Original Research Article
Occupational hazards and public health concerns of migrant
construction workers: an epidemiological study in southern India
C. J. Nirmala, S. Dharaneesh Prasad*
INTRODUCTION
The construction sector is an important sector of economy and contributes significantly to GDP. According to the NSSO estimates, 370 million workers constituted 92% of the total unorganised workforce in the country. In India, it is the largest economic activity after agriculture and since it is a labour-intensive industry consist 44% of all urban unorganized workers.1-3 This work force comprises 55% of unskilled labour, 27% skilled labour and rest the technical and support staff.2
Construction workers are at a greater risk of developing certain health disorders and sickness than workers in many other industries.4 They are exposed to multiple physical, chemical and biological agents, which make them vulnerable to various health problems that include - injuries, respiratory problems, dermatitis, musculo-skeletal disorders and gastro-intestinal diseases.2,5 The work is hard physical labour, often under difficult conditions like adverse weather conditions and the nature of work, hours of work, low pay, poor living conditions with lack of basic amenities and separation from family,
ABSTRACT
Background: Construction industry is one of the stable growing industries of the world and construction labour form 7.5% of the world labour force. In India, it is the largest economic activity after agriculture. Migrant construction workers are at a greater risk of developing certain health disorders and sickness than workers in many other industries. The objective was to study the socio demographic profile, morbidity profile among construction workers.
Methods: A cross sectional study conducted at two construction sites in southern Bangalore and all workers were enrolled as study subjects. Data was collected using a pretested semi structured questionnaire. Statistical analysis used: descriptive statistics like percentages and Chi square test for test of significance.
Results: Majority of the study population belonged to 15-45 years age group (87.3%), class IV (40.3%) socioeconomic status, Hindu religion (85%). Around 40% of them were illiterates and 68% of them were unskilled workers, rest semiskilled workers. Around 50% were from Raichur district of North Karnataka. Prevalence of injury was 8%, musculo-skeletal problems were around 50% followed by respiratory infections and gastrointestinal infections.
Conclusions: The prevalence of musculoskeletal problems, respiratory problems and gastrointestinal infections was reported to be high among unskilled and semiskilled construction workers. There is need for health education and other prevention strategies for control of the same. Measures are needed to improve the work environment of construction workers by ensuring availability of personal protective equipments, good living conditions and sanitation facilities at the sites.
Keywords: Occupational hazard, Migrant workers, Morbidity
Department ofCommunity Medicine, BGS Global Institute of Medical Sciences, Bangalore, Karnataka, India
Received: 07 December 2018
Accepted: 11 January 2019
*Correspondence:
Dr. S. Dharaneesh Prasad,
E-mail: [email protected]
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
lack of job security and lack of access to occupational health services make the situation worse.1,5,6 In the era of globalization construction is a fast growing industry and very little research has been done on the occupational health, hazards and psychosocial problems of these workers. In this context to understand the health problems, the morbidity profile among the construction workers and to enable appropriate interventions, this study was conducted.
Objectives
To study the socio demographic profile and morbidity profile among construction workers.
METHODS
This is a cross-sectional study carried out at two construction sites in Bangalore south during July- October 2015. Study was started after taking permission from Institutional ethical committee and concerned authorities at construction sites. All the migrant workers who were semiskilled and unskilled were enrolled for the study and included 315 subjects. The skilled, technical and support staffs were excluded. The job categories included manual labours, earth workers, landscaping, digging, paving, masonry, cement workers, cement mixing, concrete pumping, concreting (unskilled) and scaffolding, cutter, jack span cleaning, carpenting, painting, plumbing, pipeline fitting, rod bending, steel fixing, welding, barb making, lift/crane operating (Semiskilled).6
Data was collected in a pre-tested and semi structured questionnaire. General information like age, sex, religion, native place, education, marital status, information regarding migration i.e. reasons and duration of migration, working condition, injury during past 1 year, facilities available at working place, morbidity history, chronic illness, and hospitalization were included in the proforma. The height and weight was measured by a validated instrument using standard procedures. During medical examination, they were asked about their present health problems and physical examination was done and findings recorded. Those requiring medications were given free drugs and referrals were given.
