Accurate assignment of the evaluation and management (E&M) code for an office visit is challenging.1 The
E&M coding rules designed by the Health Care Financ-ing Administration (HCFA) have been described as un-necessarily complex and are currently in the process of redesign, in part because of the number of complaints about them.2 This complexity had led to the
publica-tion of coding aids such as the Pocket Guide to the
Documentation Guidelines published by the American
Academy of Family Physicians (AAFP).3 Many large
practices have tried to resolve the entire coding and compliance issue by hiring professional coders, thereby taking the decision away from clinicians.
The use of progress note templates that can aid in accurate coding may help return E&M coding decisions to clinicians while reducing improper coding. Although templates can improve the informational content and legibility of a note, it is not known if they can also help improve the accuracy of coding and billing. To evalu-ate the effect of a templevalu-ate on coding, we designed a template for a common office problem, the diagnosis
and treatment of group A beta-hemolytic streptococ-cus (GABHS) pharyngitis. We hypothesized that our template would increase thoroughness of documenta-tion and increase the accuracy of coding, compared with that achieved with standard progress note charting. This report presents the results of our implementation and analysis of this new tool in a family practice residency office setting.
Methods
Settings
The study practice site was the suburban Detroit fam-ily practice residency clinic of Wayne State University. Seven attending physicians and 12 resident physicians practice at the site. Our internal patient encounter data-base revealed that the average patient volume is 1,200 patients per month, and the average age of patients is 39.6 years.
The progress notes routinely used at that site were designed to facilitate recording of a full review of sys-tems, past medical-family-social history, and physical examination.4 The progress notes include check boxes
for all three of these contact areas, which can be marked as normal or can refer the reader to the handwritten note if further explanation is needed.
Use of a Template to Improve
Documentation and Coding
Edward A. Rose, MD, MSA; Arti M. Deshikachar, MD;
Kendra L. Schwartz, MD, MSPH; Richard K. Severson, PhD
Background and Objectives: Accurate assignment of evaluation and management (E&M) codes is a
challenge for physicians. Having guidelines close at hand during patient visits might improve appro-priateness and accuracy of E&M coding. We developed a template based on a clinical prediction rule for group A beta-hemolytic streptococcal (GABHS) pharyngitis to improve documentation and coding decisions. Methods: Fifty office visits for sore throat were documented using templates and were com-pared with 50 sore throat visits that were documented using progress notes. We counted history and physical examination items and compared the level of service charged to the level of service supported by the note. Results: Significantly more history of present illness and physical examination items were recorded on templates. Decisions related to treatment for patients with a low probability of GABHS were also improved by the templates. Templates had no effect on billing and coding errors. Conclusions: The template resulted in more-thorough documentation but had no effect on coding and billing errors rela-tive to progress notes.
(Fam Med 2001;33(7):516-21.)
Instrument
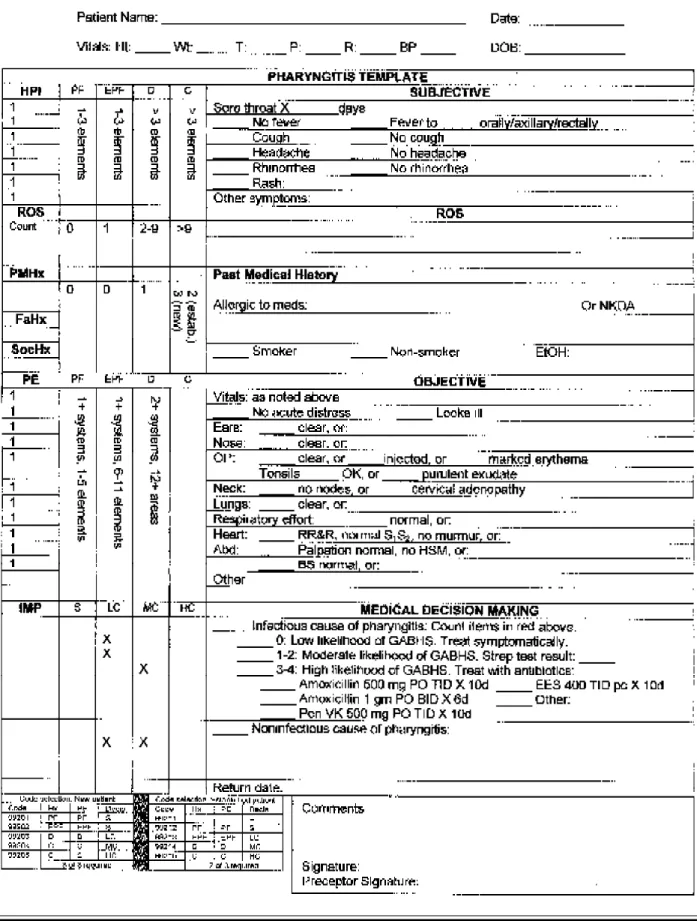
We designed a progress note template to use with patients who have signs and symptoms of GABHS phar-yngitis. The template was based on published algo-rithms that classify the relative probability of a GABHS diagnosis into three levels: low, moderate, and high.5-7
The indicators included on our template were fever, absence of cough, cervical adenopathy, and severe pha-ryngeal erythema. The template also prompted the cli-nician to add up items recorded in each section of the note, assisted in the assessment of complexity of medi-cal decision making, and then brought these factors together to arrive at an appropriate E&M code. The tem-plate is shown in Figure 1.
Procedures
