MOVEMENT EFFICIENCY IN CHRONIC ANKLE INSTABILITY PATIENTS: EXAMINING THE INDIVIDUAL MOVEMENT ERRORS IN
FUSIONETICS AND THE LANDING ERROR SCORING SYSTEM
By: Amina Ali Khan
A thesis defense submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for graduation with honors in the Department of Exercise
and Sports Science
2018
Approved by:
TABLE OF CONTENTS
CHAPTER I: INTRODUCTION...1
CHAPTER II: REVIEW OF LITERATURE...3
Epidemiology...3
Risk Factors and Adaptations...5
Dynamic Tasks in CAI...7
Star Excursion Balance Test...7
Drop-Jump Landings...8
Landing Error Scoring System-17...9
Fusionetics...10
CHAPTER III: METHODS...12
3.1 Research Design...12
3.2 Participants...12
3.3 Procedures...13
3.4 Statistical Analysis...14
CHAPTER IV: RESULTS...15
Demographics...15
Group Differences...15
CHAPTER V: DISCUSSION...18
Sample Comparison...18
Group Differences...20
Squat...20
Limitations...23
Clinical Implications and Further Research...23
Conclusions...24
APPENDICES...25
APPENDIX 1: FUSIONETICS ERROR CHECKLIST...25
APPENDIX 2: FUSIONETICS MOVEMENT TASKS...26
APPENDIX 3: LANDING ERROR SCORING SYSTEM ERRORS AND SAMPLE...27
CHAPTER I: INTRODUCTION
Ankle sprains involving injury to the lateral ligaments of the joint are one of the most frequent injuries in athletics.1 The mechanism of lateral ankle sprains (LAS) involves plantar
flexion and inversion, which commonly results in damage to the anterior talofibular ligament (ATFL) first, followed by the calcaneofibular ligament (CFL) and the posterior talofibular ligament (PTFL).2 Those who continue to have recurrent ankle sprains can develop chronic
instability; as many as 10-30% of individuals with a LAS develop some form of chronic ankle instability (CAI).3 Hertel4 defines CAI as “repetitive bouts of lateral ankle instability resulting in
numerous ankle sprains.” Characteristics of CAI include pain and swelling within the joint, mechanical and functional instability, recurrent sprains, and a decrease in strength of the surrounding musculature.5
The breakdown of CAI consists of two different components: mechanical instability and functional instability. Mechanical instability is defined as increased accessory movements due to laxity in ligamentous structures and joint dysfunction.6 Functional instability usually exists in
conjunction with mechanical instability and is defined as having proprioceptive and
neuromuscular deficits after LAS.4 While the relationship between these two forms of instability
has not been fully investigated, research has shown that they can be mutually exclusive.4
Risk factors for LAS have been identified as BMI, previous injury, muscle strength, joint laxity, and limb dominance.7 Previous injury has been shown to be the most predictive risk factor
for recurrent ankle sprains.2 Balance can be split into two categories: static and dynamic stability.
Functional tasks have been used to distinguish movement patterns in those with CAI and those without. The Star Excursion Balance Test has been used as an outcome to measure
movement dysfunction through measuring dynamic stability in balance-reach tasks.9 Drop-jump
landings can also be used to look at how well an individual can control their lower extremities after landing.10 It is hypothesized that the ankle’s position changes during a jump, which then
leaves it more susceptible to injury upon landing; therefore, drop-jump landing tests are helpful in identifying kinematic and biomechanical changes that may happen during activity.11
The Landing Error Scoring System-17 (LESS-17) is a reliable and valid test that can be used without laboratory equipment, thus making it appropriate in clinical settings.12 It can be
used to detect risks for knee injuries based on assessing errors made in jump-landing tasks.12 The
Fusionetics Movement Efficiency Screening is a tool that can also be used in a clinic. It
examines errors made during functional movement tasks and assigns rehabilitation protocols to those errors in order to improve overall movement efficiency scores.13 Because both tools can be
used with and without laboratory equipment, both are clinically applicable and may be helpful in screening athletes who may have potential for an increased risk for ankle injuries. However, previous research suggests that the overall movement scores are not sensitive to differences between uninjured controls and those with CAI, perhaps because some elements of the tasks mask differences present in other elements. Therefore, the purpose of this study is to determine if looking at the individual errors of the Fusionetics and LESS-17 screenings is a more sensitive measurement than the overall scores to detect differences between individuals with CAI and uninjured controls. We hypothesize that the individual percentages of errors at the ankle
CHAPTER II: REVIEW OF LITERATURE Epidemiology
The development of CAI is thought to come from a lack of proper functional rehabilitation after an ankle injury—most commonly a lateral ankle sprain (LAS).14 The
mechanism of injury for a LAS involves inversion of the foot at a high velocity, causing damage primarily to the anterior talofibular ligament (ATFL) followed by the calcaneofibular ligament (CFL), as well as dynamic structures such as the peroneal tendons.15 Rates of injury vary based
on upon age, population, gender, and activity levels. One study shows the incidence rate within high school athletes is 3.65 incidents per 10,000 athlete exposures.16 An estimated $4.4 billion is
spent on the treatment of lateral ankle sprains annually, with over 2 million sprains occurring in the United States every year.17,18 Lateral ankle sprains account for almost 20% of sports-related
injuries and recurring symptoms from injury can last as long as 1 year after the initial incident.19
Residual symptoms include sensorimotor dysfunction and mechanical instability. If these symptoms persist long enough, they can be considered contributors to chronic ankle instability (CAI). The condition of CAI is defined by feelings of giving way, repeated sprains, and further functional deficits associated with the recurring acute sprains.17
The risks involved with recurrent ankle sprains are enough to warrant increased medical attention and awareness after an individual suffers an initial LAS. Additional persisting issues after a first-time ankle sprain can include impingement of the joint capsule, peroneal tendon pathologies, and eventually ankle osteoarthritis.20 After an initial LAS, recurrent sprains occur in
73% of athletes.21 Residual symptoms have been shown to persist from anywhere between 6 and
About 20% of individuals that have suffered LAS have symptoms of CAI lasting at least 5 years after the incident.23 Two studies used radiography for imaging and found the presence of
talocrural osteoarthritis in individuals with persistent symptoms.24,25 Additionally, about 56% of
individuals had lesions to the ATFL in their injured ankle, as well as bone marrow edema and osteochondral lesions at the talocrural joint when examined with magnetic resonance imaging.25
The presence of osteoarthritis indicates some sort of structural modifications made in response to the recurrent sprains.26
Mechanical ankle instability involves ligamentous impairments at the joint, often associated with ligamentous laxity resulting from injury.27 Functional ankle instability refers to
the impairments in neuromuscular control, proprioception, strength, and postural control that occur after recurrent ankle sprains.27 Self-report questionnaires (i.e. patient reported outcomes)
are a valid method to quantify functional instability.17,28 It is hypothesized that there is a
relationship between these two forms of instability, but the exact causality is not known. Hertel4
noted that functional and mechanical instability could be present together in the same talocrural joint. He hypothesized that certain protective mechanisms, including strength and proprioceptive changes, are taken to try and prevent additional sprains.4 However, these functional and
mechanical changes can accumulate with repeated sprains and lead to the development of CAI if not addressed.