The following operational definitions were used for the study. An “unskilled worker” is one who possesses no special training and whose work involves the performance of the simple duties that require the exercise of little or no independent judgment or previous experience, although a familiarity with the occupational environment is necessary.6 A “semi skilled worker” is one who has got some knowledge and skills of the particular trade or to do respective work and simple job with the help of simple tools or machines and not under gone any formal training course. A person staying in the study area for 5 yrs or less was considered to be a “Migrant”.
All the collected data was coded and entered in Excel data sheet and Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) version 16.0. Prevalence was reported in percentages. Chi square test was performed to find the statistical significance. Significance level was defined as p<0.05.
RESULTS
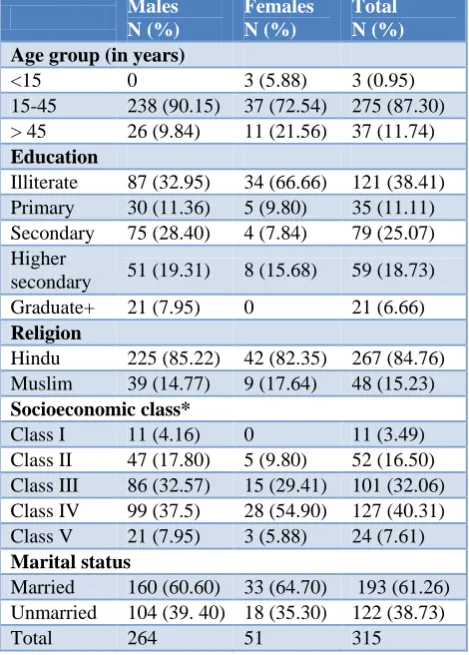
Data was collected from 315 workers. All of them were migrant workers. Most of them belonged to 15-45 year age group (87.3%), but three of them were below the age of 15 years. Majority were illiterates (38.5%), belonged to class IV (40.3%) and were Hindus (85%) followed by Muslims (Table 1).
Table 1: Sociodemographic profile of the study subjects.
Males N (%)
Females N (%)
Total N (%)
Age group (in years)
<15 0 3 (5.88) 3 (0.95) 15-45 238 (90.15) 37 (72.54) 275 (87.30) > 45 26 (9.84) 11 (21.56) 37 (11.74)
Education
Illiterate 87 (32.95) 34 (66.66) 121 (38.41) Primary 30 (11.36) 5 (9.80) 35 (11.11) Secondary 75 (28.40) 4 (7.84) 79 (25.07) Higher
secondary 51 (19.31) 8 (15.68) 59 (18.73) Graduate+ 21 (7.95) 0 21 (6.66)
Religion
Hindu 225 (85.22) 42 (82.35) 267 (84.76) Muslim 39 (14.77) 9 (17.64) 48 (15.23)
Socioeconomic class*
Class I 11 (4.16) 0 11 (3.49) Class II 47 (17.80) 5 (9.80) 52 (16.50) Class III 86 (32.57) 15 (29.41) 101 (32.06) Class IV 99 (37.5) 28 (54.90) 127 (40.31) Class V 21 (7.95) 3 (5.88) 24 (7.61)
Marital status
Married 160 (60.60) 33 (64.70) 193 (61.26) Unmarried 104 (39. 40) 18 (35.30) 122 (38.73)
Total 264 51 315
*Socioeconomic class according to modified B. G. Prasad’s classification.
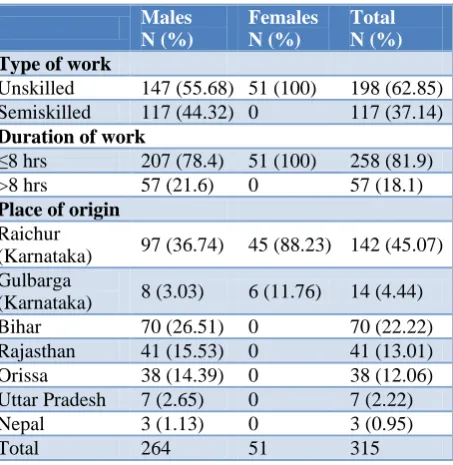
Majority of the workers (68%) were unskilled, rest semiskilled workers. Around 50% were from Raichur district of north Karnataka, 22% from Bihar and 13% from Rajasthan (Table 2). Reasons for migration included lack of job opportunities and financial reasons.