The template was used with 50 patients who pre-sented with a complaint of sore throat between July 1 and October 31, 1999. The study procedure was as fol-lows. The medical assistant who performed the intake assessment identified patients with a sore throat com-plaint, placed the template on the chart, and recorded that patient’s name and the date on a log sheet. No other progress note form was placed on the chart. If the phy-sician concluded that the visit was more complex than a sore throat (for example, the patient had a comorbid condition that required additional documentation), the template was removed by the medical assistant and re-placed with a standard progress note form, and these visits were excluded from study.
Since the template may have had an educational ef-fect on physician behavior, we selected a comparison group from visits that predated the template study pe-riod. The comparison group was comprised of visits of patients with a diagnosis of pharyngitis who were seen in the 6-month period just prior to the intervention. The comparison group consisted of 50 patients who were selected from the list of 121 eligible patients by pull-ing the chart of every other patient on the list up to a total of 50. These 50 records were examined in a simi-lar fashion.
To ensure blinding of the 50 pre-intervention and 50 post-intervention records so that our reviewers would not know the visit was coded, we used the following procedure. A list of 100 random numbers between 1 and 1,000 was generated, and progress notes and tem-plates were assigned a code number. The code number was then written on the study copy of the progress note or template, along with the age and gender of the pa-tient, whether the patient was new to the practice or established, and the level of service charged. Specifi-cally excluded were the patient name, the date of ser-vice, and the name of the physician who saw the pa-tient. A medical assistant maintained a log sheet match-ing patient names and visit information to the assigned code number.
One of the authors then extracted information from each of the 100 progress notes and templates onto a blank template. Another author reviewed the notes and extracts, and differences between the two reviewers were resolved by consensus. The code number was entered in place of the patient’s name, along with whether the patient was new or established as well as the gender and date of birth. The extracts were arranged in numerical order for review. Each coded extract was then analyzed, as designed below.
Data Analysis
The following variables were entered into a database: patient age and gender; the number of elements listed for history of present illness, review of systems, past medical, family, and social history, and for physical ex-amination; the diagnosis, including the likelihood of GABHS; whether a rapid strep screen was indicated; whether or not a strep screen was performed; the re-sults of the strep screen; whether antibiotics were indi-cated; whether antibiotics were given; name of antibi-otic given; and whether or not a first-line antibiantibi-otic was used. Finally, the note was assigned a level of service based on completeness of the note and complexity of the case according to coding guidelines published by the AAFP.3
After all variables were entered into a database, the code was broken to allow identification of patient vis-its recorded on templates versus progress notes and the level of service charged. Differences between the tem-plate and progress notes groups in the means of con-tinuous value variables (such as the number of physi-cal exam items) were assessed by an unpaired t test assuming unequal variances.8 Differences between the
template and progress notes groups in the proportions of categorical variables (such as whether or not a rapid strep test was done) were assessed by a test for a differ-ence in proportions.8 Decision-making results were
compared using chi-square analysis. Results
Of the original 100 chart notes, 96 were included in the analysis. Four of the original (pre-intervention) progress notes were illegible, while all of the templates were legible, resulting in 46 progress notes and 50 tem-plates for inclusion in the database. The average age of all patients in the study was 31.0 (SD=4.6) years. Twenty-nine (58.0%) of the template patients were fe-male, compared with 28 (60.8%) of the progress note patients. Template patients tended to be somewhat older than progress note patients (average age 32.8 versus 27.6, respectively; P<.05).
Documentation
Documentation of history and physical findings is shown in Table 1. Given the differences in age groups
Figure 1 The Study Template
between the template patients and the progress note patients, we stratified by age in our evaluation of thorough-ness of documentation. Analysis of the pooled data revealed that, com-pared to progress notes, templates had more history of present illness items (5.3 versus 4.3; P<.001), more past medical-family-social history items (1.8 versus 1.4; P=.012), and more physical exam items (10.5 versus 6.9;
P<.001). There were more
review-of-systems items recorded on the progress notes (4.1 versus 1.1;
P<.001) than on the templates. All of
these differences between templates and progress notes remained statisti-cally significant when restricted to those patients less than age 30. How-ever, when considering those patients
age 30 and older, only the review-of-systems items and the physical examination items were significantly dif-ferent (P<.05).
Diagnosis and Treatment
If a patient was assessed as having a high probabil-ity for GABHS, the clinician would not be expected to run a rapid strep test but, instead, proceed directly to treatment. As seen in Table 2, none of the high prob-ability progress note patients received a rapid strep test, whereas 50% of similar template patients underwent rapid strep testing.
Moderate likelihood patients should have a strep test performed and, if positive, should receive antibiotics. If the test was not done or was negative, antibiotics were
most likely not indicated. In the current study, com-parison of templates to progress notes revealed no sig-nificant difference in the frequency of use of the rapid strep test (44.0% versus 34.1%, respectively; P=.319) or use of antibiotics in the absence of an adequate indi-cation (44.0% versus 54.3%, respectively; P=.432).
When the template indicated a low likelihood of GABHS, rapid strep testing is not recommended and antibiotics would only be indicated if there was a comorbidity. While in our study sample there were no rapid strep tests run in such patients from either group, significantly fewer low likelihood template patients received antibiotics (10.0% versus 71.4%; P<.05), com-pared with progress note patients.
Table 1
Average Counts of Documentation Items, Progress Notes Versus Templates, by Age of Patient
TEMPLATES PROGRESS NOTES
Patients Patients All Patients Patients All # of <30 30 Patients <30 30 Patients items in: (n=23) (n=27) (n=50) (n=26) (n=20) (n=46) HPI 5.3 5.3 5.3 4.0 4.7 4.3 ROS .8 1.3 1.8 4.2 4.1 4.1 PMFSHx 1.8 1.8 1.8 1.2 1.5 1.4 PE 11.0 10.0 10.5 6.8 7.0 6.9
HPI—history of present illness ROS—review of systems
PMFSHx—past medical, family, and social history PE—physical examination
Table 2
Evaluation and Treatment Decisions, Progress Notes Versus Templates,
by Likelihood Estimate of GABHS Disease, Excluding Noninfectious Causes of Pharyngitis
TEMPLATES PROGRESS NOTES
High Moderate Low High Moderate Low
Probability Probability Probability Probability Probability Probability (n=10)* (n=25)** (n=10)*** (n= 4)* (n=35)** (n=7)***
Rapid strep done 50% 44% 0% 0% 31% 0%
Antibiotics not indicated (Antibiotics (Antibiotics
but given indicated) 44% 10% indicated) 54% 71%
Antibiotics indicated (Antibiotics (Antibiotics
but not given 10% 0% not indicated) 0% 0% not indicated)
* Rapid strep not indicated; antibiotics indicated ** Rapid strep indicated; antibiotics indicated if positive ***Rapid strep not indicated; antibiotics not indicated
Coding
Comparing templates to progress notes, there were no statistically significant differences (54.0% versus 34.8%, respectively; P=.059) in overall accuracy of coding (that is, the documentation matched the visit code). Similarly, there was no difference in the amount of undercoding (34.0% versus 41.3%, respectively) or overcoding (10.0% versus 21.7%, respectively). The number of other errors (namely, new patient billed as established patient or established patient billed as new patient) was also similar for both groups.
Discussion
For patients age 30 and under, this study showed that the templates increased the number of historical items recorded for history of present illness and for past, fam-ily, and social history. In addition, more physical ex-amination findings were recorded on the templates for both younger and older patients. Despite the differences in documentation between the template and progress note groups, however, there was no difference in cod-ing accuracy. Because the template facilitated the enu-meration of E&M elements and included information on proper assignment of a level of service code, it was expected that it would improve coding accuracy. This was not found to be the case.
As an aid in medical decision making, the templates showed some promise. Significantly fewer patients with a low likelihood of GABHS received antibiotics inap-propriately. There was no difference in inappropriate testing for GABHS or in the use of first-line antibiotics when comparing the templates to progress notes.
While the templates facilitated documentation gen-erally, it is not clear that documenting more items cor-relates with improved quality of care or better outcomes. Given the complexities of billing compliance, sufficient numbers of history and physical examination items must be recorded to support the level of service being charged. Yet, it is not clear that there is a strong corre-lation between quality of care and the length of an of-fice note. The two issues, quality of care and billing compliance, are separate and distinct. This template was designed to assist in both, but primarily the latter, and seems to have succeeded in some ways but not in oth-ers. The template design limited the amount of space that clinicians had to record review of systems, explain-ing the higher number of review-of-systems items re-corded on the progress notes. This may need to be ex-amined in a revision of the template.
The reasons why the template did not improve cod-ing accuracy are not clear. Since the template was de-signed to be self-explanatory, we did not provide any training to clinicians on how to use the form. A brief workshop or an explanatory instruction sheet may have augmented the template’s effectiveness but then it would be difficult to tell whether coding improved because of
the template or the educational intervention. A follow-up study comparing progress notes to templates, with or without additional instruction for both formats of documentation, might be helpful to answer such a question.
Reported experience with templates has been mostly positive. Template proformas have been associated with improved informational content in histopathology9,10
and laboratory reports11 both in content and quality. In
a study by Marill et al,12 a template-based medical
docu-mentation system was introduced in a county hospital emergency department. Physicians preferred the sys-tem and generated higher billings, although the syssys-tem did not save clinical time.
In addition to improving documentation, templates can also be used to improve the quality of care accord-ing to evidence-based medicine tenets. Panagiotou13 et
al have described an evidence-based well-baby record that was designed to increase the effectiveness of pri-mary care physicians who provide well-child care. While many clinicians may make evidence-based de-cisions that are supported by the medical literature with-out written prompts,14 we attempted to develop a
mecha-nism to make such decisions easier by providing the pertinent clinical prediction rules directly to our busy practitioners.
Limitations
This study has several limitations. The first is its small sample size, making generalizability difficult. Second, while the single-blind study design helps reduce bias, the auditors performing the conversion of information from the progress notes to a blank template were re-quired to do some subjective interpretation of progress note items to make them “fit” into the template. Fi-nally, our assessments of the appropriate E&M code that was supported by the note may be subject to inter-pretation, since audits of notes for E&M coding are often quite subjective.15
Conclusions
Given the challenges associated with the diagnosis and treatment of GABHS16,17 and the high frequency of
this disease,18 the template-based approach described
herein has the potential to improve the quality of medi-cal decisions while reducing costs. Even well-con-structed clinical guidelines are unlikely to succeed if they are not readily available to the clinician.19 Our
tem-plate was designed to facilitate documentation to im-prove E&M coding and has the potential to facilitate appropriate decision-making. These are issues impor-tant not only to physicians in training but physicians in practice as well.
Future study should investigate not only application of this template to a larger number of patients in a vari-ety of settings but also development of similar templates
for other conditions, as well as supporting documenta-tion and training in the use of the templates. If further refinements and training improve the performance of templates similar to the one presented in the current study, such templates could be easily incorporated into electronic medical record systems.20 As the body of
evidence-based medicine literature continues to grow, the clinical prediction rules should evolve that can be incorporated into such templates.
Acknowledgments: Financial support for this study was received from the
Southeast Michigan Academy of Family Practice Research Grants Program. This paper was presented at the March 2000 Wayne State University De-partment of Family Medicine Research Day Forum in Detroit.
We thank Victoria Neale, MD, for her editorial assistance on the manuscript.
Corresponding Author: Address correspondence to Dr Rose, Wayne State
University, Department of Family Medicine, 15400 West McNichols Drive, Detroit, MI 48235. 313-493-6425. Fax: 313-493-9387. [email protected].
REFERENCES
1. Rose EA, Roth LR, Werner PT, Keshwani A, Vallabhaneni V. Using faculty development to solve a problem of evaluation and management coding: a case study. Acad Med 2000;75:323-30.
2. Cohen JJ, Dickler RM. Auditing the Medicare billing practices of teach-ing physicians—welcome accountability, unfair approach. N Engl J Med 1997;336:1317-20.
3. American Academy of Family Physicians. Pocket guide to the docu-mentation guidelines. Kansas City, Mo: American Academy of Family Physicians, 1998.
4. Moore K. More help with exam documentation. Fam Pract Manag 1997; 4:63-75.
5. Sloane P, Slatt L, Curtis P, Ebell M. Essentials of family medicine. Baltimore: Williams & Wilkins, 1998.
6. Centor R, Witherspoon J, Dalton H, Brody C, Link K. The diagnosis of strep throat in adults in the emergency room. Med Decis Making 1981; 1:239-46.
7. Walsh B, Bookheim W, Johnson R, Tompkins R. Recognition of strep-tococcal pharyngitis in adults. Arch Intern Med 1975;135:1493-7. 8. Armitage P. Statistical methods in medical research. Oxford, UK:
Blackwell Scientific Publications, 1971.
9. Bull AD, Biffin AH, Mella J, et al. Colorectal cancer pathology report-ing: a regional audit. J Clin Pathol 1997;50:138-42.
10. Cross SS, Feeley KM, Angel CA. The effect of four interventions on the informational content of histopathology reports of resected colorectal carcinomas. J Clin Pathol 1998;51:481-2.
11. Thilagarajah R, Vale JA, Witherow RO, Walker MM. A clinicopatho-logical approach to cystitis—recommendations for simplified pathol-ogy reporting. Br J Urol 1997;79:567-71.
12. Marill KA, Gauharou ES, Nelson BK, Peterson MA, Curtis RL, Gonzalez MR. Prospective, randomized trial of template-assisted ver-sus undirected written recording of physician records in the emergency department. Ann Emerg Med 1999;33:500-9.
13. Panagiotou L, Rourke LL, Rourke JT, Wakefield JG, Winfield D. Evi-dence-based well-baby care. Part 2: Education and advice section of the next generation of the Rourke Baby Record. Can Fam Physician 1998;44:568-72.
14. Michaud G, McGowan JL, van der Jagt R, Wells G, Tugwell P. Are therapeutic decisions supported by evidence from health care research? Arch Intern Med 1998;158:1665-8.
15. Lawler FH, Purvis JR, Paris JA, Horner RD. The effect of faculty pri-vate practice experience on appropriate charging for professional ser-vices. Fam Med 1990;22(6):487-9.
16. de Silva KS, Gunatunga MW, Perera AJ, Jayamaha DJ. Can group A beta haemolytic streptococcal sore throats be identified clinically? Ceylon Med J 1998;43:196-9.
17. McIsaac WJ, Goel V, Slaughter PM, et al. Reconsidering sore throats. Part I: Problems with current clinical practice [see comments]. Can Fam Physician 1997;43:485-93.
18. Woods WA, Carter CT, Stack M, Connors AF, Jr, Schlager TA. Group A streptococcal pharyngitis in adults 30 to 65 years of age. South Med J 1999;92:491-2.
19. O’Connor PJ, Amundson G, Christianson J. Performance failure of an evidence-based upper respiratory infection clinical guideline [see com-ments]. J Fam Pract 1999;48:690-7.
20. Sujansky WV. The benefits and challenges of an electronic medical record: much more than a “word-processed” patient chart. West J Med 1998;169:176-83.