Housing discrimination at the intersection of health
condition, race and felony status
Jacob Henkels
Abstract
Those reintegrating into society from incarceration are faced with a stigma that prevents them
from receiving basic human needs. The label of "felon" creates collateral consequences that prevent access to necessities like employment, healthcare, and housing (Pager, 2003; Kugelmass, 2016; Evans, 2018). Housing has been identified as one of the most critical
necessities in the process of reentry – however, it is widely inaccessible for people with a criminal record (Garland et al., 2010; O'Brien, 2001). Health issues are also highly prevalent within the formerly incarcerated population, as reentering individuals are at significantly higher risk of having both physical illnesses and mental disorders (Pedersen, 2019; Bronson & Berzofsky, 2017). In order to live a healthy life, it is imperative to be housed due to its positive
impact on both physical and mental health (Evans, 2003; Kreiger & Higgins, 2002). While it is known that housing institutions discriminate on the basis of criminal record, it is unclear
whether health status or race play a role in affecting the accessibility of housing for a
reentering individual (Helfgott, 1997; Thacher, 2008; Evans et al., 2019). This study uses the audit method to examine the effects of health status and race on housing outcomes. Fictitious
testers, known as auditors, sent emails inquiring about rental listings to housing organizations across North Carolina. The emails that each auditor sent signal various health and racial
characteristics that are used to examine potential cases of discrimination based on the amount of positive responses each received. I did not obtain evidence that suggests differential
treatment on the basis of health with regards to housing outcomes. However, the results
Table of Contents
Introduction ………...4
Significance for public policy ………...….. 6
Literature Review ……….……….... 8
Background and historical context ………...…. 8
Housing acquisition and offender status ……….…….. 9
Health Conditions and reentry ………....… 10
Related Audit Studies ………...………..….. 12
Methods ……….………..….. 14
Auditors ………...………. 14
Housing organizations ………...…………..… 15
Study design and procedure ………..……….….. 15
Data Analysis……….….………….…. 17
Results ……….………...…… 19
Response by health status ……….……….…..… 19
Response by race ……….……….……. 21
Response by CSA (Combined Statistical Area) ………..………. 25
Discussion ….………...……….. 27
Conclusion ………...……….…………. 31
References ……….………. 32
Appendix A – Emails sent ………...……….. 40
Introduction
This thesis adds to our understanding of the housing barrier faced by the formerly incarcerated
population by examining the effect of health status and race on housing opportunities. Health conditions are central to this study due to the high prevalence of physical and mental health illnesses within the formerly incarcerated population (Bronson & Berzofsky, 2017; Massoglia,
2008). The potential for reduced housing opportunities for those with health issues and a criminal record is a pressing concern this paper seeks to address. If in fact physical or mental
illness affects the ability of a formerly incarcerated individual to obtain housing, it would be imperative for future research around the reentry housing barrier to explore this relationship further. It would also push policymakers and government institutions to consider this
relationship in the process of criminal justice reform.
Those that have been convicted of a felony are faced with a stigma that prevents them from
obtaining basic human needs, making reintegration a perpetual process. Many find it
challenging to start from scratch due to difficulty in attaining education, gaining employment and becoming financially self-sufficient (Sokoloff & Schenck-Fontaine, 2017; Sugie, 2018;
Roman, 2017). However, stable housing is consistently identified as one of the most critical and challenging necessities to obtain (Garland et al., 2010; O'Brien, 2001). These consequences, known as collateral sanctions, work as extensions of the punishment that these individuals have already incurred from the criminal justice system.
Housing is a crucial issue for people returning from incarceration. On top of being a basic
human need, it has proven to be a critical aspect of successful, comprehensive reintegration (La Vigne et al., 2004). Housing is the foundation for one to rebuild every other aspect of their life. In the private housing market, housing organizations and landlords often deny potential tenants with a felony record due to the increased presence of mandatory background checks and the unwillingness of landlords to accept a formerly incarcerated individual (Helfgott, 1997;
status alongside a felony conviction has been shown in some studies to decrease one's chance
at attaining housing in addition to the aforementioned necessities (Wheelock, 2005). This study intends to expand on previous literature by considering how mental and
physical health conditions may add another dimension to the housing discrimination faced by people with a criminal record. Both of these health problems plague people involved in the justice system at much higher rates than the general population (Bronson & Berzofsky, 2017;
Massoglia, 2008). Housing also has significant implications on health status, given that having a stable place to live leads to improvements in both physical and psychological health (Evans,
2003; Kreiger & Higgins, 2002). Given the importance of housing and its effect on health and the reentry process, this thesis aims to address the potential effects and interactions that health conditions could have on race and felony status in the housing process. Housing and health go
hand-in-hand for both the formerly incarcerated population as well as the general public. In Maslow’s Hierarchy of Needs, shelter is at the base of essential human needs. This necessity is
most-pressing for the formerly incarcerated as it provides the foundation of a successful
reintegration as well as a healthy life. In addition, this topic has not been addressed in previous audit studies examining housing discrimination and reentry.