predictive measure for determining an individual’s status as a coper versus developing some form of CAI is their perceived outcomes (i.e. patient reported outcomes).
Risk Factors and Adaptations
Because CAI exists as a long-term stability and functionality problem, it is important to understand all aspects of ankle sprains and what predisposes individuals to this injury.
Pourkazemi et al.30 conducted a study in which the researchers compared the changes to the
ankle joint after an injury with individuals who had never sustained an ankle injury before. The results noted risk factors such as previous injury, postural stability, functionality, and motor control. Fong et al.31 conducted a review of the literature and determined an increased foot width,
plantar-flexion strength, and limb dominance were also intrinsic risk factors for ankle sprain injury.
Risks for injuries increase due to previous injury. One prospective study looked at the prevalence of lower extremity injuries, including ankle sprains, and how previous injury affected those rates. It was concluded that previous injury put athletes at a higher risk for injuring the same leg in subsequent seasons.32 It is estimated that between 31-40% of individuals who have
had previous LAS develop CAI in their lifetime.27
Chen et al.33 looked at postural sway in subjects with functional and mechanical
population. Another study found that functional instability and the perception of feeling unstable also contributes to postural sway when balancing on the foot with CAI symptoms.5
Deficits in range of motion can also be identified as risk factors for CAI. A lack of dorsiflexion has been shown to be a predictive factor for ankle sprains by preventing the
talocrural joint from achieving a full, closed-packed position of stability.4,34 Additionally, muscle
strength imbalances involving the groups that perform these functions have also shown to to be present in those with CAI. Baumhauer et al.35 found that individuals who had sustained ankle
sprains had a larger eversion-to-inversion ratio and were at a higher risk for ankle injury. Dynamic stability has also been found to be altered in those with CAI. Ross and
Guskiewicz36 found that individuals with ankle instability took longer to stabilize after a
single-leg jump-landing task. Rehabilitation programs focusing on balance and stability training have also demonstrated a decrease in injury rates in sports teams.37 It is hypothesized that the muscles
of the lower leg provide a protective mechanism for the ankle during landing and balancing tasks. The ability to properly co-contract is thought to be compromised due to ankle injury, which can then lead to recurrent LAS.7
It has been reported that proprioception is also altered in individuals who have suffered an ankle sprain. One study compared proprioceptive measures of seated plantar-/dorsiflexion and inversion/eversion between an ankle-sprain group and a control group of basketball players. They found that certain movements, particularly dorsiflexion and inversion proprioception, were more varied in the ankle-sprain group.8
Chronic ankle instability can be identified through various functional tasks. The
differences between how CAI individuals and healthy controls perform on these tasks can help determine what deficits exist and how they may contribute to a subject’s movement ability. One such test is the Star Excursion Balance Test (SEBT). The SEBT is a clinical tool used to measure neuromuscular control during dynamic balance tasks and can identify deficits in those
movements.38 The test involves an individual balancing on one leg and reaching in eight different
directions; variables measured are reach distance and compensations during dynamic balancing. However, Hertel et al.39 determined that the posteromedial reach is an accurate representation of
all eight directions, thus making the test more time-efficient.
One study looked at the relationship between hip strength and dynamic stability in subjects with CAI, copers, and healthy controls. They found that subjects with CAI had worse dynamic control in the anterior reach of the SEBT, though future research is still needed to confirm that hip involvement is the primary reason for variance in those scores.40 Hertel et al.39
found significant reach deficits in the CAI group in the anterior, posteromedial, and
posterolateral directions when compared to healthy controls, but De La Motte et al.41 found no
significant differences in reach between CAI and controls. However, movement-pattern differences were identified, specifically trunk and pelvic rotation in the CAI group during the reach tasks. Therefore, compensatory movement strategies may be an adjustment to try and improve dynamic stability during activity in individuals with CAI.
also requires neuromuscular control and activation of the entire lower extremity, so the knee and hip joints are also included in measuring reach capabilities. However, the fact that the SEBT can be used in physical examinations as an overall predictor of lower extremity injury is of note. More research should be done in order to determine if individuals with CAI can be identified through SEBT scores.
