ARTICLE
A Randomized, Controlled Trial of Removable
Splinting Versus Casting for Wrist Buckle Fractures in
Children
Amy C. Plint, MDa,b, Jeffrey J. Perry, MD, MScb, Rhonda Correll, BScNc, Isabelle Gaboury, MScd, Louis Lawton, MDe
Departments ofaPediatrics,bEmergency Medicine, andeSurgery, University of Ottawa, Ottawa, Ontario, Canada;cDivision of Emergency Medicine anddChalmers Research Group, Children’s Hospital of Eastern Ontario Research Institute, Ottawa, Ontario, Canada
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.Wrist buckle fractures are a frequent reason for emergency department visits. Although textbooks recommend 2 to 4 weeks of immobilization in a short arm cast, management varies. Treatment with both casts and splints is common, and length of immobilization varies. The objective was to determine if children with distal radius and/or ulna buckle fractures treated with a removable splint have better physical functioning than those treated with a short arm cast for 3 weeks.
METHODS.This was a randomized, controlled trial in the emergency department of an academic, tertiary care children’s hospital. Participants were children 6 to 15 years of age with distal radius and/or ulna buckle fractures who were randomly assigned to treatment with a short arm cast for 3 weeks or a removable splint. Cast removal was at 3 weeks. A validated self-reported outcome tool, the Activities Scales for Kids performance version (ASKp), was used to measure physical functioning over a 4-week period. The main outcome was the ASKp score at 14 days postinjury.
RESULTS.We randomly assigned 113 patients, and 87 were included in the final analysis: 42 in the splint group and 45 in the cast group. Study groups were similar in age, gender, bone fractured, and dominant hand injured. There were significant differences in ASKp score at day 14 and change in ASKp from baseline at days 14 and 20, indicating better functioning in the splint group. Splinted children had less difficulty with bathing throughout the entire study. There were no significant differences in pain between groups as measured by visual analog scale. There were no refractures.
CONCLUSIONS.Children treated with removable splinting have better physical func-tioning and less difficulty with activities than those treated with a cast.
www.pediatrics.org/cgi/doi/10.1542/ peds.2005-0801
doi:10.1542/peds.2005-0801
This work was presented in abstract form at the annual meetings of the Society for Academic Emergency Medicine; May 16 – 19, 2004; Orlando, FL; the Canadian Association of Emergency Physicians; May 26 –30, 2004; Montreal, Quebec; and the Pediatric Academic Societies Meeting; May 1– 4, 2004; San Francisco, CA
Key Words
children, fracture, radius, ulna, treatment
Abbreviations
ED— emergency department ASKp—Activities Scales for Kids performance version VAS—visual analog scale
Accepted for publication Jul 5, 2005
Address correspondence to Amy Plint, MD, Division of Emergency Medicine, Children’s Hospital of Eastern Ontario, 401 Smyth Ave, Ottawa, Ontario, Canada K1H 8L1. E-mail: [email protected]
B
UCKLE FRACTURES OFthe distal radius and ulna are a common form of wrist fracture in children and a frequent reason for emergency department visits. When a child sustains a buckle fracture, the bony cortex is compressed on one side and the opposite cortex remains intact.Although standard orthopedic texts suggest 2 to 4 weeks of treatment in a short arm cast,1,2a recent
cross-Canada survey of pediatric emergency physicians and pediatric orthopedic surgeons found variability in both the type and length of immobilization and in the belief in need for immobilization.3 Although North American
preference seems to be casts for immobilization,1,3,4
sev-eral studies from Britain have suggested that treatment with splints is more common.5–7 Immobilization with a
splint seems to be well tolerated.5–7One study compared
3 weeks of continuous immobilization with a splint to the 3 weeks with a cast but did not examine in detail the effect of such management on a child’s daily physical functioning.6
Although no studies have been published examining the impact of casting on a patient’s quality of life, it is not unreasonable to assume that a cast results in limited mobility and, if not truly necessary for injury manage-ment, results in unnecessary morbidity. No study has compared the use of a removable splint (ie, removed at patient’s discretion) to casting in this patient population. Furthermore, the need for follow-up for cast removal represents a burden to the family, as well as the health care system. The objective of this study was to compare the daily physical functioning of children with buckle fractures of the distal radius and/or ulna who are treated with a removable splint to those treated with a cast.
