[
CLINICAL COMMENTARY
]
T
he role of muscles in joint protection and stabilization has been
of increasing interest to researchers and clinicians involved in
spinal pain and rehabilitation. Evidence for the importance of
deep posterior muscles of the spine in the management of people
with low back pain (LBP) has been provided by biomechanical
7,60,80,82and neurophysiological
46,48investigations. Imaging studies have further
allowed definition of both normal morphology and impairments
in paraspinal muscles.22,27,32,33 Rehabili-tative ultrasound imaging (RUSI) is a potentially useful tool in physical thera-py for the assessment and treatment of these muscles. The advantages of RUSI over other imaging techniques have been discussed in a recently published related
cles can be incorporated into neuromus-culoskeletal rehabilitation. The main applications of RUSI for measurement of morphological characteristics (mor-phometry) and visualization of muscle contraction for biofeedback are dis-cussed. The lumbar multifidus is the most widely studied paraspinal muscle, in both healthy populations68 and people with spinal pain and injury.22,26,27 Stud-ies of different cervical muscles are also emerging.37,39,61-63 In the thoracic region, the lower trapezius is the first muscle to be measured with ultrasound imaging.53 Quantitative evaluation of the posterior paraspinal musculature using static and dynamic imaging has been used to study muscle morphology and behavior dur-ing contraction.34,39,64,74,76 In this context, behavior relates to level of contraction (change in thickness), changes in size over time and with respect to other muscles, as well as observation of con-traction as a biofeedback tool for the pa-tient or therapist. In this commentary we review what is known about RUSI as applied to the paraspinal musculature, propose guidelines for standardizing the imaging and measurement tech-niques in clinical and research applica-tions, and propose future directions for research.
T SYNOPSIS: Interest in rehabilitative ultra-sound imaging (RUSI) of the posterior paraspinal muscles is growing, along with the body of literature to support integration of this technique into routine physical therapy practice. This clinical commentary reviews how RUSI can be used as an evaluative and treatment tool and proposes guidelines for its use for the posterior muscles of the lumbar and cervical regions. Both quantita-tive and qualitaquantita-tive applications are described, as well as measurement reliability and validity. Measurement of morphological characteristics of the muscles (morphometry) in healthy populations and people with spinal pathology are described. Preliminary normal reference data exist for mea-surements of cross-sectional area (CSA), linear
dimensions (muscle depth/thickness and width), and shape ratios. Compared to individuals without low back pain, changes in muscles’ size at rest and during the contracted state have been observed using RUSI in people with spinal pathology. Visual observation of the image during contraction indicates that RUSI may be a valuable biofeed-back tool. Further investigation of many of these observations is required using controlled studies to provide conclusive evidence that RUSI enhances clinical practice. J Orthop Sports Phys Ther 2007;37(10):581-595. doi:10.2519/jospt.2007.2599
T KEY WORDS:cervical muscles, lumbar muscles, lumbar spine, neck, morphometry, sonography
1Professor of Neuromuscular Rehabilitation, Director of Research, School of Health Professions and Rehabilitation Sciences, University of Southampton, UK; Visiting Professor,
Department of Physiotherapy, Trinity College, Dublin, Ireland.2Senior Lecturer, Division of Physiotherapy, School of Health and Rehabilitation Sciences, University of Queensland,
Brisbane, Australia; Clinical Director, UQ/Mater Back Stability Clinic, Mater Health Services, Brisbane, Australia.3Assistant Professor, Department of Physical Therapy, Regis
University, Denver, CO; Doctoral Candidate, Division of Physiotherapy, School of Health and Rehabilitation Sciences, University of Queensland, Brisbane, Australia.4Assistant
Professor, Department of Physical Therapy, University of Evansville, Evansville, IN; Assistant Professor, University of Kentucky, Lexington, KY.5Professor and NHMRC Principal
Research Fellow, Director, Division of Physiotherapy, School of Health and Rehabilitation Sciences, University of Queensland, Brisbane, Australia. Address correspondence to Dr Maria Stokes, Professor of Neuromuscular Rehabilitation and Director of Research, School of Health Professions and Rehabilitation Sciences, University of Southampton, Highfield Campus, Southampton, Hants SO17, 1BJ, UK. E-mail: [email protected]
manuscript.79
The primary purpose of this clinical commentary is to review the current scientific literature on RUSI related to the posterior paraspinal muscles and to increase the understanding of how RUSI of the posterior paraspinal
mus-Rehabilitative Ultrasound Imaging
of the Posterior Paraspinal Muscles
MARIA STOKES,PhD, MCSP1 • JULIE HIDES,PhD, MPhtySt, BPhty2
[
CLINICAL COMMENTARY
]
ANATOMY OF THE
PARASPINAL MUSCULATURE
I
nterpretation of RUSI isdepend-ent on an understanding of the ana-tomical features and function of the musculoskeletal structures of the spine. This section presents an overview of the anatomical and biomechanical properties of the paraspinal musculature, focusing on the lumbar and cervical muscles in relation to RUSI. The reader is referred to the following manuscripts for further more specific details of anatomy and function.2-4,6,8,52,55,60
Posterior Lumbar Spine Musculature
The lumbar paraspinal muscles, lying behind the transverse processes, have been divided into 3 groups by Bogduk.3 The first and deepest group includes the deep intersegmental muscles, interspi-nales, and intertransversarii mediales. These muscles are short and too small to provide sufficient clarity of their borders for adequate visualization by ultrasound imaging (USI). The second group com-prises the polysegmental muscles, which attach directly to the lumbar vertebraeand include the multifidus and lumbar portions of the erector spinae (ES), lon-gissimus, and iliocostalis muscles (TABLE 1). The third and most superficial group of muscles consists of long, polysegmen-tal muscles, which traverse the lumbar region from the thoracic levels. These muscles attach to the ilium and sacrum, and include the thoracic portions of the
ES muscles.
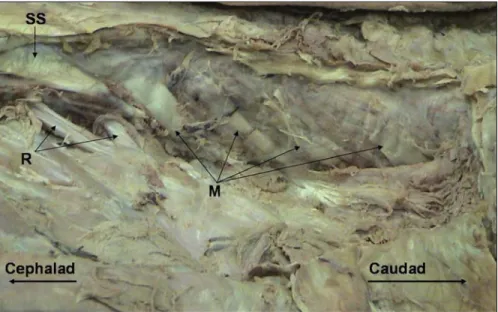
Lumbar Multifidus This is the most me-dial of the lumbar muscles and Macin-tosh et al44 have described it as a large, multifascicular muscle composed of 5 overlapping layers, with its size increas-ing in a caudal direction (FIGURE 1, TABLE 1). The morphometry of the lumbar mul-tifidus muscle can be assessed with RUSI
TABLE 1
Anatomy of Selected Lumbar and Cervical Posterior Paraspinal Muscles
Muscle Origin Insertion
Lumbar multifidus44 • Laminae and spinous processes of each lumbar vertebra • Descend in a caudal direction to cross 3 to 5
vertebrae
• Deep laminar fibers: inferior edge of a lamina • Mamillary bodies and zygapophyseal joint capsule of the vertebra 2 levels caudal
• Superficial fibers: along the spinous process • Cross up to 5 levels: attach to the mamillary processes of the caudal vertebra, sacrum, and posterior superior iliac spine
Erector spinae43
Longissimus • Lumbar transverse and accessory processes • Ventral surface of posterior superior iliac spine Iliocostalis • Tips of lumbar transverse processes and adjacent middle layer of • Ventral edge of iliac crest
the thoracolumbar fascia
Cervical multifidus2 • Laminae and spinous processes of cervical vertebrae • Capsules of cervical facet joints81
Semispinalis cervicis2 • Transverse processes of the upper 5 or 6 thoracic vertebrae • Cervical spinous processes of C2 to C5
Splenius capitis2 • Spinous processes of C7 and T3 or T4 • Just deep to sternocleidomastoid into the mastoid
process and occipital bone just below lateral third of superior nuchal line
Semispinalis capitis2 • Tips of transverse processes of T6 and T7, and C1-C3 articular processes • Mastoid process
FIGURE 1.Cadaver dissection of lumbar multifidus (M), rotatores (R), and the semispinalis (SS) musculature, showing fascicles passing down in a caudal direction over the lumbar spine.
using either a transverse or parasagittal image. On the transverse section, lumbar multifidus can be identified as a single region of muscle and separate fascicles are not often visible (FIGURES 2 and 3). The advantage of imaging using a trans-verse section is that the cross-sectional area (CSA) of the muscle can be mea-sured.21,68 Conversely, in a parasagittal (longitudinal) image, muscle fascicles can be identified from the connective tissue between muscle fibers (FIGURE 4).