Drop-Jump Landings
Drop-jump landings have been used to identify biomechanical differences and response to ground-reaction forces during drop or jump landing tasks.10 One study also used the drop-jump
landing as an outcome measure for a neuromuscular training program in female athletes.10 The
use of drop-jump landing tasks has been proposed as a clinical tool to identify those at risk for ankle sprains. Differences in landing biomechanics in those with CAI and those without may be able to distinguish the exact risk factors for LAS.43
Drop-jump landings are also effective in determining the effect of ground-reaction force (GRF) on lower extremity injury. One study proposed that musculotendinous stiffness related to decreased range of motion affected landing biomechanics. More specifically, the ability for the joint to tolerate an eccentric load, such as a 1-meter drop jump.44 Fong et al.45 conducted a study
in which they measured passive dorsiflexion and landing dorsiflexion/knee flexion ankles during a drop-landing task. They found that individuals with an increased amount of dorsiflexion during landing (with associated knee flexion increase) experienced less GRF, therefore putting them in a more stable position and making the ACL less vulnerable to injury.45 This suggests that increased
conducted in order to identify if increased GRF has a specific effect on individuals with CAI and their recurrence of sprains.
Jump-landing tasks seem to be effective predictors of movement patterns that put individuals at risk for injury because of their nature of mimicking activity. Stop-landing tasks, for example, involve quick acceleration to a jump, then jumping to maximum height
immediately after the initial landing. Brown et al.46 found that individuals with mechanical ankle
instability had greater GRF and anterior talus translation due to laxity in the ATFL. This supports the finding that individuals with CAI, specifically mechanical instability, experience differences in sensorimotor responses during activity.47 Both of these types of dynamic landing tasks have
been able to indicate differences in biomechanics and neuromuscular activation between CAI individuals, copers, and healthy controls. However, often times they are not feasible due to the need for laboratory equipment and unavailability, so alternatives may be used.
LESS-17
The Landing Error Scoring System is a functional test used to test landing kinematics after a drop jump off a box and a maximal counter-movement jump. Scoring for the test involves counting the errors made when landing, which include trunk and lower extremity positioning upon landing, feet position, and displacement of joints in the frontal and sagittal planes. Higher scores indicate more errors made in landing.
The LESS-17 is a reliable and valid test for determining movement errors during jump-landing tasks, with good inter-rater reliability and excellent intra-rater reliability.12 It has been
used in screening tests as a means for ACL injury prevention. Padua et. al.48 found that out of a
remained uninjured. Those with poor LESS-17 scores had several problems with landing kinematics, which could then be targeted through specific injury prevention protocols. Though the use of the LESS-17 in ACL injury prevention is common, more data is needed to determine which specific errors are potential risk factors for injury. However, residual issues in CAI, such as a lack of dorsiflexion and eversion muscle activation, make looking at LESS-17 worthwhile. The presence or absence of an error can help determine what kind of compensations are being made, which can then lead to deficits being addressed and corrected to improve overall function in sport.
Fusionetics
Fusionetics is a performance health platform that scores movement efficiency in
individuals based on a set of various tasks. These screenings help identify potential weak areas such as biomechanical issues, stability problems. The software creates a self-care plan for athletes to correct faulty movement patterns. The movement efficiency patterns tracked by Fusionetics testing include a double-leg squat, a double-leg squat with a heel-lift, and a single-leg squat. Scores are computed through an algorithm within the software and are based on the ranges created by the Fusionetics platform: poor (0-49.99%), moderate (50-74.99%) and good (75-100%).13 These movements are then looked at based on individual compensations that a
person may have; a plan can then be generated to target the apparent deficiencies based on the scores.
should be able to indicate specific movement compensations in individuals that have certain pathologies. Fusionetics is also a helpful clinical assessment method because it combines proprioceptive and balance tasks that can also indicate compensatory movements, such as postural sway in CAI subjects.
A comparison has been done to determine if individuals with CAI compared to those who do not have movement issues and thus worse LESS-17 and Fusionetics scores. The results indicated that there were no significant differences in test scores between groups for both tests.49
However, what LESS-17 and Fusionetics show is an overage percentage of movement errors; in other words, a sum of the individual errors adds up to the total LESS-17 or Fusionetics score. The sensitivity of these tests may not be strong enough to let their total scores identify
CHAPTER III: METHODS 3.1 Research Design
This case-control study was performed to determine if the individual errors within the LESS-17 and Fusionetics are more sensitive than their respective overall scores in identifying CAI when compared to a control population. The independent variable was the group assignment (either CAI or control). The dependent variables were the individual LESS-17 and Fusionetics scores. The Fusionetics individual scores came from an overhead double-leg squat with and without heel lift, and the single-leg squat. Between-group outcomes were measured during preseason screenings.
3.2 Participants
Ninety-nine participants from ages 18-35 from the University of North Carolina at Chapel Hill were subjects in this study. These participants were all varsity athletes and participated in at least three thirty-minute sessions of sports-related activity a week. Inclusion and exclusion from the study was determined by the criteria set forth by the International Ankle Consortium 47. Subjects were included in the CAI group if they had a history of at least one ankle
sprain happening >12 months from enrollment; the sprain also had to have inflammatory
inability to perform physical activity for at least a day. This study was approved by the Institutional Review Board (IRB) of the University of North Carolina at Chapel Hill. 3.3 Procedures
Two main movement efficiency tests were used: Fusionetics and the LESS-17. The Fusionetics test used in this study was the Movement Efficiency (ME) screen, which consists of seven total tasks. Only lower extremity tasks were performed for the purposes of this study. Scores were determined based on the compensations made when performing the overhead squat with and without heel lifts and the bilateral single leg squat. Verbal cues were given to the participants to perform the task. For both overhead squats: “feet shoulder width apart, toes pointing straight ahead, arms fully extended by your ears. Now, squat down to the height of a chair.” Before performing the overhead squat with a heel lift, a weight plate was used to elevate the heels.