METHODS
Study Design
This randomized, controlled trial compared the physical functioning of children with wrist buckle fractures treated with removable splinting to those treated with short arm casts.
Study Setting and Population
This trial was performed between August 2002 and Sep-tember 2003 at the Children’s Hospital of Eastern On-tario, an academic, tertiary care children’s hospital in Ottawa, Ontario, Canada with an annual emergency department (ED) census of 55 000/year. Children aged 6 to 15 years were eligible for inclusion if they presented to the ED with a buckle fracture of the distal radius or ulna. A buckle fracture was defined as compression of the bony cortex with the opposite cortex intact and confirmed by a pediatric radiologist. Children who had another fracture of the same limb requiring immobiliza-tion, fractures of both wrists, evidence of metabolic bone disease, a language barrier, or who lived outside the hospital catchment area were not included. Written,
informed consent and assent was obtained from parents and patients. Our institutional research board approved this study.
Study Protocol
Children were randomly assigned to receive either a short arm (below elbow) plaster cast or an individually fitted plaster splint (composed of 12 plaster layers) that attached with a tensor bandage. A plaster splint was chosen instead of a preformed commercially available splint to reflect the reality of available materials at many hospitals. The randomization sequence was computer-generated with a block size of 4. Initially, a Web-based allocation program was used for group allocation. How-ever, because of problems with timely access to the program, sealed opaque envelopes containing the group assignment were used from November 2003 onward. The research assistant accessed either the Web-based allocation program or used the next envelope to deter-mine to which group the patient was assigned. After random assignment, baseline data and study measure-ments were recorded. The intervention was applied by the research assistant or by the ED medical staff (and monitored by the research assistant). The emergency physician who referred the patient to the study made the initial diagnosis of buckle fracture. Research assistants were available 12 to 16 hours/day. Some patients were recruited when a pediatric radiologist was not available to immediately review the patient films (eg, on week-ends and evenings), but all of the radiographs were reviewed by a pediatric radiologist within 24 hours. We decided a priori to withdraw patients from the study who were subsequently determined to have a fracture other than a buckle fracture. Among these patients, those who had been randomly assigned to a cast re-mained in a cast, whereas those who were randomly assigned to a splint had their treatment changed to a cast.
with daily living and sporting activities, amount of splint use, and difficulties with cast or splint. All of the families were also provided with stamped, self-addressed enve-lopes to return the study materials in an effort to mini-mize lost data. All of the patients were asked to return to the orthopedic clinic at 21 days after injury for assess-ment and cast removal. At 6 months, families were contacted by phone (and hospital charts reviewed) to determine refractures.
Measurements
Baseline measurements at the time of enrollment in-cluded age, gender, mechanism of injury, hand domi-nance, pain score, and ASKp score. Baseline ASKp was determined by having the child consider their activities in the few days before sustaining their fracture.
The primary outcome measure was the ASKp at 14 days. The ASKp is a validated, self-report measurement of childhood physical disability, includes the perspective of children, was developed specifically for children with physical limitations because of musculoskeletal disor-ders, and has excellent reliability.8The ASKp is scored
out of 100 with a higher score reflecting higher physical functioning. The original ASKp consists of 30 questions and examines the child’s physical functioning in the week before completing the questions. For this study, we used a slightly modified version of the ASKp. It included 8 extra questions (added by the original developer of the ASKp) that captured functioning specifically related to the upper extremity, and the questions asked about activities in the previous “few days” rather than previous week. We chose ASKp at day 14 postinjury, because we believed that by this time children with buckle fractures might have minimal or no pain. As a result, we antici-pated that children in the splinting group might be using their splint less and have better functioning than those in the cast group. Because previous studies have shown that the median ASKp score correlates well with global level of disability, this score was felt to be more mean-ingful to clinicians than change in ASKp score. When children are considered to have normal functioning, the median ASKp score is 95 and children with mild, mod-erate, and severe levels of disability have median ASKp scores of 90, 59, and 26, respectively.8,9
Other outcomes included ASKp score at days 7, 20, and 28 postinjury; change from baseline in ASKp at days 7, 14, 20, and 28; pain; ability to perform daily and sporting activities throughout the study; length of splint use; parent and child satisfaction at day 28; and refrac-ture at 6 months. Pain was measured by using a visual analog scale (VAS, a 100-mm line anchored at one end with a label stating “no pain” and at the other end a label stating “worst pain”). The clinically important change for a VAS is considered to range from 10 to 15.10–12Ability to
perform daily activities was measured using a 4-point Likert scale. Children (or their parents for younger
chil-dren) were asked to rate their level of difficulty as none, mild, moderate, and severe in 5 areas of daily activities (printing/writing, drawing, feeding themselves, groom-ing [such as brushgroom-ing hair/dressgroom-ing], and bathgroom-ing/show- bathing/show-ering). Participants were asked whether or not they had returned to their normal sporting activities by days 7, 14, 20, and 28. Those in the splint group were asked to describe their splint usage using a 4-point Likert scale (always, most of the time, some of the time, and not at all) and, if relevant, the date that they had last used their splint.
