Annals of Clinical & Laboratory Science, vol. 42, no. 3, 2012
BRAF
V600E
Mutation Testing in Fine Needle Aspirates of
Thyroid Nodules: Potential Value of Real-Time PCR
Jin Young Kwak1, Kyung Hwa Han2, Jung Hyun Yoon3, Eun-Kyung Kim1, Hee Jung Moon1, Yoo-Li Kim4
Seo-Jin Park5, and Jong Rak Choi5
1Department of Radiology and Research Institute of Radiological Science, Severance Hospital, Yonsei University College
of Medicine, Seoul, Korea; 2Department of Biostatistics, Severance Hospital, Yonsei University College of Medicine,
Seoul, Korea; 3Department of Radiology, Bundang CHA Medical Center, CHA University College of Medicine,
Seong-nam, Korea; 4Department of Research and Development, BioSewoom Inc., Seoul, Korea; 5Department of Laboratory
Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
Abstract. The BRAFV600E mutation is a valuable adjunctive diagnostic tool to ultrasound (US)-guided fine-needle aspiration (US-FNA). The objective of this study was to investigate the potential value of real-time PCR to detect BRAFV600E mutation. This study included 447 thyroid nodules in 420 patients who underwent US-FNA and BRAFV600E mutation analysis using dual priming oligonucleotide-based multi-plex polymerase chain reaction (DPO-PCR) and real-time PCR. We calculated and compared the diagnos-tic performances of DPO-PCR and real-time PCR to detect BRAFV600E mutation in the thyroid nodules. Receiver operating characteristic (ROC) analysis was used to quantify the cut-off value of the Ct values of BRAFV600E mutation on real-time PCR. Optimal thresholds were determined (Youden index). We also compared the diagnostic performances between DPO-PCR and real-time PCR after applying the cut-off value on real-time PCR. Sensitivity, accuracy, and NPV were significantly higher in real-time PCR than DPO-PCR. When the optimal cut-off value of 32.4 at Ct values of BRAFV600E mutation was adjusted on real-time PCR, sensitivity was 66.2% and specificity was 100%. Sensitivity, accuracy, and NPV of real-time PCR were also significantly higher than DPO-PCR. In contrast, specificity and PPV were not significantly different between DPO-PCR and real-time PCR. Real time PCR can be a promising diagnostic method in detecting BRAFV600E mutation using optimal cut-off value.
Key words: real-time PCR, DPO-PCR, BRAF, papillary thyroid cancer
Address correspondence to Jong Rak Choi, MD; Department of Laboratory Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, Korea; phone: 82-2-2228-2445; fax: 82-2-364-1583; email: cjr0606@ yuhs.ac
0091-7370/12/0300-258. © 2012 by the Association of Clinical Scientists, Inc. Introduction
Papillary thyroid carcinoma (PTC) is the most common malignancy involving the endocrine sys-tem, and its incidence has sharply increased due to the widespread usage of high resolution ultrasound (US) for medical surveillance [1]. US-guided fine needle aspiration (US-FNA) is a highly sensitive and accurate method in the diagnosis of thyroid nodules. However, cytologic evaluation is not al-ways accurate in documenting the nature of thy-roid nodules because of non-diagnostic, indetermi-nate, false-negative, and false-positive results [2,3]. Indeed, cytology results are influenced by many
factors, including the performer’s skill, technique of preparation, and experiences of interpreting cy-tologists [4].
As an adjunctive diagnostic tool of FNA, BRAFV600E mutation can help recognize PTC in some equivocal cases, especially in thyroid nodules with “non-diagnostic” or “suspicious for malignan-cy” cytologic results [5,6]. Several methodologies have been introduced in detecting a BRAFV600E mutation in thyroid nodules. Among the various methods, pyrosequencing and dual priming oligo-nucleotide-based multiplex polymerase chain reac-tion (DPO-PCR) have been widely accepted in detecting BRAFV600E mutation in Korea because of their high sensitivity [7-11]. Most studies have demonstrated a specificity of 100% in detecting BRAFV600E mutation in thyroid cancer, except for 258
recent studies showing false-positive results when using highly sensitive methodologies, such as pyro-sequencing and DPO-PCR [7,9-11].
