A 4-Step Framework for Shared
Decision-making in Pediatrics
Douglas J. Opel, MD, MPHTreuman Katz Center for Pediatric Bioethics, Seattle Children’s Research Institute; and Department of Pediatrics, School of Medicine, University of Washington, Seattle, Washington
Dr Opel conceptualized and designed the study, drafted the manuscript, approved the final manuscript as submitted, and agrees to be accountable for all aspects of the work.
DOI: https:// doi. org/ 10. 1542/ peds. 2018- 0516E Accepted for publication Jul 3, 2018
Address correspondence to Douglas J. Opel, MD, MPH, Treuman Katz Center for Pediatric Bioethics, Seattle Children’s Research Institute, 1900 Ninth Ave, Mailstop JMB-6, Seattle, WA 98101. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2018 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The author has indicated he has no financial relationships relevant to this article to disclose. FUNDING: Supported by the Greenwall Faculty Scholars Program in Bioethics.
POTENTIAL CONFLICT OF INTEREST: The author has indicated he has no potential conflicts of interest to disclose.
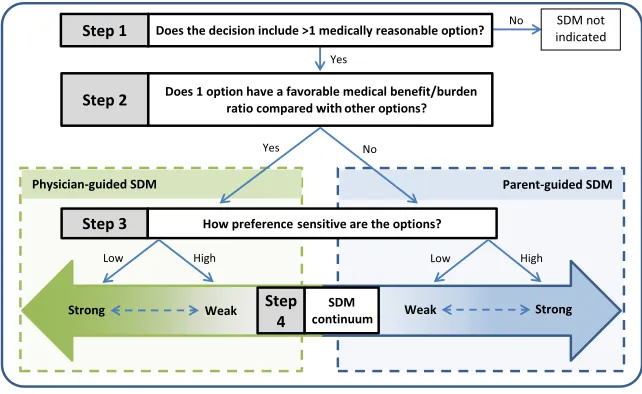
Shared decision-making (SDM) is a well-established component of patient-centered care, and yet, its application in pediatrics is poorly understood. Common features of pediatric decision-making are not completely addressed in current SDM models, such as the fact that the principal SDM participant is the patient’s surrogate, who, unlike competent adult patients deciding for themselves, has limitations on decision-making authority. To address this gap and improve the practice of SDM in pediatrics, a practical 4-step framework is presented. In step 1, physicians are posed the following question for any discrete decision: does the decision include >1 medically reasonable option? If the answer is no, SDM is not indicated. If the answer is yes, physicians proceed to step 2 and answer the following question: does 1 option have a favorable medical benefit-burden ratio compared with other options? If yes, physician-guided SDM is appropriate. If no, parent-guided SDM is appropriate. For each SDM approach, the physician proceeds to step 3 and answers the following question: how preference sensitive are the options? This helps to determine the specific SDM approach in step 4, which ranges from a strong or weak version of
physician-guided SDM to a strong or weak version of parent-guided SDM. Several decisional characteristics, if present, can also help calibrate the version of SDM used. Additional analyses are needed to consider the inclusion of adolescents into this SDM framework.
Shared decision-making (SDM) is a well-established component of patient-centered care1 and has been
defined as decision-making in which
“both parties share information…
take steps to build consensus about the preferred treatment, and [reach an agreement] on the treatment to implement.”2 Yet, how SDM
translates to pediatric settings is less understood.3 The primary
difficulty with the application of SDM to pediatrics is that it must account for the fact that the principal SDM participant is the patient’s surrogate (ie, the parent or legal guardian), who, unlike competent adult patients deciding for themselves, has limitations on decision-making authority. This essential role of the surrogate in pediatric decision-making can complicate SDM’s iconic features, such as “tak[ing] steps to build consensus.”2
This feature of pediatric decision-making is not completely addressed in current SDM models, causing confusion on when and how to apply SDM in pediatric practice.4–6
Additional conceptual work regarding SDM in pediatrics is needed. The objective for this article is to describe a practical framework for applying SDM in pediatrics that accounts for pediatrics’ unique decisional and contextual features.