Parasagittal views are easier to interpret than transverse views, both for measur-ing muscle thickness34 and for providing biofeedback of changes in the muscle during contraction.24,74
Researchers using biomechanical models based on anatomical data have suggested that the superficial fibers of lumbar multifidus create a posterior sagittal rotation (extension) of the lum-bar spine, in addition to intervertebral compression,43,4 while the deeper fibers primarily generate compressive forces, with minimal associated torque.4,47 It has been proposed that the intersegmental nature of the deep lumbar multifidus provides an advantage to the
neuromus-cular system for controlling the stability of the motion segment.55 For this rea-son, clinicians aim to include voluntary contraction of the deep fibers in their exercise (or rehabilitative) programs.24 Electromyographic (EMG) studies of arm movement suggest differential ac-tivation of the deep (earlier onset) and superficial fibers.51 This finding suggests that different exercises may be neces-sary for selectively re-educating the deep versus the superficial fibers, but this re-quires investigation.
There is consistent evidence that the lumbar multifidus muscle controls spi-nal motion, contributing to interverte-bral stiffness.31,55,80 Lumbar multifidus RUSI studies have identified reduced CSA in people with acute LBP,26,27 and EMG evidence suggests that changes in motor control may be more localized to the deep fibers.42 However, it is impor-tant to consider that all lumbar mus-cles contribute to stability of the lumbar spine.7,8,12,18,47,48,80
Lumbar ES The lumbar ES lie lateral to multifidus and consist of longissimus thoracis pars lumborum and iliocostalis lumborum pars lumborum (TABLE 1).43 In the upper lumbar region, research-ers have demonstrated that the longis-simus muscle overlaps the fibers of the multifidus muscle.43 Various studies have shown that the ES muscles contribute to lateral flexion, extension, and rotation of the lumbar spine, as well as stabil-ity.7,8,12,18,47,48,80 Regarding imaging, the ES muscles are too large to allow CSA measurements using RUSI. However, Watanabe et al78 have measured thick-ness successfully in the sagittal plane by placing the transducer longitudinally. Their technique illustrates the use of the echogenic (reflective, white) transverse processes and subcutaneous tissue-mus-cle border as landmarks to assess thick-ness of the ES muscles.
Posterior Cervical Spine Musculature
The posterior musculature of the cervi-cal spine is commonly divided into 4 lay-ers (FIGURE 5). The most superficial layer FIGURE 2.Schematic diagram of a cross section at the level of the fourth lumbar vertebra (L4). The lumbarmultifidus muscle (M) lies lateral to the spinous process, superior to the lamina (L), and medial to erector spinae (ES). Abbreviations: AT, adipose tissue; IL, iliocostal ligament; S, skin; SP, spinous process; TP, transverse process; VB, vertebral body.
FIGURE 4.Parasagittal ultrasound image of the lumbar multifidus muscle, taken lateral to the spinous process using a 5-MHz curvilinear transducer. The facet joints (F) can be used as landmarks for the lower border of the muscle.
FIGURE 3.Bilateral transverse ultrasound image at L4, using a 5-MHz curvilinear transducer, showing the spinous process (SP) in the center of the image and the echogenic laminae (L) appearing as bright white horizontal landmarks, either side of the base of the SP and beneath the lumbar multifidus (M) muscle. The lateral borders are not clear enough to enable measurement of area and require the transducer to be angled more appropriately for each side separately.
[
CLINICAL COMMENTARY
]
consists of the upper trapezius muscles, the second layer consists of the splenius capitis muscle,62 the third layer consists of the semispinalis capitis63 and semispi-nalis cervicis muscles,71 while the deepest layer contains the multifidus and rotatores muscles. Some studies place semispinalis cervicis in this deepest layer,61 while others also include the suboccipital muscles of rectus capitis posterior minor (RCPmin) and major (RCPmaj).71 We have limited the description of anatomical features of cervical muscles to those described by re-searchers using RUSI.37,39,61-63
Cervical Multifidus and Semispinalis Cer-vicis Winkelstein et al81 have suggested that the ability of the multifidus muscle to control cervical segmental motion could be compromised by its insertion directly into the capsules of the facet joints (TABLE 1), which have been widely implicated in neck pain and injury.41,56,65,82 Degenerative changes in the deep cervical paraspinal musculature have been found in studies using RUSI and magnetic resonance im-aging (MRI) in patients with persistent neck pain following trauma.15,19,37,73 The semispinalis cervicis muscle (along with the capitii musculature) is considered a primary cervical spine extensor.52 Splenius Capitis and Semispinalis Capi-tis These muscles have been described as broad and flat, extending upward and lateral to their attachment on the mastoid process (TABLE 1).62,63 The main function of these muscles is neck extension,46,71 and they are more active during large, fast movements of the neck11 than during sustained postural activity.
QUANTITATIVE EVALUATION
T
he procedures described arebased on developmental studies by Hides et al,21,26,27 Kiesel et al,34 and a relatively large population study by Stokes et al,68 and reflect the suggestions of the team of authors of this commen-tary. Both static and dynamic techniques for quantitative evaluation of muscles are described.
Imaging Procedure for Lumbar Multifidus
Images of lumbar multifidus have either been obtained from transverse (FIGURE 3)21,22,26,27,68 or parasagittal (FIGURE 4)34 orientations.Positioning As originally suggested by Hides et al,21 the subject is usually relaxed in a prone lying position. But this is not always possible, as Coldron et al10 realized when attempting to scan lumbar mul-tifidus in women who had recently given birth. Researchers have shown that the side-lying position can be used to obtain images without affecting muscle size at rest.10 But this is not the case when im-aging with the subject in a standing pos-ture.40 Lee et al40 found that in healthy control subjects, lumbar multifidus CSA increased from prone lying to upright standing, then gradually decreased dur-ing forward flexion. In patients with LBP, CSA also increased from prone to upright standing, but forward flexion produced a further increase in CSA, suggesting al-tered function of lumbar multifidus.40 As suggested by Hides et al,21 we recom-mend that, in prone lying, 1 to 2 pillows
be placed under the hips to minimize the lumbar lordosis, so that the muscles lie as horizontally as possible along the spine. Inclinometers were used by Hides et al25 and Kiesel et al34 to ensure the lumbar spine was within 10° of horizontal.
Positioning of the operator relative to the subject is important for standardiza-tion of the technique to achieve correct image interpretation. So, with the subject prone, we recommend that the scanner and operator be situated to the left of the prone subject (the opposite to imaging anterior structures in the supine subject), in keeping with standardized protocols in radiology.9,79
The lumbar spinous processes are pal-pated and their position located on the skin with an indelible marker, such as an eye liner pencil, which is water insol-uble but easily removed with an alcohol swab.54 In most individuals, the spinous process of L5 is a deep, small, blunted bony point lying at the center of the lum-bosacral depression and can be found by palpating cranially from the sacrum.5 On progression in a cranial direction is the comparatively large spinous process of L4. The remaining lumbar spinous pro-cesses are then identified by continuing palpation cranially. These locations can be verified with USI by including the sacral base in the image and counting the spinous processes cranially.
Transducers Various transducers have been used for imaging the lumbar mul-tifidus muscle, but we suggest the use of a curved transducer with a frequency of 5 MHz,which is used for transverse im-aging in the majority of studies (TABLE 2). This is because more of the sound waves emitted by a curved transducer are likely to be perpendicular to the rounded bor-der of multifidus than those from a linear transducer. For parasagittal imaging, we consider transducer shape less impor-tant, so curvilinear34 or linear25 arrays can be used. Regarding transducer frequency, the depth of lumbar multifidus is more suited to 5 MHz21,68 for image clarity than lower or higher frequencies, such as 3 MHz or 7 to 10 MHz, respectively.79 The FIGURE 5.Magnetic resonance images: (A) sagittal cross section of the C6 vertebral level; (B) the corresponding
axial scan at the C6 level showing the cervical multifidus (M), semispinalis cervicis (SEC), semispinalis capitis (SCP), splenius capitis (SC), and trapezius (T) muscles.
size of the transducer varies with differ-ent ultrasound machines (TABLE 2), but we suggest using as large a footprint (length of array surface) as possible, with a mini-mum of 5 cm, to ensure sufficient contact with the skin to enable a wide field of view on the scan. For further details on select-ing transducers, see a related publica-tion by Whittaker et al,79 which discusses the relationships between muscle shape, depth, and transducer specifications. Imaging Technique We endorse the technique used by a number of research-ers,21,25,27,68 in which the transducer was first placed longitudinally and centrally over the lower lumbar spine to orient and confirm the marks on the skin. The
indicator mark on the side of the trans-ducer (either a line or light) was directed cranially, producing a scan showing the spinous processes, as seen inFIGURE 6. For parasagittal imaging, researchers have described moving the transducer later-ally to image lumbar multifidus,34,74 using the facet joints inferiorly as a landmark (FIGURE 4). For transverse imaging, the transducer was rotated from the central
longitudinal orientation through 90°, to lie transversely in the midline with its in-dicator mark towards the operator,21,68 so that the right side of the anatomy would appear on the right side of the screen. This produced an image in which the spi-nous process and laminae could be seen, with lumbar multifidus muscles visible on both sides of the spine (FIGURE 3). If the muscles were too large for bilateral imaging, they were scanned individually by moving the transducer laterally, to the left and right (FIGURES 7 and8). As in these previously cited studies, we recommend that the echogenic (bright) vertebral laminae be used as landmarks to identify the muscle’s deep border, which is impor-tant when measuring CSA, as there is a large difference in CSA over the span of 1 vertebral level if a consistent landmark is not used.
