Lung Recruitment and Breathing Pattern During Variable Versus
Continuous Flow Nasal Continuous Positive Airway Pressure in
Premature Infants: An Evaluation of Three Devices
Sherry E. Courtney, MD*; Kee H. Pyon, PhD*; Judy G. Saslow, MD*; Gerald K. Arnold, PhD‡; Paresh B. Pandit, MD*; and Robert H. Habib, PhD§
ABSTRACT. Objective. To determine whether lung volume changes and breathing pattern parameters differ among 3 devices for delivery of nasal continuous positive airway pressure (CPAP) in premature infants.
Methods. Thirty-two premature infants receiving na-sal CPAP for apnea or mild respiratory distress were enrolled. Birth weight was (meanⴞstandard deviation) 1081ⴞ316 g, gestational age 29ⴞ2 weeks, age at study 13ⴞ 12 days, and fraction of inspired oxygen (FIO2) at study .29ⴞ .1. Three devices, applied in random order, were studied in each infant: continuous flow nasal CPAP via CPAP prongs, continuous flow nasal CPAP via mod-ified nasal cannula, and variable flow nasal CPAP. After lung recruitment to standardize volume history, changes in lung volume (⌬VL) were assessed at nasal CPAP of 8, 6, 4, and 0 cm H2O using calibrated direct current-cou-pled respiratory inductance plethysmography.
Results. ⌬VL was significantly greater overall with the variable flow device compared with both the nasal cannula and CPAP prongs. However,⌬VL was not dif-ferent between the cannula and the prongs. Respiratory rate, tidal volume, thoraco-abdominal asynchrony, and FIO2 were greater with the modified cannula than for either of the other 2 devices.
Conclusion. Compared with 2 continuous flow de-vices, the variable flow nasal CPAP device leads to greater lung recruitment. Although a nasal cannula is able to recruit lung volume, it does so at the cost of increased respiratory effort and FIO2.Pediatrics2001;107: 304 –308; nasal CPAP, lung volume changes, preterm in-fants, respiratory inductance plethysmography.
ABBREVIATIONS. CPAP, continuous positive airway pressure; ⌬VL, change in lung volume; RIP, respiratory inductance
plethys-mography; DC, direct current; Fio2, fraction of inspired oxygen;
VT, tidal volume; AC, alternating current; RR, respiratory rate; VE,
minute ventilation; SD, standard deviation.
T
he use of continuous positive airway pressure (CPAP) in premature infants was first de-scribed by Gregory et al1 in 1971. CPAP maybenefit preterm infants with respiratory distress by recruiting alveoli and stabilizing functional residual capacity.2,3In infants with obstructive apnea, it may
help splint the upper airway.4,5 Currently available
nasal CPAP devices (nasal CPAP) use a variety of prong designs and deliver CPAP via either continu-ous or variable gas flow. To our knowledge, there are no data comparing nasal CPAP devices in their abil-ity to recruit lung volume in preterm neonates. Re-liable information about lung recruitment during na-sal CPAP is useful both for the clinical management of infants and for comparison of efficacy of the var-ious methods available for its administration.
Our main objective was to compare changes in lung volume (⌬VL) and breathing pattern parameters
with 3 nasal CPAP devices that are currently used clinically in premature infants.
METHODS
Premature infants weighing⬍1800 g at birth who were receiv-ing nasal CPAP for apnea or mild respiratory distress and were otherwise medically stable were eligible for enrollment. The pro-tocol was reviewed and approved by the institutional review board of Cooper Hospital/University Medical Center. Informed consent was obtained from a parent or guardian before testing. Each infant was evaluated on each of the 3 devices, applied in random order as designated on prepared cards stored in sealed envelopes, and opened at the time of study. Three nasal CPAP devices, as described below, were evaluated.
Continuous Flow Nasal CPAP Using Nasal Prongs
The nasal prongs used were Inca nasal CPAP prongs (Ackrad Laboratories, Cranford, NJ). They were attached via ventilator tubing to an infant positive pressure ventilator set in CPAP mode. Continuous flow of 6 L/minute was used and was not changed during the study. The prong size used was the largest prong that fit the infant’s nares without blanching the surrounding tissue. As is conventionally done using this method of nasal CPAP, the amount of airway pressure applied was varied by adjusting the CPAP setting on the ventilator, which varies the resistance at the exhalation valve.