PRIMER
To begin, it is important to emphasize that the proposed goals for the framework are to increase agreement between parent choice and values as well as to improve medical outcomes for children. As such, the framework is intended to both advance the use of SDM as well as help to recognize when the use of SDM is not appropriate. Second, the proposed framework represents an ideal for which exceptions will exist. The main purpose for the framework is to provide the foundation and scaffolding for the broad use of SDM
across all pediatric disciplines. Third, several existing decision-making models were used to inform the development of the framework.7–12
These models were adapted to pediatric SDM (when necessary) by using principlism and case-based reasoning.13 This framework was
also subjected to iterative critiques by experts in ethics, pediatrics, and medical decision-making to help ensure that it comprised the key elements of pediatric decision-making. Nonetheless, the proposed framework is considered to be preliminary and amenable to further revision and adaptation. Lastly, the framework is intended for decision-making that involves nonadolescent children in which parents are the principal participant. The primary rationale for excluding adolescents is to enable an initial proof-of-concept evaluation of the framework itself. Furthermore, all that may be needed for SDM to accommodate an adolescent’s developing autonomy are minor modifications to current models.11
FRAMEWORK
The framework includes 4 steps arranged algorithmically (Fig 1). Any discrete clinical decision can
serve as the starting point. Each of the first 3 steps poses a question to the physician, with the answers directing the physician further along the algorithm. Steps 3 and 4 provide guidance on the type and version of SDM that is appropriate to use for the decision under consideration. Below, the process, rationale, justifications, and limitations are described for each step of the proposed framework.
STEP 1: DOES THE DECISION INCLUDE >1 MEDICALLY REASONABLE OPTION?
The rationale for this step is that medical situations in which there is only 1 treatment choice require a different decision-making approach than situations in which several treatment options exist. In the former situation, sharing a decision is not possible because there is no decision to share. Instead, the approach is centered on a discussion with the parent (and when appropriate, the child) about the 1 available treatment option. Conversely, in the latter situation, the approach does include presenting the several available options and helping parents choose the option that is aligned with their values.14 This is
the domain of SDM. In fact, one of the first conceptualizations of SDM
FIGURE 1
was focused on scenarios in which
“several treatment options exist with different possible outcomes.”2
Since then, there has been continued support for real choice as a
prerequisite for SDM.10, 14–16
What requires clarification, however, is what constitutes real choice. Does this mean that a decision has >1 option that represents the standard of care (SOC)? That meets a certain threshold of empirical evidence? That is reimbursed? It is apparent that there are likely a myriad of factors that might influence what is considered to be a decision with real choice, with some more defensible than others.17, 18 It is also apparent
that these factors may not be easily distinguished, such as when value judgments are masqueraded as medical fact.19, 20 Lack of clarity
on which factors compose a decision with real choice (and the propensity to conflate them) can have a fundamental influence on the practice of SDM; many decisions that should not be shared with patients are, and those that should be are not. Some have therefore proposed that real choice be defined as “equipoise”
in which “options really are options.”16 Others have suggested
that choice exists in the presence of “reasonable alternatives”15 or
“2 or more medically reasonable choices.”10 I propose that real choice
exists when there is >1 medically reasonable option, with medically reasonable defined as consistent with the SOC.
The rationale for this definition is twofold. First, it is hard to justify an option as medically reasonable if it does not fall within the SOC. The SOC guides professional practice and requires physicians to provide minimally competent care that other physicians would provide under the same circumstances.21–23 Those
who do not meet this standard risk medical malpractice, negligence, and/ or professional discipline. What is
medically reasonable therefore ought to at least reflect this basic minimum. Second, the SOC is generally based on evidence-based medicine. Ideally, interventions become the SOC because their safety and efficacy profiles are based on quality scientific evidence. Professional guideline standards also help promulgate evidence-based SOC.24, 25
Step 1 is critical because when there is only 1 medically reasonable option, SDM is not appropriate. Consider the treatment decision for a child who presents with a moderate acute asthma exacerbation. The combination of
short-acting β2-agonists (SABAs) and
corticosteroids is the 1 medically reasonable option for initial treatment.26, 27 As a result, a
non-SDM, physician-controlled approach in which a model of simple consent is used is appropriate.10 This
involves the physician explaining the intervention to the parent (and when appropriate, the child) followed by a discussion of the intervention’s risks and benefits and solicitation of the parent’s consent. Discussion of the lack of reasonable alternatives can occur on parental request. Decisions that exist within this treatment option, such as the type of SABA used (levalbuterol versus albuterol), should be considered separately within the framework.