Real time PCR was introduced to quantify mRNA expression easily [12] and has been used in various genetic fields [13,14]. Recently, real-time PCR has been used to detect genetic mutations including the BRAFV600E mutation in colorectal cancer and melanoma [15,16]. Another study used quantitative real-time PCT analyzing BRAFV600E mutation in thyroid nodules, but this study had limitations because a small sample size was included and nod-ules with undetermined cytology had been includ-ed [17]. Therefore, we investigatinclud-ed the potential value of real-time PCR in detecting BRAFV600E mutation in a relatively large sample and compared it with DPO-PCR.
Materials and Methods
The Institutional Review Board approved of this study and required neither patient approval nor in-formed consent for our review of patient images and records. However, informed consent was ob-tained from all patients for US-FNA and BRAFV600E mutation analysis prior to each procedure.
Study Population. This study was performed at Severance Hospital (a referral center) from June 2009 to October 2010. During the study period, US-FNA and BRAFV600E mutation analysis using DPO-PCR were performed on aspiration speci-mens from 1,114 thyroid nodules. The BRAFV600E mutation analysis was performed by clinicians’ re-quest or radiologists’ recommendations based on factors such as the presence of suspicious US fea-tures. Of the nodules, 558 nodules were excluded because they did not undergo further evaluation such as surgery, follow-up FNA, and follow-up US. Additional 71 nodules were excluded because they had increased in size during follow-up US. Thirty-eight nodules were also excluded because they had inconclusive cytologic results after repeated FNA. Among these, we selected 447 consecutive FNA samples to be studied with real-time PCR, of these: (a) 345 underwent thyroid surgery regardless of cy-tologic results, (b) 28 were PTC on US-FNA with-out surgery, (c) 48 had benign cytology at least
twice without surgery, and (d) 26 had benign cytol-ogy without interval change or decreased in size at follow-up US within a year. Finally, this study in-cluded 447 thyroid nodules in 420 patients (346 women and 74 men). 394 patients had one thyroid nodule, 25 had two nodules, and 1 had three nodules. Mean age of the patients was 48 years of age (range, 17 – 78 years). The mean size of nodules was 9.2 mm (range, 3 - 52 mm).
US Analysis. US images were obtained using iU22 5–12 MHz linear probe (Philips Medical Systems, Bothell, WA) or a 6–13 MHz linear probe (Hitachi Medical, Tokyo, Japan) in the evaluation of thyroid glands and neck areas. Compound imaging was obtained in all images from the iU22 machine. Real-time US imaging was performed by 7 board-certified radiologists with 1 - 15 years of experi-ences in thyroid imaging.
US features of all thyroid nodules that underwent US-FNA were prospectively recorded according to the internal component, echogenicity, margin, cal-cification, and shape at the time of US examina-tion. Microcalcifications, irregular or microlobu-lated margins marked hypoechogenicity, and taller than wide shape are the US characteristics that are considered malignant in our institution. Suspicious malignant nodules were defined as those showing one or more of the suspicious US findings present-ed above [18].
US- FNA and Cytologic Analysis. After US ex-aminations, US-FNA was performed by the same radiologists who evaluated the thyroid gland with US. At our institution, US-FNAs were performed on either the thyroid nodule with suspicious US features or the largest thyroid nodule if no suspi-cious US features were detected. US-FNA was per-formed with a 23-gauge needle attached to a 2-mL disposable plastic syringe with free hand technique. Each lesion was aspirated at least twice. Materials obtained from aspiration were expelled onto glass slides and smeared. All smears were placed imme-diately in 95% alcohol for Papanicolaou staining. Cytopathologists were not on site during the biopsy. Additional special staining was done on a case-by-case basis according to the cytopatholo-gist’s needs. One of five cytopathologists specializ-ing in thyroid cytology interpreted the
smears obtained from US-FNA. In our institution, cytology reports were divided into the following 5 categories from June 2009 to November 2009: 1) benign, 2) indeterminate cytology, 3) suspicious for papillary thyroid carcinoma (PTC), 4) malignant, and 5) inadequate [19]. After December 2009, the Bethesda classifications have been used in the clas-sification of cytology results: category 1) nondiag-nostic, category 2) benign, category 3) atypia, cat-egory 4) follicular neoplasm or suspicious for follicular neoplasm, category 5) suspicious for ma-lignancy, and category 6) malignant [20].