Sample Size
Because ⬃30 points separate the median ASKp scores for children with disability classification of mild, moder-ate, and severe,8,9a minimal clinically important
differ-ence of 15 was chosen to avoid missing significant dif-ferences between groups. Moreover, an earlier study suggested that patients with casted upper extremity frac-tures would score in the moderate disability range.13
Therefore, sample-size calculations were based on the following assumptions: (1) to detect a difference of 15 units on the ASKp scale; (2) SD of 24 units8; (3) 2-sided
test; and (4) a power of 80% and false-positive (type I error) rate of 0.05. With these assumptions, the sample size was 81 children, to which we added 15% for poten-tial loss to follow-up, for a sample size of 113 children.14
Statistical Analysis
Because of skewness of the data, a nonparametric Wil-coxon Mann-Whitney test was used to compare ASKp and pain scores at days 7, 14, 20, and 28 postinjury. Study groups were compared for change from baseline of the ASKp scores using the Student ttest. The differ-ence in ordered categorical outcomes, such as ability to perform daily activities (rated on a Likert scale), was assessed with Wilcoxon Mann-Whitney test. Fisher’s ex-act tests were used to contrast the 2 study groups in terms of the child’s capacity to return to his/her normal playing and sporting activities at days 7, 14, 20, and 28. All of the reported P values are 2-sided and were de-clared statistically significant when they reached P ⫽ 0.05. All of the patients entered in the study as per protocol were included in this analysis.15All of the data
RESULTS
Patient Recruitment and Baseline Characteristics
Two hundred twelve children were diagnosed by the ED physicians with wrist buckle fractures during the time the study nurses were available, and 113 were randomly assigned (Fig 1). Eighty-seven children were included in the final analysis. Enrolled patients were similar in both the splint and the cast groups with respect to age, gen-der, mechanism of injury, dominant hand injured, bone fractured, baseline ASKp score, and VAS score (Table 1).
ASKp and Pain Scores
ASKp scores, pain scores, and differences in scores with their 95% confidence intervals16are presented in Table
2. Patients in the splint group had a significantly higher ASKp score at day 14 postinjury than the cast group (P ⫽.041). ASKp score was not significantly different be-tween the groups for days 7, 20, and 28 postinjury. The change in ASKp score from baseline was significantly different at days 14 and 20 postinjury between the splint and cast group, with the splint group showing better functioning than the cast group. There was no significant difference in VAS score between groups at any time during the study.
Ability to Perform Daily Activities and Sporting/Physical Play Activities
Splinted children had significantly less difficulty with bathing and showering at days 7, 14, and 20 postinjury than casted children (P ⬍.001). Splinted children also had less difficulty with printing/writing (P ⫽ .005),
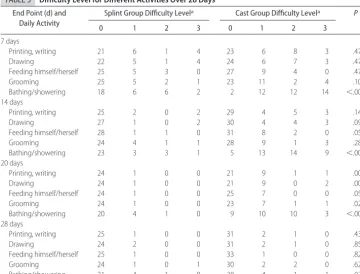
drawing (P⫽.005), and grooming (P⫽0.023) at day 20, although these differences do not remain significant af-ter Bonferroni adjustment for multiple testing. There were no other significant differences between groups at days 7, 14, 20, and 28. These results are given in detail in Table 3. More children in the splinted group were able to return to their regular sporting/physical play activities by days 20 and 28 postinjury (18 of 25 vs 13 of 32 [P ⫽ .031] and 25 of 26 vs 23of 34 [P⫽.008], respectively).
FIGURE 1
Flow of patients through the study.aOne child withdrew immediately after random assignment, 2 children with-drew within 24 hours, and 1 withwith-drew at day 7. Of the 2 children who withdrew within 24 hours, the families did not have problems with the splints but after enrolling decided that they did not want to participate in the study. The child who withdrew at day 7 reported no problems with the splint but no longer wished to partic-ipate in the trial follow-up.bPatient for whom no fol-low-up is available.
TABLE 1 Baseline Characteristics Characteristic Splint Group
(n⫽42)
Cast Group (n⫽45)
Age, y
Mean (SD) 9.48 (2.66) 9.94 (2.07)
Range (5.12–14.17) (5.87–13.65)
Male,n(%) 30 (71.4) 27 (60.0)
Dominant hand injured,n(%) 22 (52.4) 21 (46.7)
Mechanism of injury,n(%)
Fall 35 (83.3) 43 (95.6)
Direct blow 7 (16.7) 2 (4.4)
Radius injured,n(%) 42 (100) 45 (100)
Minor fracture 26 (61.9) 22 (48.9)
Moderate fracture 16 (38.1) 23 (51.1)
Ulna injured,n(%)a 5 (11.9) 2 (4.4)
Minor fracture,n 5 2
Moderate fracture,n 0 0
Time since injury (range), d 0.0 (0–7) 1.0 (0–7)
ASKp score, median (interquartile range)
93.01 (83.45–98.66) 96.98 (89.08–100.00)
VAS score, median (interquartile range)
49.0 (23.38–65.00) 38.5 (22.75–61.00)
Complications
Five children in the cast group returned to the ED for problems with their casts (4 returned for wet casts and 1 had placed a pencil under the cast). No children in the splint group returned to the ED for problems with their splint. At 6 months, telephone follow-up was available for 34 patients in the splint group and 41 in the cast group. No family reported that their child had a refrac-ture. We also reviewed all of the enrolled patient
hospi-tal charts at 6 months, and no refractures were docu-mented.
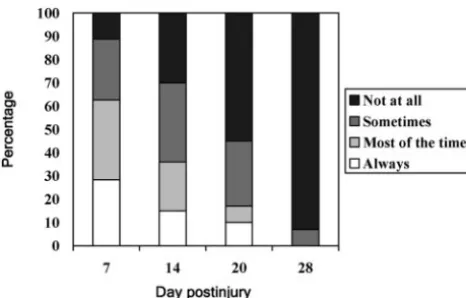
Length of Immobilization and Satisfaction
Children in the splint group wore their splints for at least some part of the day/night for an average of 13.7 days (SD ⫾6.0). Children were also asked to describe their splint use, and continuous use of the splint rapidly de-clined (Fig 2). Parents and children were asked at day 28
TABLE 2 ASKp Score, Change in ASKp, and VAS Score Over 28 Days
Outcome Splint Group Cast Group Difference Between
Study Groups, Median (IQR) P
na Median (IQR) na Median (IQR)
ASKp score
Day 7 38 83.48 (75.67 to 93.37) 44 88.67 (78.02 to 92.98) ⫺2.70 (⫺8.44 to 2.41) .331
Day 14 38 93.77 (87.26 to 99.15) 45 89.29 (82.33 to 95.69) 2.97 (0.00 to 6.90) .041
Day 20 34 96.55 (92.45 to 100.00) 40 93.97 (85.66 to 98.06) ⫺1.72 (⫺0.31 to 5.31) .091
Day 28 28 99.04 (95.29 to 100.00) 37 99.11 (96.42 to 100.00) 0.00 (⫺2.13 to 0.86) .934
Change from baseline ASKp score
Day 7 38 ⫺8.42 (15.74)b 43 ⫺7.83 (14.82)b ⫺0.59 (⫺7.35 to 6.18) .863
Day 14 38 1.04 (11.97)b 44 ⫺4.83 (13.33)b 5.87 (0.27 to 11.48) .040
Day 20 34 4.21 (10.96)b 39 ⫺3.41 (10.80)b 7.62 (2.53 to 12.71) .004
Day 28 28 7.10 (11.42)b 37 3.96 (13.25)b 3.14 (⫺3.12 to 9.39) .320
VAS score
Day 7 30 14.50 (2.75 to 35.00) 37 7.00 (0.00 to 23.00) 4.00 (0.00 to 14.00) .092
Day 14 29 1.00 (0.00 to 6.50) 37 1.00 (0.00 to 12.00) 0.00 (⫺2.00 to 0.00) .768
Day 20 27 0.00 (0.00 to 1.00) 38 0.00 (0.00 to 1.00) 0.00 (0.00 to 0.00) .926
Day 28 18 0.00 (0.00 to 0.00) 25 0.00 (0.00 to 0.50) 0.00 (0.00 to 0.00) .096
IQR indicates interquartile range.
aSample size varies, because follow-up was not available for all patients at every time point in the study. bMean (SD).