STEP 1 ISSUES
Several potential issues are raised by step 1. First, determinations of what is medically reasonable should remain distinct from determinations of the appropriateness of a
parent’s response to medically reasonable options. For instance, some parents will refuse the 1 medically acceptable option. Whether this refusal is acceptable requires separate consideration (eg, use of the harm principle to assess whether intervening against parental decision-making authority
is justifiable7) and will vary by
the refusal (eg, parental refusal of SABAs and corticosteroids would likely not be respected, whereas parental refusal of newborn screening, another decision with only 1 medically reasonable option, would28). A non-SDM,
physician-controlled decision-making approach, however, is appropriate in both scenarios.
Second, determinations of what is medically reasonable can be difficult when there is not consensus regarding the SOC. These scenarios are not uncommon in pediatrics; surgical intervention in hypoplastic left heart syndrome29–31 or trisomy
1332, 33 are 2 examples. However, it
is precisely these scenarios in which there is a lack of consensus that >1 acceptable option likely exists, and moving to step 2 is warranted. Third, the SOC may not be evidence-based. For example, an option based on scant evidence can become the SOC simply by being codified in a professional guideline. Although it is true that as an ideal, the SOC should be referent only to high-quality, reproducible scientific evidence, there is a practical argument for being more inclusive. For instance, lower-quality evidence may be the only evidence available. As such, it may be appropriate for such evidence to serve as the SOC until stronger evidence exists. In addition, keeping what is medically reasonable anchored to the SOC helps to ensure that minimum requirements for quality evidence are met. Options based on patient testimonials, opinion polls, or ideology, for instance, are generally excluded from the SOC because they don’t meet the minimally competent care requirement.
allergies. Although physician-controlled decision-making is appropriate for the decision whether to use an antihistamine (it is the 1 medically reasonable option), the low severity of the illness and elective nature of this treatment can make SDM appropriate for when the antihistamine is started.
Lastly, despite added specificity for what constitutes a medically reasonable option, an element of subjectivity remains. Physicians’
own biases and values, for instance, may still influence determinations of reasonableness. Furthermore, these factors may wield their influence implicitly under the façade of evidence-based SOC. However, my hope is that step 1 reduces this subjectivity.
STEP 2: DOES 1 OPTION HAVE A FAVORABLE MEDICAL BENEFIT/BURDEN RATIO COMPARED WITH OTHER OPTIONS?
If a clinical decision includes >1 medically reasonable option, it is appropriate to proceed to step 2 to make a reasoned estimation of the ratio of medical benefits to burdens for each option. The rationale for this step is to fulfill physician obligations in pediatrics to ensure that surrogate decisions promote the child’s best interests.13 If 1 option has a
favorable medical benefit-burden ratio compared with other options, it is appropriate for the physician to assume a more directive role in SDM. This is called physician-guided SDM. When there is not a favorable option, it is appropriate to allow the parent to assume a more directive role. This is called parent-guided SDM.
Critical to this step is determining what constitutes a favorable option. This involves a judgment based on evidence-based probabilities and magnitudes of the medical benefits and burdens of the options as well as an assessment of the certainty surrounding those probabilities
and magnitudes. When there is an absence of quality evidence, physicians can still make favorability assessments on the basis of physician experience or expert opinion but should be wary of doing so and resist making strong favorability judgments.