Using an experimental audit study, I will investigate the effects of health status on housing outcomes among formerly incarcerated individuals. Pager (2003) has previously analyzed
differential treatment caused by criminal stigmatization and race with regards to employment outcomes using this experimental method. She discovered that applicants who disclose a former felony on a job application had lesser chances for employment, and that being Black
further amplified this disparity. The current study examines these findings with respect to housing with the inclusion of health status, asking the question: how does felony status and
race interact with health status to affect a formerly incarcerated individual's ability to gain rental housing? The results will be discussed in light of my initial expectations that having some health problem will lower the level of housing opportunities for the auditors reporting
Significance for Public Policy
Every year, more than 650,000 people are released into their communities from state and federal prisons (Department of Justice, n.d.). Within this population, more than 10% of those
coming in and out of prisons return to homelessness in the near-future (“Formerly
Incarcerated People,” 2018). However, there is more nuance to this number that complicates our image of reentry and homelessness. According to the Prison Policy Initiative (2018), those
who have experienced incarceration once are seven times more likely to experience
homelessness than the general public, whereas those who have experienced incarceration more
than once are 13 times more likely than the public. With these numbers in mind, it is also necessary to mention how homelessness is measured and the effect it has on these estimates. HUD utilizes a method known as Point-in-Time (PIT) that utilizes volunteers to identify and
report the number of sheltered and unsheltered people experiencing homelessness in their county on an annual basis. The inherent flaw with PIT stems from the inability for volunteers
to provide a comprehensive illustration of the homelessness count within their counties, in addition to neglecting the transitory nature of homelessness (“Don’t Count on It,” 2017). The primary implication here is that estimates of homelessness, including the aforementioned
numbers, are always underestimated.
The relationship between reentry and homelessness is alarming, particularly when
compared to the general public. Formerly incarcerated people are almost ten times more likely to be homeless than the public. This statistic is exacerbated for those incarcerated more than once, recently released individuals, women, and people of color (Couloute, 2018). One of the
policy issues closely related to this study and reentry housing is recidivism. Central to the relationship between incarceration and homeless is the revolving door that pushes individuals
in and out of jail and/or prison. About 44% of those released from state prisons in 2005 were rearrested within a year of release, 68% within three years, and 83% in nine years (Alper et al., 2018). Homelessness itself is criminalized through current policies and aggressive law
enforcement tactics such as confiscating items like tents, bedding, or papers, making panhandling illegal, and enforcing “quality of life” ordinances related to public activity and
Given the state of homeless in the reentry process and its relationship with adverse health
conditions, particularly for mental health, this study seeks to examine how health conditions relate to housing outcomes for reentering individuals (Mallik-Kane & Visher, 2008).
Homelessness and health status have an alarming relationship. Mental health issues are highly prominent among both the reentry and homeless populations, so much so that 20% of those reentering with a mental illness return to society without stable housing or any housing
whatsoever (McKernan, n.d.). The high presence of psychological issues alongside
homelessness is well-documented. In a study of 979 people experiencing homelessness in Ohio,
one third reported the need for mental health services (Roth & Bean, 1986). The range of mental illnesses is also quite broad, ranging from anxiety and depression to disorders such as psychosis, alcoholism, bipolar disorder, and various personality disorders (Bassuk et al., 1984). Additionally, substance abuse is a strong risk factor for incarceration among both homeless and non-homeless former inmates (Greenberg & Rosenheck, 2008).
On the topic of physical health, there are also pressing public health problems at-hand. Homeless people are at significantly higher risk of physical health issues than those with
housing due to a slew of causes: extreme poverty, delays in seeking care, and the adverse health
effects of homelessness itself all contribute to major disease severity (Hwang, 2001). Common medical problems among the homeless population include asthma, seizures, arthritis, chronic
obstructive pulmonary disease, or multiple forms of musculoskeletal disorders (Crowe & Hardill, 1993). Moreover, people who are homeless die on average of 12 years sooner than the general U.S. population (“Homelessness & Health,” 2019). Yet despite the significant health
disparities associated with incarceration and homelessness, there is an immense lack of health services dedicated to these populations (Hwang, 2001). Not only does the current state of
Literature Review
Background and Historical Context
It is commonly known that the United States incarcerates more people than any other country, so much so that 698 of every 100,000 US residents (Sawyer & Wagner, 2020). This means that an upwards of 2.3 million individuals are incarcerated at this time in 2020. Key aspects when
discussing the total prison population are race and gender, each with critical disparities at-play. The difference in the racial proportion of the incarcerated population is such that 2,207
per every 100,00 of Black individuals are incarcerated, as opposed to 380 per 100,00 of White individuals. And on the gender disparity, about 93% of those incarcerated are male, which is why I chose to only signal male auditors. The prison population is also filled with a large
proportion of young people, especially when it comes to the population of incarcerated young Black men – so much so that 9% of Black males in their late twenties are incarcerated (Wagner,
2012). Another common factor underlying the state of incarceration in the US is poverty, as people in jail or prison are disproportionally poor compared to the general population. In 2014, the incarcerated population had a median annual income of 41% less than
non-incarcerated people of similar ages (Rabuy & Kopf, 2015). It is also no secret that the prison population are at a disproportionally higher risk to have chronic health problems, including
diabetes, HIV, high blood pressure, asthma, on top of substance abuse and mental health problems (Sawyer, 2017). The criminal justice system and its massive incarcerated population has brought the overall U.S. life expectancy down by 5 years, as its been shown that each year
in prison takes an average of two years off an individual’s life expectancy (Widra, 2017). Formerly incarcerated individuals in the United States face a prejudice that can be
explained by the negative social construction of "others". This term is widely used to describe groups that have ultimately been illegitimated due to socio-demographic characteristics such as race, gender, or felony status (Alexander, 2010). Individuals re-entering from incarceration
have been "othered" by housing providers and long-standing policies that both frequently deny potential tenants with a criminal history. One of the most significant policy strikes against
You're Out," narrowed its focus on removing anybody with a felony record from public
housing (Tress, 2009). Political rhetoric and the media at this time established the long-standing image of the "felon monster," making it easy for housing providers to take on the
attitude of denying these people housing the same way government tends to do (Stuntz, 2001; Carey, 2005; Goff et al., 2008).
