatment (esthetic – resins, porcelain, metals – gold, silver links), satisfaction, suggestions, complaints...
• Principal supplier data – price negotiations, form of payment, and punctuality of product delivery, equipment and/or medication;
• People – performance and satisfaction;
• Establish cost-benefit relation of the organization.
Each tool can and should be adapted to the reality of the organization and the information should be collected according to the proposed objectives. There is no such thing as a prewritten model, each organization will have to, parting from various analyses, create the ideal method to implant and manage the processes based on the quality methodology. In the TQM world, the existence of processes based on a matrix from one end of the organization to the other is indispensable so it could be well succeeded reaching competitive advantage.
The quality management and administration is not only a strategy, it is a working style, and therefore infinite.
BIBLIOGRAPHY
LOVELOCK, Christopher. Serviços - Marketing e Gestão. São Paulo: Ed. Saraiva. 2002.
JORNAL DA APCD – Associação Paulista de Cirurgiões Dentistas – Outubro de 2000 “Anais – Academia Brasileira de Odontologia – 469 p – Esdeva Empresa Gráfica S/A – Juiz de Fora, MG. 1974.
Revista do Conselho Regional de Odontologia do Rio de Janeiro. Ano XIX – nº 5, maio 2002.
NOGUEIRA, Luiz Carlos Lima. Gerenciando Pela Qualidade Total na Saúde. Fundação Christiano Ottoni, Belo Horizonte, MG, 1996.
JURAN, J.M., A Qualidade desde o projeto – Os Novos Passos para o planejamento da Qualidade em Produtos e Serviços; Livraria Pioneira Editora, São Paulo, 1992.
GARVIN, David. Construção da Organização que Aprende. In: GESTÃO do Conhecimento. Rio de Janeiro: Campos, 2000. p. 50 – 81.
SVEIBY, Karl Erik. A Nova Riqueza das Organizações: gerenciando e avaliando patrimônios de conhecimento. Rio de Janeiro: Campos. 1998.
DAVENPORT, Thomas H.; PRUSAK, Laurence. Conhecimento Empresarial: como as organizações gerenciam o seu capital intelectual. Rio de Janeiro: Editora Campus, 1998.
NONAKA, Ikujiro e TAKEUCHI, Hirotaka. The Knowledge-Creating Company. New York: Oxford University Press, 1995.
BARATIERE. Cols – Dentística – Procedimentos Preventivos e Restauradores. Rio de Janeiro: Livraria Editora Santos 1991.