In addition, although a physician’s primary obligation is to promote the health and welfare of the patient, physicians also have a duty to promote public health.34 It is
therefore critical that SDM accounts for these dual responsibilities. As such, the favorability calculus in step 2 should not only include benefit-burden assessments relative to the individual child’s health but also include, when appropriate, benefit-burden assessments relative to the public’s health. Consider the scenario in which several oral antibiotics represent medically acceptable empirical first-line treatments for a child with a presumed urinary tract infection on the basis of local
Escherichia coli–resistant patterns. A favorability calculus that includes only benefit-burden assessments of the antibiotic options relative to the individual child’s health (eg, assessments that might include comparisons of frequency of
administration, side effects, and cost) might render a judgment that fails to fulfill duties to adhere to public health antimicrobial stewardship goals to promote the use of the most narrow-spectrum efficacious antibiotic.
STEP 2 ISSUES
What balance of probabilities and magnitudes is favorable and which benefits and burdens to prioritize in the calculus can vary among physicians. Therefore, as with step 1, what constitutes a favorable medical benefit-burden ratio remains subjective and prone to physician bias. Hopefully, this framework will
help to reduce such bias by making these judgments more explicit. A second issue relates to how to integrate public health
considerations into the favorability calculus. Although the importance of integrating public health considerations may be clear, the extent to which they should influence the favorability calculus is not. For instance, in the aforementioned antibiotic example, how should an antibiotic with some unfavorable public health characteristics (eg, it is broad spectrum) but some favorable individual-level characteristics (eg, once a day dosing) fare against an antibiotic with favorable public health characteristics (eg, it is narrow spectrum) but some unfavorable individual-level characteristics (eg, 4 times a day dosing)? Should the importance of antimicrobial stewardship for public health hold sway over individual-level characteristics in the favorability calculus? If so, which individual-level characteristics? The weight that public health considerations deserve compared with those that affect the child’s health requires additional analysis.
STEP 3: HOW PREFERENCE SENSITIVE ARE THE OPTIONS?
After making a favorability assessment in step 2, the next step is to determine the parents’
preferences regarding the options (Fig 1). The rationale for this step is to ensure that parental values and preferences align with the chosen option. In one of the first known descriptions of SDM, the President’s Commission acknowledged the importance of “the rights and responsibilities of patients” and proposed SDM as the “ideal for the patient-professional relationship”
as medicine shifted away from paternalism.35
reasonable options, physician obligations to respect the rights and responsibilities of parents justify eliciting and incorporating their preferences into decision-making. Parents know their children best, are able to weigh competing family interests best, and are allowed to instill in their children the values they have deemed the best.7 When
options exist (and even when 1 option appears favorable to the physician), “the best choice depends on how [the parent] values the risks and benefits of the treatments available.”36
The intent of step 3, however, is not to simply elicit what the parent would like to do. Rather, the role of the physician ought to be more expansive and include helping parents to articulate their values and preferences: “respecting and responding to patient preferences—
the hallmark of patient-centered care—means eliciting, exploring, and questioning preferences and helping patients construct them.”37
Indeed, the ideal physician “is a caring physician who integrates the information and relevant values to make a recommendation and, through discussion, attempts to persuade the patient to accept this recommendation as the intervention that bests proposes his or her overall well-being.”9
The justification for a more expansive physician role in this step is
threefold. First, a person’s values and preferences (indeed, selfhood) are rarely clear or stable; rather, what one values and prefers is an ongoing process subject to one’s capacity for change and reflection. Second, this process is relational: “much of who we are and what we value is rooted in our relationship and affinities with others.”38 It is through our
relationships and interactions with others (physicians included) that the development and revision of preferences is facilitated. Third, this more expansive role aligns with the
intent of the President’s Commission for SDM to represent “an appropriate balance” between patient autonomy and a physician’s obligation to promote the patient’s health and well-being.35 Simply eliciting parent
values and preferences falls short of this balance.
This is not to say that physicians ought to coerce, manipulate, or be confrontational with parents or patients. Nor is it meant to infer that physicians no longer have an obligation to acknowledge and communicate their own biases. Rather, step 3 is designed to empower physicians to be involved in helping parents to assess the worthiness of certain health-related values and to prevent physicians from presuming what parents prefer. Parents may not have a preference between available options despite evidence or experiences suggesting they should (and vice versa), and/ or the degree to which preferences matter to the decision will vary between parents.39, 40 Step 3 makes
explicit what parents prefer and how influential those preferences are to their decision-making.