In Keesha Middlemass's Convicted and Condemned: The Politics and Policies of Prisoner Reentry, a felony status is described as a "social disability". In the same vein that the medical model of disability focuses on impairments that limit life activities, formerly incarcerated
individuals are legally disabled and incapacitated, limiting their ability to engage with society (Hill & Hill, 2002). While housing is a top priority in the reintegration process, other major limitations include revoked voting rights (over six million prevented from voting since 2016)
and subtle laws and biases that prevent access to employment (“Felony Disenfranchisement,” 2016). The political and policy landscape regarding prison reentry over the last few decades has
shaped the lives of millions exiting incarceration and prevents individuals from fully escaping the grasp of the criminal justice system.
Housing acquisition and offender status
A stable home provides the foundation for one to build a healthy, successful life. A life without
a home blocks families and individuals from securing basic necessities such as good health, income, and shelter. There are also lesser-realized needs that are blocked by homelessness, such as a lack of a mailing address (which is a requirement for plenty of job applications),
having a bank account, obtaining a driver's license, and owning a cell phone as well. With regard to reentry, housing is viewed as the first necessary step to begin a successful
reintegration (La Vigne et al., 2004). Unfortunately, housing is widely inaccessible to
individuals attempting to reintegrate (Roman & Travis, 2004). Landlords and public housing providers frequently deny anyone with a felony record right off the bat. Others tend to use
"case-by-case" approaches that typically deny felony records as well. Another aspect related to criminal records in the housing process is credit history, which is often a basis for denial
There are more factors that play into the chance that a formerly incarcerated individual has
to gain rental housing. Demonstration of rehabilitation is known to be important for gaining housing, as shown in a previous audit study (Leasure & Martin, 2017). If one demonstrates
they are undergoing rehabilitation by providing a Certificate of Qualification for Employment (CQE), there is a much more likely chance that they can gain housing. A CQE is a court-provided document that reports rehabilitation and other encouraging steps of progress that
works to alleviate barriers to basic necessities, which is a proven benefit for those reentering and seeking rental housing (Leasure & Martin, 2017). This demonstrates the importance of
healing for acquiring housing. In terms of other social characteristics, gender has been shown not to play a significant role in the difference in housing opportunities for reentering
individuals (Evans et al., 2019). The role of race in affecting housing opportunities for the formerly incarcerated has been a research question with no definite answers, given that studies have reporting both some or no differential treatment on the basis of race in the housing
market (Evans et al., 2019; Hogan & Berry, 2011). Given this uncertainty, this study hopes to add to the discussion on racial discrimination in the rental housing market for the formerly incarcerated.
Health conditions and reentry
A significant factor in the process of reentry is addressing health issues both mentally and physically. Not only are these issues standalone problems, they also get in the way of other reentry necessities like acquiring employment or housing. According to the U.S. Department
of Justice, 14% of federal prisoners and 26% of jail inmates report meeting the threshold for serious psychological distress (SPD). In addition, 37% of prisoners have been diagnosed with a
mental disorder (Bronson & Berzofsky, 2017). These statistics make sense due to the intersection of mental illness and justice-involvement: mental illness may be a partial motivator/cause of crime, and the psychological distress caused by incarceration can lead to
problems in itself. The rates of mental disorders also do not vary greater among people that have committed different forms of crime. The aforementioned statistics also mean that prison
of coordination between criminal justice, mental health, and social service professionals that
takes place to assist these individuals in reentry, which causes the treatment process to be ineffective and time-consuming (Draine et al., 2005). The myriad of services in place to meet
these mental health needs are currently inadequate, even though there exist exemplary programs that have shown progress (Hammett et al., 2001).