The material remaining in the syringe after cyto-logical preparation was collected for BRAFV600E mutation analysis. DNA was extracted immedi-ately upon arrival at the laboratory and stored at -20°C until testing for real-time PCR analysis. Detection of BRAFV600E Mutation.
Dual priming oligonucleotide-based multiplex poly-merase chain reaction (DPO-PCR). BRAFV600E mutation analysis using the DPO technology was performed using the Seeplex BRAF ACE detection system (Seegene, Seoul, Korea) as described previ-ously [9].
Real-time PCR. Real-time PCR was performed us-ing Applied Biosystems 7500 real-time PCR sys-tem (Applied Biosyssys-tems, Foster City, CA, USA) under the following conditions: at 50°C for 2 min for one cycle, denaturation at 95°C for 10 min for
one cycle and then denaturation at 95°C for 15 sec, and one step of annealing and elongation at 62°C for 45 sec for 40 cycles. Real-Q BRAFV600E Detection Kit (BioSewoom, Korea) was used to carry out PCR reaction. The Real-Q BRAF Detection Kit constitutes a ready-to-use kit for the detection of the BRAF V600E(1799T>A) somatic mutation in the BRAF oncogene in a background of wild type genomic DNA in a multiplex real time PCR assay based on TaqMan MGB probe system. The kit supplies two assays. The BRAF mutation assay is labeled with VIC; it contains allele specific forward primer for the discrimination of the V600E mutation. The internal control assay, labeled with FAM, is used to check for nucleic acid isolation and possible PCR inhibition. It amplifies a region of exon 8 of the BRAF gene. The primers and probe have been designed to avoid any known BRAF polymorphisms.
In assay with clinical sample, the positive reaction of BRAF V600E mutation was determined as in-structions for use of Real-Q BRAFV600E Detection Kit. If FAM signal (control assay) and VIC signal (mutation assay) were observed simultaneously, ∆Ct values by subtracting control Ct value from mutation Ct value were calculated. Samples which showed ∆Ct over 13 cycles were determined as a negative reaction of BRAF V600E mutation, ac-cording to instructions for use of Real-Q BRAFV600E Detection Kit. Using 120 normal ge-nomic DNA samples not containing the BRAF
Figure 1.Cytological and pathological diagnoses of the Surgery Group.
PTC, papillary thyroid carcinoma; PTC, FV, follicular variant of papillary thyroid carcinoma; AH, adenomatous hyper-plasia; FC, MI, minimal invasive follicular carcinoma; FA, follicular adenoma; HCA, Hurthle cell adenoma; MC, medullary carcinoma; PTC, other, Warthin variant of papillary thyroid carcinoma.
V600E mutation, we performed tests of BRAF di-agnostic specificity on Real-Q BRAFV600E Detection Kit. Five DNA samples among 120 DNA samples were amplified between Ct 32.58 and Ct 34.19 in BRAF V600E mutation assay. However, these samples were verified as BRAF V600E negative because it was identified that they calculated ∆Ct (mutation Ct-control Ct) for more than 13 cycles. These 5 samples were amplified be-tween Ct 17.95 and Ct 18.76 in control assay and showed ∆Ct between 14.38 and 16.02. As a result, all of 120 samples were identified BRAF V600E negative.
The 242 bp of partial BRAF gene containing V600E region was amplified from human melano-ma cell line, SK-MEL-28 (ATCC, Manassas, VA, USA) with BRAFV600E mutation and it was in-serted into the pZEM-T Easy Vector (Promega, Madison, WI, USA) to produce the BRAFV600E plasmid DNA. The analytical sensitivity was evalu-ated using the plasmid clone BRAFV600E mutation and the 95% positive cut-off value (limit of detec-tion; LOD) was calculated at 21.5 copy/ul by the Probit analysis.
To determine the cut-off Ct value of BRAF V600E test, 100 repeats of low-positive concentrations of the BRAF V600E plasmid DNA of 64.5copy/ul representing a BRAF V600E concentration equiva-lent to 3x the 95% positive cut-off concentration was used. The positive rate was 100% and the
average Ct value of the 100 repeats was 39.9 cycle. Based on this test, the cut-off point for BRAF V600E positive was set to Ct 40.