TABLE 3 Difficulty Level for Different Activities Over 28 Days End Point (d) and
Daily Activity
Splint Group Difficulty Levela Cast Group Difficulty Levela P
0 1 2 3 0 1 2 3
7 days
Printing, writing 21 6 1 4 23 6 8 3 .472
Drawing 22 5 1 4 24 6 7 3 .479
Feeding himself/herself 25 5 3 0 27 9 4 0 .477
Grooming 25 5 2 1 23 11 2 4 .107
Bathing/showering 18 6 6 2 2 12 12 14 ⬍.001
14 days
Printing, writing 25 2 0 2 29 4 5 3 .140
Drawing 27 1 0 2 30 4 4 3 .097
Feeding himself/herself 28 1 1 0 31 8 2 0 .058
Grooming 24 4 1 1 28 9 1 3 .280
Bathing/showering 23 3 3 1 5 13 14 9 ⬍.001
20 days
Printing, writing 24 1 0 0 21 9 1 1 .005
Drawing 24 1 0 0 21 9 0 2 .005
Feeding himself/herself 24 1 0 0 25 7 0 0 .056
Grooming 24 1 0 0 23 7 1 1 .023
Bathing/showering 20 4 1 0 9 10 10 3 ⬍.001
28 days
Printing, writing 25 1 0 0 31 2 1 0 .438
Drawing 24 2 0 0 31 2 1 0 .852
Feeding himself/herself 25 1 0 0 33 1 0 0 .829
Grooming 24 1 0 1 30 2 2 0 .626
Bathing/showering 21 4 1 0 28 4 1 1 .921
if they would prefer a cast or splint in the future for the same injury (assuming both were equally safe and effec-tive). Of 21 children responding in the splint group, 20 (95%) preferred a splint, whereas 17 (85%) of 20 par-ents preferred a splint. Of 23 children in the cast group, 18 (78%) preferred a splint, whereas 13 (52%) of 25 parents preferred a splint.
Subgroup Analysis
Groups were analyzed according to dominant/nondomi-nant hand injured and degree of fracture. However, given the subgroup nature of these analyses, results should be interpreted with caution and are limited by the small sample of each subgroup.17When children had
their nondominant hand injured, significantly higher changes from baseline in ASKp score were found in the splinting group compared with the casting group at days 14 (P⫽.006), 20 (P⫽.028), and 28 (P⫽.028). No other significant differences were found.
When subgroups were created based on severity of injury, children in the minor-injury subgroup and ran-domly assigned to the splint group were found to have a better ASKp score at day 14 (P⫽.047). A significantly different change from baseline in ASKp score between the study groups was also found at days 14 and 20 for participants in the moderate injury group (P⫽.027 and P ⫽.017, respectively), with those in the splint group having better functioning. No other significant differ-ences were found.
DISCUSSION
Buckle fractures of the wrist are common injuries among children, yet little has been published regarding their treatment or outcomes. North American preference seems to be casts for immobilization,1,3,4but several
stud-ies from the United Kingdom have suggested that treat-ment with splints is common.5–7 Our study, the first to
compare in detail the functioning of children with wrist buckle fractures treated with a removable splint to a cast, has shown that splinted children have better physical functioning, less difficulty with many activities, are able
to return to sports sooner, and suffer no significantly greater pain. Although the overall difference between splint and cast groups in the primary outcome (ASKp score at day 14) was not large, it does reflect a significant difference in function. Specifically, the children in the splint group had close to “normal” ASKp scores at day 14, whereas those in the cast group had scores that correlate with mild disability.8,9Furthermore, at all of the
time points, the splinted children had less difficulty with bathing and returned to sports sooner. We found that children treated with splints wear them (for some point during the day) on average for 14 days. Interestingly, even by day 7 postinjury, only 15% report wearing them all day and night. It seems that for many children with wrist buckle fractures, 3 weeks of constant immobiliza-tion is not necessary. As well, there was no clinically significant difference between the groups with regard to pain at any time point.
Our result is similar to another study that compared children managed with casts versus continuously used splints and found that at 3 weeks there seemed to be no difference in clinical or radiologic outcome.6 However,
this study did not give any sample-size calculation, did not give good definitions of the outcome measures, and was inadequately randomized. In another study, 87 pa-tients were treated with splints, with half removing at home at 3 weeks and half removing in clinic at 3 weeks.5
In that study, all of the parents preferred to remove the splint at home. A third study reported on a cohort of children treated with fiberglass splint and found that the majority of parents were satisfied with this treatment.7
Interestingly, a common theme in these studies,5,6and in
our study, is that a number of patients are lost to fol-low-up in their cast or splint. Presumably these patients remove their cast or splint at home. Although the out-come is obviously unknown for these patients, we sug-gest that it is unlikely they had significant pain or func-tional limitation, or they would have returned for orthopedic or ED follow-up.
Subsequent ED and follow-up visits certainly add to health care costs and are time consuming for the patient and their family. We found that 5 patients (10%) in the cast group had unscheduled return visits to the ED for problems, which is similar to our retrospective cohort study of children with wrist buckle fractures in which 12% of casted patients returned to the ED for prob-lems.18Although the children in our study were seen in
clinic at 3 weeks postinjury, such a visit would not be necessary if the child is functioning well and does not require cast removal. Of course, it is always possible that some families may wish to seek reassurance regarding their child’s fracture and schedule a follow-up visit. Such visits could be managed by primary care providers, and the resultant cost to the health care system for these visits would still be less than those for cast removal or follow-up with an orthopedic surgeon.
FIGURE 2
We had identified in an earlier study3that physicians
were concerned about refracture if children with distal radius and/or ulna buckle fractures were not immobi-lized. The refracture rate quoted in the literature for distal radius/ulna fractures is 2%,19and for wrist buckle
fractures our earlier study has showed a refracture rate of ⬍1%.18 No children in this randomized, controlled
trial suffered a refracture, and other studies examining splint use did not report any refractures. Using a baseline refracture rate of 1%, we would need to enroll⬎5000 patients in a study comparing casting to removable splinting to detect a doubling in this rate (assuming a power of 80% and a type I error of 0.05).
Limitations
The main limitation in this study is the loss to follow-up of patients as the study progressed. Although only 5 patients were lost to all follow-up, we were not able to capture data at all time points for all of the patients in the study (despite frequent telephone follow-up and the use of stamped, self-addressed envelopes). It is notable that completion of the VAS by most participants was less than completion of the ASKp. Most of the patients, however, were seen in person (by the research assistant) at day 21 in clinic (36 of 42 in the splint group and 40 of 45 in the cast group) and did not report any significant problems to the research assistant or the orthopedic surgeon at that time. There were more missing data among the splint patients, but our hospital is the only pediatric orthopedic center in our catchment area, and if patients in the splint group had poor functioning, they would have returned or been referred to our hospital for reassessment. General orthopedic surgeons do not fol-low children with complications from fractures within our region. We believe that it is likely that there were more patients lost to follow-up in the splint group be-cause they were doing well, and parents decided that they did not require any additional care. Also, we found that the majority of children in both groups reported preferring a splint to a cast for future management (as-suming both were equally safe), but we do not know how many children had prior injuries in which they had experience with a splint or cast and could use this pre-vious experience as a point of reference.
We also had 15 children diagnosed with buckle frac-tures by the emergency physician treating the child that were subsequently determined to be greenstick fractures (usually with no displacement). Although we had de-cided a priori to remove these patients from the study, it behooves the treating physician to be careful about the distinction between greenstick and buckle fractures and not to extrapolate to greenstick fractures the results of this trial without further study.
CONCLUSIONS
Children treated with removable splinting have better physical functioning and less difficulty with some
activ-ities than those treated with a cast, with no difference in their level of pain. The use of removable splinting may reduce the need for follow-up visits and, as a result, health care costs. We recommend the use of removable splints in the treatment of this common injury.
ACKNOWLEDGMENTS
This study was supported by a grant from the Physician Services Incorporated Foundation. Dr Plint is supported, in part, by a Junior Clinical Investigator Award from the Children’s Hospital of Eastern Ontario Research Insti-tute.