STEP 3 ISSUES
A major limitation to step 3 is that it can be time consuming. Many parents do not routinely examine their values or preferences to be able to articulate them easily. Even if parents can articulate their preferences, it still can be cumbersome for parents to know how to prioritize these preferences within a novel context, such as the health care environment. Physicians may also feel reluctant to assume a role that encourages them to do more than elicit parental preferences. To some, this more expansive role may seem inappropriately intrusive and prone to injecting bias into the decision-making process. The debate surrounding whether and how to answer the patient
question “What would you do?”
is illustrative41–48 because some
have argued for a nondirective or value-neutral response to avoid inappropriately influencing the outcome of a preference-sensitive decision.41, 44, 47 My position is that a
directive response to this question, particularly after clarifying the parents’ intention and disclosing one’s own biases and experiences, can support parents in receiving what they desire: help to “clarify relevant values of their own” and to clarify which values “should rightly shape such difficult decisions.”48
STEP 4: CALIBRATING THE SDM APPROACH
In this last step, we reach a specific SDM approach. Here, SDM is visualized as a continuum, with a physician-guided SDM approach occupying one-half and a parent-guided SDM approach occupying the other (Fig 1). Within each approach, there are strong and weak versions, with the strong versions signifying that the parent or physician is appreciably guiding SDM and the weak versions embodying an SDM in which the decision-making is more mutual.
subsequently, the physician elicits and helps articulate the parent’s preferences. After determining that parental preferences are minimal, the physician seeks explicit parental agreement with the physician-preferred option. If the parent’s preferences change over the course of the discussion, the physician may try to persuade the parent to embrace the values and preferences that align with the physician-preferred option but remains willing to implement the option that is most aligned with the parent’s preferences.
An example in which a strong version of physician-guided SDM may be appropriate is the decision regarding surgical versus medical management in early, uncomplicated appendicitis. Although medical management has emerged as a medically reasonable option to surgical management, the certainty of its risks and benefits is lower compared with surgical management given a paucity of high-quality studies. This, combined with the high efficacy and rare risks with surgical management, makes surgical management the favorable option.49–51 Use of a strong version
of physician-guided SDM, however, would be contingent on this decision not being preference sensitive to the parents. If it is clear in step 3 that this is not the case, a weak version of physician-guided SDM would be indicated. In this weak version, the physician may still try to persuade the parent to embrace the values and preferences that align with the physician-preferred option, but the physician is more committed to working with the parent to reach a mutual decision that is aligned with the parent’s values and preferences. To justify the strong version of the parent-guided SDM approach, there must be (1) >1 medically reasonable option for a decision (step 1), (2) no favorable option based on medical benefit-burden ratios (step 2), and (3) the options are preference
sensitive to the parent making the decision (step 3). Using a strong version of parent-guided SDM, the physician explains each option and its risks and benefits to ensure that the parent is fully informed. The physician explains that each option is medically appropriate and that there is no consensus regarding which option is better. In eliciting and helping articulate the parent’s preferences, the physician is committed to implementing the intervention that is most closely aligned with the parent’s preferences. The physician may make transparent the physician’s preferred option on the basis of expertise, experience, and interpretation of the evidence but usually does so only on parental request.
Male newborn circumcision is illustrative here. Circumcision and no circumcision are both medically reasonable options, and although the medical benefits of circumcision outweigh the risks, “the medical benefits [of circumcision] alone may not outweigh” other considerations to not circumcise, such as religious, cultural, or personal preferences.52
If circumcision is indeed highly preference sensitive to the particular parents facing this decision, a strong-version of parent-guided SDM is appropriate. If it is not preference sensitive, a weak version of parent-guided SDM is indicated. In this version, the physician still explains that each option is medically appropriate and that there is no consensus regarding which option is better, but on determining that this is not a preference sensitive decision to the parents, the physician is more willing to convey the preferred option on the basis of expertise, experience, and/or interpretation of the evidence. The physician may even try to persuade the parent to embrace the values and preferences that align with the physician-preferred option, but the physician is more committed to working with
the parent to reach a mutual decision aligned with the parent’s (evolving) values and preferences.