Data and Statistical Analysis. The Gold standard for data analysis was based on pathologic results (n=345) (Figure 1). Among the remaining 102 nodules which were not confirmed on pathology, follow-up cytology and US were used to determine gold standard (Figure 2). Categorical data was summarized using frequencies and percentages. We used the χ2 test to compare malignancy to cat-egorical variables. An independent two-sample t
test was used to evaluate the association of malig-nancy to continuous variables.
We calculated the diagnostic performances of DPO-PCR and real-time PCR to detect the BRAFV600E mutation at the thyroid nodules. In this study, we considered cytopathologic results as the gold standard. We compared BRAF status to the gold standard. Detection of BRAFV600E muta-tion in the aspirates that were cytopathologically confirmed as malignant, were considered as TP when calculating the diagnostic performances of BRAFV600E mutation testing. Detection of BRAFV600E mutation in the aspirates that were cy-topathologically confirmed as benign were catego-rized as FP. Failure to detect BRAFV600E mutation group on the benign lesions were considered as TN, and failure to detect BRAFV600E mutation group in the malignant lesions was categorized as
FN. The following statistical values were calculated as: Sensitivity = TP/(TP + FN) x 100; specificity = TN/(TN + FP) x 100; positive predictive value (PPV) = TP/(TP + FP) x 100; negative predictive value (NPV) = TN/(TN + FN) x 100; accuracy = (TP + TN)/(TP + TN + FP + FN) x 100. Receiver operating characteristic (ROC) analysis was used to quantify cut-off value of the Ct values of BRAFV600E mutation on real-time PCR. Optimal thresholds were determined by the Youden index. To compare the diagnostic performances between DPO-PCR and real-time PCR, we used logistic re-gression with GEE (generalized estimating equa-tion) method. We also compared the diagnostic performances between DPO-PCR and real-time PCR after applying the cut-off value on real-time PCR.
Analysis was performed using SAS software (ver-sion 9.1.3; SAS Institute, Cary, NC). Statistical sig-nificance was assumed when the P value was less than 0.05. All reported P values are 2-sided. Results
Of the 447 nodules, 361 nodules (80.8%) were ma-lignant and 86 (19.2%) were benign. Of the 345 nodules which had been operated on, 333 were di-agnosed as malignant. They included conventional
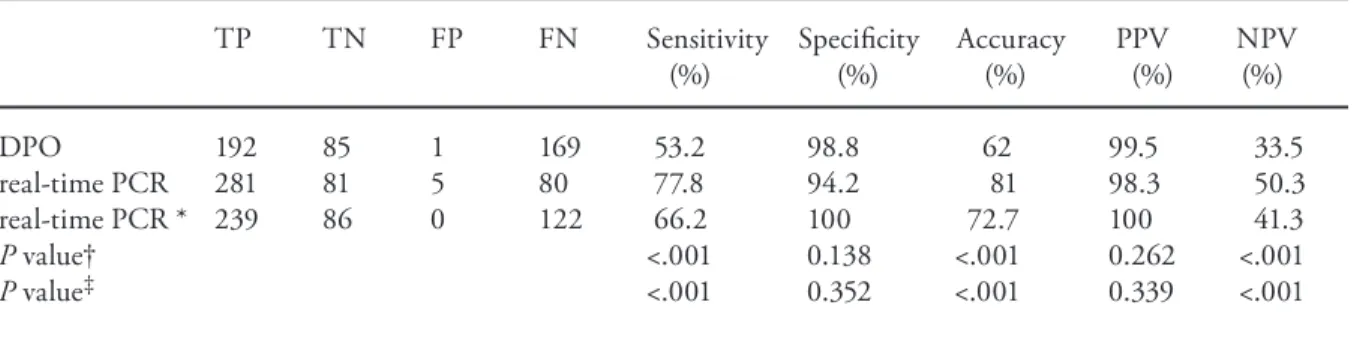
PTC (n = 306), follicular variant of PTC (n = 23), Warthin's tumor like variant of PTC (n=1), minimally invasive follicular carcinoma (n = 2), and medullary carcinoma (n = 1). The 12 benign operated nodules were adenomatous hyperplasia (n=9), follicular adenoma (n=2), and Hurthle cell adenoma (n=1). The mean size of the benign nod-ules was 12 ± 8.8 mm, which was significantly larger than that of malignant nodules, which were 8.5 ± 5.7 mm (P < .001). Patients with malignant nodules were significantly younger (47.3 ± 11.5 years) than those with benign nodules (50.7 ± 10.9 years, P = .013). There was no statistically signifi-cant relationship between gender and malignancy. Sensitivity, accuracy, and NPV were significantly higher when using real-time PCR (77.8%, 81%, and 50.3%, respectively) than DPO-PCR (53.2%, 62%, and 33.5%, respectively) (Table 1). When the optimal cut-off value of 32.4 at Ct values of BRAFV600E mutation was adjusted on real-time PCR, sensitivity was 66.2% and specificity was 100%. Sensitivity, accuracy, NPV, and the area un-der the ROC curve (Az) of real-time PCR were also significantly higher than DPO-PCR (Table 1, Figure 3).