The lateral border of the lumbar mul-tifidus muscle is often difficult to dis-tinguish from the lumbar longissimus muscle, and strategies to produce muscle contraction can help to identify the bor-der during real-time imaging (TABLE 3). However, if a test movement is used, it is important that the subject relaxes before measurements are taken. Off-line mea-surements on stored images do not have the advantage of dynamic (real-time) im-aging for locating muscle borders and it may me more of a matter of extrapolating between identifiable areas of a border.
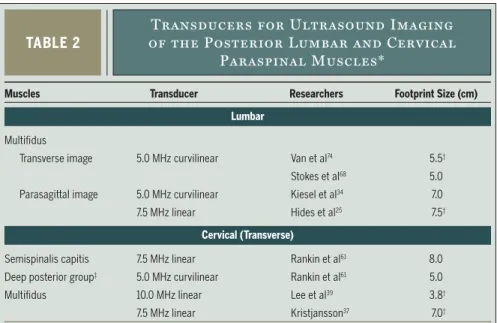
TABLE 2
Transducers for Ultrasound Imaging
of the Posterior Lumbar and Cervical
Paraspinal Muscles*
Muscles Transducer Researchers Footprint Size (cm)
Lumbar
Multifidus
Transverse image 5.0 MHz curvilinear Van et al74 5.5†
Stokes et al68 5.0
Parasagittal image 5.0 MHz curvilinear Kiesel et al34 7.0
7.5 MHz linear Hides et al25 7.5†
Cervical (Transverse)
Semispinalis capitis 7.5 MHz linear Rankin et al61 8.0
Deep posterior group‡ 5.0 MHz curvilinear Rankin et al61 5.0
Multifidus 10.0 MHz linear Lee et al39 3.8†
7.5 MHz linear Kristjansson37 7.0†
*Transducers with a large footprint (>5 cm) are preferable for sufficient contact with the skin to enable
a wide field of view. Transducer size and frequency depend on availability with a particular scanner. The preferable transducer for transverse imaging of lumbar multifidus is 5 MHz curvilinear.
†Not reported in paper cited (detail gained from authors).
‡The deep posterior cervical group comprises the semispinalis cervicis, multifidus, and rotatores.
FIGURE 6.Ultrasound image showing a sagittal view of the lumbar spine. The 5-MHz linear transducer was placed centrally over the spinous processes (SP).
FIGURE 8.Transverse ultrasound image of the right lumbar multifidus muscle at L5, using a 5-MHz curvilinear transducer. The spinous process (SP) is shorter and the lateral edge less steep than at L4 (Figure 7). (Reproduced from Stokes et al,68 with
permission).
FIGURE 7.Transverse ultrasound image of a left lumbar multifidus (M) muscle at L4, using a 5-MHz curvilinear transducer. The oval shape of the muscle is evident and is bordered inferiorly by the lamina (L), medially by the spinous process (SP), and laterally by longissimus (Lo).
[
CLINICAL COMMENTARY
]
Static Measurement of Lumbar Multifidus
The CSA (cm2) of multifidus is measured by tracing around the muscle border with the on-screen cursor or off-line us-ing an image-processus-ing package such as ImageJ (http://rsb.info.nih.gov/ij/docs/ index.html). For consistency, the precise part of the border needs to be traced each time and the inner edge of the border is often used.68 Two linear dimensions are often measured, defined as the great-est depth (anteroposterior [AP]) and the greatest width (lateral dimension [Lat]), lying perpendicular to the AP dimension.21 Hides et al21 described the shape of the lumbar multifidus muscle as a ratio of the linear measurements, with the AP divided by the lateral dimension (AP/Lat). Stokes et al68 made anthropo-metric measurements on ultrasound im-ages to examine their relationships with CSA, including the length (cm) of the spinous process (SPL) and the horizontal distance (cm) between the lateral edge of each lamina (bilateral lamina width). Researchers have also used whole-body measurements and characteristics to as-sess their predictive value for estimat-ing lumbar multifidus size, includestimat-ing height, age, body mass, and body mass index (BMI).21,27,68 Relationships alluded to here, particularly between muscle di-mensions, will be discussed later in the commentary.Dynamic
Measurement
of
Lumbar
Multifidus
Real-time RUSI can be used to assess muscle during active movements. Dy-namic measures are described for the posterior cervical39 and the lumbar mul-tifidus,34,74,75as well as muscular fatigue.64 The most common RUSI measurement of the paraspinal muscles to represent muscle contraction is change in muscle thickness. Watanabe et al78 measured thickness change of the lumbar ES mus-cles in the sagittal plane. Significant differences were found in measures ob-tained in neutral, flexed, and extended static postures. Kiesel et al34 used graded resistance of contralateral upper extrem-ity lifts, performed in prone, to produce incremental activation of lumbar mul-tifidus and demonstrated a positive re-lationship between increases in muscle thickness and fine-wire EMG signals (see validity section below). Vasseljen et al75 used high-speed motion mode (M-mode) ultrasound, compared with fine-wire EMG, to identify movement of the deep fibers of the lumbar multifidus muscle during rapid arm lifting. Lee et al39 found significant increases in thickness of cervi-cal multifidus during contractions, which were similar at 3 levels from C4 to C6.
It is clear that RUSI can be used to measure thickness of the posterior trunk musculature.34 Preliminary studies of
as-ymptomatic subjects comparing RUSI to the gold standard of intramuscular EMG are encouraging and suggest that RUSI may be used to measure both magni-tude34,39 and timing75 of activation in the paraspinal muscles.
Morphometry of the Lumbar Multifidus
The lumbar multifidus muscle, in the ab-sence of pathology, has been described as generally round or oval in shape, and its size varies among the vertebral levels.25 Studies with similar methodology and subject groups provide consistent data, as summarized inTABLE 4.Cross-sectional Area At the level of the fourth lumbar vertebra (L4), the mean CSA of multifidus has been reported to be approximately 8 cm2 in males and ap-proximately 6 cm2 in females (TABLE 4). The muscle becomes larger at L5 (ap-proximately 9 cm2 in males and approxi-mately 7 cm2 in females). The CSAs at L4 and L5 are highly correlated (r = 0.82 for males, 0.80 for females), so one could be reasonably well estimated from the other using predictive equations.68 A multilevel analysis of the entire lumbar spine indi-cated that multifidus CSA increases from L2 to L5 and then decreases at S1.25 Mean data from a group of 10 young females were approximately 2.0 cm2 at L2, 3.3 cm2 at L3, 4.9 cm2 at L4, 7.1 cm2 at L5, and 6.4 cm2 at S1.
Linear Dimensions The thickness or AP dimension of lumbar multifidus is approximately 2.6 cm and the lateral dimension is approximately 2.8 cm in healthy males (TABLE 4). In females, the mean values are approximately 2.2 cm for the AP dimension and 3.0 cm for the lateral dimension.
Muscle Shape The linear dimensions in-dicate that the muscle is almost round in males but more oval in a horizontal di-rection in females (ie, flatter).21,68 A study of 120 healthy subjects reported round, oval, and triangular lumbar multifidus muscle shapes.68 Gender, age, vertebral level, and physical activity accounted for these different shapes.
