_____________________________________________________________________________________________________
www.sciencedomain.org
A Regression Model to Predict Diameter of Mitral
Valve Prosthesis Preoperatively: An Aid to Clinical
Decision Making
Praveen Sharma
1, Ankur Joshi
2*, B. S. Yadav
3, Saket Kale
4, M. C. Songara
51Department of Cardio-Thoracic and Vascular Surgery, Gandhi Medical College, Bhopal,
Madhya Pradesh, India. 2
Department of Community Medicine, Gandhi Medical College, Bhopal, Madhya Pradesh, India. 3
Department of Cardiology, Gandhi Medical College, Bhopal, Madhya Pradesh, India. 4Technical Support Unit, Madhya Pradesh State AIDS Control Society, India.
5Department of Surgery, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
Authors’ contributions
This work was carried out in collaboration among all authors. Author PS raised the issue, took all intra-operative measurements, wrote the clinical protocol and assisted author AJ to think critically. Author AJ shaped the idea, designed the study, wrote the statistical protocol, analyzed the data and wrote first draft of manuscript. Author BSY primarily performed all the Echocardiography pre-operatively and assisted authors PS and AJ to prepare the protocol. Author SK managed the literature
search and assisted author AJ in modeling. Author MCS helped author PS in intra-operative measurement, provided technical inputs and assisted in literature search. All authors read and approved the final manuscript.
Article Information
DOI: 10.9734/BJMMR/2015/16835 Editor(s): (1)Gaetano Santulli, College of Physicians and Surgeons Columbia University Medical Center, New York, USA. Reviewers: (1)Francesco Nappi, Department of Cardiac Surgery, Centre Cardiologique du Nord, St. Denis, France.
(2)Anonymous, USA. (3)John Skoularigis, Cardiology Department, Larissa University Hospital, Greece. Complete Peer review History:http://www.sciencedomain.org/review-history.php?iid=1116&id=12&aid=9012
Received 15th February 2015 Accepted 11th April 2015 Published 28th April 2015
ABSTRACT
Aim: Accurate estimation of the prosthetic valve size pre-operatively can aid to the efficiency and effectiveness to mitral valve surgery. Traditionally Two dimensional Echocardiography is being used for this purpose but cannot be claimed as optimum tool. This study computes and analyses several linear regression equations in order to obtain a best fit model for predicting mitral
prosthesis size well before operation.
Materials and Methods: This hospital based longitudinal study was conducted in a tertiary care Cardio Thoracic Vascular Department from August 2011 to August 2012. A total of 67 participants suffering from Rheumatic Heart Disease (with severe mitral valve disease) were recruited. Short and long axis of the mitral annulus were measured through 2-dimensional transthoracic echocardiography. Further three regression models were plots using short axis, long axis and area of the annulus as independent variables and diameter of prosthetic valve as dependent variable. Results: Among the three predictors namely the anterio-posterior axis (short axis), commissure-commissural axis (long axis) and area of mitral valve annulus; the regression equation with short axis predicted the diameter of prosthesis more accurately. The optimum regression model for short axis is calculated as -Diameter of prosthetic valve= -0.165 + 0.769X short axis of Ellipse. The coefficient of determination for this equation (R2) is 0.905. This equation offers the explanation for maximum observations in the model (F=609.48).
Conclusion: The size of optimum prosthetic valve may be determined preoperatively as a function of anterio-posterior axis (short axis) of annulus through non invasive 2-D Echocardiography. However this finding is amenable for further multi-centric validation.
Keywords: Mitral valve annulus; two dimensional transthoracic echocardiography; regression model; rheumatic heart disease.
1. INTRODUCTION
Cardiovascular events have achieved the infamous paramount rank as leading cause of mortality world-wide [1]. Of all the cardiovascular surgeries, valvular heart disease shares a substantial contribution of 10-20% among all the cardiovascular surgies [2]. Mitral valve affliction due to Rheumatic Heart Disease in developing world shares a major portion of valvular heart disease [3].