In this study, 245 out of the 361 cancers were pre-operatively diagnosed as malignancy on cytology.
Table 1. Diagnostic performances of dual priming oligonucleotide-based multiplex PCR and real-time PCR in the 447 thyroid nodules in detecting detect malignancy, respectively, and comparison of diagnostic performances between the two methods
TP TN FP FN Sensitivity Specificity Accuracy PPV NPV (%) (%) (%) (%) (%) DPO 192 85 1 169 53.2 98.8 62 99.5 33.5 real-time PCR 281 81 5 80 77.8 94.2 81 98.3 50.3 real-time PCR * 239 86 0 122 66.2 100 72.7 100 41.3 P value† <.001 0.138 <.001 0.262 <.001 P value‡ <.001 0.352 <.001 0.339 <.001
TP, true positive; TN, true negative; FP, false positive; FN, false negative; PPV, positive predictive value; NPV, negative predictive value; DPO-PCR, dual priming oligonucleotide-based multiplex PCR.
real-time PCR*, the cut-off value of threshold cycle was 32.4. P value†, P value between DPO-PCR and real-time PCR.
Among the remaining 116 cancers, the BRAFV600E mutation using DPO-PCR was not detected in 82 nodules. Out of those 82 nodules, of which were detected the BRAFV600E mutation using real time PCR at 17 nodules when Ct cut-off value was 32.4. In contrast, specificity and PPV were not signifi-cantly different between DPO-PCR and real-time PCR.
Discussion
The BRAFV600E mutation is the most common ge-netic event observed in PTC of adults and is seen in approximately 80% of Korean patients [7,21]. Because the BRAFV600E mutation occurs exclu-sively in PTC and PTC-derived anaplastic thyroid cancers and shows high prevalence in Korea, the BRAFV600E mutation has been used as
a complementary diagnostic tool to US-FNA in the diagnosis of malig-nancy in a thyroid nodule [6,9-11,19,22-26]. Recently, highly sensi-tive diagnostic methods for detecting the BRAFV600E mutation, such as py-rosequencing and DPO-PCR, have been introduced and lead us believe that they are a promising diagnostic tool to overcome the limitations of US-FNA [7-11].
Because many reports demonstrated 100% specificity of BRAFV600E muta-tion testing in detecting malignancy, recent detection methods such as py-rosequencing and DPO-PCR have fo-cused on improving diagnostic sensi-tivity [9,11,24,27,28]. However, recent studies showed an exceptionally high diagnostic accuracy (more than 0.9 of Az values) using highly sensitive pyro-sequencing and DPO-PCR (Figure 3), resulting in false positive results of BRAFV600E mutation [7,8]. The false-positive results of BRAFV600E muta-tion may be explained by the trade-off of improved sensitivity by sacrificing specificity [7,8,10]. Az value nearly reached 0.9 even when using direct DNA sequencing, showing a high di-agnostic accuracy with a case showing false positive result (however the sample size was small, necessitating further studies) [23]. To avoid false-positive results of BRAFV600E mutation test, an optimal cut-off value should be applied to reach 100% specificity, albeit sacrificing sensitivity of the test [10]. In this study, we tried to detect BRAFV600E mutation using real-time PCR, and compare it with DPO-PCR. When the optimal cut-off value of 32.4 at Ct values of BRAFV600E mutation was adjusted on real-time PCR, sensitivity, accuracy, and NPV of real-time PCR were also significantly higher than DPO-PCR (Table 1). Comparing with Yeo et al’s study using pyrosequencing, Az value of in our study using real-time PCR was higher than that reported in Yeo’s study (Figure 3). In this study, 116 out of the 361 cancers were pre-operatively not definitely diagnosed as malignant on cytology. BRAFV600E mutation using
Figure 3. Receiver operating characteristic (ROC) curve of BRAFV600E mutation testing in fine-needle aspirates from several studies and this study.