Importantly, step 4 permits some calibration of SDM on the basis of the presence of other decisional characteristics besides parental preferences that can shape the SDM approach.53 These
decisional characteristics include the urgency of the decision (as discussed previously), whether the intervention is longitudinal (versus single event), and whether the intervention is provider (or parent) implemented.53–57 For instance,
longitudinal interventions, such as those that occur in the context of chronic disease (eg, insulin treatment in diabetes or stimulant medications in attention-deficit/ hyperactivity disorder), can calibrate SDM to be more parent guided. This is justified by the need to support more interaction and negotiation as well as to maintain compliance in the context of revisiting an intervention over time. Contextual features of the decision may also change over time: patients might get sicker or have adverse effects from previous experiences with the intervention. As such, a strong version of physician-guided SDM may be calibrated to a weaker one or a weak version of parent-guided SDM may be calibrated to a stronger one.
and comfort with the intervention as well as the physician’s knowledge of unique system-level variables that may influence the success of implementing the intervention in the present clinical setting (eg, ketamine versus propofol sedation for
fracture reduction in the emergency department).
STEP 4 ISSUES
Step 4 builds on Kon’s8 model for
SDM by incorporating additional variables beyond parental preferences to calibrate SDM. Although a few examples of these variables and how they might change the SDM approach used are discussed in this article, there are many others and more complex ways in which they likely influence SDM. Indeed, these calibration variables may even conflict. Longitudinal but physician-implemented interventions, for instance, may impose opposite pressures on how SDM is calibrated. Whether these variables are canceling or should be weighted differently requires additional analyses.
CONCLUSIONS
What I have attempted to advance is a preliminary 4-step framework for when and how to implement SDM in pediatrics. These 4 steps and the justifications therein can help to ensure that SDM is used appropriately and accounts for the decisional and contextual features unique to pediatrics. Additional analyses are needed to consider the inclusion of adolescents into this SDM framework.
ACKNOWLEDGMENTS
I thank Katherine Lepere, BA, Doug Diekema, MD, MPH, Ben Wilfond, MD, Seema Shah, JD, Abby Rosenberg, MD, Jon Tilburt, MD, Mara Buchbinder, PhD, Neal Dickert, MD, Jennifer
Blumenthal-Barby, PhD, Amy McGuire, JD, and Bernie Lo, MD, for their comments on earlier versions of the framework and/or article.
ABBREVIATIONS
SABA: short-acting β2-agonist SDM: shared decision-making SOC: standard of care
REFERENCES
1. Barry MJ, Edgman-Levitan S. Shared decision making–pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780–781
2. Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med. 1997;44(5):681–692
3. Opel DJ. A push for progress with shared decision-making in pediatrics.
Pediatrics. 2017;139(2):e20162526
4. Aronson PL, Fraenkel L. Is shared decision-making the right approach for febrile infants? Pediatrics. 2017;140(3):e20170225
5. Birchley G. Deciding together? Best interests and shared decision-making in paediatric intensive care. Health Care Anal. 2014;22(3):203–222
6. Gillam L, Wilkinson D, Xafis V, Isaacs D. Decision-making at the borderline of viability: who should decide and on what basis? J Paediatr Child Health. 2017;53(2):105–111
7. Diekema DS. Parental refusals of medical treatment: the harm principle as threshold for state intervention.
Theor Med Bioeth. 2004;25(4): 243–264
8. Kon AA. The shared decision-making continuum. JAMA. 2010;304(8):903–904
9. Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship.
JAMA. 1992;267(16):2221–2226
10. Whitney SN, McGuire AL, McCullough LB. A typology of shared decision making, informed consent, and simple consent. Ann Intern Med. 2004;140(1):54–59
11. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367
12. Sandman L, Munthe C. Shared decision making, paternalism and patient choice. Health Care Anal. 2010;18(1):60–84
13. Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 5th ed. New York, NY: Oxford University Press; 2001 14. Whitney SN, Holmes-Rovner M, Brody
H, et al. Beyond shared decision making: an expanded typology of medical decisions. Med Decis Making. 2008;28(5):699–705
15. Elwyn G, Frosch DL, Kobrin S.
Implementing shared decision-making: consider all the consequences.
Implement Sci. 2016;11:114 16. Gwyn R, Elwyn G. When is a shared
decision not (quite) a shared decision? Negotiating preferences in a general practice encounter. Soc Sci Med. 1999;49(4):437–447
17. Sculpher M, Gafni A, Watt I. Shared treatment decision making in a collectively funded health care system: possible conflicts and some potential solutions. Soc Sci Med. 2002;54(9):1369–1377
18. Wirtz V, Cribb A, Barber N. Patient-doctor decision-making about treatment within the consultation–a critical analysis of models. Soc Sci Med. 2006;62(1):116–124
19. Opel DJ, Taylor JA, Phillipi CA, Diekema DS. The intersection of evidence and values in clinical guidelines: who decides what constitutes acceptable risk in the care of children? Hosp Pediatr. 2013;3(2):87–91
20. Ubel PA. Medical facts versus value judgments–toward preference-sensitive guidelines. N Engl J Med. 2015;372(26):2475–2477
21. Hall v Hilburn, 466 So 2d 856 (Miss 1985)
22. McCourt v Abernathy, 457 SE 2d 603 (SC 1995)
23. Johnston v St. Francis Medical Center, Inc, 799 So 2d 671 (La Ct App 2001) 24. Graham R, Mancher M, Miller Wolman
Standards for Developing Trustworthy Clinical Practice Guidelines, Board on Health Care Services. Clinical Practice Guidelines We Can Trust. Washington, DC: National Academies Press; 2011
25. Guyatt GH, Oxman AD, Vist GE, et al; GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926
26. Castro-Rodriguez JA, Rodrigo GJ, Rodríguez-Martínez CE. Principal findings of systematic reviews of acute asthma treatment in childhood.
J Asthma. 2015;52(10):1038–1045
27. Okpapi A, Friend AJ, Turner SW. Asthma and other recurrent wheezing disorders in children (acute). BMJ Clin Evid. 2012;2012:0300
28. Committee on Bioethics; Committee on Genetics; American College of Medical Genetics and Genomics Social, Ethical, and Legal Issues Committee. Ethical and policy issues in genetic testing and screening of children. Pediatrics. 2013;131(3):620–622
29. Feudtner C. Ethics in the midst of therapeutic evolution. Arch Pediatr Adolesc Med. 2008;162(9):854–857
30. Kon AA. Healthcare providers must offer palliative treatment to parents of neonates with hypoplastic left heart syndrome. Arch Pediatr Adolesc Med. 2008;162(9):844–848
31. Wernovsky G. The paradigm shift toward surgical intervention for neonates with hypoplastic left heart syndrome. Arch Pediatr Adolesc Med. 2008;162(9):849–854
32. Nelson KE, Rosella LC, Mahant S, Guttmann A. Survival and surgical interventions for children with trisomy 13 and 18. JAMA. 2016;316(4):420–428
33. Lantos JD. Trisomy 13 and 18– treatment decisions in a stable gray zone. JAMA. 2016;316(4):396–398
34. American Medical Association.
Code of Medical Ethics. Chicago, IL: American Medical Association; 2016. Available at: https:// www. ama- assn. org/ delivering- care/
code- medical- ethics- physicians- health- community. Accessed May 9, 2018 35. President’s Commission for the Study
of Ethical Problems in Medicine and Biomedical and Behavioral Research.