Instructions for the single legs squats were as follows: “toes facing forward, balance on one leg with hands on hips and squat to the height of a chair.” The evaluator assessed each movement task from a front, side, and back view. Each view had a list of compensations to watch for at each checkpoint (ankle, knee, and hip). If the compensation was made (i.e. foot turns out, low back rounds, asymmetrical weight shift), it was marked on the appropriate side.
The second clinical test used in the procedure was the Landing Error Scoring System-17 (LESS-17). The LESS-17 involves participants standing on a 30cm box at a distance 50% of the participant’s height away from the landing target. The participants were instructed to jump off the box with both feet, landing in the target area and then immediately jumping straight up as high as they could. The PhysiMax Software determined a successful test using the videos of the jumps taken by a Microsoft Kinect Camera. The LESS-17 has an inter-rater reliability of .72 to .81.50 For the LESS-17, three trials of the drop-landing jump were performed and immediately
scored with the Physimax Software to determine if the jumps were successful. A list of errors can be found in Appendix 3.
3.4 Statistical Analysis
CHAPTER IV: RESULTS Demographics
Ninety-nine subjects from six Division I NCAA sports met the inclusion and exclusion criteria. These subjects were previously separated into each group based on their IdFAI scores. The FAAM-S questionnaire was used to determine overall level of perceived disabiilty for each subject. Forty-nine participants were determined to have CAI and fifty participants were part of the uninjured control group. Nonparametric statistics were used prior to this study to determine that there were no differences in age, height, and weight between groups. The number of
participants in each group per sport can be found in Table 4-1. The demographics of the subjects can be found in Table 4-2.
Table 4-1: Number of participants per sport
Sport CAI Control
Women’s Crew 10 9
Field Hockey 6 8
Men’s Soccer 9 12
Women’s Soccer 4 3
Men’s Lacrosse 11 14
Women’s Lacrosse 9 4
Total 49 50
Table 4-2: Demographics of subjects per group
Group Sex Age Weight
(kg)
Height (cm) IdFAI FAAM-S # of sprains
M F
CAI 20 29 19.86±1.24 68.59±3.14 159.41±25.67 15.63±3.86 94.58±9.61% 2.69±2.22 Control 26 24 19.64±1.08 69.82±3.54 159.82±25.94 1.20±2.30 98.82±5.42% 0
Group Differences
squat showed differences in the proportion of individual’s who made an uncontrolled trunk movement. No specific correlations were found between the presence of CAI and the frequency of errors made during each movement task. Tables listing the percentages of errors made per group and their respecitve signficance values (1-sided) can be found below.
Table 4-3: Specific movement compensations (errors) made during the
double limb squat. Data are presented as the percentage of participants that committed a specific compensation.
Checkpoin
t Movement compensations Control (n=50) CAI (n=49) Significance
Foot/Ankle Foot Turns Out 54.0% 55.1% 0.537
Foot Flattens 28.0% 22.4% 0.343
Heel of Foot Lifts 6.0% 6.1% 0.651
Knee Knee Valgus 16.0% 16.3% 0.590
Knee Varus 30.0% 36.7% 0.310
L-P-H-C Excessive Forward
Lean 68.0% 65.3% 0.472
Low Back Combined 42.0% 46.9% 0.385
Asymmetrical Weight
Shift 48.0% 42.8% 0.378
Shoulder Arms Fall Forward 64.0% 59.2% 0.387
L-P-H-C: Lumbo-pelvic-hip complex
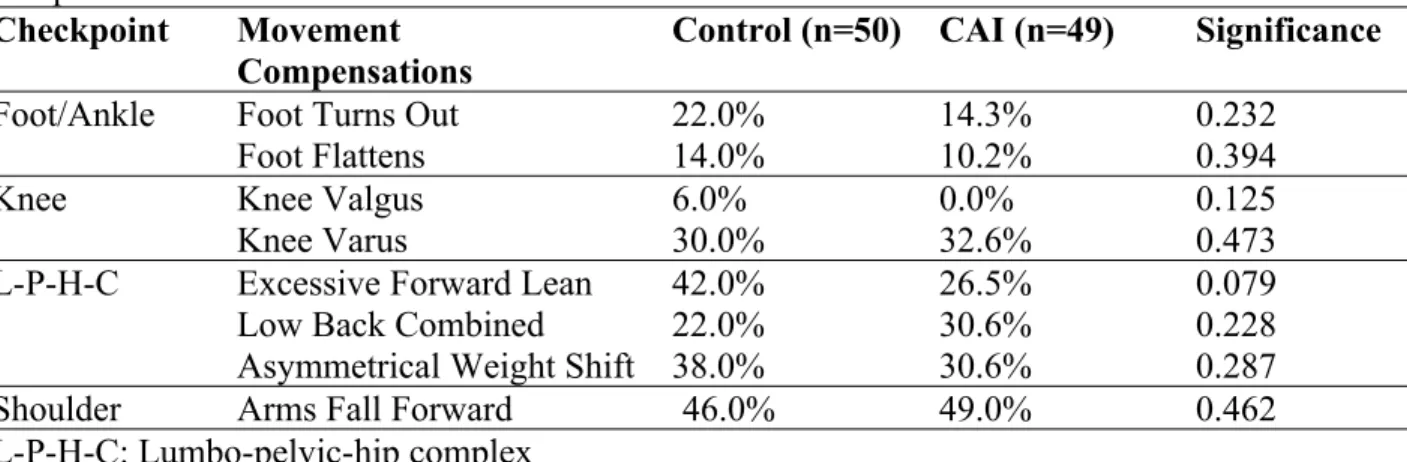
Table 4-4: Specific movement compensations (errors) made during the double limb squat with heel lift. Data are presented as the percentage of participants that committed a specific
compensation.