Similar to the mental health conditions involved with prison reentry, the case of physical
health conditions is quite similar. Formerly incarcerated individuals prove to be much more prone to poor physical health, partially due to the lack of housing available for reentering
individuals (Pedersen, 2019). As previously mentioned, common health problems in the incarcerated/formerly incarcerated population include chronic conditions such as diabetes, HIV, high blood pressure, and asthma (Sawyer, 2017). Studies have shown the deleterious
effect of incarceration on morbidities related to infectious diseases (Massoglia, 2008). Plenty of these conditions are associated with confinement, as its been shown that incarceration worsens
general health symptoms over short periods during the life course (Lee et al., 2017). When it comes to the status of the formerly incarcerated population and access to healthcare, there is evidence that access to both medical and dental care is far worse than for
people who have not experienced incarceration (Kulkarni et al., 2010). A majority of people returning from incarceration also have less access to health insurance, preventing the
treatment of chronic health conditions which also leads to higher levels of emergency room use (Mallik-Kane & Visher, 2018). There is a pressing situation with the health conditions of the formerly incarcerated population, which makes it harder for individuals to work on their
reintegration process. It also causes housing providers to view applicants as higher-risk, which can further decrease the chance of accessing private housing rental. For these reasons, the
inclusion of health condition in the audit study is central and imperative. Because both mental and physical health problems are highly prevalent in the formerly incarcerated population, it is imperative that this study examines if health status may potentially be another mechanism of
Related audit studies
Audit studies are a relatively new method in social science that was pioneered by the late Devah Pager in her paper The Mark of a Criminal Record (2003). While I have already detailed this study, it is important to mention the influence of the paper on future audit studies
including this thesis. Pager's paper solidified the use of audit studies to prove differential treatment for justice-involved individuals as well as the racial disparities that exist within the
system. As many audit studies would utilize in the future, the auditors Pager utilized sent out job applications while reporting various social characteristics to dissect potential cases of
differential treatment. The Mark of a Criminal Record specifically used four auditors that varied by race and held other characteristics like age and educational attainment constant. Audit studies utilizing emailing or other forms of communication came later and are inspired
by Pager's study.
One of the top scholars who utilizes audit studies is Michael Gaddis, whose paper An Introduction to Audit Studies in Social Sciences (2018) has provided academics a detailed guide to conduct their own audit studies on a multitude of topics. The use of email audit studies, also known as correspondence studies, has been a new way for researchers to conduct these
experiments. Charles Crabtree is a pioneer in the use of correspondence studies and has provided guidance in this paper. Crabtree’s An Introduction to Conducting Email Audit Studies
(2018) covers topics such as email address collection, email delivery, outcome collection, and signaling. These papers were heavily influential in the methodology of this study.
The audit study most related to this study is titled Examining housing discrimination across race, gender and felony history (Evans et al., 2019). The primary pieces of this paper that inspired this study was first the key question: how do race, gender, and criminal history affect
housing outcomes? Of course, this study differs by replacing gender with health condition. Although the study utilized calling as the method of auditing as opposed to emailing, the use of names to signal social characteristics was replicated in this study. Evans found that a criminal
record negatively affected housing opportunities immensely, but no difference in minority and non-minority testers. While this thesis hypothesizes that race will make a difference in the
Another study titled Criminal records and housing: an experimental study provided guidance and inspiration for this study (Leasure & Martin, 2017). The paper posed two key questions: does a person with an old criminal record fare better in private housing outcomes
than one with a recent record, and does a person with a misdemeanor record fare better than someone with a felony record? While these questions differ from the question I pose, the auditing methodology the Leasure study utilizes and aspects of its data analysis provided
further direction to this thesis. Leasure and Martin constructed an audit model that used calling, in which a male tester called property managers in order to suggest differences in
housing outcomes on the basis of the type of conviction. The key results had multiple
implications. First, it was found that an applicant that provided evidence of rehabilitation by reporting a Certificate of Relief (known in Ohio as a Certificate of Qualification for
employment) was significantly more likely to be considered for housing than someone who does not present the same evidence. Second, as a direct answer to the key questions, was that
people with misdemeanor convictions as opposed to felony convictions had better housing outcomes.
This thesis seeks to expand on the past audit studies examining criminal records and
housing outcomes by inserting health status into the methodology. The conclusions to come also take a look at the same underlying issues that each of the previous papers discuss: the
collateral consequences of a criminal record that prevents individuals from accessing housing. This paper will also have similar implications related to the revolving door that housing inaccessibility creates that cycles individuals in and out of homelessness and reincarceration.
Methods
This study utilizes an experimental audit design to assess the effects of health status and race of
formerly incarcerated men on the level of housing opportunities they receive. Audit studies, which involve data collection through real-world interactions, have been used to detect discrimination in a variety of settings, including employment, doctor appointments, or
housing (Pager, 2003; Kugelmass, 2016; Evans, 2018). In this study, six email accounts were created representing six fictitious people (the "auditors") posing as individuals seeking
apartments. All six emailed housing organizations across North Carolina to assess their responses to rental inquires. Responses came in both email and voicemail form; with that being said, all voicemails were automatically transcribed into email form using Google Voice
and were analyzed the same way.
Auditors
The six auditors varied by health status and race. All six auditors were also signaled as male due to the disproportionate amount of men in the criminal justice system. Three auditors
posed as Black men and the other three as White men. Within each set of three, one auditor reported no health conditions, one reported having a mental health condition, and one
reported having asthma as a proxy for physical health status as a whole. For physical health conditions, I chose to use asthma as a common health condition that may also raise certain concerns with regards to housing with factors at play such as the varying air quality of a
community, potential for mold, etc. Asthma is also more prevalent for people with a history of incarceration than those without. (Wang & Green, 2010). Utilizing six different auditors, I am
able to examine the impact of health status and its intersection with race compared to
applicants with no health conditions. Utilizing six different auditors, I am able to examine the impact of race and its intersection with health status compared to potential tenants with no
health conditions. All three of the Black auditors were given the name Jamal Williams, and the White auditors named Robert Walsh. For each email account, phone numbers were also given
Housing Organizations
The data for this study was drawn from a sample of housing organizations with rental property listings posted online, located in the 7 most populated combined statistical areas (CSA) in
North Carolina. A rent cap was of $900 was put in place in order to consider affordable prices at a flat rate across North Carolina; because the level of "affordability" is relative to every city and county, $900 was chosen to maintain a consistent rate that is less than the median rent for
a one-bedroom apartment in the US, which was $1,078 at the end of 2019 (Temple, 2019). In searching for listings, I used apartments.com and apartmentfinder.com and set the listings to
only include one-bedroom or studio floor layouts. I also set the listings county-by-county for those included in each CSA. Once these settings produced the listings, I created a set that all had studios and/or one-bedrooms available on websites of their own. Any organization that
offered apartments without a website and/or email was excluded due to the concern that reaching out to an organization through a third-party website (i.e., Zillow) as opposed to a
direct inquiry would potentially alter response rates. The final sample was comprised of 350 housing organizations. Random selection was utilized within each county so that each auditor sent the same number of emails to organizations within each area. The listings provided by the
housing organizations were located in urban or suburban settings and all within a county containing a major North Carolina city (i.e., Raleigh, Charlotte, Wilmington).
Study design and procedure
All six of the auditors posed as potential tenants and wrote emails to housing organizations
inquiring about rental properties. The email used signaling techniques in order to
communicate race and health status, and the full emails can be found in Appendix A. All three
emails include mention of a parole officer and a case manager. For the emails including health conditions, the case manager is provided to assist in the signaling of a health condition. The emails reporting no health condition include the case manager in order to remain consistent in
the email content. The emails signaling mental health were kept broad in order to prevent variation with mental illnesses that carry different stigma along with them. For example,
All emails were sent out from 8:00-11:00 AM in order to prevent variation with the
housing organizations viewing and responding to emails outside of hours of operation. Also, the emails were sent out on Monday, Tuesday, and Wednesday of the same week for the same
reason as the time of day. On Monday, 20 emails were sent out from each auditor for a total of 120. On Tuesday, the two auditors reporting no health conditions sent out 20 emails each while the four remaining auditors reporting health conditions each sent out 19. All six auditors
sent 19 emails on Wednesday, totaling 59 emails for each of the auditors reporting no health condition and 58 for each of the auditors reporting mental illness or asthma, for a total of 350
emails sent. A lot of the housing organizations provided "Contact Us" forms on their websites as opposed to email addresses, to which I inputted the same text as the email drafts. For forms that required phone numbers, I added the line "(prefer email to call)" at the bottom of the
message to prevent an influx of calling as opposed to emails. Any requirement on the form to include a current address was filled in as "N/A." There was no order in terms of CSAs to which
I sent out the emails – the order was dictated by another random selection after the randomization of email accounts linked to each housing organization. Because all email responses were collected as data, no further correspondence took place. The IRB approval for
this study allows for the use of the housing organizations as audit participants, but with the stipulation that there are not multiple forms of contact.
The emails were coded into a spreadsheet that aggregated the various responses and categorized them into a dichotomous "positive or negative." A positive response corresponds with an apparent willingness on behalf of the housing organization to consider the potential
tenant, while negative responses indicate unwillingness. The criteria for organizing responses into positive and negative categories were inspired by an audit study that analyzed subtle
discrimination among landlords with respect to race and the use of language in emails (Hanson & Hawley, 2011). The study aggregated positive and negative keywords to an
extensive level, given its focus within the study, but inspired the method I utilized for placing
emails as positive or negative. Positive emails were chosen based on positive keywords, such as polite phrases like "Thanks, please call, sincerely, etc.". In contrast, negative use of language
were examined on the proportion of positive and negative phrases and words utilized, and
were placed in their respective categories based on which form of language was used more. Given that each email account was given a Google Voice number, all voicemails received were
automatically transcribed into email form and were judged based on the same criteria mentioned. Nonresponses were also recorded in total for each auditor and are central to the data analysis.
Data Analysis
Descriptive statistics are provided which describe the breakdown of auditor characteristics and emails sent in addition to the locations of the housing organizations. These numbers can be
found in Tables 1 & 2. The primary research question was answered by calculating the total response rate and positive response rate for the samples of auditors reporting either some or
no health condition. The same process was replicated for each of the following questions regarding the potential difference in form of health condition (mental illness or asthma), and then controlling for race by general health condition and form of health condition. I then
examined whether and how the results by health status varied geographically by comparing the results across the three most populated CSAs in the sample of housing organizations. Each set
of response rates are illustrated using basic bar graphs. Once all results are reported, I conducted z-tests to determine if there is a statistical difference between the means of each group. The p-values for each set of responses are recorded in Appendix B.
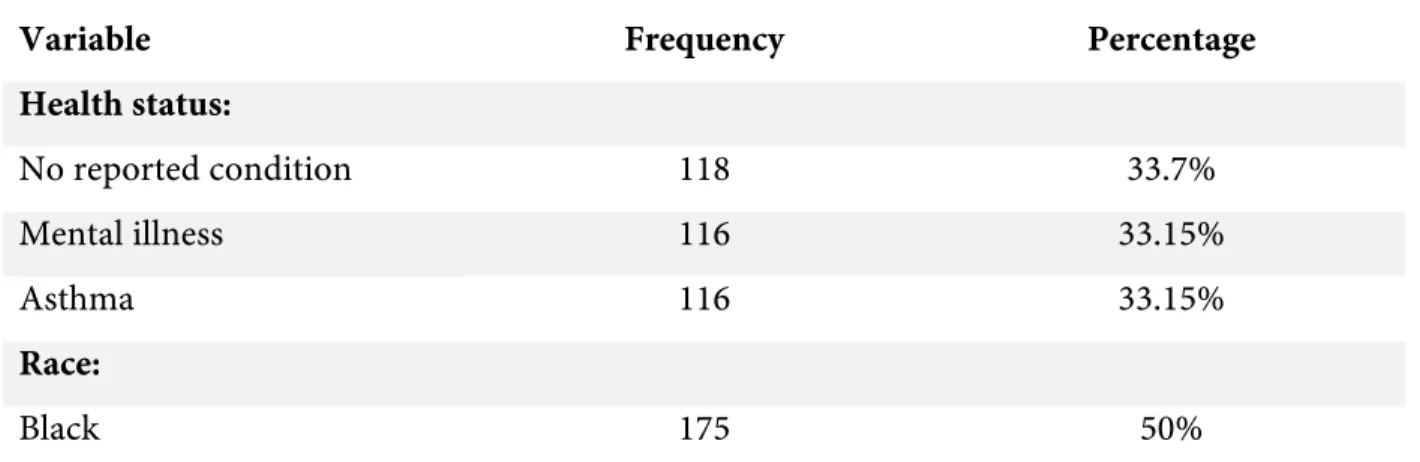
Table 1 - Descriptive statistics of auditors
Variable Frequency Percentage
Health status:
No reported condition 118 33.7%
Mental illness 116 33.15%
Asthma 116 33.15%
Race:
White 175 50%
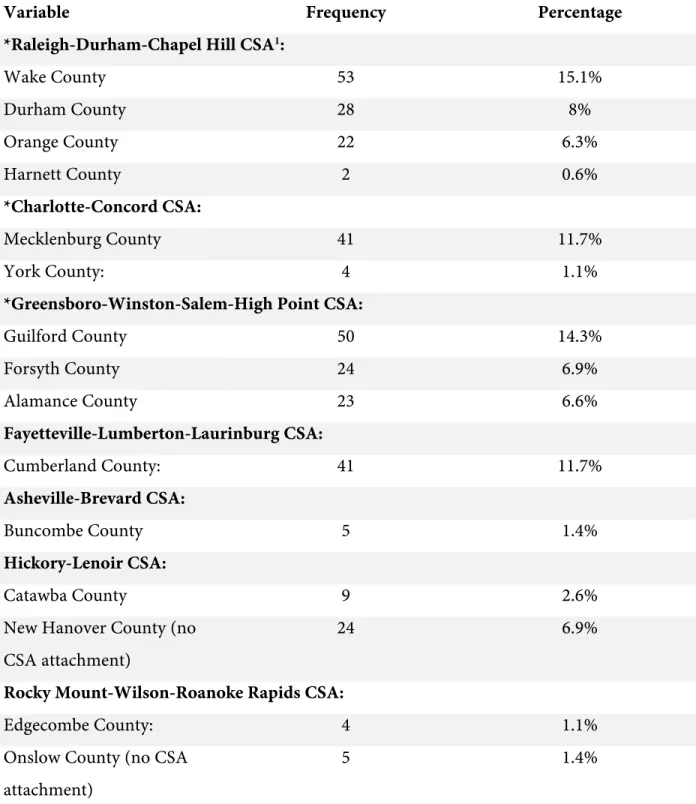
Table 2 - Distribution of housing organizations by common statistical area (CSA) and county
Variable Frequency Percentage
*Raleigh-Durham-Chapel Hill CSA1:
Wake County 53 15.1%
Durham County 28 8%
Orange County 22 6.3%
Harnett County 2 0.6%
*Charlotte-Concord CSA:
Mecklenburg County 41 11.7%
York County: 4 1.1%
*Greensboro-Winston-Salem-High Point CSA:
Guilford County 50 14.3%
Forsyth County 24 6.9%
Alamance County 23 6.6%
Fayetteville-Lumberton-Laurinburg CSA:
Cumberland County: 41 11.7%
Asheville-Brevard CSA:
Buncombe County 5 1.4%
Hickory-Lenoir CSA:
Catawba County 9 2.6%
New Hanover County (no CSA attachment)
24 6.9%
Rocky Mount-Wilson-Roanoke Rapids CSA:
Edgecombe County: 4 1.1%
Onslow County (no CSA
attachment)
5 1.4%
Results
Response by health status
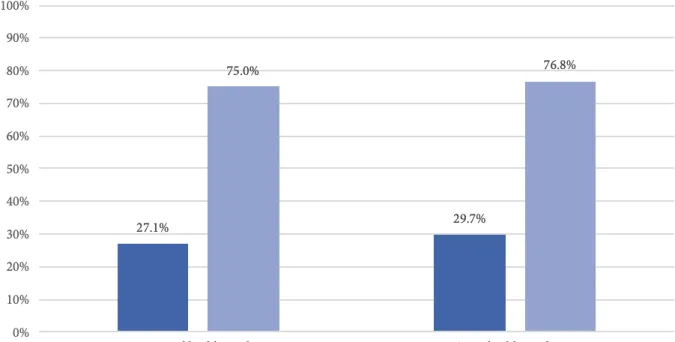
Figure 1 addresses the question of if there is a difference in housing opportunities for formerly incarcerated individuals with or without health problems. For the upcoming figures, total response rate is calculated by dividing the total responses from the given sample of auditors by
the total number of emails sent out. This same method of calculation is conducted for the following rates as well. For the sample of auditors reporting no health problems, there was a
positive response rate of 75% based on a total response rate of 27.1%. For the sample of
auditors who reported health problems, there was a positive response rate of 76.8% based on a total response rate of 29.7%, both which are surprisingly higher than the rates of auditors
reporting no health issues. Although the differences are small, it still stands out as results that are contradictory to initial expectations. The z-test for the total responses resulted in a p-value
of 0.70 meaning that the differences are not statistically different. The same can be said for the difference in positive response rates, as the p-value here was 1.
Figure 2 addresses the question of if there is a difference in housing opportunities for formerly
incarcerated people by mental illness and asthma. For the sample of auditors that reported mental illness, they received a positive response rate of 77.8% based on a total response rate of
31%. For auditors reporting asthma, they received a positive response rate of 75.8% based on a total response rate of 28.4%. The auditors reporting mental health issues showed to have higher positive and total response rates by a slight margin. Again, with these small differences,
it still stands out that the sample of auditors reporting mental illness fared better in both positive and total response rates than those reporting asthma. The p-value for the difference in
total response rates was 0.77 and 1 for the difference in positive response rates, indicating no statistical difference.
Response by race
Next, I examined whether there is a difference in housing opportunities by race for formerly incarcerated people with health problems. However, I begin by combining those in all health
categories into the binary categories of race. Figure 3 address the question of if there is a difference in housing opportunities by race alone. For the sample of White auditors, they received a positive response rate of 83.9% based on a total response rate of 35.4%. The Black
auditors received a positive response rate of 64.1% based on a total response rate of 22.3%. These results suggest that there is a difference in housing opportunities based on race alone.
The positive response rates show a difference of almost 20 percentage points, in which the Black auditors receive a much lower rate than the White auditors. This is based on the set of total response rates in which the White auditor received a rate of about 13 percentage points
higher than the Black auditors. The z-test for the set of total response rates here gave a p-value of 0.009, indicating that the difference is statistically significant. The difference in positive
response rates here is also statistically different with a p-value of 0.04.
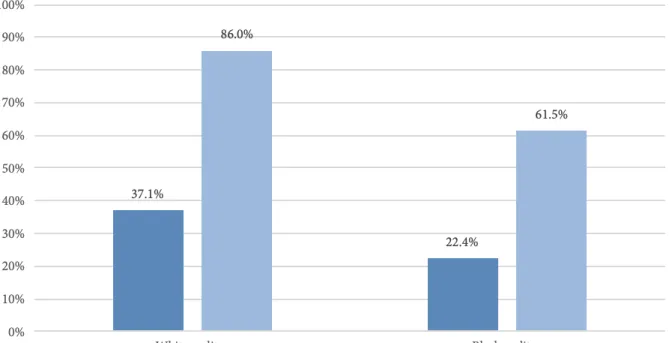
Next, I analyzed whether there may be a difference in housing opportunities for formerly
incarcerated individuals on the basis of race within the sample of auditors reporting some health condition. The White auditors reporting some health condition had a positive response rate of 86% based on a total response rate of 37.1%. The Black auditors reporting some health condition had a positive response rate of 61.5% based on a total response rate of 22.4%. The results
indicate that the racial difference in response rates for those reporting some health condition does not vary greatly compared to the differences not including health. The positive response rates are similar to the previous rates, as there is a difference of about 15 percentage points with the Black auditors receiving a lower rate. These positive response rates are based on total response rates that differ by about 24.5 percentage points, again with the Black auditors receiving less. It appears that White auditors reporting some health condition received slightly higher response rates than the overall set of White auditors. The Black auditors reporting some health condition received a slightly lower positive response rate than the overall set of Black auditors. The z-test for the total response rates here resulted in a p-value of 0.02 making it statistically different. The difference in positive response rates here is also statistically different with a p-value of 0.04.