REFERENCES
1. Lawton LJ. Fractures of the distal radius and ulna. In: Letts MR, ed. Management of Pediatric Fractures. Philadelphia, PA: Churchill Livingstone, Inc; 1994:345–368
2. Armstrong PF, Joughlin VE, Clarke HM. Pediatric fractures of the forearm, wrist, and hand. In: Green NE, Swiontkowski MF, eds. Skeletal Trauma in Children. Philadelphia, PA: WB Saunders; 1998:157
3. Plint AC, Clifford T, Perry J, et al. Wrist buckle fractures: a survey of current practice patterns and attitudes towards im-mobilization.Can J Emerg Med.2003;5:95–100
4. Farbman KS, Vinci RJ, Cranley WR, Creevy WR, Bauchner H. The role of serial radiographs in the management of pediatric torus fractures.Arch Pediatr Adolesc Med.1999;153:923–925 5. Symons S, Rowsell M, Bhowal B, Dias JJ. Hospital versus home
management of children with buckle fractures of the distal radius: a prospective, randomised trial. J Bone Joint Surg Br. 2001;83:556 –560
6. Davidson JS, Brown DJ, Barnes SN, Bruce CE. Simple treat-ment for torus fractures of the distal radius.J Bone Joint Surg Br. 2001;83:1173–1175
7. Solan MC, Rees R, Daly K. Current management of torus fractures of the distal radius.Injury.2002;33:503–505 8. Young NL, Williams JI, Yoshida KK, Wright JG. Measurement
properties of the Activities Scale for Kids. J Clin Epidemiol. 2000;53:125–137
9. Plint AC, Gaboury I, Owen J, Young NL. Activities Scale for Kids: an analysis of normals.J Pediatr Orthop.2003;23:788 –790 10. Powell CV, Kelly AM, Williams A. Determining the minimum clinically significant difference in visual analog pain score for children.Ann Emerg Med.2001;37:28 –31
11. Todd KH, Funk KG, Funk JP, Bonacci R. Clinical significance of reported changes in pain severity. Ann Emerg Med.1996;27: 485– 489
12. Kelly AM. The minimum clinically significant difference in visual analogue scale pain score does not differ with severity of pain.Emerg Med J.2001;18:205–207
13. Pencharz J, Young NL, Owen LJ, Wright JG. Comparison of three outcome instruments in children.J Pediatr Orthop.2001; 21:425– 432
14. Lachin JM. Introduction to sample size determination and power analysis for clinical trials. Control Clin Trials. 1981;2: 93–113
15. Paintadosi S. Clinical Trials: A Methodological Perspective. New York, NY: Wiley; 1997
16. Altman DG, Machin D, Bryant TN, Gardner MJ.Statistics With Confidence. 2nd ed. Bristol, United Kingdom: BMJ Books; 2000 17. Oxman AD, Guyatt GH. A consumer’s guide to subgroup
anal-yses.Ann Intern Med.1992;116:78 – 84
18. Plint A, Perry JJ, Tsang JYL. Pediatric wrist buckle fractures: management and outcomes.Can J Emerg Med.2004;6:397– 401 19. Harbison JS, Stevenson TM, Lipert JR. Forearm fractures in
DOI: 10.1542/peds.2005-0801
2006;117;691
Pediatrics
Amy C. Plint, Jeffrey J. Perry, Rhonda Correll, Isabelle Gaboury and Louis Lawton
Wrist Buckle Fractures in Children
A Randomized, Controlled Trial of Removable Splinting Versus Casting for
Services
Updated Information &
http://pediatrics.aappublications.org/content/117/3/691
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/117/3/691#BIBL
This article cites 15 articles, 1 of which you can access for free at:
Subspecialty Collections
skeletal_disorders_sub
http://www.aappublications.org/cgi/collection/rheumatology:musculo
Rheumatology/Musculoskeletal Disorders following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2005-0801
2006;117;691
Pediatrics
Amy C. Plint, Jeffrey J. Perry, Rhonda Correll, Isabelle Gaboury and Louis Lawton
Wrist Buckle Fractures in Children
A Randomized, Controlled Trial of Removable Splinting Versus Casting for
http://pediatrics.aappublications.org/content/117/3/691
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.