Checkpoint Movement Compensations
Control (n=50) CAI (n=49) Significance
Foot/Ankle Foot Turns Out 22.0% 14.3% 0.232
Foot Flattens 14.0% 10.2% 0.394
Knee Knee Valgus 6.0% 0.0% 0.125
Knee Varus 30.0% 32.6% 0.473
L-P-H-C Excessive Forward Lean 42.0% 26.5% 0.079
Low Back Combined 22.0% 30.6% 0.228
Asymmetrical Weight Shift 38.0% 30.6% 0.287
Shoulder Arms Fall Forward 46.0% 49.0% 0.462
Table 4-5: Specific movement compensations (errors) made during the single limb squat. Data are presented as the percentage of participants that
committed a specific compensation. Checkpoin
t Movement Compensation Control (n=50) CAI (n=49) Significance
Foot/Ankle Foot Flattens 42.0% 38.8% 0.452
Knee Knee Valgus 68.0% 75.5% 0.272
Knee Varus 14.0% 12.2% 0.516
L-P-H-C Uncontrolled Trunk
Motion 50.0% 75.5% 0.008*
Loss of Balance 34.0% 24.5% 0.207
L-P-H-C: Lumbo-pelvic-hip complex
Table 4-6: Specific movement compensations (errors) made during the Landing Error Scoring System (LESS-17) test. Data are presented as the percentage of participants that committed a specific error.
Body
Part Error Control (n=50) CAI (n=49) Significance Foot/
Ankle IC Plantar flexion Angle 38.0% 42.8% 0.387
Asymmetrical Foot
Contact 18.0% 36.7% 0.074
Wide Stance 0.0% 0.0%
--Narrow Stance 76.0% 73.5% 0.477
Foot Internal Rotation 0.0% 2.0% 0.495
Foot External Rotation 42.0% 51.0% 0.243
Knee IC Knee Flexion 8.0% 16.3% 0.168
Medial Knee Position 14.0% 22.4% 0.204
Knee Displacement 20.0% 14.3% 0.314
Maximum Medial Knee
Displacement 32.0% 32.6% 0.558
Hip IC Hip Flexion 0.0% 0.0%
--Hip Displacement 14.0% 10.2% 0.394
Trunk IC Trunk Flexion 2.0% 4.1% 0.492
Lateral Trunk Flexion 34.0% 34.7% 0.555
Excessive Trunk Flexion
CHAPTER V: DISCUSSION
The purpose of this study was to analyze the movement quality in subjects with CAI and healthy controls using the three lower extremity Fusionetics tasks (DL squat, DL squat with heel lift, and SL squat) and the LESS-17. Our hypothesis proposed that in subjects with CAI, the percentages of errors committed would be higher (i.e. worse movement efficiency) compared to the control group. The results from this study failed to support our a priori hypotheses fully. However, there are findings worth discussion and may fuel future research.
Sample Comparison
The inclusion criteria for this study consisted of having sustained at least one lateral ankle sprain prior to enrollment in the study, as well as at least two episodes of giving way within six months prior to enrollment, which is consistent with studies referenced in the literature.26,30,36,40,51
One study did not specify participants needing to demonstrate feelings of giving way, solely requiring a history of recurrent ankle sprains.5 Additionally, subjects in the CAI group for our
study were to have scored >10 on the IdFAI. Two papers implement the use of the IdFAI, one of which investigaed spinal reflex excitability and joint-laxity measures, and the other measured hip strength and SEBT deficits in those with CAI.40,51 Both studies required that the participants
subject has CAI.5,17,26,29,30,36,40,41,51 Houston et al. attempts to differentiate the use of these tools,
stating the CAIT and the AII are “discriminative tools” that are validly able to determine if an individual has CAI. The FAAM-S and the FADI are more questionnaires that determine an individual’s functional limitations within CAI.17 The IdFAI has been shown to have good
reliability in identifiying individuals who should be included in a CAI population for research purposes (Gurav, 2014 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4215489/). Though evidence suggests that in general, there lacks a consensus regarding true inclusion criteria for CAI, the International Ankle Consortium recommends the use of the majority of those mentioned above.47,52
It is not known if this particular sample population contributed to the lack of group differences. Having Division I NCAA athletes across a wide variety of sports—some of which may not have aspects of competition that could directly lead to a lateral ankle sprain (i.e. women’s crew)—may have made our sample size too homogenous due to their higher levels of functioning during activity. McCriskin reports that intensity of competition and skill level of participants does effect the risk of ankle sprains, noting an increased risk in collegiate athletes.18
However, this paper also notes decreased risks in certain sports, which may suggest that the higher skill level required of intercollegiate athletes may cause changes in the relative incidence rates of ankle sprains among populations similar to that of this study.18 While no studies in the
al.’s paper (101.4%LL ± 16.4% vs. 80.13% ±10.34%).41,53 This data could support McCriskin’s
idea that athletes involved in higher levels of competition may influence ankle stability and risk for ankle injury in that it may decrease their risk as their movmenets become more efficient in their respecitve sport.
Group Differences Squat
Because the Fusionetics scores are calculated with a propriatary scoring algorithm, certain errors are weighed more heavily than others. It is not known if this weighting favors certain errors over others due to the fact that the algorithm only involves a “yes/no” input from the test administrator; thus, it is difficult to determine if the overall scores would change if ankle-specific errors were weighed more favorably. This investigation focused on the presence of an individual error but we were unable to account for the severity of an error and this may be an important factor that current movement screening procedures do not account for. Errors at the ankle were the concern; however, the overall scores only accounted for the frequency of errors made, not how severe they were.
Postural stability is an area within the investigation of chronic ankle instability that has been widely researched. Gribble et al.9 and McCann et al.40 both concluded that individuals with
CAI had compromised dynamic postural stability in the anteromedial direction when using the SEBT as the evaluative tool. Similarly, in Hertel et al.’s39 analysis of the simplification of the
SEBT, the anteromedial and posteromedial directions had signficant reach differences between groups, with the CAI group having a shorter distance. The SEBT is a postural control and balance assessment tool that can validly and reliably screen for lower extremity injury risk.42 The
SEBT—one could argue that it requires more control based on the goal of each task (depth of squat vs. reach distance). The only significant difference found between groups in this study came from the single-leg squat task. Individuals with CAI exhibited more uncontrolled trunk motion compared to healthy controls. The single-leg squat most closely mimics a reach in the anterior direction, which has also been identified as a potential direction for group differences to occur.40
Jump Landings
Jump landing tasks have been used to try and identify differing landing biomechanics in those with CAI and those without. The use of the LESS-17 in this study was to try and pinpoint where landing errors were occuring during the clinician-oriented task. While no significant differences were noted, those with CAI more frequently demonstrated a knee flexion angle error at initial contact and also made more asymmetrical foot contact errors. It could be argued that errors may be due to a lack of dorsiflexion, which has already been identified as a risk factor for developing CAI, but the Physimax scoring software used in this study did not indicate any differences in dorsiflexion or any other range of motion values between groups.4
Movement variability has been analyzed to determine if those with functional and/or mechanical instability are at a higher risk for having more episodes of giving way. Brown et. al46
examined the movement patterns during a stop-jump task, which is similar to the LESS-17. They found signficant group differences that indicated more frontal plane movement may increase the risk of instability.46 Uncontrolled trunk motion has some potential to incorporate frontal plane
movement when an individual is attempting to stabilize, and this was the only noted difference between groups in this study. Previous studies in the literature have also investigated the
major differences. Delahunt et al.11 found more frontal plane motion, increased GRF, and
increased inversion upon landing in those with functional ankle instability. The LESS-17 technology used in this study was unable to detect ankle inversion angles, so it is difficult to determine if those measures found in Delahunt et al. would necessarily be true in this study.
Though there is sufficient evidence to show that the LESS-17 is a valid and reliable tool to analyze jump-landing biomechanics, success has primarily been focused at the knee.12 Padua
et al.48 used the LESS-17 to screen for ACL injury risk in youth soccer players, with the most
predictive factors for injury being trunk-flexion displacement, hip-flexion displacement, joint displacement, trunk flexion: initial contact, foot position: external rotation, and knee-flexion displacement. The ability for those investigators to identify predisposing errors at the knee was what this study was trying to recreate. The individual errors associated with the LESS-17 in this study did not indicate major overall differences in the drop-jump landings between groups— further research might explore whether this test can be applicable in prevention screening for other injuries.
It is also important to mention the fact that though the experimental group reported higher FAAM-S scores, self-perceived CAI is still present. While we cannot fully assert why these athletes are still reporting some sort of disability when there is only one group difference, it may be once again due to their elite nature. One could argue that their sport specialization and
Limitations
This study had several limitations. Firstly, one of the largest limitations was that we were not able to distinguish errors between the involved and uninvolved limbs as our statistics were run as combined errors. Though we found one difference, the percentage of the errors made on the injured versus uninjured limbs is not specified. Therefore, we cannot determine if the full 75% of the CAI individuals that made the single leg squat error made the error on their injured leg. Secondly, the subjects used were Division I NCAA athletes who function at a uniquely high level of sport. While the population itself may not have been a limitation as it sparks the interest for further research on how elite athletic populations may influence data on sport performance, the results from this study may not be able to be applied to other populations such as
recreationally active or adolescent athletes. Another potential limitation is that the equipment used during data collection is not research oriented—the LESS-17 and Fusionetics are designed to be used clinically. This could lead to inaccuracies such as errors made from test
administrators, and could make small differences undetectable between groups. Finally, the majority of errors within these two tests are centered around the knee. Additionally, much of the research done with these tests, especially the LESS-17, are focused on knee injuries. Therefore, these may not be the most suited for detecting specific errors at the ankle.
Clinical Implications and Further Research
predisposition to injury. However, these tests may not be sensitive enough to differentiate between group with and without a pathology—in this case, CAI. Therefore, these tasks likely cannot be used with their current technology to pick up on risk factors for ankle injury. Because one difference was noted in the single leg squat task, further research could be geared toward investigating screening tools focused on single leg squat tasks and trunk motion in patients with ankle instability.
Conclusions
APPENDIX 1: Fusionetics Error Checklist
2-leg Squat
Checkpoint Compensation Right Left View: Front
Foot/ankle Foot turns out Foot flattens
Knee Knee moves in (valgus)
Knee moves out (varus)
View: Side
L-P-H-C Excessive forwardlead
Low back arches
Low back rounds
Shoulder Arms fall foward
View: Back
Foot/ankle Heel of foot lifts
L-P-H-C Asymmetrical weight shift
2-leg squat with heel lift
Checkpoint Compensation Right Left View: Front
Foot/ankle Foot turns out Foot flattens
Knee Knee moves in (valgus)
Knee moves out (varus)
View: Side
L-P-H-C Excessive forwardlead
Low back arches
Low back rounds
Shoulder Arms fall foward
View: Back
L-P-H-C Asymmetrical weight shift
Checkpoint Compensation Right Left View: Front
Foot/ankle Foot flattens
Knee Knee moves in (valgus)
Knee moves out (varus)
L-P-H-C Uncontrolled trunk: flexion, rotation, and/or hip shift Loss of balance
REFERENCES
1. Chan KW, Ding BC, Mroczek KJ. Acute and chronic lateral ankle instability in the athlete. Bull NYU Hosp Jt Dis. 2011;69(1):17–26.
2. Hubbard TJ, Wikstrom EA. Ankle sprain: pathophysiology, predisposing factors, and management strategies. Open access J Sport Med [Internet]. 2010;1:115–22. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/24198549%5Cnhttp://www.pubmedcentral.nih.gov/ articlerender.fcgi?artid=PMC3781861
3. Peters J, Trevino S, Renstrom P. Chronic Lateral Ankle Instability. Foot Ankle Int. 1991;12(3):182–91.
4. Hertel J. Functional Instability Following Lateral Ankle Sprain. Sport Med [Internet]. 2000;29(5):361–71. Available from: http://link.springer.com/content/pdf/10.1007/978-1-4613-1107-2_51.pdf
5. Hiller CE, Kilbreath SL, Refshauge KM. Chronic ankle instability: Evolution of the model. J Athl Train. 2011;46(2):133–41.
6. Denegar CR, Miller SJ. Can chronic ankle instability be prevented? Rethinking management of lateral ankle sprains. J Athl Train. 2002;37(4):430–5.
7. Beynnon BD, Murphy DF, Alosa DM. Predictive factors for lateral ankle sprains: a literature review. J Athl Train [Internet]. 2002;37(4):376–80. Available from: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?
cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=12937558
8. Payne KA, Berg K, Latin RW. Ankle injuries and ankle strength, flexibility, and proprioception in college basketball players. J Athl Train. 1997;32(3):221–5.
9. Gribble PA, Hertel J, Plisky P. Using the star excursion balance test to assess dynamic postural-control deficits and outcomes in lower extremity injury: A literature and systematic review. J Athl Train. 2012;47(3):339–57.
10. Noyes FR, Barber-Westin SD, Fleckenstein C, Walsh C, West J. The Drop-Jump Screening Test. Am J Sports Med [Internet]. 2005;33(2):197–207. Available from: http://journals.sagepub.com/doi/10.1177/0363546504266484
11. Delahunt E, Monaghan K, Caulfield B. Changes in Lower Limb Kinematics, Kinetics, and Muscle Activity in Subjects with Functional Instability of the Ankle Joint during a Single Leg Drop Jump. J Orthop Res. 2006;24(10).
12. Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE, Beutler AI. The Landing Error Scoring System (LESS) Is a Valid and Reliable Clinical Assessment Tool of Jump-Landing Biomechanics. Am J Sports Med [Internet]. 2009;37(10):1996–2002. Available from: http://journals.sagepub.com/doi/10.1177/0363546509343200
13. Fusionetics. Fusionetics Home. Secondary Fusionetics Home. 2016; Available from: http://www.fusionetics.com/.
14. Al-Mohrej OA, Al-Kenani NS. Chronic ankle instability: current perspectives. Avicenna J Med [Internet]. 2016;6(4):103–8. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5054646/
15. Dubin JC, Comeau D, McClelland RI, Dubin RA, Ferrel E. Lateral and syndesmotic ankle sprain injuries: A narrative literature review. J Chiropr Med [Internet]. 2011;10(3):204– 19. Available from: http://dx.doi.org/10.1016/j.jcm.2011.02.001
Sports-Related Ligamentous Ankle Injuries, 2005/06-2010/11. 2014;23(3):190–6.
17. Houston MN, Hoch JM, Hoch MC. Patient-reported outcome measures in individuals with chronic ankle instability: A systematic review. J Athl Train. 2015;50(10):1019–33.
18. McCriskin BJ. Management and prevention of acute and chronic lateral ankle instability in athletic patient populations. World J Orthop [Internet]. 2015;6(2):161. Available from: http://www.wjgnet.com/2218-5836/full/v6/i2/161.htm
19. Petersen W, Rembitzki IV, Koppenburg AG, Ellermann A, Liebau C, Brüggemann GP, et al. Treatment of acute ankle ligament injuries: A systematic review. Arch Orthop Trauma Surg. 2013;133(8):1129–41.
20. Janssen KW, van Mechelen W, Verhagen EALM. Bracing superior to neuromuscular training for the prevention of self-reported recurrent ankle sprains: a three-arm
randomised controlled trial. Br J Sports Med [Internet]. 2014;48(16):1235–9. Available from: http://bjsm.bmj.com/lookup/doi/10.1136/bjsports-2013-092947
21. Yeung M, Chan K, So C, Yuan W. An epidemiological survey on ankle sprain. Br J Sports Med [Internet]. 1994;28(2):112–6. Available from:
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?
cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=7921910%5Cnpapers2:// publication/uuid/2C52E0D3-3144-482E-8AC6-69E3109DC39A
22. Braun BL. Effects of ankle sprain in a general clinic population 6 to 18 months after medical evaluation. Arch Fam Med. 1999;8:143–8.
23. Mailuhu A, Oei E, Putte-Katier Van N, van Ochten J, Bindels P, Bierma-Zeinstra S, et al. Clinical and radiological predictors for persistent complaints five years after a lateral ankle sprain: A long-term follow-up study in primary care. J Sci Med Sport. 2017;
24. Van Ochten JM, Mos MCE, Van Putte-Katier N, Oei EHG, Bindels PJE, Bierma-Zeinstra SMA, et al. Structural abnormalities and persistent complaints after an ankle sprain are not associated: An observational case control study in primary care. Br J Gen Pract.
2014;64(626):e545–53.
25. Van Putte-Katier N, Van Ochten JM, Van Middelkoop M, Bierma-Zeinstra SMA, Oei EHG. Magnetic resonance imaging abnormalities after lateral ankle trauma in injured and contralateral ankles. Eur J Radiol [Internet]. 2015;84(12):2586–92. Available from: http:// dx.doi.org/10.1016/j.ejrad.2015.09.028
26. Golditz T, Steib S, Pfeifer K, Uder M, Gelse K, Janka R, et al. Functional ankle instability as a risk factor for osteoarthritis: Using T2-mapping to analyze early cartilage
degeneration in the ankle joint of young athletes. Osteoarthr Cartil [Internet]. 2014;22(10):1377–85. Available from: http://dx.doi.org/10.1016/j.joca.2014.04.029 27. Hubbard TJ, Kramer LC, Denegar CR, Hertel J. Correlations among multiple measures of
functional and mechanical instability in subjects with chronic ankle instability. J Athl Train. 2007;42(3):361–6.