Continuous Flow Nasal CPAP Using a Nasal Cannula
This device, commonly used in our nursery before this study, was fashioned by connecting a 2.5-mm endotracheal tube adapter to an infant-sized nasal cannula (prong internal diameter: 1.5 mm; Salter Laboratories, Arvin, CA). The device could then be attached to any conventional infant ventilator set in CPAP mode. As with the nasal prongs, a continuous flow of 6 L/minute was used in all infants and was not changed during the study. Also similarly, the
From the *Robert Wood Johnson Medical School at Camden and the De-partment of Pediatrics, Division of Neonatology, the Children’s Regional Hospital at Cooper Hospital/University Medical Center, Camden, New Jersey; ‡American College of Physicians and American Society of Internal Medicine, Philadelphia, Pennsylvania; and §Mercy Children’s Hospital at St Vincent’s Mercy Medical Center and the Department of Pediatrics, Medical College of Ohio, Toledo, Ohio.
This work was presented in part at the Society for Pediatric Research Meeting; May 1–5, 1998; New Orleans, LA.
Received for publication Jan 31, 2000; accepted May 30, 2000.
Reprint requests to (S.E.C.) Department of Pediatrics, Division of Neona-tology, Children’s Regional Hospital at Cooper Hospital/University Med-ical Center, One Cooper Plaza, Camden, NJ 08103. E-mail: courtnse@ umdnj.edu
amount of CPAP delivered was varied by changing the CPAP setting on the ventilator.
Variable Flow Nasal CPAP
The variable flow device used was the Aladdin/Infant Flow nasal CPAP system (Hamilton Medical, Reno, NV; manufactured by EME, Ltd, Brighton, UK; currently distributed by SensorMedics Corp, Yorba Linda, CA as the Infant Flow Nasal CPAP system). The amount of CPAP delivered with this device is changed by varying the amount of gas flow. The largest prongs that fit easily into the nares were used in each infant.
Instrumentation
Infants were fed just before instrumentation. Respiratory in-ductance plethysmography (RIP) bands were then fitted around the chest and abdomen (SensorMedics Corp). The RIP equipment was direct current (DC)-coupled to record static⌬VL(Somnostar;
SensorMedics Corp). An esophageal balloon catheter (Neonatal Esophageal Balloon Catheters; Ackrad Laboratories, Cranford, NJ) was positioned in the lower esophagus for estimation of pleural pressure. Appropriate positioning of the esophageal catheter was confirmed by noting a reproducible pressure tracing that closely tracked airway-opening pressure when the airway was occluded. Air leaks from the mouth were detected using a thermistor (BreathSensor; Nellcor Puritan Bennett, Eden Prairie, MN) and its output was continuously recorded (EdenTrace II Plus; EdenTec, Eden Prairie, MN). Only data with no air leak at the mouth were used. If necessary, the infant’s mouth was gently closed during data collection. Respiratory rate, heart rate, and oxygen saturation were continuously monitored during study on the infant’s bedside monitor. Fraction of inspired oxygen (Fio2) was recorded at start
of study and was adjusted when necessary to maintain oxygen saturation between 90% and 96%.
Data Acquisition and Analysis
All infants were studied supine and while resting quietly. After placing the RIP bands around the infant’s chest and abdomen, and before initiating the nasal CPAP protocol, baseline airflow and pressure were measured using facemask pneumotachography (Neonatal Flow Sensor 7218 [dead space: .8 mL]; Novametrix, Wallingford, CT). Esophageal (transpulmonary) pressure and air-way flows were measured with the Ventrak system (Novametrix). From a series of 10 to 15 leak-free breaths, airway flow was integrated to calculate tidal volume (VT). These breaths were then
matched with the corresponding RIP breaths to calibrate the lat-ter.6,7Esophageal pressure, flow, and volume data were used to
obtain baseline lung mechanics data as well as to calibrate the RIP. Each nasal CPAP device was then applied to the infant in random order. With each device, CPAP was first increased over 10 to 15 minutes to 8 cm H2O, to allow comparable lung recruitment
in all infants. Nasal CPAP was then decreased to 6, 4, and 0 cm H2O. Infants were kept for 3 to 5 minutes at each nasal CPAP level,
and the breaths spanning the last 20 to 30 seconds at each setting were used for subsequent analysis (Fig 1).