Mitral valve anatomically and physiologically can be best described as complex of several structures functioning in synchronization rather than a distinct entity. Moreover its fibrous continuity with aortic valve (aortic-mitral curtain), peculiar oblique location, vicinity to vital conduction bundle and central fibrous body spatially grant the mitral valve both strategic and vulnerable position [4]. An apt tensor apparatus of valve with adjacent ventricular musculature is a essential requirement for optimum functioning of mitral valve. Therefore any morphological insult either in mitral annulus, leaflet, chordae or in papillary musculature may cause varying degree of stenosis to regurgitation. The resultant change in fluid dynamics across regurgitating / stenotic valve may further accelerate the calcium and fibrin deposition which in turn leads to irreversible deformity [5].
On account of above, mitral valve surgeries is always a challenge as to what should be the optimum size of the prosthesis which may be ‘best-fit’ for rather D-shaped annulus without /
minimally affecting its morphological and
functional integrity. Predominantly
Echocardiography does capture the sectional anatomy and dimensions of the mitral valve by short axis and long axis parasternal, apical views. This facilitates to accommodate circular prosthetic valve into a rather wobbly ellipsoid area up to an extent only. Moreover from the arithmetical measurement perspective; annulus itself is very imprecise and perplexing because of indefinite hinge line at aortic-mitral curtain, variation in completeness of annulus and sub-valvular deformity itself contributes to anatomical alteration from normalcy [6]. These all factors in unison offer a very little ‘objectivity’ to decide the optimum size of prosthetic valve pre-operatively with the aid of Echocardiography; consequently so far a cardiac surgeon depends on their experiential clinical acumen to guess the size pre-operatively.
With this context and problem statement; this study attempts to construct a ‘best fit’ regression model to predict the diameter of the circular prosthetic valve based on the short axis, long axis and area of valvular annulus. This exploration may provide some initial objective evidences to determine the prosthetic valve size pre-operatively and thus will aid to efficiency and effectiveness of mitral valve surgery.
2. MATERIALS AND METHODS
(RHD) patients with severe mitral valve disease i.e. valvular area <1 cm2 (severe Mitral Stenosis), regurgitant valve with jet reaching up to pulmonary vein(severe Mitral Regurgitation), combined stenotic and regurgitant lesion. The patients who presented with simultaneous significant aortic valve disease and/or coronary artery disease with mitral valve involvement were excluded from the study because of the potential of these two ailments to alter valve geometry independently. t. Written Informed consent was obtained from each participant before enrolment.
Assuming the anticipated effect size 0.15 (small effect size, more conservative), type –I error rate at 0.05 and desired statistical power level at 0.80, minimal sample size calculated was 54.
The 2-dimensional transthoracic
echocardiography was performed on all these patients preoperatively to determine mitral valve annular dimensions by traditional method. Anterio-posterior (short axis) of mitral valve annulus was obtained by parasternal long axis view. The posterior annulus was located at the junction of leaflet and the left atrium, and the anterior annulus was located at the junction of left atrium and the aortic root. Long axis measurement (commissure-commissural) of mitral annulus was obtained from the apical four chamber view at the junction of leaflet and the left atrium. All measurement were done at peak systole, determined by visual perception of Echo-cardiologist.
Transthoracic echocardiography was performed with ASPEN ACUSONmain echocardiography machine incl 33503 with multi frequency probe of 3-5 MHz.
Before performing the actual linear regression analysis, data was checked for the appropriateness to use linear regression. Linear
relationship between dependant and
independent variable was ascertained through calculating co-relation co-efficient and by transformation of data. Case wise diagnostic was used to detect outliers and Durbin Johnson statistic to ascertain independence of observation. Normal distribution of residuals and homoscedasticity of the data duly checked by plotting histograms for residuals and scatter diagram.