28. Carcia CR, Martin RL, Drouin JM. Validity of the foot and ankle ability measure in athletes with chronic ankle instability. J Athl Train. 2008;43(2):179–83.
29. Wikstrom EA, Tillman MD, Chmielewski TL, Cauraugh JH, Naugle KE, Borsa PA. Discriminating between copers and people with chronic ankle instability. J Athl Train. 2012;47(2):136–42.
31. Fong DT, Chan Y-Y, Mok K-M, Yung PS, Chan K-M. Understanding acute ankle ligamentous sprain injury in sports. BMC Sports Sci Med Rehabil [Internet]. 2009;1(1):14. Available from:
http://bmcsportsscimedrehabil.biomedcentral.com/articles/10.1186/1758-2555-1-14 32. Hagglund M. Previous injury as a risk factor for injury in elite football: a prospective
study over two consecutive seasons. Br J Sports Med [Internet]. 2006;40(9):767–72. Available from: http://bjsm.bmj.com/cgi/doi/10.1136/bjsm.2006.026609
33. Chen H, Li H-Y, Zhang J, Hua Y-H, Chen S-Y. Differences in Postural Control Between Patients With Functional and Mechanical Ankle Instability. Foot Ankle Int.
2014;35(10):1068–74.
34. Willems TM, Witvrouw E, Delbaere K, Mahieu N, De Bourdeaudhuij I, De Clercq D. Intrinsic Risk Factors for Inversion Ankle Sprains in Male Subjects. Am J Sports Med [Internet]. 2005;33(3):415–23. Available from:
http://journals.sagepub.com/doi/10.1177/0363546504268137
35. Baumhauer JF, Alosa DM, Renström PAFH, Trevino S, Beynnon B. A Prospective Study of Ankle Injury Risk Factors. Am J Sports Med [Internet]. 1995;23(5):564–70. Available from: http://ajs.sagepub.com/content/23/5/564.abstract
36. Ross SE, Guskiewicz KM, Yu B. Single-leg jump-landing stabilization times in subjects with functionally unstable ankles. J Athl Train. 2005;40(4):298–304.
37. Faizullin I, Faizullina E. Effects of balance training on post-sprained ankle joint instability. Int J Risk Saf Med [Internet]. 2015;27(s1):S99–101. Available from: http://www.medra.org/servlet/aliasResolver?alias=iospress&doi=10.3233/JRS-150707 38. Gribble PA, Hertel J. Considerations for Normalizing Measures of the Star Excursion
Balance Test. Meas Phys Educ Exerc Sci [Internet]. 2003;7(2):89–100. Available from: http://www.tandfonline.com/doi/abs/10.1207/S15327841MPEE0702_3
39. Hertel J, Braham RA, Hale SA, Olmsted-Kramer LC. Simplifying the Star Excursion Balance Test: Analyses of Subjects With and Without Chronic Ankle Instability. J Orthop Sport Phys Ther [Internet]. 2006;36(3):131–7. Available from:
http://www.jospt.org/doi/10.2519/jospt.2006.36.3.131
40. McCann RS, Crossett ID, Terada M, Kosik KB, Bolding BA, Gribble PA. Hip strength and star excursion balance test deficits of patients with chronic ankle instability. J Sci Med Sport [Internet]. 2017;20(11):992–6. Available from:
http://dx.doi.org/10.1016/j.jsams.2017.05.005
41. De La Motte S, Arnold BL, Ross SE. Trunk-rotation differences at maximal reach of the Star Excursion Balance Test in participants with chronic ankle instability. J Athl Train. 2015;50(4):358–65.
42. Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star Excursion Balance Test as a Predictor of Lower Extremity Injury in High School Basketball Players. J Orthop Sport Phys Ther [Internet]. 2006;36(12):911–9. Available from:
http://www.jospt.org/doi/10.2519/jospt.2006.2244
43. Self BP, Paine D. Ankle biomechanics during four landing techniques. Med Sci Sports Exerc. 2001;33(8):1338.
44. Walshe AD, Wilson GJ. The Influence of Musculotendinous Stiffness on Drop Jump Performance. Can J Appl Physiol. 1997;22(2):117–32.
46. Brown CN, Padua DA, Marshall SW, Guskiewicz KM. Variability of motion in
individuals with mechanical or functional ankle instability during a stop jump maneuver. Clin Biomech. 2009;24(9):762–8.
47. Gribble PA, Delahunt E, Bleakley CM, Caulfield B, Docherty CL, Fong DTP, et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the international ankle consortium. J Athl Train. 2014;49(1):121–7. 48. Padua DA, DiStefano LJ, Beutler AI, De La Motte SJ, DiStefano MJ, Marshall SW. The
landing error scoring system as a screening tool for an anterior cruciate ligament injury-prevention program in elite-youth soccer athletes. J Athl Train. 2015;50(6):589–95. 49. Harriss JE. Detecting Movement Errors in Chronic Ankle Instability Patients: Comparing
Fusionetics to the LESS. 2017.
50. Padua D, Boling M, Distefano L, Al E. Reliability of the landing error scoring system-real time, a clinical assessment tool of jump-landing biomechanics. J Sport Rehabil.
2011;20(2):145–56.
51. Bowker S, Terada M, Thomas AC, Pietrosimone BG, Hiller CE, Gribble PA. Neural excitability and joint laxity in chronic ankle instability, coper, and control groups. J Athl Train. 2016;51(4):336–43.
52. Yu B, Lin C-F, Garrett WE. Lower extremity biomechanics during the landing of a stop-jump task. Clin Biomech. 2006;21(3):297–305.