1. Az value was 0.926 by pyrosequencing [7] 2. Az value was 0.909 by DPO-PCR [8]
3. Az value was 0.895 by direct DNA sequencing [23] 4. Az value was 0.688 by direct DNA sequencing [32] 5. Az value was 0.759 by pyrosequencing [10]* 6. Az value was 0.76 by DPO-PCR in this study. 7. Az value was 0.831 by real-time PCR in this study.
*Diagnostic performances were calculated using optimal cut-off value. †The cut-off value of threshold cycle was 32.4.
DPO-PCR were not detected in 82 nodules of which were detected the BRAFV600E mutation us-ing real time PCR at 17 nodules. Therefore, the BRAFV600E mutation test using real time PCR can help these patients to avoid delayed diagnosis. In this study, we found false-positive results in highly sensitive methods (both DPO-PCR and re-al-time PCR). False-positive results can be due to faint low density of mutation band associated with an extensive contamination with wild-type DNA in DPO-PCR [8,29], and non-specific DNA am-plification in real-time PCR [12]. On real-time PCR, Ct value is very important in an accurate and reproducible quantification [30], and Ct values de-crease linearly with increasing input target quanti-ty, which can be used as a quantitative measure-ment of the input target. In this study, we evaluated the optimal cut-off value using Ct values in real-time PCR to obtain 100% specificity of real-real-time PCR. In a real-time PCR setting, we usually regard it negative when the Ct values were larger than or equal to 40. When we regarded the optimal cut-off value of 32.4 in Ct values of BRAFV600E mutation, specificity was 100% and sensitivity was 66.5%. The sensitivity was higher than those of another study using optimal cut-off value of pyrosequening [10], suggesting it a promising method in detecting BRAFV600E mutation.
There are several potential limitations in this study. First, the nodules which had not undergone follow-up or surgery were included, based on the cytology results. This may have affected our results in ways of false-negative or false-positive cytologic results [2,31]. Second, the number of benign nodules in-cluded in this study was relatively small for deter-mining their specificity.
In conclusion, real time PCR can be a promising diagnostic method in detecting BRAFV600E muta-tion using optimal cut-off value.
Acknowledgements
This research was supported by a faculty research grant from Yonsei University College of Medicine for 2011 (No. 6-2011-0081). This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2011-0007711).
References
1. Ezzat S, Sarti DA, Cain DR, Braunstein GD. Thyroid inciden-talomas. Prevalence by palpation and ultrasonography. Arch Intern Med 1994;154:1838-1840.
2. Kwak JY, Koo H, Youk JH, Kim MJ, Moon HJ, Son EJ, Kim EK. Value of US correlation of a thyroid nodule with initially benign cytologic results. Radiology 2010;254:292-300. 3. Yoon JH, Kwak JY, Kim EK, Moon HJ, Kim MJ, Kim JY, Koo
HR, Kim MH. How to approach thyroid nodules with indeter-minate cytology. Ann Surg Oncol 2010;17:2147-2155. 4. Choi SH, Han KH, Yoon JH, Moon HJ, Son EJ, Youk JH,
Kim EK, Kwak JY. Factors affecting inadequate sampling of ultrasound-guided fine-needle aspiration biopsy of thyroid nodules. Clin Endocrinol (Oxf) 2011;74:776-782.
5. Xing M. BRAF mutation in papillary thyroid cancer: patho-genic role, molecular bases, and clinical implications. Endocr Rev 2007;28:742-762.