After ascertaining the aptness of data three linear regression model were constructed by presupposing diameter of the circular prosthetic valve as dependent variable in reference with
the short axis, long axis and area of the ellipse of the mitral valve annulus (determined by Echo) as independent variables respectively with the help of SPSS version-16.
3. RESULTS
There were 25 males and 43 females in the study. The average age of the participants was 30.12 (±11.26) years in the range of 49(11 years-60 years). The mean Body Surface Area (BSA) and Body Mass Index (BMI) of the participants respectively were 1.34 (±0.15) m2 and 17.72 (±3.68) kg/m2.
The end diastolic left Atrial dimensions were varying from 25 mm to 85 mm (average- 45.20±9.82 mm). 2-D ECHO measured end systolic left ventricular size from 25 mm-49 mm (average-36.54±5.10 mm) and end diastolic size as 35-65 mm (average- 48.12±6.10 mm). Ejection Fractions of the participants were in the
range of 20% (50%-70%). During
echocardiography, 14/67 patients were assumed to have LA clot (hyper echoic shadows) but on opening only 10 out of14 patients were actually had it. Incidentally, LA clots were detected in 2 patients with no hyper-echoic findings in Echocardiography.
This study searches for best-fit predictors (namely short axis, long axis and area of mitral valve) dimensions estimated through 2-D Echo to envisage the area of circle (prosthesis valve). Here the underlying geometrical assumption is that natural valve has an elliptical shape (long and short arm) while prosthetic valve is circular (diameter).
So the generalize linear regression equation used in this study is-
Diameter of circle (Prosthetic valve) =a+ b* (predictors).
Where a is the intercept on Y-axis and b* is the slope for the predictors. Symbol ‘a’ shows the hypothetical value of diameter of prosthetic valve at zero X-axis value of predctors. Another symbol ‘b’ depicts the change in dependent variable (diameter of prosthetic valve) as the function of unit change in predictors.
Table 1 shows that short axis of annulus explains the diameter of prosthetic valve more deterministically compared to other predictors i.e. more than 90% of observed value of the prosthetic valve can be explained by the model in which short axis of the annulus is used as predictor variable.
The next table (Table 2) The tabe-2 summarizes the analysis of variance measures which divides variability into into categories that fit out models and residuals that do not fit our models.
F-ratio in all three models support the alternative hypothesis (states that calculated R2 values are real and not because of chance elements). This indicates that all three models can predict the diameter of prosthetic valve as per their R2 value; maximum variability explained by short axis.
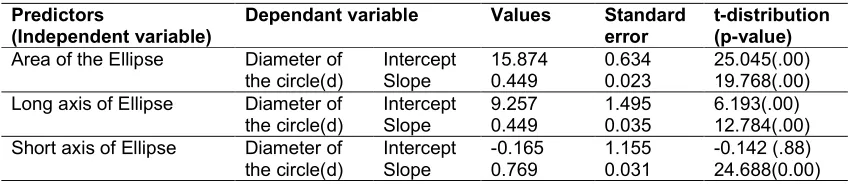
Table 3 shows the values of intercept and slope with standard errors in three linear regression model.
The inference drawn from Table 3 should be in the light of positive or negative sign assigned to the values. Interestingly the short axis intercept shows a negative point estimate (-0.165) and a relatively bigger positive standard error (1.155) than the point estimate. This indicates that the interval estimate for the intercept (point estimate± standard error) consists of zero value for intercept as well. Mathematically zero intercept shows a perfect linear relationship between two variables (the line for linear equation originates from X (0), Y (0) co-ordinates). This mathematical computation of perfect linear relationship also provides an indirect evidence for superiority of short axis as predictor compared to two other predictors.
The linear regression equation to predict the prosthetic valve diameter (dependant variable) using the short axis of ellipse (independent variable) is as under-
Diameter of prosthetic valve= -0.165+ 0.769X short axis of Ellipse.