There was no statistical significant association between type of work, duration of work with morbidity status (Table 4).
Around 70% of the sick had taken treatment and the rest had not taken mainly because of financial reasons and time constraints. Around 65% had visited doctor and 35% had taken treatment from pharmacy. Around 14% were hospitalized in the past 1 year and around 5% were suffering from chronic illness.
Table 2: Distribution of study subjects according to type of work and place of origin.
Males N (%)
Females N (%)
Total N (%)
Type of work
Unskilled 147 (55.68) 51 (100) 198 (62.85) Semiskilled 117 (44.32) 0 117 (37.14)
Duration of work
≤8 hrs 207 (78.4) 51 (100) 258 (81.9) >8 hrs 57 (21.6) 0 57 (18.1)
Place of origin
Raichur
(Karnataka) 97 (36.74) 45 (88.23) 142 (45.07) Gulbarga
(Karnataka) 8 (3.03) 6 (11.76) 14 (4.44) Bihar 70 (26.51) 0 70 (22.22) Rajasthan 41 (15.53) 0 41 (13.01) Orissa 38 (14.39) 0 38 (12.06) Uttar Pradesh 7 (2.65) 0 7 (2.22) Nepal 3 (1.13) 0 3 (0.95)
Total 264 51 315
Table 3: Morbidity profile of the study subjects.
Morbidity Total N (%)
Skin problems 10 (3.17)
Fever 42 (13.33)
Gastrointestinal problems 54 (17.14)
Injuries 24 (7.61)
Accidents 6 (1.90)
Respiratory infections 81 (25.71)
Urinary infections 16 (5.07)
Ophthalmological problems 30 (9.52)
Musculoskeletal problems 153 (48.57)
Hear problems 12 (3.80)
Head ache 48 (15.23)
Asymptomatic 60 (19.04)
Around 55% of the workers reported that they were satisfied with their living conditions, 60% reported that they were satisfied with their Job and 57% reported that they received social support from family. Personal protective equipments were used constantly only in 65% and the rest did not use because it was not comfortable and sometimes obstructs from work. Around 90% of them were not covered under any social insurance. Around 5% were found to be hypertensive and 25% had pallor. On examination, apthous ulcers, fungal infections, redness of the eyes, skin rashes, teeth discoloration, toe nail infections, tenderness in the joints were the common findings.
Table 4: Association between variables and health status of the study subjects.
Parameter Morbidity Chi square P value
Present Absent
Type of work Unskilled 156 442 1.61 0.1
Semiskilled 99 18
Duration of work ≤8 hrs 207 51 0.47 0.24
>8 hrs 48 9
DISCUSSION
The construction workers are exposed to multiple risks at working and living places. They are exposed to physical, chemical, biological, ergonomic hazards, environmental and psycho social risks.2,6 In most places the workers reside in make shift camps inside the project sites that expose them to health risks even after working hours. Due to poor environmental conditions at work sites chances of diseases from poor sanitation and unsafe drinking water are high.2,5,6
Construction workers have got an attributable risk of 50% for musculo-skeletal injuries, higher than all other workers.3,7 Postural changes like bending forward or standing and weight bearing may cause backache, low
breathing difficulties similar to earlier reports, which may be exaggerated by lack of personal protective measures such as, using mask, work practices like wet grinding and overcrowding.3
Occupational safety hazards in construction work occur due to poorly designed ladders, unsuitable or poorly maintained lifting appliances, improper material handling, improper walking surfaces, high platforms, improperly shored trenches, badly maintained tools and inadequate illuminations.3 Construction work accidents contribute to 16.4% of fatal global occupational accidents.2 Relative risk of accidents in Indian construction industry were 8 compared to other manufacturing sector and fatal accident frequency rate was 15.8 incidents/1000 employees/year.3,5 An operational study on accidents in construction industry reported that problems arising from workers were 70%, workplace issues 49%, shortcomings with equipment 56% and deficiencies with risk management (84%).11 In our study, around 8% had sustained work-related accident/injury during last 1 year. Poor language skills prevent them from understanding the safety