DC (static) and alternating current (AC; dynamic) components of the RIP signal were used to estimate⌬VLand tidal ventilation
parameters, respectively.4,8 Specifically, we assessed respiratory
rate (RR; minute⫺1), V
T (mL/kg), and minute ventilation (VE;
RR ⫻ VT; mL/kg/minute) as well as phase angle, which was
calculated by the RespiEvents Software (NIMS, Inc, Miami, FL). The time lag between chest and abdominal movement and result-ing width of the Lissajous loop can be quantified by the phase angle (in degrees), which is proportional to the degree of thora-coabdominal asynchrony.
Sample Size Calculation
Sample size calculations were based on finding a clinically significant⌬VLbetween any 2 of the 3 devices. On the assumption
that a difference of 20% would be clinically significant, and using a .05 significance criterion for testing mean differences and a desired power of 80% to 85%, the required sample size was between 28 and 32.9
Statistical Analysis
⌬VL,, VT, VE, and RR data were analyzed as mixed linear
models in a randomized block factorial design, where devices and
nasal CPAP levels were considered fixed effects and participants were treated as random blocks.10Differences in Fio
2were
ana-lyzed using the Wilcoxon rank sum test. Least square, pair-wise mean comparisons were used to test for differences between de-vices, within nasal CPAP levels, and devices-within-nasal CPAP levels. Satterthwaite approximations were used to adjust for the effects of missing cells. Analyses were performed using the mixed procedure inSAS, Version 6.12(SAS Institute Inc, Cary, NC).
RESULTS
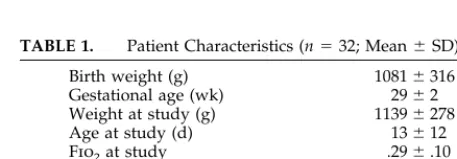
Measurements were successfully obtained in 32 of 35 recruited infants. A summary of their demograph-ics and baseline clinical parameters is provided in Table 1.
Lung Recruitment (⌬VL)
⌬VLat the 3 different nasal CPAP levels relative to
nasal CPAP⫽ 0 are shown in Fig 2.⌬VLdecreased
with decreasing nasal CPAP support for all 3 de-vices. The⌬VLwas similar for both continuous flow
devices. However,⌬VLwas significantly larger
over-all with the variable flow device (P⬍ .001).
Breathing Pattern (VT, RR, and VE)
Tidal volumes did not differ among the groups at any nasal CPAP level. Respiratory rate, and, there-fore, VE, was significantly higher with the cannula, at all 3 nasal CPAP levels, than with the other 2 devices (Fig 3).
Breathing Efficiency (and Oxygen Requirement) Thoracoabdominal asynchrony as determined by RIP phase angle () is shown in Fig 4. No significant differences were found between with any nasal
Fig 1. Stylized representation of lung recruitment, then derecruit-ment, in the study patients. CPAP levels are in cm H2O. Arrows
indicate⌬VLcalculated at each CPAP level (baseline⫽0 cm H2O).
TABLE 1. Patient Characteristics (n⫽32; Mean⫾SD)
Birth weight (g) 1081⫾316
Gestational age (wk) 29⫾2
Weight at study (g) 1139⫾278
Age at study (d) 13⫾12
Fio2at study .29⫾.10
Previous days on ventilator 7⫾11 Baseline CL(ml/cm H2O) 3.26⫾2.42
Baseline RL(cm H2O/L/s) 54.5⫾38.0
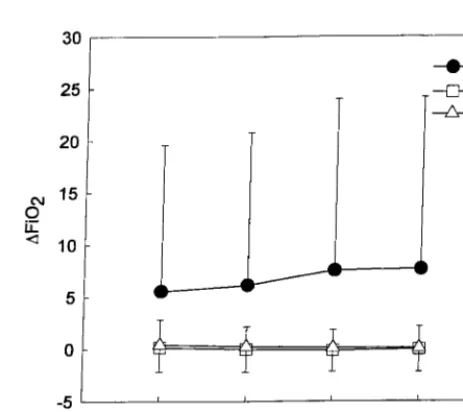
CPAP level for the continuous flow nasal prongs compared with the variable flow device. However, was significantly higher for the cannula, compared with both the other devices (P⬍.001). Percent oxy-gen required to maintain saturation between 90% and 96% increased from baseline (before study) by an average of 7% during study with the cannula, compared with both the other devices. Oxygen changes from baseline were small and similar for the variable flow device and the continuous flow nasal prongs (Fig 5).
DISCUSSION
Few comparative studies of nasal CPAP devices have been published. In particular, we are unaware
of any studies that compare lung recruitment with different nasal CPAP devices as they are currently being used in infants. The main objective of this study was to compare the efficacy of 3 distinct de-vices—2 continuous flow devices and 1 variable flow device—in recruiting lung volume at various nasal CPAP levels.
Factors determining the effectiveness of any nasal CPAP device include its associated work of breath-ing, flow characteristics, ease of application, and the comfort level of the infant once the device is in place. Continuous flow nasal CPAP is increased or de-creased by varying the resistance to exhalation at the exhalation valve on an infant ventilator. Nasal prongs are commonly used to provide continuous
Fig 2. Comparison of the 3 devices:⌬VL(mean⫾standard
devi-ation [SD]) as a function of nasal CPAP level. NC indicates nasal cannula; VF, variable flow device; NP, nasal prongs (P⬍.001 VF vs both NC and NP).
Fig 3. Comparison of the 3 devices: respiratory rate (mean⫾SD), as a function of nasal CPAP level. NC indicates nasal cannula; VF, variable flow device; NP, nasal prongs (P⬍.001 NC vs VF;P⫽ .001 NC vs NP).
Fig 4. Comparison of devices: phase angle (; mean⫾SD), as a function of nasal CPAP level. NC indicates nasal cannula; VF, variable flow device; NP, nasal prongs (P⬍.001 NC vs VF and NP).
Fig 5. Comparison of devices:⌬Fio2from baseline level before
flow nasal CPAP. Concerns exist, however, about increased work of breathing with nasal prongs, com-pared with face mask CPAP.11 Additionally, nasal
prongs often become dislodged making care of these infants difficult. Locke et al12 demonstrated that
in-advertent CPAP can be provided with flow through a nasal cannula. Because nasal cannulas are easy to apply and keep in place, their use had become pop-ular in our neonatal intensive care unit to provide nasal CPAP. This cannula system had not been in-vestigated, and the amount of CPAP actually gener-ated was not clear.
The variable flow nasal CPAP device, in contrast to the continuous flow devices, generates CPAP at the airway. It uses jet flows at high velocity, which can entrain gas to assist inspiration on demand and keep the CPAP level constant. On exhalation, the design of the nasal prongs results in gas flow being shunted through an expiratory outlet rather than continue toward the nares, which can increase expi-ratory work.13–15 Two physical model studies of
the variable flow device have been published. Moa et al13 compared it with a continuous flow system
using a lung model and found that the variable flow device showed less variation in mean airway pressure and external workload. Using a simulated breathing apparatus, Klausner et al15 compared
work of breathing via nasal prongs with the variable flow system and a commonly used continuous flow device. They concluded that the imposed work of breathing with the variable flow system was approx-imately one fourth that of the continuous flow sys-tem. We are aware of only one clinical study com-paring a variable flow device with a continuous flow device. Ahluwalia et al16compared the variable flow
system with nasal CPAP delivered by an endotra-cheal tube inserted into one nostril. In a crossover design in 20 infants over a total study time of 8 hours, no differences were found in Fio2, respiratory
rate, heart rate, blood pressure, or comfort score between devices.
To evaluate lung recruitment with the 3 nasal CPAP devices, we applied DC-coupled RIP to mon-itor static lung volume changes. Inline pneumota-chography cannot be used to measure lung volume changes once a nasal CPAP device is applied to the infant, and changes in breathing synchrony cannot be assessed with pneumotachograpy. Respiratory in-ductance plethysmography, however, is a noninva-sive technique for obtaining real-time data on breath-ing patterns. Accurate calibration of RIP usbreath-ing a face mask with pneumotachograph has been demon-strated in both lambs and premature infants.6,7
DC-coupled RIP allows for a constant baseline so that ⌬VL can be measured. These changes can then be
converted to volume (in mL) based on previous cal-ibration by facemask pneumotachography. The sum of the rib cage and abdominal motion equals the tidal volume, and the phase angle between the rib cage and abdominal motion indicates the degree of para-doxical breathing. An increase in parapara-doxical breath-ing may indicate an increased work of breathbreath-ing.17
Additionally, Locke et al4have shown that in infants
with respiratory insufficiency, increasing CPAP
re-sults in a decreasing phase angle that is directly and significantly correlated with changes in esophageal pressures.
Our results indicate that the variable flow nasal CPAP system recruits lung volume better than both continuous flow devices. The(hence breathing syn-chrony) obtained with the continuous flow nasal prong system was, surprisingly, similar to that ob-tained with the variable flow system despite signifi-cantly higher lung recruitment with the latter. There are 2 possible, albeit related, explanations for this intriguing finding. First, the decrease inwith lung recruitment (or nasal CPAP) may be nonlinear. Sec-ond, the decrease inwith recruitment may change or possibly reverse when the lungs are either overd-istended (decreased compliance) or above an optimal lung volume. The presence or absence of these con-ditions is not available from our data, which only show⌬VLfrom baseline (on nasal CPAP ⫽0).
The decreased variability in the mean airway pres-sure during nasal CPAP provided with the variable flow device13–15 compared with conventional nasal
CPAP systems is perhaps the critical factor leading to the increased lung recruitment with this system. An-other factor that alters the efficacy of any nasal CPAP delivery system is the airway leak around the prongs. Because the prongs are mechanically in par-allel with the lungs, a larger leak around them results in lower effective nasal CPAP or less recruitment. The use of relatively larger prongs is possible with variable flow systems, both because of the design of the delivery system and the prongs themselves. When the nasal CPAP level is reached at the proxi-mal airway (nares), the inflow from the device is shunted away from the infant.13–15 The prongs are
made of a thin, soft material, which may flare out during gas inflow, thus increasing the effective inter-nal diameter and decreasing the leak around the prongs. In contrast to conventional nasal CPAP, the wider ID and thinner walls of the prongs coupled with no gas inflow during exhalation all may effec-tively reduce the imposed work of breathing because of the mechanical device.
Differences in flow rate inherent between the de-vices may also affect lung recruitment. Although variable flow devices by definition vary CPAP at-tained by varying the flow rate, actual flow delivered to the nares of the infant has not been assessed. Much of the flow with these systems is shunted away from the infant and out the expiratory limb of the CPAP circuit.
Continuous flow nasal CPAP via the modified na-sal cannula recruited lung volume equally to the nasal CPAP prongs, but at a very high cost: RR, , and Fio2all increased significantly with the modified
nasal cannula. In the study by Locke et al,12no CPAP
modi-fied nasal cannula device not only indicate that use of such a system for provision of nasal CPAP should be discouraged but raise some questions as well about the respiratory effects of providing oxygen to the preterm neonate by nasal cannula.
CONCLUSION
Nasal cannulas can provide equal ⌬VLas prongs
designed for nasal CPAP when continuous flow rates are sufficiently high. However, thoracoabdominal asynchrony is higher with the nasal cannula CPAP, as is the RR, VE, and Fio2required. Thus, work of
breathing is likely higher with the cannula, and its use to provide nasal CPAP cannot be recommended. We have also shown that variable flow nasal CPAP recruits lung volume more effectively than the 2 continuous flow devices at similar CPAP levels. In-deed, clinicians should be aware that, when using such a device, lower CPAP levels may be indicated than are usually used with continuous flow devices. Because use of this system does not adversely alter breathing efficiency (, oxygen requirement) or breathing pattern (RR, VT, and VE), we conclude that
variable flow nasal CPAP provides more effective nasal CPAP at all levels. Future studies should com-pare work of breathing between the variable flow and conventional continuous flow nasal CPAP in infants, given the important implications of in-creased work of breathing on failure of nasal CPAP and subsequent need for reintubation.
ACKNOWLEDGMENTS
This work was supported in large part by a grant from The Cooper Faculty Practice Foundation. Hamilton Medical, Inc (Reno, NV) provided the variable flow nasal CPAP device, manufactured by EME, Ltd (Brighton, England). It is currently distributed by SensorMedics, Inc (Yorba Linda, CA).
We thank Dr Lee Brooks for his critical review of the manu-script.