Table 1. Correlation coefficient, coefficient of determination with error estimates for three regression models
Predictors
(Independent variable)
Dependent variable Co-relation coefficient(r)
Coefficient of determination(r2)
Standard error of estimate Area of the ellipse Diameter of the circle
(Prosthetic valve)
0.925 0.856 0.586
Long axis of ellipse Diameter of the circle (Prosthetic valve)
0.844 0.712 0.827
Short axis of ellipse Diameter of the circle (Prosthetic valve)
0.950 0.905 0.482
Table 2. Variance summary table showing explained variability in three models
Predictors
(Independent variable)
Sum of square (df)
Mean square value
F-distribution P- value Area of the
ellipse
Regression sum of square 134.214(1) 134.214 390.774 .00
Residual sum of square 22.668(66) 0.343 Long axis of
ellipse
Regression sum of square 111.753(1) 111.753(1) 163.437 .00 Residual sum of square 45.129(66) 0.684
Short axis of ellipse
Regression sum of square 141.554(1) 141.554 609.486 .00
Residual sum of square 15.329(66) 0.0232
Table 3. Intercept and slope values in three regression models
Predictors
(Independent variable)
Dependant variable Values Standard
error
t-distribution (p-value) Area of the Ellipse Diameter of
the circle(d)
Intercept 15.874 0.634 25.045(.00)
Slope 0.449 0.023 19.768(.00)
Long axis of Ellipse Diameter of the circle(d)
Intercept 9.257 1.495 6.193(.00)
Slope 0.449 0.035 12.784(.00)
Short axis of Ellipse Diameter of the circle(d)
Intercept -0.165 1.155 -0.142 (.88)
4. DISCUSSION
Normal mitral valve area depends on age, body surface area, height, left ventricle size, inter-papillary muscle distance [7]. The variability in the size of mitral valve depending primarily on the Body Surface Area(BSA) and other relevant factors y (MVA=4.83* BSA -0.07) hence offering a range of valve size in a premature infant to grown adult as per BSA [8].
Thromboembolism, endocarditis and
complication of anticoagulant therapy are some of the potential are some of dread complications of replacement surgeries [9]. Coupled with preoperative optimal prosthesis size determination is very important for replacement surgery. Oversize prosthesis produces aortic-mitral fibrous complex and left ventricular geometric distortion which leads to prosthesis malfunction. Under size prosthesis also may lead to significant residual gradient across prosthesis further culminating into high turbulence, haemolysis, and coagulopathy [10].
To address the issue, various studies were performed to determine mitral annular dimensions by indirect and direct methods. Indirect method consists of imaging modalities like echocardiography, multi slice cardiac computer tomography (CT), cardiac magnetic resonance imaging (cardiac MRI), and nuclear imaging techniques [11,12]. Direct methods include autopsy, cadaveric study and intraoperative direct measurements [13].
Ideal methods among the tools and techniques describe above is the one which is easy available, reproducible, harmless, non-ambiguous, inexpensive, and quick to perform and analyze. Although direct measurements produce the most accurate results, autopsy and cadaveric studies are not applicable to diseased populations [13]. Additionally, during the intra– operative procedure a heart rests in a cardioplegic state that itself may alter the geometrical dimension of it.
Imaging techniques like Multi slice cardiac CT, cardiac MRI, Nuclear Imaging techniques are more sophisticated and accurate tool of measurement compared to 2-D ECHO yet the incurred cost leads to limited availability of these modalities in some higher centres only. In a country with high prevalence of Rheumatic Heart Disease and limited resources, 2-D ECHO is still the chosen modality being a less costly one. This modality also offers the benefits like scope of
repetition without exposing to additional risk to patients.
ECHO technology has an element of subjectivity. A study conducted in United States compared the dimensions of mitral valve annulus measured from 2-D ECHO with multi slice cardiac CT method (as reference standard). The 2-D ECHO in the study could draw anatomical planes in 50% patients on adhering to corrected geometrical and anatomical principle compared to conventional view measurement. But the conventional view measurement correlated poorly with reference standard compared to corrected one. It can be inferred that there is always a trade-off between accuracy and probability of dropping-out while drawing a anatomical plane using 2-D ECHO [14]. In the current study conventional method of trans- thoracic 2 D Echo was used to evaluate short (A-P) axis and long (C-C) axis of all 67 recruited patients.