The shape of the lumbar multifidus
TABLE 3
Strategies for Identifying the Lateral
Border of Lumbar Multifidus During
Transverse Imaging
Maneuver by the Subject
• Raise (extend) the ipsilateral lower limb slightly24
• Shorten ipsilateral limb gently • Raise the contralateral upper limb34
• Imagine the muscles are sausages on either side of the spine and try to shorten and fatten the sausages • Note: ensure that movements are minimal to maintain the test position and avoid movement of the transducer
from the scanning site
Observe on Transverse Image
• Movement of multifidus and adjacent erector spinae muscle (longissimus) in relation to each other. Fascicles of multifidus move in a swirling motion, sliding round against each other, which differs from the movements of longissimus
muscle is not always regular, particularly in subjects with relatively large muscles, where it can appear more triangular68 (FIGURE 9). The medial and inferior (deep) borders of the multifidus are confined by the spinous process and lamina, so the multifidus can only hypertrophy in a lat-eral or superior (superficial) direction, which may explain the more triangular shape of hypertrophied muscles.68 In such cases, the shape ratio is mislead-ing as it would tend to suggest a round shape. Stokes et al68 suggested that it may be more appropriate to describe a trian-gular-shaped muscle using 3 measure-ments (the superior, medial, and lateral borders), but this requires investigation. The clinical relevance of lumbar multifi-dus shape and whether or not it reflects muscle tone have yet to be explored.
Prediction of CSA From Linear Mea-surements Researchers have shown that
linear measurements can reflect CSA ac-curately.21,27,68 Linear measurements can be made more quickly and easily than tracing the muscle border to measure area (an option not available on all ultra-sound apparatus). Linear measurements are therefore more applicable for clinical use than CSA, provided they predict CSA accurately. The combined linear measure-ments (AP Lat) were highly correlated with CSA at L4 and L5 (range in males,
r = 0.95 to 0.98; range in females,r = 0.93 to 0.95) in 3 studies (TABLE 4).21,27,68 However, it is known that this correla-tion for resting muscle weakens when muscle becomes atrophied (r = 0.75 and 0.85 in males and females, respectively27) and cannot be assumed in all situations. Thus the clinical utility of the prediction of CSA from resting linear measures may
TABLE 4
Lumbar Multifidus Morphometry From Images
in Prone Lying in Healthy Populations
Abbreviations: AP, anteroposterior; CSA, cross-sectional area; L, left; NR, not reported; R, right.
* Mean 1 SD, range.
CSA Versus Linear AP Dimension Lateral Dimensions Population Age (y)* Researchers CSA (cm2)* Shape Ratio* Thickness (cm)* Dimension (cm)* Multiplied (r)
Fourth Lumbar Vertebra
Males n = 21 18-35 Hides et al21 6.150.93 (4.35-8.5) 0.910.12 (0.68-1.19) 2.550.3 (2.03-3.35) 2.820.23 (2.50-3.31) 0.98 n = 52 4013 (20-69) Stokes et al68 7.781.85 (4.24-11.5 [95%]) 1.020.15 (0.72-1.33) NR NR 0.96 n = 19 41.7 (35-47) Lee et al40 R, 7.681.29; L, 7.621.38 NR NR NR NR Females n = 27 18-35 Hides et al21 5.60.8 (4.18-7.23) 0.750.13 (0.42-0.98) 2.242.98 (1.63-2.75) 3.053.25 (2.35-3.96) 0.93 n = 10 25.5 (21-31) Hides et al27 4.871.22 NR NR NR NR n = 68 3413 (20-64) Stokes et al68 5.551.28 (3.03-8.06 [95%]) 1.050.21 (0.64-1.47) NR NR 0.95
Fifth Lumbar Vertebra
Males n = 45 3913 (20-69) Stokes et al68 8.911.68 (5.62-12.30 [95%]) 1.030.17 (0.70-1.36) NR NR 0.95 n = 19 41.7 (35-47) Lee et al40 R, 7.252.11; L, 7.141.55 NR NR NR NR Females n = 10 25.5 (21-31) Hides et al27 7.120.68 NR NR NR NR n = 46 3212 (20-64) Stokes et al68 6.651.0 (4.69-8.60 [95%]) 0.950.17 (0.62-1.28) NR NR 0.94 L4/5
Males and 285.6 Kiesel et al34 NR NR 2.480.19 NR NR
females, n = 5
FIGURE 9.Transverse ultrasound image of a triangular shaped left lumbar multifidus muscle at L4, taken using a 5-MHz curvilinear transducer. (Reproduced from Stokes et al,68with permission.)
[
CLINICAL COMMENTARY
]
be limited, as in most cases comparison of atrophied and nonatrophied muscles is the objective of the assessment. Dur-ing contraction, however, Kiesel et al33 found that the AP linear measurement of lumbar multifidus was consistently decreased by induced pain, indicating that this simple, time-efficient measure may be clinically useful for assessment of contraction capability. Correlations were found to be poor between muscle size and body anthropometry.68
Muscle thickness (AP dimension) was also highly correlated with CSA at L4 (males,r = 0.8; females,r = 0.7). Howev-er,at L5, although statistically significant (P.001), the relationship was not strong enough to be of clinical value (males,r = 0.66; females,r= 0.54), assuming that correlation coefficients above 0.70 are required to be clinically significant.36 We suggest that multiplication of the linear dimensions, although not representative of a round or oval shape, is preferable to a single measurement when area cannot be measured, based on evidence of its high correlation with lumbar multifidus CSA.21,27,68
Symmetry Mean between-side differ-ence in lumbar multifidus muscle size in healthy individuals without pain or pathology has been found to be below 10% (mean SD, 3 4%27; 9.6% 8% in males,68 8.1% 6% in females68). Marked asymmetry can occur with acute LBP27 and be a useful clinical indicator of abnormality.
Effect of Age Researchers have not found differences in lumbar multifidus muscle size among different age groups.68 How-ever, the quality of the muscle may be-come altered, as changes in water and fat content that occur with age produce changes in signal intensity on MRI scans.72 Infiltration with fatty or fibrous tissue increases the echogenicity of mus-cle, making it appear whiter than usual, as observed in some of the older subjects (up to age 69 years) studied by Stokes et al.68 But a reliable method for quantifica-tion of these changes in ultrasound im-ages has yet to be developed.
Imaging Procedure for the Posterior
Cervical Muscles
There are limited published data on RUSI of the cervical muscles. Those studied include splenius capitis,62 semispinalis capitis,61,63 multifidus,37,39 and the deep posterior cervical muscle group compris-ing semispinalis cervicis, multifidus, and rotators.61
Positioning Imaging of the cervical mus-cles has been described with the subject sitting39,63 or prone lying,37,61,62,63 with the neck in a neutral position. Rezasoltani et al63 used an inclinometer to help ensure that the thoracic and cervical postures were horizontal during the ultrasound measurements. Locating the vertebral levels to be imaged has been achieved by palpation of the cervical spinous process-es between C2 (the first bony landmark caudal to the occiput) and C7 (the most prominent spinous process), as detailed by Lee et al.39
Transducers Examples of transducers used for the different muscles are listed inTABLE 2. For example, a 7.5-MHz lin-ear transducer was used for imaging semispinalis capitis61,63 and splenius ca-pitis,62 which are relatively superficial flat muscles, while a 5-MHz curvilinear transducer was used for the deep muscle group, which has a more oval shape.61 Conversely, for imaging cervical multifi-dus, a deep oval muscle, Lee et al39 used a 10-MHz linear transducer and Kristjans-son37 used a 7.5-MHz linear transducer, possibly determined by availability of transducers rather than suitability. Most researchers have held the transducer in place manually, but custom-made devices to hold the transducer have also been de-scribed.39 The devices can enable a more consistent technique than manual appli-cation but need to allow the transducer to be tilted or angled to sharpen the image if necessary. Devices obviously have cost implications.
Imaging Technique Procedures have been described for splenius capitis at C3,62 semispinalis capitis at C3,61,63 the deep muscles as a group at C3,61 and mul-tifidus at C437 and C4 to C6.39 In all cases,
the transducer was placed transversely in the midline over the spinous process at the level of interest and then moved lat-erally to image the left or right muscles. Identification of the echogenic (bright, reflective) laminae is then useful, which-ever muscles are imaged.
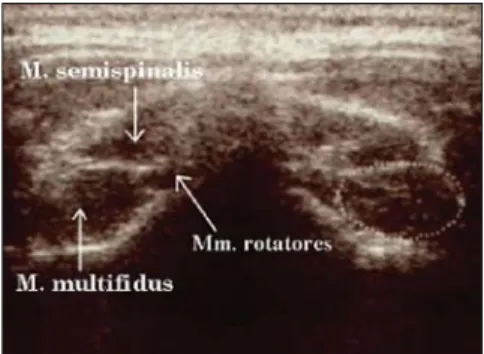
The splenius capitis lies deep to the trapezius and is a broad, flat muscle. The semispinalis capitis is easily recognized as a long, strap-like muscle divided into 2 sections by an aponeurotic intersection (FIGURE 10). The deep neck muscle group has a distinctive teardrop shape, but the fascia between the 3 constituent muscles (semispinalis cervicis, multifidus, and rotatores) are not always easy to distin-guish in symptomatic or asymptomatic subjects with RUSI (FIGURE 11). The cervi-cal multifidus muscle lies ventral to the semispinalis cervicis and the fascia be-tween them is more consistently defined using 7.5- to 10.0-MHz linear transduc-ers than a 5.0-MHz curvilinear trans-ducer (FIGURE 11).
Morphometry of the Posterior Cervical
Muscles
Researchers have reported data for CSA, linear dimensions, and shape ratios in healthy populations and some examples are shown inTABLE 5. The muscles of the neck are relatively small (mean CSA be-tween 1 and 3 cm2) compared with the lumbar muscles. Atrophy of the cervical multifidus muscle was demonstrated in women with chronic whiplash-associ-ated disorder (mean SD multifidus CSA at C4: right, 0.96 0.19 cm2; left,
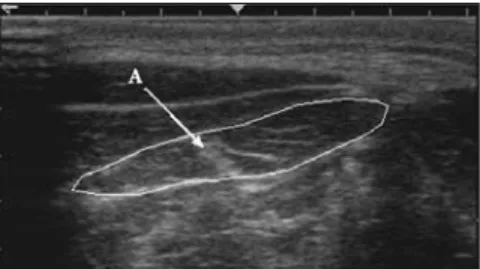
FIGURE 10.Transverse ultrasound image of the left semispinalis capitis muscle, a long strap-like muscle, using a 7.5-MHz linear transducer. The cross-sectional area and aponeurosis (A) dividing the muscle into medial and lateral parts are indicated. (Reproduced from Rankin et al,61 with permission).
1.06 0.19 cm2) compared with healthy females (right, 1.23 0.09 cm2; left, 1.25
0.10 cm2) (P.05).37 Studies of mul-tifidus at C4 showed slight differences in CSA between the groups studied but marked differences in shape ratio,37,39 as
evident inTABLE 5. These differences for cervical multifidus could have been due to the different postures used for imag-ing, as in 1 study the subjects were ly-ing prone37 and in the other they were sitting,39 which could have affected the tonic activity of the resting muscle. There were no differences in measurements of the semispinalis capitis muscle made in prone and sitting,63 and the 2 studies of the semispinalis capitis were in agree-ment.61,63 The shape ratio value indicates the shape well, for example, the 2 flat superficial muscles, splenius capitis and semispinalis capitis, were approximately 7 to 8 times wider than they were thick. The multiplied linear dimensions were correlated with CSA in all muscles (r = 0.77-0.96).
Reliability of Measurement of Paraspinal
Muscles
Various factors influence the robustness
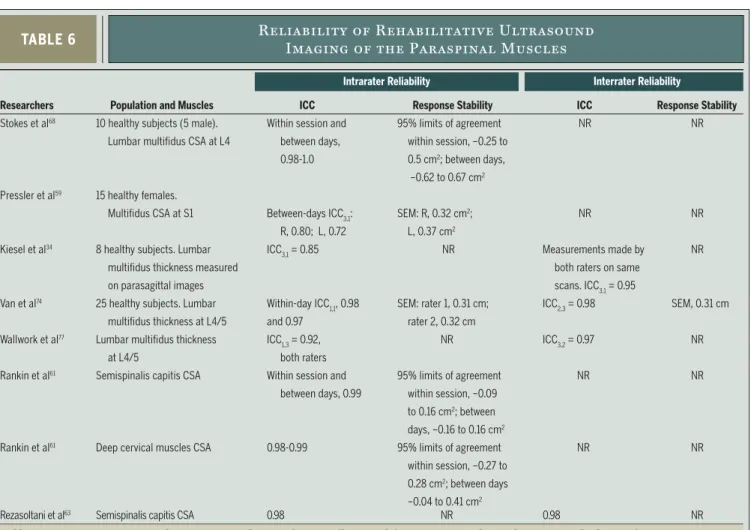
of measurements and have been discussed elsewhere in a related commentary.79 Con-sistently recognizable bony features can be useful internal landmarks, such as the echogenic vertebral laminae, when imag-ing the paraspinal muscles.68 To our knowl-edge, 8 studies have reported the reliability of using RUSI to measure paraspinal mus-culature. Differences in study design, sta-tistical tests, and reporting method make direct comparisons somewhat difficult, but those values considered key when in-terpreting reliability have been included in
TABLE 6. The majority of researchers mea-sured muscle girth (CSA),59,61,63,68 while others measured thickness utilizing the parasagittal view.34,74,76 Intraclass correla-tion coefficient (ICC) values range from 0.72 to 0.98.
In addition to the ICCs, the standard error of measurement (SEM) or 95% lim-its of agreement, both of which are con-sidered measures of response stability, FIGURE 11.Bilateral transverse ultrasound image of
the deep posterior cervical muscle group, using a 7.5-MHz linear transducer, showing the teardrop shape, consisting of multifidus, rotatores, and semispinalis. The cross-sectional area of cervical multifidus is indicated on the right side of the image. (Reproduced from Kristjansson37with permission.)
TABLE 5
Cervical Paraspinal Muscle Morphometry in Healthy Populations*
Abbreviations: AP, anteroposterior; CSA, cross-sectional area; Lat, lateral; L, left; NR, not reported; R, right. * Subject positioning is indicated for each study. Data are mean 1 SD, except for age ranges, with 2 exceptions.
CSA Versus Lat Linear Shape AP Dimension Dimension Dimensions Muscle/Position Level Population Age (y) CSA (cm2) Ratio Lat/AP (Thickness) (cm) (cm) Multiplied (r)
Splenius capitis
Prone lying62 C3 Females, n = 10 19-29 R, 1.90
0.23 R, 8.831.05 NR NR 0.77 L, 1.760.25 L, 8.541.08 Semispinalis capitis Sitting63 C3 Males, n = 18 19-34 R, 1.99 0.37 R, 6.820.93 R, 0.580.08 R, 3.850.39 0.85 L, 1.930.38 L, 6.581.04 L, 0.590.08 L, 3.760.36 Females, n = 28 19-34 R, 1.570.35 R, 7.001.07 R, 0.510.08 R, 3.550.42 L, 1.560.34 L, 6.861.10 L, 0.520.07 L, 3.530.41 Prone lying61 C3 Males, n = 46 20-72 1.77
0.40 7.201.14 0.530.08 3.730.39 0.86 Females, n = 53 18-70 1.340.42 7.101.34 0.480.11 3.270.48 0.84 Deep neck muscles
Prone lying61 C3 Males, n = 46 20-72 3.15
0.67 0.570.06 2.760.36 1.570.17 0.96 Females, n = 53 18-70 2.600.05 0.570.10 2.490.28 1.400.19 0.84 Cervical multifidus
Sitting39 C4-C6 Males and 26.8
3.8 C4, 0.920.16 C4, 2.400.47 C4, 0.720.10 C4, 1.700.20 NR females, n = 17 C5, 0.960.16 C5, 2.670.52 C5, 0.680.08 C5, 1.800.25 NR C6, 1.200.29 C6, 2.540.63 C6, 0.770.09 C6, 1.900.38 NR Prone lying37 C4 Females n = 10 31.5
11.4 R, 1.230.09 R, 1.680.19 NR NR NR L, 1.250.10 L, 1.580.14 NR NR NR
[
CLINICAL COMMENTARY
]
may be reported (TABLE 6). The purpose of the measurement must also be taken into consideration. For example, it has been shown that by taking an average of 3 measures of the transversus abdominis muscle with RUSI, the SEM is reduced by approximately 50%.67 Reducing the SEM may be helpful in detecting group difference, but may be more important when the purpose of the measure is to as-sess change postintervention. To be 95% confident that true change (greater than measurement error) has occurred from preintervention to postintervention, the change score must exceed the minimal detectable change (MDC) for that mea-sure. The MDC95 is SEM 2 1.96, where 1.96 represents the value of thet
distribution for a 95% confidence inter-val (CI) and is in the units of the mea-sure. For example, Van et al74 used RUSI
to measure lumbar multifidus muscle thickness during contraction. The ICC was reported to be 0.98 and the SEM was 0.31 cm. If this measurement were used to assess change in muscle thickness fol-lowing an intervention period, the MDC95 could be calculated. To be 95% confident that true change occurred, the thickness measured would have had to change by at least the value of the MDC95, which is 0.86 cm, based on 0.31 2 1.96 = 0.86. In general, the reliability of using RUSI to measure paraspinal musculature can be considered to be fair to excellent (ICC = 0.72-0.98) and acceptable for clinical use, as defined by Portney and Watkins.58
Validity of Measurements of Paraspinal
Muscles
Hides et al25 conducted a study to
deter-mine the validity of RUSI measures of lumbar multifidus compared with MRI. Bilateral measurements of CSA were made at vertebral levels from L2 to S1 in healthy females. No significant differ-ences were demonstrated between RUSI and MRI, despite the inherent differenc-es in position for imaging (prone lying for RUSI and supine lying for MRI), when researchers adhered to a strict measure-ment protocol.25
To validate the use of RUSI for mea-suring muscle contraction, changes in muscle thickness have been compared to EMG activity of various muscles, includ-ing the transversus abdominis49,29 and lumbar multifidus muscles.34 The rela-tionship varies between muscles and the experimental protocol (eg, contraction type), but, in general, it is considered to be curvilinear.
TABLE 6
Reliability of Rehabilitative Ultrasound
Imaging of the Paraspinal Muscles
Abbreviations: CSA, cross-sectional area; ICC, intraclass correlation coefficient; L, left; NR, not reported; R, right; SEM, standard error of measurement.
Interrater Reliability
Researchers Population and Muscles ICC Response Stability ICC Response Stability
Stokes et al68 10 healthy subjects (5 male). Within session and 95% limits of agreement NR NR
Lumbar multifidus CSA at L4 between days, within session, –0.25 to 0.98-1.0 0.5 cm2; between days,
–0.62 to 0.67 cm2
Pressler et al59 15 healthy females.
Multifidus CSA at S1 Between-days ICC3,1: SEM: R, 0.32 cm
2; NR NR
R, 0.80; L, 0.72 L, 0.37 cm2
Kiesel et al34 8 healthy subjects. Lumbar ICC
3,1= 0.85 NR Measurements made by NR
multifidus thickness measured both raters on same on parasagittal images scans. ICC3,1= 0.95
Van et al74 25 healthy subjects. Lumbar Within-day ICC
1,1, 0.98 SEM: rater 1, 0.31 cm; ICC2,3= 0.98 SEM, 0.31 cm
multifidus thickness at L4/5 and 0.97 rater 2, 0.32 cm Wallwork et al77 Lumbar multifidus thickness ICC
1,3= 0.92, NR ICC3,2= 0.97 NR
at L4/5 both raters
Rankin et al61 Semispinalis capitis CSA Within session and 95% limits of agreement NR NR
between days, 0.99 within session, –0.09 to 0.16 cm2; between
days, –0.16 to 0.16 cm2
Rankin et al61 Deep cervical muscles CSA 0.98-0.99 95% limits of agreement NR NR
within session, –0.27 to 0.28 cm2; between days
–0.04 to 0.41 cm2
Rezasoltani et al63 Semispinalis capitis CSA 0.98 NR 0.98 NR
In the parasagittal view of the lum-bar multifidus muscles, Kiesel et al34 studied the relationship between thick-ness change (percent change from rest) and fine-wire EMG activity (percent of maximum) during a contralateral prone arm-lifting task with increasing resis-tance, which automatically recruited the ipsilateral multifidus muscle. This task produced contractions from 19% to 43% of maximum effort, with a strong corre-lation (r = 0.79,P.001) between thick-ness change and EMG activity. But, there was no significant difference in multifi-dus thickness change between the last 2 levels of activation, indicating that the EMG signal continued to increase with load but thickness change was nearing its maximum. Muscles are considered to reach their maximum thickness at relatively low EMG values (approxi-mately 20% of maximal contraction).29 In isometric contractions this relates to the point at which tendon stiffness pre-cludes further tendon stretch and the muscle continues to form cross-bridges and increase electrical activity, but with minimal further change in length and, therefore, thickness. Many functional daily activities involve contractions at relatively low forces, which would fall within the linear part of the relationship, where change in EMG reflects change in muscle thickness. With respect to joint stabilization, mathematical models have predicted that only low-level contrac-tions of the lumbar multifidus muscle are required to stiffen the spine.6 Clini-cians have therefore advocated low-level voluntary contractions to train the mul-tifidus muscle for this role, which can be aided by observing changes in thickness on RUSI images.24
Vasseljen et al75 used high-speed M-mode ultrasound to identify deformation of the deep fibers of the lumbar multifid-us mmultifid-uscle with concurrent EMG signal to test the validity of using the ultrasound to measure the timing of activation. Sub-jects performed rapid arm lifting, which is known to activate the deep and superfi-cial lumbar multifidus muscle,51 the onset
of which may be delayed in patients with LBP. Visual determination of the muscle onset using ultrasound was comparable to EMG, but with a small systematic de-lay. Although preliminary, these results suggest that ultrasound may be used in the future to measure deep muscle onsets clinically.
Validity of RUSI against MRI was ex-amined for the cervical multifidus muscle in 10 healthy subjects at 3 cervical levels from C4 to C6.39 Lee et al39 considered that validity was acceptable for muscle thickness measurements (R2 = 0.42-0.64), but not for CSA (R2 = 0.11-0.39) and width (R2 = 0.16-0.69). The small CSA of the muscle (approximately 1 cm2 compared with 7 cm2 for lumbar multi-fidus) may amplify errors, thus influence the variability of measurements.
CLINICAL STUDIES OF STATIC
PARAMETERS
T
he paraspinal muscles have beenstudied using RUSI to assess the ef-fects of acute and chronic LBP, as well as the effects of interventions, such as exercise and spinal surgery.
Acute LBP
Hides et al27 found marked side-to-side asymmetry of the lumbar multifidus mus-cle CSA in 26 patients with first-episode acute unilateral LBP. The smaller muscle was found at the symptomatic segment (identified by manual palpation), was on the side ipsilateral to symptoms, and was confined predominantly to 1 vertebral level. In the 26 subjects with LBP, aver-age (SD) between-side difference was 31% 8%, compared with 3% 4% in 51 asymptomatic subjects. It was not pos-sible to determine whether the reduction in CSA was pre-existing in these subjects. However, data from a study using a por-cine model have confirmed that the CSA of the lumbar multifidus muscle reduces rapidly (as early as 3 days) after injury to an intervertebral disc, is isolated to a sin-gle segment (the level below the injured disc), and is associated with
histochemi-cal changes in the muscle.28
Kiesel et al33 demonstrated the effect of pain on lumbar multifidus muscle func-tion experimentally in humans. Increases in multifidus thickness during arm-lifting tasks were significantly reduced by pain in response to injection of saline into the erector spinae muscles. This investigative application of RUSI not only contributed to knowledge about the effects of pain on muscle activation but added to the valid-ity of RUSI as a clinical measurement of muscle dysfunction.
Chronic LBP
Significant atrophy of CSA was found by Hides et al22 in patients with chronic LBP compared with healthy controls at the lowest 2 lumbar vertebral levels. Greatest asymmetry was seen at L5 in those with unilateral pain. These results were in agree-ment with previous computed tomography studies indicating that the pattern of lum-bar multifidus muscle atrophy in patients with chronic LBP was localized to the lower region of the spine rather than generalized13 and that asymmetry occurred in those with unilateral pain.1 In an MRI study of patients with LBP, Barker et al1 also reported this selective, localized atrophy. Conversely, an-other study using computed tomography to measure patients with chronic LBP found generalized atrophy in the lumbar spine but also relatively greater CSA of multifi-dus on the symptomatic side.70 This finding was consistent with histological evidence of type I fiber hypertrophy and type II fiber atrophy in individuals with chronic LBP,17 possibly indicating an adaptive response to muscle wasting. We speculate that this pseudohypertrophy could also be related to fatty infiltration.35
Prelumbar Surgery and Postlumbar
Surgery
Imaging techniques have proved use-ful for investigating the effects of spi-nal surgery on the lumbar multifidus muscle.32,38,66 In cases of unilateral LBP, researchers using computed tomography found that paraspinal muscles were 10% to 30% smaller on the affected side
com-[
CLINICAL COMMENTARY
]
pared to the unaffected side and fatty de-generation was also evident.38 Reduced muscle CSA was seen using RUSI in patients prior to surgery with atrophy being more severe in those with greater LBP.32 Postoperative images showed no further decrease in CSA. However, it was not possible to confirm that muscle at-rophy had not occurred, as size changes could have been masked by intramus-cular inflammation, seen as hypoechoic areas. Long-term follow-up at 1 year in-dicated that multifidus muscle atrophy was long lasting.
QUALITATIVE ASSESSMENT
AND FEEDBACK
B
oth static and dynamicparam-eters can be assessed qualitatively using RUSI. Static assessment gen-erally involves evaluating the ultrasound image focusing on tissue quality. The as-sessment of dynamic parameters includes using USI to evaluate the ability of the muscle to contract and teaching muscle activation using the image as a source of biofeedback.
Assessment of Static Parameters
Impairments of the lumbar muscles in subjects with LBP have been demon-strated in terms of both decreased mus-cle size and density.27,50 Decreased muscle density can be caused by fatty infiltration (increased fat-muscle fiber ratio) or ac-tual fatty replacement of fibers.35,45While changes in density have been predomi-nantly reported in computed tomography and MRI studies, changes in consistency of the lumbar multifidus muscles have been observed using USI.27,32 The ultra-sound appearance of healthy muscle is usually dark, due to its excellent perfu-sion and resultant high fluid content. The presence of fatty infiltration, fibrous changes, or scar tissue (noncontractile tissue) leads to a change in its sonograph-ic appearance, as noncontractile tissue is hyperechoic, making muscle appear more white (FIGURE 12).27 On computerized to-mographic scans, normal healthy muscleappears grey and uniform. Consistency changes will present as dark areas. In contrast, on specific MRI sequencing, fatty infiltration and fibrous changes ap-pear white. Consistency changes have most commonly been reported in sub-jects with chronic LBP.30
The fat content of the lumbar multifi-dus and longissimus muscles was mea-sured in 25 patients with chronic LBP and 25 matched asymptomatic volun-teers using MR spectroscopy.50 There was a significantly higher mean percentage of fat content in subjects with chronic LBP (23.6%; 95% CI: 17.5%, 29.7%) than in asymptomatic subjects (14.5%; 95% CI: 10.8%, 18.3%). Values for the longissi-mus longissi-muscle did not differ between pa-tients and control subjects. Further work
is required to validate the interpretation of muscle density on RUSI and to de-termine reliability. This is likely to be a complex task because image brightness is influenced by the individualized gain settings used by the operator.
Lumbar multifidus muscle atrophy ap-pears to be a common finding in patients with chronic LBP. In a recent MRI study of 78 patients with LBP (with and without lower extremity pain), changes in multif-idus muscle consistency were graded as mild (fatty or fibrous tissue replacement less than 10%), moderate (replacement less than 50%), and severe (greater than 50%).30 Degeneration of multifidus was present in 80% of the subjects with LBP, and most commonly occurred at the L4-L5 and L4-L5-SI levels. Sixty-six of the 78 patients with LBP (85%) had degener-ated lumbar discs on MRI.
Assessment of Dynamic Parameters
Clinical assessment of paraspinal muscle performance involves palpation of the lumbar multifidus muscles at each ver-tebral level as the patient preferentially activates the muscle. Muscle thickness changes can be seen using real-time RUSI (FIGURE 13) as the patient performs the test maneuver and have been dem-onstrated reliably in the lumbar24,26 and cervical muscles.39FIGURE 13.Biofeedback of lumbar multifidus: parasagittal view using split-screen function and 5-MHz curvilinear transducer. The facet joints (F) were used as landmarks for the lower borders of the multifidus (M) muscle. During contraction (right panel), the muscle becomes thicker and the angle of the fibers becomes steeper, providing feedback. The left panel shows the muscle at rest.
FIGURE 12.Hyperechoic lumbar multifidus muscle at L5 in a patient with chronic low back pain, using a 5-MHz curvilinear transducer. The muscle tissue appears whiter compared with that in the scans of normal subjects in Figures 3, 7, 8, and 9.
The ability of patients with chronic LBP to activate the lumbar multifidus muscle has been found to be reduced, as evidenced by smaller increases in thick-ness on RUSI images during contrac-tion than in asymptomatic controls.77 A randomized controlled trial of healthy subjects by Van et al74 examined whether visual biofeedback using RUSI enhanced the ability to activate the lumbar multifi-dus muscle. All subjects received clinical instruction on how to activate the mul-tifidus muscle isometrically and verbal feedback on performance (acquisition phase). The intervention group received visual biofeedback with RUSI in parasag-ittal section.24,26,34 Both subject groups improved voluntary contraction (increas-es from r(increas-esting thickn(increas-ess) in the acqui-sition phase, but the RUSI biofeedback group achieved greater improvements. On reassessment a week later (retention phase), the RUSI group maintained the improvements, whereas performance in the control group decreased.
A clinical randomized controlled tri-al of people with acute LBP used RUSI successfully for feedback of lumbar mul-tifidus muscle activation.26 Symmetry of multifidus CSA was restored in the exer-cise intervention group within 4 weeks. Despite pain relief and the general muscle use associated with return to normal ac-tivity levels, patients in the control group (conventional treatment) still displayed multifidus atrophy at a 10-week fol-low-up. Long-term results revealed that subjects from the specific-exercise group experienced fewer recurrences of LBP than the control group.23 A limitation of this work is the lack of comparison with an exercise group focusing on multifidus rehabilitation without RUSI feedback. Nevertheless, other investigators have similarly advocated the benefits of RUSI for teaching muscle activation.14,20,24,74
The principles of motor learning16 may explain why visual feedback is of benefit for subjects with LBP. In the initial stages of learning a new skill (cognitive stage), time is spent understanding the demands of the task, what to do, and what to feel. The
clin-ical observation that people with LBP find it difficult to contract the lumbar multifi-dus muscle may be due to processes such as reflex inhibition,69 which was thought to play a role in multifidus wasting in individ-uals with acute LBP.27 Biofeedback may be beneficial as subjects with LBP have been shown to have decreased proprioception,57 which affects their ability to provide and process internal feedback.
Clinical Implications
Prescription of therapeutic exercise for the patient with LBP is based on knowl-edge of normal function of the paraspinal muscles, and the presence and nature of impairment in terms of size or activation. Impairment of lumbar multifidus is of-ten specific to the side and vertebral level of symptoms22,24,26,27 and this has been found in subjects with acute and chronic LBP. Before the introduction of RUSI into clinical practice, physical therapists could only palpate for multifidus muscle atrophy. This may have previously led to an underestimation of atrophy. Via visualization of the paraspinal muscles using RUSI, impairments can be better assessed and documented. In addition to objective measurements of muscle size, changes in muscle consistency can also be observed. RUSI can be used to pro-vide baseline measures of impairments, and also to document improvements over time and with intervention. Therapeutic exercise may need to be as specific as the impairments that occur in order to address them. RUSI can provide visual feedback to enhance motor learning for contracting a specific muscle or part of a muscle. From a clinical perspective, the use of imaging techniques has already provided a wealth of information in both research and clinical practice.
Evidence that feedback with RUSI en-hances motor learning holds promise for the future but studies are needed on sub-jects with LBP, and therapeutic exercise interventions need to be compared with and without the use of RUSI for biofeed-back, to ultimately determine the benefits of this rehabilitation tool.
DIRECTION OF FUTURE
RESEARCH
A
lmost all lines of research onparaspinal muscles produce more questions or uncover areas of un-certainty. If RUSI is to become a routine aid to physical therapy practice and a ro-bust research tool, standardized protocols are needed. Technical studies of the size of the transducer and whether linear and curvilinear arrays produce the same mea-surements are needed to provide guid-ance on appropriate methodology. The predictive value of linear measurements to provide an estimate of CSA needs to be established for different muscles in dif-ferent states, such as resting, contracted, wasted, or hypertrophied. The validity of using linear measurements to predict the CSA of irregularly shaped muscles re-quires attention.
Comprehensive studies of healthy populations are needed to generate refer-ence databases for assessing the effects of pathology and interventions. Factors to consider include age, gender, body type (physical characteristics including height and body mass), ethnicity, geographic distribution (due to lifestyle differences), and levels of habitual physical activity from sedentary to elite sporting groups. Data for interrelationships between dif-ferent spinal levels would be useful for detecting abnormality at a specific level.
Substantial work remains to validate the dynamic techniques for measuring both magnitude and timing of changes in muscle for clinical use. Longitudinal epi-demiological studies are needed to deter-mine those at risk of developing LBP or neck conditions, whether wasting occurs before the onset of injury and/or pain, and to help elucidate the mechanisms of wasting.