6. Moon HJ, Kwak JY, Kim EK, Choi JR, Hong SW, Kim MJ, Son EJ. The role of BRAFV600E mutation and ultrasonogra-phy for the surgical management of a thyroid nodule suspicious for papillary thyroid carcinoma on cytology. Ann Surg Oncol 2009;16:3125-3131.
7. Kim SK, Hwang TS, Yoo YB, Han HS, Kim DL, Song KH, Lim SD, Kim WS, Paik NS. Surgical results of thyroid nodules according to a management guideline based on the BRAF(V600E) mutation status. J Clin Endocrinol Metab 2011;96:658-664.
8. Kim SW, Lee JI, Kim JW, Ki CS, Oh YL, Choi YL, Shin JH, Kim HK, Jang HW, Chung JH. BRAFV600E mutation analy-sis in fine-needle aspiration cytology specimens for evaluation of thyroid nodule: a large series in a BRAFV600E-prevalent population. J Clin Endocrinol Metab 2010;95:3693-3700. 9. Kwak JY, Kim EK, Kim JK, Han JH, Hong SW, Park TS, Choi
JR. Dual priming oligonucleotide-based multiplex PCR analy-sis for detection of BRAFV600E mutation in FNAB samples of thyroid nodules in BRAFV600E mutation-prevalent area. Head Neck 2010;32:490-498.
10. Yeo MK, Liang ZL, Oh T, Moon Y, An S, Kim MK, Kim KS, Shong M, Kim JM, Jo YS. Pyrosequencing cut-off value identi-fying BRAF(V600E) mutation in fine needle aspiration sam-ples of thyroid nodules. Clin Endocrinol (Oxf) 2011;75:555-560.
11. Lee HJ, Choi J, Hwang TS, Shong YK, Hong SJ, Gong G. Detection of BRAF mutations in thyroid nodules by allele-specific PCR using a dual priming oligonucleotide system. Am J Clin Pathol 2010;133:802-808.
12. Giulietti A, Overbergh L, Valckx D, Decallonne B, Bouillon R, Mathieu C. An overview of real-time quantitative PCR: ap-plications to quantify cytokine gene expression. Methods 2001;25:386-401.
13. Maciel BM, Dias JC, Romano CC, Sriranganathan N, Brendel M, Rezende RP. Detection of Salmonella Enteritidis in asymp-tomatic carrier animals: comparison of quantitative real-time PCR and bacteriological culture methods. Genet Mol Res 2011;10:2578-2588.
14. Sirichotiyakul S, Charoenkwan P, Sanguansermsri T. Prenatal diagnosis of homozygous alpha-thalassemia-1 by cell-free fetal DNA in maternal plasma. Prenat Diagn 2011.
15. Hamfjord J, Stangeland AM, Skrede ML, Tveit KM, Ikdahl T, Kure EH. Wobble-enhanced ARMS method for detection of KRAS and BRAF mutations. Diagn Mol Pathol 2011;20:158-165.
16. Halait H, Demartin K, Shah S, Soviero S, Langland R, Cheng S, Hillman G, Wu L, Lawrence HJ. Analytical performance of a real-time PCR-based assay for V600 mutations in the BRAF gene, used as the companion diagnostic test for the novel BRAF inhibitor vemurafenib in metastatic melanoma. Diagn Mol Pathol 2012;21:1-8.
17. Tonacchera M, Agretti P, Rago T, De Marco G, Niccolai F, Molinaro A, Scutari M, Candelieri A, Conforti D, Musmanno R, Di Coscio G, Basolo F, Iacconi P, Miccoli P, Pinchera A, Vitti P. Genetic Markers to Discriminate Benign and Malignant Thyroid Nodules with Undetermined Cytology in an Area of Borderline Iodine Deficiency. . J Endocrinol Invest 2011.
18. Kim EK, Park CS, Chung WY, Oh KK, Kim DI, Lee JT, Yoo HS. New sonographic criteria for recommending fine-needle aspiration biopsy of nonpalpable solid nodules of the thyroid. AJR Am J Roentgenol 2002;178:687-691.
19. Moon HJ, Kim EK, Chung WY, Choi JR, Yoon JH, Kwak JY. Diagnostic value of BRAF(V600E) mutation analysis of thy-roid nodules according to ultrasonographic features and the time of aspiration. Ann Surg Oncol 2011;18:792-799. 20. Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid
Cytopathology. Thyroid 2009;19:1159-1165.
21. Kim KH, Kang DW, Kim SH, Seong IO, Kang DY. Mutations of the BRAF gene in papillary thyroid carcinoma in a Korean population. Yonsei Med J 2004;45:818-821.
22. Fugazzola L, Puxeddu E, Avenia N, Romei C, Cirello V, Cavaliere A, Faviana P, Mannavola D, Moretti S, Rossi S, Sculli M, Bottici V, Beck-Peccoz P, Pacini F, Pinchera A, Santeusanio F, Elisei R. Correlation between B-RAFV600E mutation and clinico-pathologic parameters in papillary thy-roid carcinoma: data from a multicentric Italian study and re-view of the literature. Endocr Relat Cancer 2006;13:455-464. 23. Chung KW, Yang SK, Lee GK, Kim EY, Kwon S, Lee SH, Park
do J, Lee HS, Cho BY, Lee ES, Kim SW. Detection of BRAFV600E mutation on fine needle aspiration specimens of thyroid nodule refines cyto-pathology diagnosis, especially in BRAF600E mutation-prevalent area. Clin Endocrinol (Oxf) 2006;65:660-666.
24. Xing M, Tufano RP, Tufaro AP, Basaria S, Ewertz M, Rosenbaum E, Byrne PJ, Wang J, Sidransky D, Ladenson PW. Detection of BRAF mutation on fine needle aspiration biopsy specimens: a new diagnostic tool for papillary thyroid cancer. J Clin Endocrinol Metab 2004;89:2867-2872.
25. Nam SY, Han BK, Ko EY, Kang SS, Hahn SY, Hwang JY, Nam MY, Kim JW, Chung JH, Oh YL, Shin JH. BRAF V600E mu-tation analysis of thyroid nodules needle aspirates in relation to their ultrasongraphic classification: a potential guide for selec-tion of samples for molecular analysis. Thyroid 2010;20:273-279.
26. Rowe LR, Bentz BG, Bentz JS. Utility of BRAF V600E muta-tion detecmuta-tion in cytologically indeterminate thyroid nodules. Cytojournal 2006;3:10.
27. Kim SK, Kim DL, Han HS, Kim WS, Kim SJ, Moon WJ, Oh SY, Hwang TS. Pyrosequencing analysis for detection of a BRAFV600E mutation in an FNAB specimen of thyroid nod-ules. Diagn Mol Pathol 2008;17:118-125.
28. Nikiforov YE, Steward DL, Robinson-Smith TM, Haugen BR, Klopper JP, Zhu Z, Fagin JA, Falciglia M, Weber K, Nikiforova MN. Molecular testing for mutations in improving the fine-needle aspiration diagnosis of thyroid nodules. J Clin Endocrinol Metab 2009;94:2092-2098.
29. Jo YS, Huang S, Kim YJ, Lee IS, Kim SS, Kim JR, Oh T, Moon Y, An S, Ro HK, Kim JM, Shong M. Diagnostic value of pyro-sequencing for the BRAF V600E mutation in ultrasound-guid-ed fine-neultrasound-guid-edle aspiration biopsy samples of thyroid incidentalo-mas. Clin Endocrinol (Oxf) 2009;70:139-144.
30. Higuchi R, Fockler C, Dollinger G, Watson R. Kinetic PCR analysis: real-time monitoring of DNA amplification reactions. Biotechnology (N Y) 1993;11:1026-1030.
31. Gharib H, Goellner JR. Fine-needle aspiration biopsy of the thyroid: an appraisal. Ann Intern Med 1993;118:282-289. 32. Sapio MR, Guerra A, Posca D, Limone PP, Deandrea M,
Motta M, Troncone G, Caleo A, Vallefuoco P, Rossi G, Fenzi G, Vitale M. Combined analysis of galectin-3 and BRAFV600E improves the accuracy of fine-needle aspiration biopsy with cy-tological findings suspicious for papillary thyroid carcinoma. Endocr Relat Cancer 2007;14:1089-1097.