There is an spatial anatomical relationship among the aortic root, inter-valvular septum, left atrium and anterior mitral annulus in the physiologic setting. This fact sometimes make it difficult to appreciate the aortic root and the anterior mitral annulus separately through 2 D echocardiography. This mis-appropriation may lead to significant overestimation. Foster et al. [14] in his study observed this overestimation of short axis measurement upto 23.3% in traditional method of trans- thoracic 2 D echocardiography compared to cardiac CT. Duplessis et al. [15] and Walmsley et al. [16] also labelled in their study aortic root, left atrium and mitral annulus as separate but closely associated structures.
This inability to draw a correct anatomical plane and further overestimation of A-P axis through conventional 2-D ECHO; motivated the researcher to calculate some mathematical correction or conversion factors. In anexperimental study conducted by Suk Jung Choo et al. [17] suggested that the conversion factor of 0.80 could be reliably used to calculate value of intertrigonal distance in order to select the correct mitral annuloplasty ring size. This in vitro study used aortic roots of human and animal origin. They omitted all defective aortic roots from their analysis [17].
(I.T.D.) was measured independently via direct observations as well as andaortic annulus
diameter measurements by 2D trans
oesophageal echocardiography.
Echocardiographic I.T.D. was determined by dividing aortic annulus diameter by a factor of 0.80. Agreement between the 2 measurements were assessed statistically and difference between the two methods was detected as 2 mm [18]. Aortic valve was normal in this study as well. Because rheumatic heart disease commonly has aortic valve malformations through proteolysis, absence of an effective remodelling mechanism and calcification of the aortic leaflets, a better linear regression model is needed to more accurately determine mitral valve measurements preoperatively for these patientsThis fact is important in view with few reports which states the inability of even dobutamine stress echocardiography to deterministically ascertain the severity of ‘low-flow-low gradient ‘aortic valve stenosis [19]. Mitral valve dimension may be affected by other factors such as: left atrial size, rhythm abnormalities (atrial fibrillation, atrial flutter, etc.), co-morbid tricuspid valve abnormalities, age, and pulmonary arterial hypertension. All these factors may act in unison to predict the size of mitral valve. At this juncture this study does not compute multiple regression models to measure independently the effects of co-variables because of less numbers of subjects in each sub group. Because our study focused on adult populations, it may not be a sensitive predictor for other age groups. Additional research on various ages should be performed to augment our understanding of age related differences and better serve all populations with these deficits.
5. CONCLUSION
Measurement of mitral valve annulus has paramount importance to determine optimal mitral valve prosthesis size. This study attempts to compute equation to optimize valve measurement accuracy.
g. Results from the current study indicate that our regression model may greatly enhance current pre-operative measurement techniques and should be considered for patients of similar ages with valvular deficits. Additional studies are needed to maximize the benefits of this technology across age, gender and body size parameters.
CONSENT
Written informed consent was obtained from each patient before enrolment in the study.
All authors declare that ‘written informed consent was obtained from the patient (or other approved parties).
ETHICAL APPROVAL
Authors have obtained all necessary ethical approval from Institutional Ethical Committee of Gandhi Medical College. This study is not against the public interest, or that the release of information is allowed by legislation.
COMPETING INTERESTS
Authors have declared that no competing interests exist.
REFERENCES
1. Santulli G. Epidemiology of Cardiovascular Disease in the 21st Century: Updated numbers and updated facts. Journal of Cardiovascular Disease. 2013;1:1-2. 2. Maganti K, Rigolin VH, Sarano ME, Bonow
RO. Valvular Heart Disease: Diagnosis
and Management. Mayo Clinic
Proceedings. 2010;85(5):483-500. DOI:10.4065/mcp.2009.0706.