Making Health Care Decisions: A Report on the Ethical and Legal Implications of Informed Consent in the Patient-Practitioner Relationship. Washington, DC: US Government Printing Office; 1982
36. Elwyn G, Frosch D, Rollnick S. Dual equipoise shared decision making: definitions for decision and behaviour support interventions. Implement Sci. 2009;4:75
37. Epstein RM, Peters E. Beyond information: exploring patients’ preferences. JAMA. 2009;302(2):195–197
38. Sherwin S; Feminist Health Care Ethics Research Network. The Politics of Women’s Health: Exploring Agency and Autonomy. Philadelphia, PA: Temple University Press; 1998
39. Madrigal VN, Carroll KW, Hexem KR, Faerber JA, Morrison WE, Feudtner C. Parental decision-making preferences in the pediatric intensive care unit. Crit Care Med. 2012;40(10):2876–2882 40. Tom DM, Aquino C, Arredondo AR, Foster BA. Parent preferences for shared decision-making in acute versus chronic illness. Hosp Pediatr. 2017;7(10):602–609
41. Gutgesell HP. What if it were your child?
Am J Cardiol. 2002;89(7):856
42. Truog R. Revisiting “doctor, if this were your child, what would you do?”J Clin Ethics. 2003;14(1–2):63–67
43. Halpern J. Responding to the need behind the question “doctor, if this were your child, what would you do?”
J Clin Ethics. 2003;14(1–2):71–78 44. Ruddick W. Answering parents’
questions. J Clin Ethics. 2003;14(1–2):68–70
45. Ross LF. Why “doctor, if this were your child, what would you do?” deserves an answer. J Clin Ethics. 2003;14(1–2):59–62
46. Kon AA. Answering the question: “doctor, if this were your child,
what would you do?”Pediatrics. 2006;118(1):393–397
47. Truog RD. “Doctor, if this were your child, what would you do”? Pediatrics. 1999;103(1):153–154
48. Tucker Edmonds B, Torke AM, Helft P, Wocial LD. Doctor, what would you do? An ANSWER for patients requesting advice about value-laden decisions.
Pediatrics. 2015;136(4):740–745 49. Huang L, Yin Y, Yang L, Wang C, Li
Y, Zhou Z. Comparison of antibiotic therapy and appendectomy for acute uncomplicated appendicitis in children: a meta-analysis. JAMA Pediatr. 2017;171(5):426–434 50. Lopez ME, Wesson DE. Medical
treatment of pediatric appendicitis: are we there yet? JAMA Pediatr. 2017;171(5):419–420
51. Bachur RG, Rangel SJ. The threat of diagnostic uncertainty in the medical management of uncomplicated appendicitis. JAMA Pediatr. 2017;171(6):505–506
52. American Academy of Pediatrics Task Force on Circumcision. Male circumcision. Pediatrics. 2012;130(3). Available at: www. pediatrics. org/ cgi/ content/ full/ 130/ 3/ e756
53. Montori VM, Gafni A, Charles C. A shared treatment decision-making approach between patients with chronic conditions and their clinicians: the case of diabetes. Health Expect. 2006;9(1):25–36
54. Weiss EM, Barg FK, Cook N, Black E, Joffe S. Parental decision-making preferences in neonatal intensive care.
J Pediatr. 2016;179:36–41.e3
55. Müller-Engelmann M, Keller H, Donner-Banzhoff N, Krones T. Shared decision making in medicine: the influence of situational treatment factors. Patient Educ Couns. 2011;82(2):240–246
56. Kaplan RM. Shared medical decision making. A new tool for preventive medicine. Am J Prev Med. 2004;26(1):81–83
DOI: 10.1542/peds.2018-0516E
2018;142;S149
Pediatrics
Douglas J. Opel
A 4-Step Framework for Shared Decision-making in Pediatrics
Services
Updated Information &
http://pediatrics.aappublications.org/content/142/Supplement_3/S149 including high resolution figures, can be found at:
References
#BIBL
http://pediatrics.aappublications.org/content/142/Supplement_3/S149 This article cites 49 articles, 10 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2018-0516E
2018;142;S149
Pediatrics
Douglas J. Opel
A 4-Step Framework for Shared Decision-making in Pediatrics
http://pediatrics.aappublications.org/content/142/Supplement_3/S149
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.