The contribution of noncontractile tissue to CSA, affecting the density (or consistency) of muscle, needs to be quan-tified to determine true muscle size with pathology, particularly in subjects with chronic pain, and aging. The sonographic technique of elastography is potentially
[
CLINICAL COMMENTARY
]
@
MORE INFORMATION
WWW.JOSPT.ORG
REFERENCES
1.Barker KL, Shamley DR, Jackson D. Changes in the cross-sectional area of multifidus and psoas in patients with unilateral back pain: the rela-tionship to pain and disability.Spine.2004;29: E515-519.
2.Bogduk N. The clinical anatomy of the cervical dorsal rami.Spine.1982;7:319-330.
3.Bogduk N. ClinicalAnatomy of the Lumbar Spine and Sacrum.Edinburgh, UK: Churchill Livingston; 2006.
4.Bogduk N, Macintosh JE, Pearcy MJ. A universal
model of the lumbar back muscles in the up-right position.Spine.1992;17:897-913.
5.Burton A. Regional lumbar sagittal mobility: measurement by flexicurves.Clin Biomech.
1986;1:20-26.
6.Cholewicki J, McGill SM. Mechanical stability of the in vivo lumbar spine: implications for injury and chronic low back pain.Clin Biomech (Bris-tol, Avon).1996;11:1-15.
7.Cholewicki J, Panjabi MM, Khachatryan A. Stabilizing function of trunk flexor-extensor muscles around a neutral spine posture.Spine.
1997;22:2207-2212.
8. Cholewicki J, VanVliet JJ. Relative contribution of trunk muscles to the stability of the lumbar spine during isometric exertions.Clin Biomech (Bristol, Avon).2002;17:99-105.
9.Chudleigh T, Thilaganathan B.Obstetric Ultra-sound.London, UK: Churchill Livingstone; 2004.
10.Coldron Y, Stokes M, Cook K. Lumbar multifidus muscle size does not differ whether ultrasound imaging is performed in prone or side lying.Man Ther.2003;8:161-165.
11.Corneil BD, Olivier E, Richmond FJ, Loeb GE, Mu-noz DP. Neck muscles in the rhesus monkey. II. Electromyographic patterns of activation under-lying postures and movements.J Neurophysiol.
2001;86:1729-1749.
12.Crisco JJ, third, Panjabi MM. The intersegmental and multisegmental muscles of the lumbar spine. A biomechanical model comparing lateral stabilizing potential.Spine.1991;16:793-799.
13. Danneels LA, Vanderstraeten GG, Cambier DC, Witvrouw EE, De Cuyper HJ. CT imaging of trunk muscles in chronic low back pain patients and healthy control subjects.Eur Spine J.
2000;9:266-272.
14.Dietz HP, Wilson PD, Clarke B. The use of peri-neal ultrasound to quantify levator activity and teach pelvic floor muscle exercises. Int Urogy-necol J Pelvic Floor Dysfunct.2001;12:166-168; discussion 168-169.
15. Elliott J, Jull G, Noteboom JT, Darnell R, Gal-loway G, Gibbon WW. Fatty infiltration in the cervical extensor muscles in persistent whiplash-associated disorders: a magnetic resonance imaging analysis.Spine.2006;31: E847-855.
16.Fitts PM, Posner MI.Human Performance. Bel-mont, CA: Brooks/Cole; 1967.
17.Fitzmaurice R, Cooper RG, Freemont AJ. A histo-morphometric comparison of muscle biopsies from normal subjects and patients with ankylos-ing spondylitis and severe mechanical low back pain.J Pathol.1992;163:182A.
18.Granata KP, Marras WS. Cost-benefit of muscle cocontraction in protecting against spinal insta-bility.Spine.2000;25:1398-1404.
19.Hayashi N, Masumoto T, Abe O, Aoki S, Ohtomo K, Tajiri Y. Accuracy of abnormal paraspinal muscle findings on contrast-enhanced MR im-ages as indirect signs of unilateral cervical root-avulsion injury.Radiology.2002;223:397-402.
20.Henry SM, Westervelt KC. The use of real-time ultrasound feedback in teaching abdominal
hol-lowing exercises to healthy subjects.J Orthop Sports Phys Ther.2005;35:338-345.
21.Hides J, Cooper DH, Stokes MJ. Diagnostic ultra-sound imaging for measurement of the lumbar multifidus muscle in normal young adults. Phys-iother Theor Pract.1992;8:19-26.
22.Hides J, Gilmore C, Stanton W, Bohlscheid E. Multifidus size and symmetry among chronic LBP and healthy asymptomatic subjects.Man Ther.2006 Oct 26; [Epub ahead of print].
23.Hides JA, Jull GA, Richardson CA. Long-term ef-fects of specific stabilizing exercises for first-ep-isode low back pain.Spine.2001;26:E243-248.
24.Hides JA, Richardson CA, Jull G. Use of real-time ultrasound imaging for feedback in reha-bilitation.Man Ther.1998;3:125-131.
25.Hides JA, Richardson CA, Jull GA. Magnetic resonance imaging and ultrasonography of the lumbar multifidus muscle. Comparison of two different modalities.Spine.1995;20:54-58.
26.Hides JA, Richardson CA, Jull GA. Multifidus muscle recovery is not automatic after resolu-tion of acute, first-episode low back pain.Spine.
1996;21:2763-2769.
27.Hides JA, Stokes MJ, Saide M, Jull GA, Cooper DH. Evidence of lumbar multifidus muscle wasting ipsilateral to symptoms in patients with acute/subacute low back pain.Spine.
1994;19:165-172.
28.Hodges P, Holm AK, Hansson T, Holm S. Rapid atrophy of the lumbar multifidus follows ex-perimental disc or nerve root injury.Spine.
2006;31:2926-2933.
29.Hodges PW, Pengel LH, Herbert RD, Gande-via SC. Measurement of muscle contraction with ultrasound imaging.Muscle Nerve.
2003;27:682-692.
30.Kader DF, Wardlaw D, Smith FW. Correla-tion between the MRI changes in the lumbar multifidus muscles and leg pain.Clin Radiol.
2000;55:145-149.
31. Kaigle AM, Holm SH, Hansson TH. Experi-mental instability in the lumbar spine.Spine.
1995;20:421-430.
32.Kelley SM.The Effect of Two Exercise Programs Following Back Surgery [thesis]. Queensland, Australia: University of Queensland; 2005.
33.Kiesel KB, Uhl T, Underwood FB, Nitz AJ. Re-habilitative ultrasound measurement of select trunk muscle activation during induced pain.
Man Ther.2006 Dec 30; [Epub ahead of print].
34.Kiesel KB, Uhl TL, Underwood FB, Rodd DW, Nitz AJ. Measurement of lumbar multifidus muscle contraction with rehabilitative ultrasound imag-ing.Man Ther.2007;12:161-166.
35.Kjaer P, Bendix T, Sorensen JS, Korsholm L, Le-boeuf-Yde C. Are MRI-defined fat infiltrations in the multifidus muscles associated with low back pain?BMC Med.2007;5:2.
36.Kline P.A Handbook of Test Construction. Lon-don, UK: Methuen; 1986.
37.Kristjansson E. Reliability of ultrasonography for the cervical multifidus muscle in asymp-tomatic and sympasymp-tomatic subjects.Man Ther.
2004;9:83-88.
useful for distinguishing the biome-chanical behavior of these tissues.53,79 It would be of interest to know if the ratio of noncontractile tissue to contractile tissue can be altered with therapeutic exercise. Elastography may also help distinguish between activity of the deep and superfi-cial parts of muscle to study their differ-ing functions.
The effects of different pathologies on the paraspinal muscles need to be established in musculoskeletal and neu-rological disorders. Large randomized controlled trials are needed to demon-strate that RUSI is a reliable outcome measure for assessing the effects of in-terventions. We recommend that future studies present data consistently and use the same statistical methods, as outlined by Whittaker et al79 to enable valid com-parison between studies and to enhance accumulation of large reference databas-es as a common rdatabas-esource for evaluation of abnormality.
ACKNOWLEDGEMENTS
W
e thank the following forproviding images for the figures: Dr Cliff Barnes, Associate Pro-fessor in charge of Neuroanatomy in the Department of Physical Therapy at Regis University, Denver, for help with produc-ing the image of the cadaver dissection in FIGURE 1; Nick Smith, Peter Worsley, and Martin Warner, School of Health Professions and Rehabilitation Sciences, University of Southampton, UK, for the ultrasound scan inFIGURE 4.