REFERENCES
1. Gregory GA, Kitterman JA, Phibbs RH, Tooley WH, Hamilton WK.
Treatment of the idiopathic respiratory distress syndrome with contin-uous positive airway pressure.N Engl J Med. 1971;284:1333–1340 2. Shaffer TH, Koen PA, Moskowitz GD, Ferguson JD,
Delivoria-Papadopoulos M. Positive end expiratory pressure: effects on lung mechanics of premature lambs.Biol Neonate. 1978;34:1–10
3. Richardson CP, Jung AL. Effects of continuous positive airway pressure on pulmonary function and blood gases of infants with respiratory distress syndrome.Pediatr Res. 1978;12:771–774
4. Locke R, Greenspan JS, Shaffer TH, Rubenstein SD, Wolfson MR. Effect of nasal CPAP on thoracoabdominal motion in neonates with respira-tory insufficiency.Pediatr Pulmonol. 1991;11:259 –264
5. Miller MJ, DiFiore JM, Strohl KP, Martin RJ. Effects of nasal CPAP on supraglottic and total pulmonary resistance in preterm infants.J Appl Physiol. 1990;68:141–146
6. Warren RH, Alderson SH. Face mask application for calibration of respiratory inductive plethysmography in lambs.J Dev Physiol. 1988;10: 175–178
7. Brooks LJ, DiFiore JM, Martin RJ, CHIME Study Group. Assessment of tidal volume over time in preterm infants using respiratory inductance plethysmography.Pediatr Pulmonol. 1997;23:429 – 433
8. Sandberg KL, Lindstrom DP, Krueger ED, Sundell H, Cotton RB. Mea-surement of tidal volume during high frequency ventilation by imped-ance plethysmograph.Pediatr Res. 1988;23:253–256
9. Cohen J.Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Lawrence Erlbaum; 1988:48 –52, 274 –280
10. Kirk R.Experimental Design: Procedures for the Behavioral Sciences. Pacific Grove, CA: Brooks/Cole; 1995:454 – 473
11. Goldman SL, Brady JP, Dumpit FM. Increased work of breathing asso-ciated with nasal prongs.Pediatrics. 1979;64:160 –164
12. Locke RG, Wolfson MR, Shaffer TH, Rubenstein D, Greenspan JS. Inadvertent administration of positive end-distending pressure during nasal cannula flow.Pediatrics. 1993;91:135–138
13. Moa G, Nilsson K, Zetterstrom H, Jonsson LO. A new device for administration of nasal continuous positive airway pressure in the newborn: an experimental study.Crit Care Med. 1988;16:1238 –1242 14. Moa G, Nilsson K. Nasal continuous positive airway pressure:
experi-ences with a new technical approach.Acta Paediatr. 1993;82:210 –211 15. Klausner JF, Lee AY, Hutchison AA. Decreased imposed work with a
new nasal continuous positive airway pressure device.Pediatr Pulmonol. 1996;22:188 –194
16. Ahluwalia JS, White DK, Morley CJ. Infant flow driver or single prong nasal continuous positive airway pressure: short-term physiological effects.Acta Paediatr. 1998;87:325–327
17. Springer C, Godfrey S, Vilozni D, Bar-Yishay E, Noviski N, Avital A. Comparison of respiratory inductance plethysmography with thoraco-abdominal compression in bronchial challenges in infants and young children.Am J Respir Crit Care Med. 1996;154:665– 669
HAPPINESS IS NOT GETTING WHAT YOU WANT
“We go from anticipation to anticipation, not from satisfaction to satisfaction.”
DOI: 10.1542/peds.107.2.304
2001;107;304
Pediatrics
and Robert H. Habib
Sherry E. Courtney, Kee H. Pyon, Judy G. Saslow, Gerald K. Arnold, Paresh B. Pandit
Evaluation of Three Devices
Flow Nasal Continuous Positive Airway Pressure in Premature Infants: An
Lung Recruitment and Breathing Pattern During Variable Versus Continuous
Services
Updated Information &
http://pediatrics.aappublications.org/content/107/2/304
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/107/2/304#BIBL
This article cites 15 articles, 2 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.107.2.304
2001;107;304
Pediatrics
and Robert H. Habib
Sherry E. Courtney, Kee H. Pyon, Judy G. Saslow, Gerald K. Arnold, Paresh B. Pandit
Evaluation of Three Devices
Flow Nasal Continuous Positive Airway Pressure in Premature Infants: An
Lung Recruitment and Breathing Pattern During Variable Versus Continuous
http://pediatrics.aappublications.org/content/107/2/304
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.