3. Kumar RK, Tandon R. Rheumatic fever & rheumatic heart disease: The last 50 years. Indian J Med Res. 2013;137(4):643-58.
4. Ho SY. Anatomy of the mitral valve Heart. 2002;88(Suppl IV):45–410.
5. McCarthy KP, Ring L, Rana BS. Anatomy of the mitral valve: understanding the mitral valve complex in mitral regurgitation. Eur J Echocardiogr. 2010;11(10):13-19.
6. Tomasz A. Timek G. Randall Green, Frederick A. Tibayan, David T. Lai, et al. Aorto-mitral annular dynamics Ann Thorac Surg. 2003;76(6):1944–50.
7. Sonne C, Sugeng L, Watanabe N, Weinert L, Saito K, Tsukiji M, et al. Age and body surface area dependency of mitral valve and papillary apparatus parameters: assessment by real-time three-dimensional echocardiography. Eur J Echocardiogr. 2009;10(2):287-94.
orifice area in infants and children by two-dimensional echocardiography. J Am Coll Cardiol. 1983;1(3):873-8.
9. Masuda M, Kado H, Tatewaki H, Shiokawa Y, Yasui H. Late results after mitral valve replacement with bileaflet mechanical prosthesis in children: evaluation of prosthesis-patient mismatch. Ann Thorac Surg. 2004;77(3):913-7.
10. Bolognesi M, Bolognesi D.
Echocardiographic Findings Before and After "edge to edge" Mitral Valve Repair for Myxomatous Prolapse and Severe Mitral Regurgitation. Journal of Cardiovascular Diseases. 2013;1(2):21-25.
11. Ormiston JA, Shah PM, Tei C, Wong M. Size and motion of the mitral valve annulus
in man. I. A two-dimensional
echocardiographic method and findings in normal subjects. Circulation. 1981;64:113-20.
12. Alkadhi H, Bettex D, Wildermuth S, Baumert B, Plass A, Grunenfelder J, et al. Dynamic cine imaging of the mitral valve with 16-MDCT: a feasibility study. AJR Am J Roentgenol. 2005;185:636-46.
13. Gupta C, Shetti VR, Manju BVM. Dimensions of the human adult mitral valve in the embalmed cadaver. J. Morphol. Sci. 2013;30(1):6-10.
14. Foster GP, Dunn AK, Abraham S, Ahmadi N, Sarraf G. Accurate measurement of
mitral annular dimensions by
echocardiography: Importance of correctly aligned imaging planes and anatomic landmarks. J Am Soc Echocardiogr. 2009;22(5):458-63.
15. DuPlessis LA, Marchand P. The anatomy of the mitral valve and its associated structures. Thorax. 1964;19:221-7.
16. Walmsley R. Anatomy of human mitral valve in adult cadaver and comparative anatomy of the valve. Br Heart J. 1978; 40:351-66.
17. Choo SJ, Olomon J, Bowles C, Luo HH, Pang D, Oury J Hetal. An In vitro study of the correlation between aortic valve diameter and mitral intertrigonal distance: A simple method to select the correct mitral annuloplasty ring size. J Heart Valve Dis. 1998;7(5):593-7.
18. Cooray SD, Tutungi E, Mezzatesta JP,
Moshinsky R, Almeida AA.
Echocardiographic measurement of mitral intertrigonal distance is an adjunct to annuloplasty ring sizing. J Heart Valve Dis. 2009;18(1):106-10.
19. Mistiaen WP, Van Cauwelaert P, Muylaert P. Pitfalls in the Estimation of the Severity of a “Low-Flow Low-Gradient” Aortic Valve Stenosis in absence of Contractile Reserve. JCvD. 2014;2(4):213-217.
© 2015 Sharma et al.; This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Peer-review history:
The peer review history for this paper can be accessed here: