FACTORS THAT INFLUENCE COMMUNITY PHARMACY ADOPTION OF TYPE 2 DIABETES PREVENTION PROGRAMS
Sara E. Roszak
A dissertation submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Public Health in the Department of Health Policy and Management of the Gillings School of Global Public
Health.
Chapel Hill 2019
ABSTRACT
Sara E. Roszak: Factors that Influence Community Pharmacy Adoption of Type 2 Diabetes Prevention Programs
(Under the direction of Rebecca Slifkin)
Diabetes imposes a significant societal and public health burden — more than 100 million Americans live with diabetes (30.3 million) or prediabetes (84.1 million). Developing type 2 diabetes is a gradual, but preventable process. While many strategies exist to address prediabetes, the Center for Disease Control and Prevention’s National Diabetes Prevention Program is the largest, evidence-based effort to deliver a lifestyle change program to communities across the United States.
As public health stakeholders look to lessen the burden of diabetes, ensuring that prevention programs are high quality and adequately utilized is important. One opportunity for partnership is with pharmacies. Pharmacists are medication experts whose traditional role has expanded to include delivery of patient care services. Many pharmacies offer walk-in services and hours that typically extend beyond that of physician offices into nights and weekends.
Most study participants said their company currently offers diabetes prevention programs, while the rest had previously offered such programs or had never offered them. The principal investigator identified the following findings: (1) Financial feasibility and sustainable reimbursement models are critical for adoption of diabetes prevention programs, with grant funding a catalyst most commonly utilized by independent pharmacies and
grocery stores with pharmacies; (2) Inadequate consumer participation in diabetes prevention programs is problematic, but pharmacies are committed to solving this issue; (3) Operational fit is important and appropriate use of non-pharmacists is essential to adoption and success of diabetes prevention programs; (4) Customer loyalty is a top advantage gained by pharmacy adopters of diabetes prevention programs, but specific characteristics of grocery stores that made delivery of those programs easier was an advantage not seen in other settings; and (5) Pharmacies are focused on expanding healthcare access to at-risk populations and
To Andy:
For being my biggest supporter, champion, and true love. To my parents and grandparents:
ACKNOWLEDGEMENTS
I wish to acknowledge my committee members for their guidance, wisdom, and expertise. I have benefited greatly from these accomplished women who so generously joined my efforts:
• Dr. Rebecca Slifkin, for her outstanding leadership — challenging and supporting me through each milestone;
• Dr. Sandra Greene, for her advice and direction — shaping my experience in the DrPH program for the better;
• Dr. Leah Devlin, for her insightful contributions and public health expertise; • Dr. Stefanie Ferreri, for her encouragement and passion to advance innovative
community pharmacy practice; and
• Dr. Lisa M. Koonin, for planting the seed to pursue a DrPH program years ago and her unwavering belief that I would succeed.
I enjoyed learning alongside my classmates from Cohort 12 and am grateful for their
TABLE OF CONTENTS
LIST OF TABLES ... ix
LIST OF FIGURES ...x
LIST OF ABBREVIATIONS ... xi
CHAPTER 1: THE TOPIC...1
Background ... 1
Lifestyle Change and the National Diabetes Prevention Program (National DPP) ... 5
The Potential Role of Pharmacy in Diabetes Prevention ... 13
Conceptual Framework ... 18
Research Question and Aims ... 22
Research Interest ... 24
CHAPTER 2: LITERATURE REVIEW ...25
Methods... 25
Results ... 27
Discussion ... 36
CHAPTER 3: METHODOLOGY ...40
Study Design and Methodology ... 40
IRB and Protection of Human Subjects ... 41
Sample Size and Eligible Participants ... 41
Participant Identification ... 42
Data Collection ... 45
Data Analysis ... 46
CHAPTER 4: RESULTS ...49
Key Findings and Major Themes ... 52
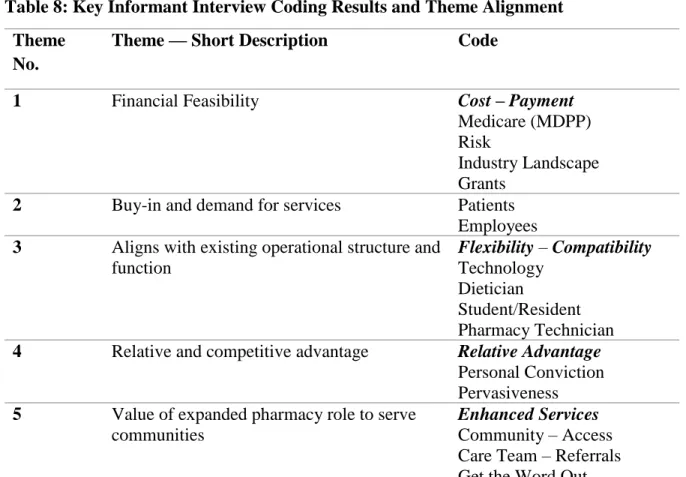
Theme 1: Financial Feasibility ... 54
Theme 2: Buy-in and demand for services... 61
Theme 5: Value of expanded pharmacy role to serve communities ... 79
CHAPTER 5: DISCUSSION ...83
Finding #1 ... 84
Finding #2 ... 88
Finding #3 ... 89
Finding #4 ... 91
Finding #5 ... 92
CHAPTER 6: PLAN FOR CHANGE ...95
Background ... 95
Change Framework ... 95
Applied Leadership Principles ... 97
Spreading the Innovation through Pharmacy ... 100
Initiation of Plan (Completed)... 100
Implementation: Future Action Needed ... 102
Strengths and Limitations of Plan for Change ... 111
APPENDIX A: DIABETES PREVENTION RECOGNITION PROGRAM PROCESS ...113
APPENDIX B: CONCEPTUAL MODEL ...115
APPENDIX C: LIST OF STUDIES INCLUDED IN LITERATURE SEARCH ONE ...116
APPENDIX D: LIST OF STUDIES INCLUDED IN LITERATURE SEARCH TWO ...120
APPENDIX E: RECRUITMENT EMAIL FOR KEY INFORMANT INTERVIEW PARTICIPANTS ...121
APPENDIX F: REMINDER EMAIL FOR KEY INFORMANT INTERVIEW PARTICIPANTS ...123
APPENDIX G: KEY INFORMANT INTERVIEW GUIDE ...124
LIST OF TABLES
Table 1: Identifying Diabetes and Learning about Prediabetes ...4
Table 2: Payer Coverage of the National DPP Lifestyle Change Program ...11
Table 3: Defining Innovation Characteristics in the Context of Diabetes Prevention ...21
Table 4: Summary of Research Data Collection Methods and Tool ...40
Table 5: Tenure of Service for Participants at Pharmacy or Company by Range of Years Served...49
Table 6: Participants’ Company Experience with Diabetes Screening for Prevention by Type of Pharmacy ...50
Table 7: Participants’ Company Experience with Delivery of Diabetes Prevention Lifestyle Change Programs by Type of Pharmacy ...52
Table 8: Key Informant Interview Coding Results and Theme Alignment ...53
Table 9: Major Themes Identified from Key Informant Interviews ...54
Table 10: Significant Findings for Discussion that Correlate to Themes ...84
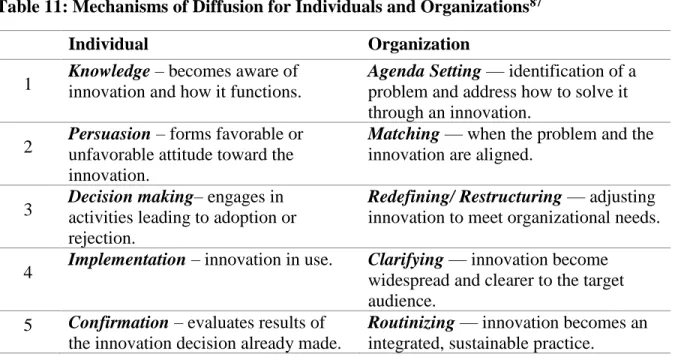
Table 11: Mechanisms of Diffusion for Individuals and Organizations ...97
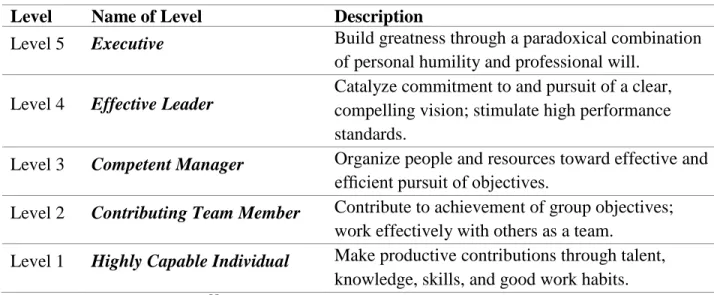
Table 12: Hierarchy of Leadership Capabilities ...98
Table 13: Concepts with Level 5 Leaders and Application to Plan for Change ...99
LIST OF FIGURES
Figure 1: Conceptual model for this dissertation adapted from Frambach
LIST OF ABBREVIATIONS
A1C Glycated Hemoglobin
AADE American Association of Diabetes Educators ACA Patient Protection and Affordable Care Act of 2010
ACO Accountable Care Organization
ADA American Diabetes Association
APhA American Pharmacists Association
APHA American Public Health Association
ASTHO Association of State and Territorial Health Officials
BMI Body Mass Index
CDC Centers for Disease Control and Prevention CLIA Clinical Laboratory Improvement Amendments CMMI Center for Medicare & Medicaid Innovation CMS Centers for Medicare and Medicaid Services
CBSA Core Based Statistical Area
CPA Collaborative Practice Agreement
DPP Diabetes Prevention Program
DPP GLB Diabetes Prevention Program Group Lifestyle Balance DPRP Diabetes Prevention Recognition Program
FPG Fasting Plasma Glucose
GAS Group A Streptococcus
JCCP Joint Commission of Pharmacy Practitioners
MDPP Medicare Diabetes Prevention Program
MTM Medication Therapy Management
NCPA National Community Pharmacists Association NCSL National Conference of State Legislatures
NGA National Governors Association
NACCHO National Association of County and City Health Officials NACDS National Association of Chain Drug Stores
National DPP National Diabetes Prevention Program
NIH National Institutes of Health
PFS Physician Fee Schedule
PGT Plasma Glucose Test
PharmD Doctor of Pharmacy
PPPY Per Patient Per Year
QALD Quality Adjusted Life Day
QUALY Quality Adjusted Life Year
RDN Registered Dietician Nutritionist
ROI Return on Investment
SSA U.S. Social Security Act (1935)
TB Tuberculosis
U.S. United States of America
USPSTF U.S. Preventive Services Task Force
YMCA Young Men’s Christian Association
CHAPTER 1: THE TOPIC Background
In recent decades, total health expenditures in the United States (U.S.) have increased substantially while the population progressively has become older and sicker. Healthcare spending accounts for 17.8 percent of the U.S. economy, reaching $3.2 trillion in 2015.1 By 2050, experts project the population aged 65 and older will reach 83.7 million, almost double its size in 2012.2 Further, 171 million people are projected to have multiple chronic
conditions by 2030, up from 141 million in 2010.3 One of these chronic conditions is diabetes, which the Centers for Disease Control and Prevention (CDC) classified as the seventh leading cause of death in the U.S., but a 2017 study argued diabetes is third, behind only heart disease and cancer.4–6
Given the existing physician shortage, other healthcare personnel are needed to address diabetes and other chronic diseases. Demand for physicians continues to outpace supply,7 and experts expect by 2025 the shortfall of physicians in the U.S. will be between 46,100 and 90,400, with a primary care shortage of 12,500 to 31,100.7 The shortage in the healthcare workforce is more staggering in context of support needed to prevent and delay diabetes and other chronic diseases.
Diabetes in America
Diabetes imposes a significant societal and public health burden — more than 100 million Americans (9.4 percent of the population) — live with diabetes (30.3 million) or prediabetes (84.1 million).8 The majority of people living with diabetes worldwide have type 2 diabetes, while approximately 5 percent have type 1. In type 2 diabetes, the body does not use insulin properly; in type 1 diabetes, the body produces little or no insulin.9,10 Although the number of diabetes cases is still increasing, the rate of growth is slowing. The CDC estimated 1.5 million new cases of diabetes among adults in 2015. Rates of newly-diagnosed diabetes increase with age of the population.8
Diabetes is a serious disease; while type 1 diabetes is not preventable, many people with can prevent or delay type 2 diabetes onset with lifestyle changes.9 Type 2 diabetes can often be managed through physical activity, diet, and appropriate use of insulin and other medications to control blood sugar levels.6 People with type 2 diabetes are at increased risk of health complications such as premature death, vision loss, heart disease, stroke, kidney failure, and amputation.6 In addition to being a public health burden, diabetes management is expensive.
According to a 2012 study led by the American Diabetes Association (ADA), the direct and indirect estimated cost of diagnosed diabetes is $245 billion.11 The study measured the economic burden of diabetes in terms of health resource use and lost productivity,
Prediabetes
Developing type 2 diabetes is a gradual process, and the concept of preventing diabetes or living with prediabetes is only related to type 2. For people with prediabetes, reducing bodyweight and exercising moderately can prevent or delay onset of diabetes, returning blood glucose to normal levels.12 According to the CDC, risk factors for
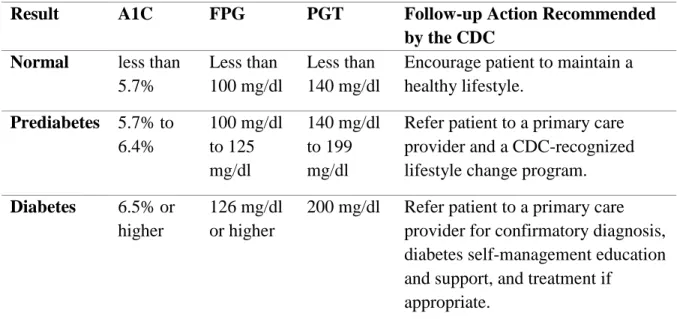
prediabetes include being overweight; age 45 years or older; having a parent, brother or sister with type 2 diabetes; being physically active less than three times a week; and for women, having gestational diabetes or giving birth to a baby weighing more than nine pounds or having polycystic ovary syndrome.13 Several types of diagnostic tests are used to detect increased levels of blood glucose, which can indicate the presence of prediabetes or diabetes (Table 1). A pharmacy may offer a customer a finger stick test for blood glucose levels, or, in a state that permits use of the A1C test, a pharmacy may offer the A1C provided its
location(s) offering this service has a Certificate of Waiver to the Clinical Laboratory Improvement Amendments (CLIA). Some doctors’ offices have a laboratory and phlebotomist on-site to offer any blood glucose tests.
The A1C test measures average blood glucose for the past 2 to 3 months. The Fasting Plasma Glucose (FPG) test checks blood glucose levels after someone has fasted for 8 hours, and the Plasma Glucose Test (PGT) measures glucose 2 hours after administration of a 75gm glucose load.12 If a patient presents at a pharmacy and has already received a diagnostic test from their physician, the pharmacist can request a copy of the test results from the
blood glucose test is offered at any healthcare destination, pharmacists and other members of the care coordination team can send or receive the relevant patient data to or from one another.
Table 1: Identifying Diabetes and Learning about Prediabetes12,14
Result A1C FPG PGT Follow-up Action Recommended
by the CDC Normal less than
5.7%
Less than 100 mg/dl
Less than 140 mg/dl
Encourage patient to maintain a healthy lifestyle.
Prediabetes 5.7% to 6.4% 100 mg/dl to 125 mg/dl 140 mg/dl to 199 mg/dl
Refer patient to a primary care provider and a CDC-recognized lifestyle change program. Diabetes 6.5% or
higher
126 mg/dl or higher
200 mg/dl Refer patient to a primary care provider for confirmatory diagnosis, diabetes self-management education and support, and treatment if
appropriate.
* FPG requirement for Medicare Diabetes Prevention Program suppliers is 110–125 mg/dL. ** Based on Table 1 in Rx for the National Diabetes Prevention Program: Action Guide for
Community Pharmacists.14
prediabetes who lose weight through healthy eating and exercise can cut their risk of getting type 2 diabetes in half.15 Lifestyle change is the most effective method to prevent diabetes.
In 2008, the ADA began recommending the drug metformin for some instances of prediabetes, including people with a Body Mass Index (BMI) of 35 or higher and women with a history of gestational diabetes. Then, the ADA expanded the recommendation to include considering metformin for people with prediabetes who have an A1C level between 5.7 percent and 6.4 percent.16 Metformin may be underutilized for management of
prediabetes;17,18 however, pharmaceutical interventions are not the focus of this study. Lifestyle Change and the National Diabetes Prevention Program (National DPP)
Since the release of the first report in 1979, Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention, the Healthy People initiative has been
spearheaded by the U.S. Department of Health and Human Services (HHS) and has evolved into a multi-year process with input from diverse stakeholders to identify nationwide health improvement priorities, increase public awareness, and measure progress.19
HHS accepted public comment for the Healthy People 2030 proposed framework through January 17, 2019. The proposed framework includes nine core objectives relates to diabetes, with the following most relevant to this study:20
• Reduce the annual number of new cases of diagnosed diabetes in the population;
• Reduce the proportion of adults with diagnosed diabetes with an A1C value greater than 9 percent; and
Healthy People 2020 goals called for a 10 percent reduction in the number of diabetics ages 18 to 84. To meet these goals, substantial interventions are needed on a national scale. Reviews by the U.S. Preventive Services Task Force (USPSTF) and their Guide to Community Preventive Services (the Community Guide) from 2012 to 2016 have supported the notion that lifestyle change is an effective way to prevent development of type 2 diabetes. The USPSTF released the following evidence-based recommendation urging clinicians to screen for abnormal blood glucose “as part of cardiovascular risk assessment in adults aged 40 to 70 years who are overweight or obese. Clinicians should offer or refer patients with abnormal blood glucose to intensive behavioral counseling interventions to promote a healthful diet and physical activity.”21 The recommendation to refer people who have signs of prediabetes into lifestyle change programs is based on findings from a 2015 systematic literature review that updated the 2008 USPSTF review on diabetes screening for adults.22 Offering the National DPP lifestyle change program is one way to fulfill that recommendation.
with prediabetes in the U.S. The CDC’s strategic approach to the National DPP includes four core elements:
• Train the workforce that can implement the program cost effectively;
• Implement a recognition program that will: assure quality, lead to reimbursement, and allow the CDC to develop a program registry;
• Develop intervention sites that will build infrastructure for the program; and • Increase referrals to and use of the prevention program.
The National DPP lifestyle change program is offered in-person, online, and via distance learning, or a combination, by a trained lifestyle coach who encourages participants to meet health goals and stay motivated. Retaining participants for the full year curriculum is essential to ingrain new habits into participants’ daily routines and reduce their risk for type 2 diabetes. The average cost to participate in the National DPP lifestyle change program is $500 per participant, far less than the average cost to manage diabetes.24 These are the defining characteristics of the National DPP lifestyle change programs:14
• One-year group program (offered in-person, online, via distance learning or a combination) and consisting of:
o An initial 6-month phase with at least 16 weekly sessions offered over a period of 16 to 24 weeks; and
o A second 6-month phase with at least 1 session a month (minimum of 6 sessions).
• Focuses on behavior change to improve healthy eating, increase physical activity, and manage stress; and
• Provides peer support.
The CDC-approved National DPP lifestyle change curriculum can be offered by programs that meet a certain quality standard defined by the CDC’s Diabetes Prevention Recognition Program (DPRP) process and can range from pre-application to pending to preliminary to full recognition status (Appendix A). A program with full recognition status must demonstrate body weight documentation in 80 percent of their sessions, physical activity documentation at 60 percent of their sessions, participant weight loss of an average of 5 percent body weight over 12 months, and participant eligibility with 35 percent entering the program after blood glucose test indicates prediabetes or a history of gestational diabetes. Additionally, full recognition programs must meet all requirements for pending and
preliminary programs, including participant retention requirements and data collection requirements (e.g. provide data that at least 60 percent of participants attended at least nine sessions in months one to six and at least 60 percent attended at least three sessions in months seven to 12. In March 2018, the CDC’s publicly available registry noted 1693 locations as DPRP pending, preliminary or full recognition. Notably, over the last nine years since the program’s authorization by Congress, less than 1 percent of those whom could benefit from the program had enrolled (as of October 1, 2018, fewer than 250,000 had enrolled).
months to one year to encourage lifestyle change (these programs also included additional maintenance phase to prevent relapse).25 These studies — including the DPP led by the National Institutes of Health (NIH) — influenced the creation of the National DPP.
The initial DPP trial began enrolling patients in 1996.26 The researchers randomly assigned 3234 non-diabetic individuals with elevated fasting and post-load plasma glucose concentrations to the following groups: (1) placebo, (2) metformin (850 mg twice daily), or (3) lifestyle-modification program with the goal of at least 7 percent weight loss and at least 150 minutes of physical activity per week. The average follow-up was 2.8 years; the
researchers found that participants in the lifestyle-modification program reduced their risk of developing diabetes by 58 percent (71 percent reduction for those aged 60 and older) and participants in the metformin group reduced their risk by 31 percent as compared to the placebo group.27 Further, only 5 percent of the lifestyle change group developed diabetes as compared to 11 percent in the placebo group.27 A subsequent, related study that followed the same cohort for a full 10 years after the DPP intervention concluded that cumulative
incidence by either lifestyle change or metformin therapy persisted for at least 10 years.26 After 10 years, individuals who were in the lifestyle-modification program group of the DPP trial were 33 percent less likely to develop diabetes.26 As a result of these promising DPP findings from communities across the U.S., the CDC endeavored to develop an evidence-based, low cost intervention to move diabetes prevention from research to implementation.25 Coverage of the National DPP Lifestyle Change Program
DPP lifestyle change program is growing (Table 2). Expanding coverage of the program is an important step to more readily reach eligible participants and reduce financial burdens for recipients and suppliers of the program.
The CDC has funded health departments in all states and the District of Columbia to partner with Medicaid sister agencies to advocate for coverage. Further, nine states have full or partial coverage of the National DPP lifestyle change program through Medicaid
Table 2: Payer Coverage of the National DPP Lifestyle Change Program23 COMMERCIAL INSURERS
Many commercial health plans provide some coverage for the National DPP lifestyle change program.
• AmeriHealth
• Anthem
• BCBS Florida
• BS California
• BCBS Louisiana
• Cigna
• Denver Health Managed Care: Medicaid, Medicare, Public Employees
• Emblem Health: NY
• GEHA
• Highmark
• Humana
• Kaiser: CO & GA
• LA Care: Medicaid
• MVP’s Medicare Advantage
• Priority Health: MI
• United Health Care (national, state, local, private and public employees)
U.S. GOVERNMENT The Centers for Medicare and Medicaid issued a final rule that allows for coverage of the National DPP lifestyle change program on a pay-for-performance basis.
• Medicare (April 2018) • Medicaid
STATE COVERAGE Over 3.4 million public
employees/dependents in 19 states have the National DPP as a covered benefit. Demonstration projects ongoing in North Dakota, Pennsylvania, and Utah.
• California
• Colorado
• Connecticut (DoT workers)
• Delaware
• Georgia (Kaiser Permanente)
• Indiana
• Kentucky
• Louisiana
• Maine
• Maryland (partial payment)
• Minnesota
• New Hampshire
• New York
• Oregon (educators)
• Rhode Island
• Tennessee
• Texas
• Vermont
On November 2, 2017, the Centers for Medicare and Medicaid Services (CMS) issued the Calendar Year 2018 Physician Fee Schedule (PFS) final rule, which included policy to commence the MDPP, a new benefit that covers the National DPP lifestyle change program for eligible Medicare beneficiaries.28 Positive research findings from the Centers for Medicare & Medicaid Innovation (CMMI) pilot study led to the final rule. In the 15-month study, the Young Men’s Christian Association (YMCA) enrolled and retained eligible Medicare beneficiaries in the National DPP lifestyle change program, which yielded a cost savings of $2650 per enrollee.29
While the CDC still administers the National DPP, the MDPP broadens its reach by connecting a national payer for the lifestyle change program with a specific group of at-risk beneficiaries. Rather than reimbursing healthcare providers directly, the 2018 PFS final rule created a MDPP supplier program, allowing both clinical and non-clinical entities that administer the program to gain reimbursement (e.g. YMCA, pharmacies, health systems, doctors’ offices, etc.). MDPP supplier requirements apply to the organizations delivering the National DPP lifestyle change program, not individual lifestyle coaches. A minimal amount of training and no clinical background is required to be National DPP lifestyle change lifestyle coach program.
Enrollment to become an MDPP supplier opened on January 1, 2018 and
reimbursement for approved MDPP suppliers began on April 1, 2018. Eligibility to become and maintain status as an MDPP supplier is dependent on an organization achieving quality standards through the CDC’s DPRP process.28
becoming eligible to apply as an MDPP supplier, a process that takes one year, at minimum. MDPP suppliers are eligible for reimbursement for delivery of the lifestyle change program through a pay-for-performance structure that ties payment amount to performance goals based on attendance and weight loss of individual participants. MDPP does not include reimbursement for blood glucose testing conducted to determine eligibility for enrollment in the lifestyle change program, even though half the participants must enroll based on blood testing (up from CDC’s 35 percent requirement). A MDPP supplier can earn reimbursement from $195 up to $670 per enrolled Medicare eligible participant depending on achievement of performance goals.28 New financial incentives have the potential to influence an
organization’s implementation of the lifestyle change program. The Potential Role of Pharmacy in Diabetes Prevention
Pharmacies are well-positioned to expand their role in diabetes prevention. Many pharmacies offer walk-in services and hours that typically extend beyond that of physician offices into nights and weekends. One study found that high-risk Medicaid patients visited their pharmacy 35 times per year versus seeing their primary care doctor four times per year and specialists nine times.30 Most Americans (97.1 percent) live within 5 miles of a
pharmacy.
independent and privately-held. People in rural areas may have limited access to healthcare, contributing toward the potential role of independent pharmacies to fill preventive health gaps. Sometimes the lines between independent and chain drug stores are blurred because small, regional chain-pharmacies with tens of stores may have characteristics similar to independent pharmacies with hundreds of stores; and the leadership may identify their companies, or the companies may be perceived by others as independent, chain, or both.
Pharmacists and pharmacy staff could play a critical role in identifying eligible participants, and potentially, delivering diabetes prevention lifestyle change programs. Not only can healthcare teams in pharmacies provide the requisite screenings and referrals into appropriate lifestyle change or disease state management programs, but they can help fill healthcare gaps by collaborating with physicians and other providers.32 Understanding the factors that influence initiation and implementation of diabetes prevention strategies are central to this study. The delivery of the National DPP lifestyle change program via pharmacy is still nascent.
Even though pharmacists can serve as lifestyle coaches — an especially smooth transition for pharmacists who are ADA or American Association of Diabetes Educators (AADE) certified for diabetes management counseling — it may be more financially feasible for lifestyle coach roles to be filled by lower paid staff. Pharmacy technician roles are
legislative and/or board rule changes depending on the state, to include more advanced administrative tasks, further allowing pharmacists to free up their time for patient care activities.33–37 Additionally, technicians now have the option to become certified, which can prepare them for increasingly complex roles. Certification and education requirements for pharmacy technicians vary by state.
Beyond pharmacy staff, some grocery stores with pharmacies also employ Registered Dietician Nutritionists (RDNs) and dietician technicians to support health and wellness programs. RDNs are food and nutrition experts capable of translating the science of nutrition into practical solutions for healthy lifestyles. RDNs are licensed professionals with a
minimum of a bachelor’s degree, experience from an internship, a passing grade on a
registration exam, and a state license to practice. Dietician technicians work alongside RDNs in some settings and support their work, in the same way that pharmacy technicians support pharmacists.
Implementation of the National DPP lifestyle change program could involve many levels of engagement for those with prediabetes or at risk for type 2 diabetes at a pharmacy, including: screening, referring (if not offering the National DPP in-house), or delivering the National DPP lifestyle change program. Further, some pharmacies may choose to offer lifestyle change programs that are modifications of or unrelated to the National DPP. The Role of Pharmacists in Patient Care
However, in the last 20 years that traditional role has expanded due to changes in technology that simplify the medication dispensing process, an increased pharmacist baseline level of education, and increased role of pharmacy technicians.
In the 1990s, the profession of pharmacy transitioned from a bachelor’s degree to the Doctor of Pharmacy (PharmD) degree as the sole entry-level degree for the profession with a focus on biomedical, pharmaceutical, behavioral, and clinical sciences.38 A pharmacist’s
level of education and training is similar to a dentist’s and in many cases surpasses the education and training required of other non-physician practitioners. Further, pharmacists must pass state board exams before being awarded a license to practice.39Pharmacists are
well-educated healthcare professionals who are not only medication experts, but also are highly skilled at providing patient care services. Further, professional, governmental and academic institutions have increasingly recognized the need to provide pharmacy students with an understanding of public health, as some students assume public health roles after graduation.40
Despite mounting evidence on the value of pharmacists as patient care
providers,26,39,41–43 legal, regulatory and reimbursement frameworks have not kept pace by recognizing pharmacists as providers, expanding state scope of practice (often due to
Eligibility to Provide Patient Care
Although CMS now provides coverage for the MDPP for lifestyle change, the Social
Security Act (SSA) sets provider eligibility criteria for health care programs such as
Medicare Part B. Pharmacists are not listed as providers in key sections of the SSA, which
limits beneficiaries’ access to pharmacist-delivered services. Within the law, healthcare
professionals listed as providers of medical care and other preventive services include
physicians, physician assistants, certified nurse practitioners, qualified psychologists, clinical
social workers, certified nurse midwives, and certified nurse anesthetists. In addition to
federal law that does not acknowledge pharmacists as providers of patient care nor eligible
for payment of patient care services by federal programs, the ability for pharmacists to
conduct these services is regulated by state scope of practice, which varies considerably
state-by-state. This means that the federal government does not reimburse pharmacists in the
community pharmacy setting for providing preventive screenings, such as blood glucose tests
(A1C, etc.) or wellness visits, among other services. Pharmacies can apply for reimbursement
as MDPP suppliers, since the program does not relate to provider status and National DPP
program activities are not considered patient care, but pharmacists are not eligible to receive
reimbursement through Medicare for screenings.
Payment for Pharmacist-Delivered Patient Care Services
The ripple effect of pharmacists’ lack of provider status under Medicare Part B is
far-reaching. Private health plans and state plans routinely cite the omission of pharmacists as
providers under Medicare Part B as a reason for lack of compensation for
pharmacist-provided, patient-centered care. This omission has also created barriers to pharmacist
performance metrics such as medical homes and accountable care organizations (ACOs).44
One article makes the case for pharmacists as members of the medical home and care
coordination team, pointing to multiple evidence-based research studies that show inclusion
of pharmacist care improves patient care and decreases costs.45
Given the non-recognition of pharmacists as providers of patient care services under
Medicare Part B, and few state laws that independently recognize pharmacists as providers,
there is need to validate and demonstrate the importance of pharmacy-based services to the
broader U.S. healthcare system. As an example of a state leading the way, Washington
became the first state in 2015 to sign into law a bill that required inclusion of pharmacists in
health insurance provider networks, essentially ensuring reimbursement if a pharmacist
performed a covered service.46 Implementation of this bill has been underway since 2017, but a full understanding of its effects has yet to be determined. The Washington State Pharmacy Association (WSPA) formed a workgroup to determine the metrics to evaluate and report quality and outcomes of using pharmacists to provide patient care in their state. Pharmacists within U.S. federal government systems (e.g. U.S. Public Health Service, Veterans Affairs, Indian Health Service, U.S. military), who have a broader scope of practice beyond what is outlined in the SSA for Medicare-related services, provide patient management assistance in collaboration with other care providers through medication and other clinical pharmacy services.47 Despite these successes, such models are not fully utilized in the non-federal sector due to policy, political, and payment barriers.39
Conceptual Framework
sometimes preventable, public health problem — type 2 diabetes. While pharmacies have the potential to promote and offer diabetes prevention programs, doing so is a corporate decision. This dissertation focuses on understanding the factors that might encourage pharmacies to: (1) screen people with prediabetes or at risk for prediabetes, and (2) deliver a diabetes prevention lifestyle change program to those eligible. This study analyzed factors that influenced whether a pharmacy decision maker adopted (initiated and/or implemented) diabetes prevention programs so as to promote further adoption of this program by pharmacies.
Figure 1: Conceptual model for this dissertation adapted from Frambach and Schillewaert (2002)48 and Grol et al. (2007)49
External forces feed into innovation characteristics, and then both innovation and adopter characteristics influence whether an innovation is adopted and continually used. The innovation characteristics of flexibility, pervasiveness, risk, and cost were pulled from Grol et al.9 to supplement this conceptual model with characteristics that are commonly used to study improvement in patient care programs.49
External forces are environmental and social forces that indirectly affect innovation characteristics. While external forces may influence this research, they do not have a direct effect on the development of the research aims. Frambach and Schillewaert stated that innovation is a key driver of corporate success and sought to understand the characteristics that lead to successes and failures of innovations.48 Innovation characteristics derived directly from Frambach include: relative advantage, compatibility, and flexibility; whereas
pervasiveness, risk and cost were adapted from Grol et al.49 A subset of characteristics (those circled in red within the conceptual diagram) were the driving characteristics that influenced the study’s aims. Table 3 provides an explanation of how those broad characteristics could be applied to diabetes prevention.
Table 3: Defining Innovation Characteristics in the Context of Diabetes Prevention CHARACTERISTIC APPLICABILITY TO STUDY
Cost Reimbursement of services and programs; business case to adopt program; financial sustainability of services and programs. Flexibility Adaptability of services and programs to fit pharmacy structure
(e.g. staffing needs, pharmacy workflow, store set up); flexibility in intervention offered.
Pervasiveness Magnitude of services and programs offered; sustainability; intent or interest to expand.
Relative Advantage Perceived competitive advantage, either financial or otherwise, from offering the services and programs.
culture were also relevant characteristics to consider but were not directly part of this study’s conceptual model.
Within the conceptual model, both innovation and adopter characteristics influence the adoption decision and continued use. As shown in the conceptual model (Figure 1), there are several phases before the adoption decision that are not highlighted by a red border. One of the most interesting aspects of the Frambach model not seen in all implementation science frameworks is the recognition of non-adoption as a possible outcome.48 Depending on how an innovation is perceived within the competitive market, non-adoption may occur.
Research Question and Aims
The purpose of this research was to answer the following question:What factors influence a pharmacy decision maker’s adoption of diabetes prevention programs? In this context, adoption refers to initiation and/or implementation of diabetes prevention programs. The diabetes prevention programs referred to within the research question include:
(1) Screening of people with prediabetes or at risk of type 2 diabetes, and (2) Delivery of a diabetes prevention lifestyle change program to those eligible. Each of the study aims focuses on a different diabetes prevention program while applying the same innovation characteristics.
AIM 1: Determine how innovation characteristics influence a pharmacy’s adoption of
programs to screen people for prediabetes.
• Flexibility Determine how screenings are conducted within a store. The flexibility with which screenings can be conducted within a store could influence adoption of the service. Flexibility could mean the difference between conducting screenings as people arrive at a pharmacy, by appointment via a dietician or through designated weekly or monthly health screening days, among other options.
• Relative Advantage Determine the perceived advantages gained by screening people. Relative advantage for screening programs could be improving customer loyalty, doing what is right for the community, or offering a program that competition does not offer.
• Pervasiveness Determine the extent to which pharmacies offer screenings, either within one store or more broadly across a company. This also applies to how health solutions are shared with customers, so referral is an important component.
• Research Method Conduct qualitative/key informant interviews with independent and chain pharmacy decision makers until saturation reached (target goal:
approximately 20 interviews).
AIM 2: Determine how innovation characteristics influence a pharmacy’s adoption of a
lifestyle change program.
• Flexibility Determine how a lifestyle change program is delivered, for those engaged. Understand the target audiences for the delivered programs and why they were selected. Determine if the structure of a lifestyle change program could influence its adoption.
• Relative Advantage Understand the motivations to participate in the program,
some of which may be non-financial (e.g. customer loyalty, community benefit, reach potential diabetic population, etc.). Determine the perceived advantages gained by delivering a lifestyle change program
• Pervasiveness Determine the extent to which lifestyle change programs are offered in pharmacies. In locations where a company may not offer the program, gauge the interest to refer eligible participants to a community-based organization, such as the YMCA, that may offer the program.
• Research Method Conduct qualitative/key informant interviews as in Aim 1. Research Interest
The principal investigator’s interest in public health formed while she served as a Gubernatorial Fellow at the Florida Division of Emergency Management. A few years later, while working at the National Association of County and City Health Officials (NACCHO), she managed several CDC grants aimed at leveraging pharmacies to improve community resilience and response to pandemic influenza outbreaks. From NACCHO to the principal investigator’s current role at the National Association of Chain Drug Stores (NACDS), she developed the conviction that public-private partnerships are paramount to optimal
CHAPTER 2: LITERATURE REVIEW
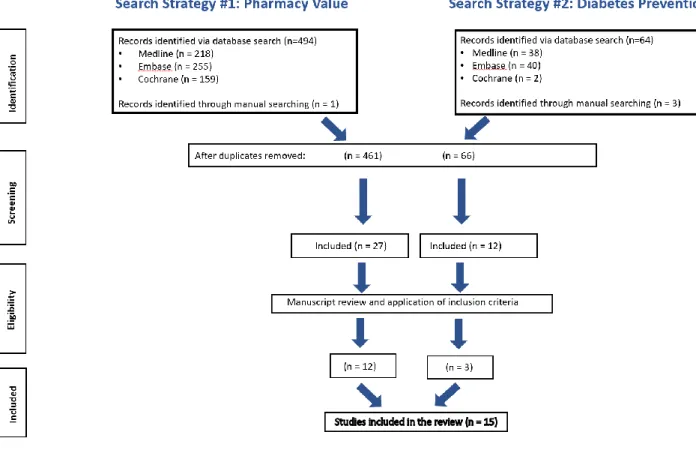
The principal investigator conducted this literature review, which included two searches on the following topics: first, the cost effectiveness of community pharmacy
services, and second, diabetes prevention in community pharmacies. The findings from these searches demonstrate the value and promise of community pharmacy, but a paucity of literature exists on the specific topic of diabetes prevention programs in community pharmacy.
Methods
This literature review was conducted from March through December 2017. The review examined the value of patient care services within community pharmacy as compared to usual care and adoption of diabetes prevention programs in community pharmacy. Rather than examine all aspects of value — including access, quality, and cost — this review sought to better understand primarily cost, which is the least understood dimension of value in community pharmacy. The purpose of this review was to identify gaps in existing research regarding the value of diabetes prevention programs.
Prior literature reviews42,50,51,52 have demonstrated the cost effectiveness of pharmacy services and the value of pharmacists as members of the care team across settings, for
identified, so the principal investigator conducted a second search on adoption of diabetes prevention programs in pharmacies, regardless of cost.
The principal investigator identified studies for the two searches using the same methods. First, she searched the following electronic databases: (1) the U.S. National Library of Medicine’s MEDLINE/PubMed; (2) Elseveir’s Embase; and (3) ESCOhost’s International Pharmaceutical Abstracts. The principal investigator manually searched the bibliography sections of relevant articles and reviews and perused four systematic literature reviews identified through the database search.50,52–54 For both searches, the principal investigator used similar search terms related to community pharmacy (e.g. community, retail, chain, independent pharmacy, or pharmacist). For the first search, she also used search terms related to cost (e.g. economic outcome, cost effective, cost savings, healthcare cost,
pharmacoeconomics). For the second search, in addition to community pharmacy terms, she searched for diabetes prevention and adoption terms (e.g. prevent diabetes, prediabetes, program, adopt, implement, initiate, intervention, strategy).
The principal investigator independently determined the eligibility of articles without a second reviewer. She imported all identified articles into F1000 Workspace, a free
reference manager software, and then moved them into Covidence, a Cochrane technology platform meant to accelerate and organize the review process for screening based on titles and abstracts. The principal investigator exported full-text articles that met the inclusion criteria back into F1000 Workspace for this final review. The technology she used in the review process automatically eliminated duplicate articles. She developed a data extraction spreadsheet to summarize and categorize included studies, garnering the following general information from each study: (1) study name (2) setting, (3) intervention and objective, (4) overall outcomes, (5) study location, (6) study period, and (7) quality. The process used to extract and categorize economic evaluations reflected an approach used in another pharmacy management study.52
Results
The second search yielded 83 articles, 80 from online databases and three from manual searching, with 17 duplicates. In the initial title and abstract review, the principal investigator decreased the number of eligible articles from 66 to 12 articles eligible for full-text review. She excluded nine articles in the full-full-text review because the research was not completed in the U.S. or focused on diabetes management without mention of prevention. She identified the three included studies via database searches only67–69 (Appendix D). Figure 2: Flow chart of the literature search methodology
Overview of Results — Search 1: Cost Effectiveness of Pharmacy Patient Care Services
up to 6 years58), with half of them55,56,58,60–62 published before 2010. The majority of these (n=10) had a prospective design, with the exception of two studies.63,65 Of the prospective studies, seven in 10 implemented a quasi-experimental, longitudinal design. Shireman and Svarstad64 implemented a randomized trial with a control group, and Tran et al.62 compared a pharmacist-managed smoking-cessation program with a self-directed attempt to quit.
Across the included studies, a mix of independent and chain pharmacies participated, and a few studies included ambulatory care clinics or hospital pharmacies as additional sites. While not all studies reported the number of participating pharmacies, the range was from a dozen on the low end to the 2014 study by Pringle et al.59 that evaluated medication
adherence across 107 intervention pharmacies and 111 control pharmacies. Asheville Project Influence
presence in this review, more than half (n=7) of the studies occurred in North Carolina, two-thirds (n=8) included an MTM intervention, and about two-fifths (n=5) focused on diabetes.
For this review, MTM included pharmacist-delivered, face-to-face patient assessment
and intervention, aimed to optimize a patient’s response to medications and manage
treatment-related medication interactions (e.g. review of patient history, medication profile,
clinical recommendations, etc.).70 Another important term for this review is Collaborative
Practice Agreements (CPAs), which allow pharmacists to work in a collaborative relationship
with physicians or other providers to offer expanded services to patients.
Clinical Findings
Most prospective studies reported on both clinical and economic outcomes. The number of enrolled patients ranged from 48 patients in a pharmacist-directed smoking cessation program62 up to 29,042 patients in a medication adherence study.59 Participants were aged 18 and older, and had a certain disease state or were currently taking certain medication(s) in most studies. In their 2016 study Shireman and Svarstad64 noted race as eligibility criteria, focusing on black patients with uncontrolled hypertension where 60 percent of the control group was Medicaid eligible. All Asheville Project studies or inspired studies55,56,58,60,61,66 focused on beneficiaries of the City of Asheville and employer-based payers, whereas the 2014 study by Pringle et al.59 included patients covered by multiple government and commercial payers.
thirds (n=8) of the studies focused on MTM interventions, whereas Shireman64 looked at adherence issues through an education program,64 and Pringle addressed that same issue through screening and brief interventions.59 Klepser et al.’s 2012 study65 explored a model of pharmacist-as-provider for the diagnosis and treatment of pharyngitis (economic model only). All other studies lacked pharmacist prescribing autonomy as a research factor.
Understanding the change in health outcomes provided context for the focus of this first search: cost effectiveness, or value more broadly, of patient care services in community pharmacy. Several studies showed improvements in key clinical outcomes measured across disease states. Four studies demonstrated positive patient outcomes for cardiovascular health.58,59,64,66 In general, the positive patient outcomes related to improvement in blood pressure goals and attainment of improved cholesterol.58,59,64,66 Among the cardiovascular health studies, the 2011 study by Bunting et al.66 was the only one that did not show statistically significant improvements.
Economic Findings
Two thirds of studies (n=8) reported on economic outcomes from the payer’s perspective, while the remaining studies focused on the societal62,65 or pharmacy
perspective.63,64 Most studies compared cost in relation to usual care (e.g. control group, usual physician services, or historical healthcare utilization data). Most studies looked at cost-effectiveness in these ways: direct or indirect cost savings, dollars per patient per year (PPPY), combined savings, savings overall compared to medication costs, and savings in terms of emergency department visits or hospitalizations. Klepser et al.65 and Tran et al.62 evaluated economic outcomes from the societal perspective and used Quality Adjusted Life Years (QALY) or Quality Adjusted Life Days (QALD) for comparison.62,65
Several studies identified savings or averted costs. In the 2006 study Bunting et al.56 compared costs against historical patient data and reported combined savings of $584,307 over 5 years for its asthma MTM program. Bunting also used historical data for comparison and reported $928,926 in averted cardiovascular-related medical event costs and a decrease in cardiovascular-related medical costs from 30.6 to 19 percent of total cost of care. In their 2011 study Bunting et al.66 used historical data for comparison and reported cumulative net health plan savings for the 3-year diabetes program estimated at $762,426. In their 2009 study Fera et al.55 estimated averted total costs for employers as $278,512 and for patients as $339,875 during the program’s first year.
found the integrated model had greater ROI than hub and spoke ($22,072.91 vs. $7,600.74), but both models demonstrated positive ROI (1:12 – 1:21).9 Tran et al.62 found the
incremental cost for an additional patient to quit smoking using the pharmacist-directed program alternatives versus a self-directed quit attempt was $236 for the cold-turkey method, $936 for nicotine patch, $1,232 for nicotine gum, and $1,150 for bupropion. Dependent on the smoker's age at the time of cessation, the incremental discounted cost-effectiveness was $720 to $1,418 per life-year saved.
Only Shireman et al.64 reported costs incurred by the pharmacy rather than costs saved. The cost of helping one more person achieve the BP goal < 140/90 mm Hg) was $665.2 ± 265.2; the cost of helping one more person achieve good refill adherence was $463.3 ± 110.7.64 These costs took personnel time into account, among other factors. Shireman et al. concluded that pharmacists can implement a cost-effective intervention to improve hypertension control in African-Americans, even with costs incurred by the
pharmacy. This study made no mention of reimbursement for pharmacist-delivered services. Pringle et al.59 found a significant reduction in health care spending per patient for those taking statins ($241) and oral diabetes medications ($341) due to medication adherence interventions. The study postulated that for a payer with 10,000 members, implementation of their brief adherence intervention could translate into $1.4 million saved over 12 months. If a payer had exclusively contracted with their intervention group pharmacies, it would have increased their quality ratings by one Medicare star. For a Medicare Advantage plan with one million patients, that one star rating increase could translate into $100 million in new
a mean total prescription cost increased from $656 to $2,188 per person per year from the study’s first to fifth year. Despite that trend, the mean total cost of care decreased annually.
Overview of Results — Search 2: Diabetes Prevention Programs in Community Pharmacy
The first search for this review demonstrated that pharmacist-delivered diabetes management interventions have clinical and economic value, like other disease state interventions, but those studies did not address diabetes prevention. So, the principal investigator initiated a second search to better understand pharmacy adoption of diabetes prevention programs. Most of the excluded studies in the abstract and title review focused on disease management instead of prevention. Two of the included studies had a cross-sectional design68,69 and one a mixed-method evaluation.67 Two studies pertained to student
pharmacists and diabetes prevention,67,69 while the other study addressed cardiovascular health and wellness, including screening for metabolic syndrome, for which diabetes is a risk factor. These studies addressed lifestyle change and education; however, only Woodard et al.67 published in 2016, referenced the DPP studies, and none referenced the National DPP, established in 2010, the year the other two included studies were published.
Cross-sectional Studies
ethnic group, and sedentary lifestyle reported by 20 percent of participants. The number of reported risk factors increased significantly for participants aged 40 and older.69 Letassy demonstrated the feasibility of student pharmacists offering diabetes risk assessments and education in community pharmacies, but the study did not track whether the risk assessment affected health outcomes nor did it address reimbursement. Further, the study did not report on subsequent patient initiation of lifestyle changes or success in making such changes.69
Olenak et al.68 led a 2010 cross-sectional study in Pennsylvania to determine the 10-year risk of developing coronary heart disease (CHD) and measure effectiveness of patient lifestyle changes. The 239 patients aged 18 years or older with no history of CHD were screened for metabolic syndrome, Framingham risk assessment, and medication use. Pharmacists discussed screening results with patients and educated them on metabolic syndrome and lifestyle change recommendations; patients also received a follow-up survey.68 Metabolic syndrome is a collection of conditions including increased blood pressure, high blood sugar, unhealthy cholesterol levels, and excess abdominal fact; having metabolic syndrome increases the risk of developing diabetes by five times. The prevalence of metabolic syndrome in the study was 36 percent. Of the study population with no known history of diabetes or prediabetes, 26 percent had an abnormal glucose reading. In the 3 to 6-month follow-up period, 87 percent of those with metabolic syndrome self-reported a lifestyle modification of diet, exercise, and/or weight loss.68
Descriptive Study
Diabetes Prevention Program Group Lifestyle Balance (DPP GLB), which is an adaptation of the DPP developed by the University of Pittsburgh Diabetes Prevention Support Center. The course’s learning objectives included: summarize the burden of diabetes in the U.S.; evaluate scientific evidence for the value of the DPP to prevent diabetes; discuss the role of weight management and physical activity to prevent diabetes; and lead a DPP GLB course.67 Students took a pre/post course assessment that reviewed content and evaluated their confidence to serve as lifestyle coaches. For the 49 participating students, baseline
knowledge increased from 58 percent to 61 percent at course completion. Confidence scores improved from a mean of 2.2 at baseline and 4.4 after course completion. Students did not serve as lifestyle coaches beyond practice in the classroom, but the skills learned were directly applicable to the community pharmacy setting.67
Discussion
The literature searches demonstrate the potential value pharmacies can deliver through diabetes prevention programs. No cost-effectiveness information exists on the value of pharmacist-delivered diabetes prevention programs, but given their effective management of diabetes and other chronic diseases, their role in diabetes prevention is promising. The first search confirmed that community pharmacists can cost effectively improve patient health outcomes. Of the eight studies that evaluated patient care outcomes,55,56,58–61,64,66 all but the 2011 Bunting66 study produced statistically significant results about health outcomes.
changes. These two studies focused on student pharmacists rather than registered
pharmacists, and a third study by Woodard et al.67 published in 2016 simply discussed the impact of a course to prepare student pharmacists to serve as lifestyle coaches. The focus on students indicates that some student pharmacists have acquired the skills needed to assess diabetes risk factors and serve as lifestyle coaches.
While evidence indicates the National DPP is an effective lifestyle change program,72,26 no peer-reviewed literature through 2017 demonstrated effectiveness of executing the program by a pharmacy. Pharmacies are increasingly offering the National DPP lifestyle change program, either by delivering the program directly or referring patients to the program. Some literature exists on the role of community pharmacies in weight management programs broadly,68,73-75 although not specific to the National DPP lifestyle change program, diabetes prevention, or prediabetes detection. Given evidence of success pharmacies have achieved by assisting patients with managing their diabetes through A1C testing and other measures,55,59–61,66 it is reasonable to consider that pharmacists could use that same skillset to identify people with prediabetes. Several articles address prediabetes and the role of pharmacists in other countries,76,77 but little research exists within the U.S.
contracts with each one, given the lack of Medicare provider status and discrepancy across state scope of practice. This literature review did not identify information on the cost effectiveness of diabetes prevention programs in pharmacies, nor studies seeking to determine whether a sustainable business model for such programs exists.
While still focused on medication management, Pringle et al.59 took a notable step in a positive direction by linking cost savings with quality measures for health plans. As the healthcare sector shifts toward a focus on value-based care, partnership with health plans and physicians will become increasingly important for community pharmacy. Such as shift is now occurring in diabetes prevention with Medicare offering a pay-for-performance model for delivery of the MDPP. Only Pringle59 highlighted an important finding that pharmacists can increase value, by supporting team-based care efforts to attain higher
quality/performance metrics, while improving patient safety and enhancing care delivery. Medication optimization and adherence are critical issues that pharmacists can address. However, there are several gaps in other areas of care. Nearly all states enable pharmacists with some type of prescriptive authority across the spectrum of collaborative prescribing to autonomous prescribing. Collaborative models offer a broad framework for the treatment of acute or chronic disease whereas current autonomous prescribing models have focused on a limited range of medications for which a specific diagnosis is not needed.78 Within this literature review only the 2012 study by Klepser et al.65 referenced a care management program utilizing pharmacist prescribing.
As part of the review process, included studies were rated for quality. Factors
quality;55–58,60,61,63–66 Tran et al.’s 2002 study62 was low quality; whereas Pringle et al.’s 2014 study59 was high quality. Asheville Projects studies had overall medium-to medium-high quality, but used data from the same patient population pool and relied on historical data as a comparison group. For the second search, the Olenak and Calpin68 study was rated as high quality, while Letassy et al.69 and Woodard et al.67 studies were medium quality.
CHAPTER 3: METHODOLOGY Study Design and Methodology
The research question for this study was: What factors influence a pharmacy decision maker’s adoption of diabetes prevention programs? Adoption referred to initiation and/or
implementation of diabetes prevention programs, including screenings and lifestyle change programs. The principal investigator employed qualitative research methods for this study, including semi-structured in-depth interviews by phone (Table 4). A constructivist
worldview guided this research, as she sought to establish meaning of phenomenon shared by study participants.79 Specifically, the principal investigator utilized grounded theory by applying theoretical learnings from her conceptual model to drive the overall research approach.80
Table 4: Summary of Research Data Collection Method and Tool
Aims Data Collection Method Data Collection Tool
Determine how innovation characteristics influence a pharmacy’s adoption of: 1. Diabetes screening 2. Lifestyle change
program for people with prediabetes and at-risk for type 2 diabetes.
In-depth interviews; 30-45 minutes by telephone (recorded when allowed)
Interview guide developed by PI that mapped back to conceptual model
reached but began with a goal of approximately 20 interviews. Saturation is a concept derived from grounded theory80 that means data are collected until no new ideas are generated. The interview questions mapped back to the study aims and aligned with key characteristics identified in the study’s conceptual model. In April 2018, the principal investigator pilot tested the interview guide with three individuals — two who worked in community pharmacy and one who worked at an academic pharmacy clinic with similar characteristics to a community pharmacy. The principal investigator revised and finalized the interview guide (Appendix G) based on pilot interviews prior to data collection.
IRB and Protection of Human Subjects
The Office of Human Research Ethics, Institutional Review Board (IRB) at the University of North Carolina (UNC) Chapel Hill reviewed this study (#17-2619) and
determined it to be exempt from further review on March 3, 2018. While this research study had minimal risks to participate, the principal investigator took precautions to protect the privacy of study participants and prevent the possibility of a breach in confidentiality. Sample Size and Eligible Participants
The principal investigator employed purposeful sampling — a common approach used in qualitative research — to garner a variety of pharmacy executive perspectives regarding diabetes prevention. Eligible participants for the study had to meet the following requirements: (1) employee of a community pharmacy company, and (2) decision maker who can determine if a new clinical service is initiated or implemented in the company.
study, with an added goal of reaching some participants affiliated with pharmacies that are engaged in lifestyle change programs and some that are not. Further, given variation across types of chain pharmacies, she proactively sought to include national and regional chains, including traditional drug stores, as well as grocery stores and mass merchants with pharmacies.
The principal investigator conducted 22 interviews but deemed one ineligible and subsequently excluded it. The ineligible interview included a decision maker with autonomy over one store but not an entire chain, therefore a corporate-level decision maker from the same company was interviewed instead. In total, 21 individuals from 21 companies
participated in the study — 11 independent and 10 chain pharmacy decision makers. The 10 chain pharmacy decision makers represented a mix of five national and five regional
companies, including three traditional drug stores, five grocery stores, and two mass merchants. Most regional chain participants represented companies operating about 200 or more stores, while one operated fewer than 20 stores. The 11 independent pharmacy decision makers involved were affiliated with pharmacies located in Illinois, North Carolina,
Pennsylvania, Tennessee, Texas, Utah, and the District of Columbia. Participant Identification
The principal investigator identified potential participants for the study through the following strategies:
• Pharmacies Engaged in Lifestyle Change Programs
On March 30, 2018, she downloaded the publicly available registry of organizations that have pending, preliminary, or full recognition status through the CDC’s Diabetes Prevention Recognition Program (DPRP), the quality assurance arm of CDC’s National Diabetes Prevention Program (National DPP) lifestyle change program.81 She reviewed the list of 1,693 organizations, and used key words (e.g. specific company names, pharmacy, drug store, grocery, food, etc.) to identify all listed community pharmacies, a total of 26 independents and nine chain pharmacy locations representing a total of five corporate entities.
She identified the appropriate executive at the 26 independent pharmacies by contacting a colleague at the National Community Pharmacy Association (NCPA) who provided her with names and e-mail addresses for 24 of the 26 (no data available for two on the list). For the five chain pharmacies, she used her professional contacts, supplemented by searching her employer’s membership database to identify executives at companies that were unfamiliar to her.
• Pharmacies Not Engaged in Lifestyle Change Programs
More than 18,000 independent pharmacies operate across the country, but the principal investigator did not have access to a database that allowed for random selection of participants. She therefore used a convenience sample to reach out to independent
independent pharmacies (e.g. a dissertation committee member, multiple community pharmacy professors in different states, a professor from a medical school, and a state
pharmacy association executive) for assistance. Through these individuals, she acquired a list of nine independent pharmacy contacts. She e-mailed all of them, and successfully completed interviews with two individuals from North Carolina and Tennessee, respectively.
For the chain pharmacies in this category, she primarily targeted the top 25
pharmacies, categorized by number of pharmacies, percentage of U.S. pharmacy locations, and percentage of U.S. prescription share. Fewer than 100 chain pharmacy companies exist in the U.S., yet a relatively small number of companies own hundreds or thousands of stores due to consolidation in recent decades. She purposefully prioritized contacting the 25 largest pharmacies to understand perspectives of larger regional and national chains. Very small chain pharmacies may have overlapping characteristics with independent pharmacies with several stores, and she wanted to seek a potentially different viewpoint in independent and chain participants. She identified decision makers from these companies by using her professional contacts, supplemented by searching her employer’s membership database.
• Crossover Across Groups
change program (e.g. looking to enroll their first class in a few months), so their information was not listed in the CDC’s DPRP database when she downloaded it in March 2018.
• Additional Efforts to Reach Participants
The principal investigator had an advantage in conducting outreach to chain pharmacies because of personal connections and the nature of her professional work. For a handful of pharmacies, if her first and second e-mail invitations to participate went unanswered, she identified and e-mailed a different individual in the organization whom she thought would still be appropriate to participate and likely to respond. In other cases, she e-mailed a
colleague at a chain pharmacy with the specific purpose of asking them to help her reach the appropriate contact within the company for an interview. These approaches increased
participation across chains, especially traditional chains and mass merchants. Such strategies would make this study particularly difficult for other researchers to replicate because the principal investigator had greater access to potential interview participants than a researcher without similar connections.
Data Collection