precautions given and to follow the instructions given by supervisors. The prevalence of injuries in previous studies were 7.9%, 7.56%, 6.6% and 25.42% respectively.6,5,10,12 The reduction may be attributed to increased mechanization and good work practices. They were also less literate, which make them less aware of accident risks and precautions to be taken. Owing to their working in heights on moving cranes, unstable walking surfaces and probably poor illumination, the frequency of accidents were higher among building workers. More of mechanized work and on-site periodic safety induction training and practice may reduce the accidents.12
The absence of recreational facilities, the nature of work, hours of work, low pay, poor housing and separation from family, lack of job security and lack of access to occupational health services cause anxiety in these workers.2,5
CONCLUSION
The prevalence of musculoskeletal problems, respiratory problems and injury were reported to be high among unskilled and semiskilled construction workers. Those workers with severe morbidity may leave the job and due to the “healthy worker effect” the results may be an under reporting. This can cause high morbidities associated with them. There is an urgent need for health education and other prevention strategies for control of the same. Measures are needed to improve the work environment of construction workers by ensuring availability of personal protective equipments, good living conditions and sanitation facilities at the sites. There should be a health facility which is easily accessible to the health workers. A system of health recording and routine surveillance of construction workers has to be set up. Local medical colleges and occupational health institutes should be
encouraged to study the health of construction workers and better their health status in order to keep their working abilities efficient. Migrant workers form an important proportion of unorganised sector and due to their vulnerability to health problems are to be covered under social security measures.
ACKNOWLEDGEMENTS
Head of the Institution, BGS-Global Institute of Medical Sciences, Builders and Construction Workers.
Funding: No funding sources Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committee
REFERENCES
1. Shah KR, Tiwari RR. Occupational skin problems in construction workers. Indian J Dermatol. 2010;55:348-51.
2. Kulkarni GK. Construction industry: More needs to be done. Indian J Occup Environ Med. 2007;11:1-2. 3. Tiwary G, Gangopadhyay PK. A review on the
occupational health and social security of unorganized workers in the construction industry. Indian J Occup Environ Med. 2011;15:18-24. 4. Taimela S, Laara E, Malmivaara A, Tiekso J,
Sintonen H, Justen S, et al. Self-reported health problems and sickness absence in different age groups predominantly engaged in physical work. Occup Environ Med. 2007;64:739-46.
5. Gurav RB, Kartikeyan S, Wayal R, Joshi SD. Assessment of daily wage labourers. Indian J Occup Environ Med. 2005;9:115-7.
6. Adsul BB, Laad PS, Howal PV, Chaturvedi RM. Health problems among migrant construction workers: A unique public-private partnership project. Indian J Occup Environ Med. 2011;15:29-32.
7. Schneider SP. Musculoskeletal injuries in construction: A review of the literature. Appl Occup Environ Hyg. 2001;16:1056-64.
8. Bodhare T, Valsangkar S, Bele S. An epidemiological study of work-related musculoskeletal disorders among construction workers in Karimnagar, Andhra Pradesh. Indian J Community Med. 2011;36:304-7.
9. Mohopatra R. Occupational health hazards in small scale and other industries. In: Mohopatra R, editor. Occupational Health Hazards and Remedies. 1st ed. New Delhi: Jaypee Brothers Medical Publishers Pvt. Ltd.; 2002: 54-55,203-204.
10. Jayakrishnan T, Thomas B, Rao B, George B. Occupational health problems of construction workers in India. Int J Med Public Health. 2013;3:225-9.
construction accidents. Appl Ergon. 2005;36:401-15.
12. Shah CK, Mehta H. Study of injuries among construction workers in Ahmadabad city, Gujarat. Indian J Pract Doct. 2009;5:4-8.