Then, I examined whether there was a difference in housing opportunities for formerly
incarcerated individuals by race within the four auditors reporting either mental illness or asthma. This involves comparing the total and positive response rates between the pairs of
auditors reporting mental illness and then the two reporting asthma. The White auditor reporting mental illness received a positive response rate of 83.3% based on a total response rate of 41.4%. The Black auditor reporting mental illness received a positive response rate of
66.7% based on a total response rate of 20.7%. The Black auditor received a total response rate of about 20 percentage points less than the White auditor, and a positive response rate of 16.6
percentage points lower than the White auditor. The difference in total response rates was statistically different with a p-value of 0.027, whereas the difference in positive response rates was insignificant with a p-value of 0.48.
Last, I analyzed whether there was a difference in housing opportunities between the Black and
White auditors reporting asthma. The White auditor reporting asthma received a positive response rate of 89.5% based on a total response rate of 32.8%. The Black auditor reporting
asthma received a positive response rate of 57.1% based on a total response rate of 24.1%. The difference between the positive response rates here is larger than the preceding positive
response rates between the two races, at about 32 percentage points lower for the Black auditor
reporting asthma. These results show that the positive response rate for the Black auditor reporting asthma is nearly 10 percentage points lower than the Black auditor reporting mental
illness, albeit with a slightly higher total response rate. It also appears that the White auditor reporting mental illness fared better than the White auditor reporting asthma in total response rate, while the White auditor reporting asthma did slightly better in positive response rate
compared to its mental illness counterpart. The slight difference in total response rates was not statistically significant with a p-value of 0.41. The z-test testing the difference in positive
response rates resulted in a p-value of 0.08 which is not statistically different, albeit very close.
Response by CSA (Combined Statistical Area)
The last set of data examined extends the research question to whether potential
discrimination may vary geographically by CSA. In order to address this question, I examine
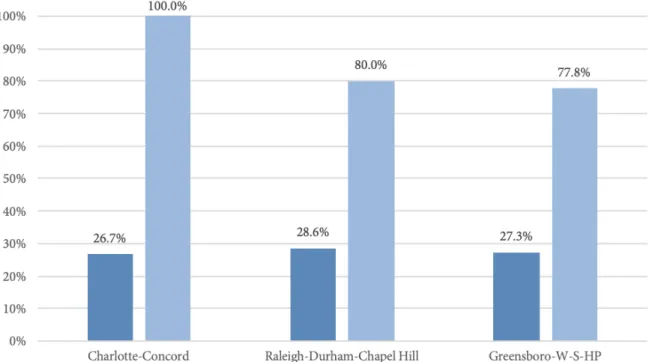
the positive and total response rates between the auditors reporting either some or no health condition across the three most populated CSAs – Charlotte-Concord, Raleigh-Durham-Chapel Hill, and Greensboro-Winston-Salem-High Point. I begin by analyzing the response
rates for those reporting no health condition across the three CSAs. First, it is important to point out that while the positive response rate for Charlotte-Concord is 100%, it is based on a
sample size of four total responses which were all positive. The auditors reporting no health conditions in the Raleigh-Durham-Chapel Hill CSA received a positive response rate of 80% based on a total response rate of 28.6%. The auditors reporting no health conditions within the
Greensboro-Winston-Salem-High Point CSA received a positive response rate of 77.8% based on a total response rate of 27.3%. While this CSA received the lowest positive response rate, it
is only marginally less than the positive response rate for Raleigh-Durham-Chapel Hill. None of the differences below were statistically difference.
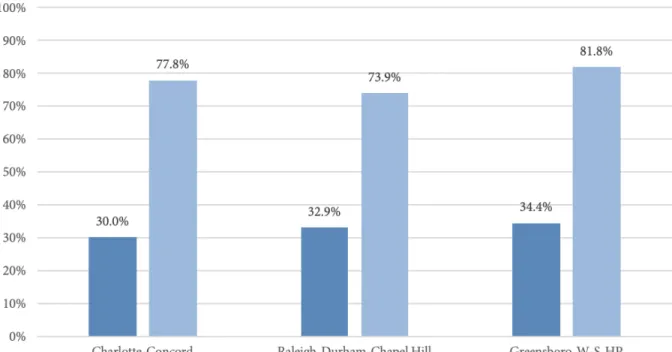
Next, I analyzed the response rates for the auditors reporting some health condition within the
three CSAs. The auditors reporting some health condition in the Charlotte-Concord CSA received a positive response rate of 77.8% based on a total response rate of 30%. The auditors
in the Raleigh-Durham-Chapel Hill CSA received a positive response rate of 73.9% based on a total response rate of 32.9%. Finally, it appears that the auditors reporting some health
condition within the Greensboro-Winston-Salem-High Point CSA received positive and total
response rates higher than the preceding two sets. These auditors received a positive response rate of 81.8% based on a total response rate of 34.4%, both of which are marginally higher than
the rates from the Charlotte-Concord and Raleigh-Durham-Chapel Hill CSAs. Once again, none of the differences were statistically different.
Discussion
This study adds to the body of literature using audit studies to examine differential treatment
in the housing market for formerly incarcerated individuals. A prior criminal record is a well-documented determinant for the inaccessibility of housing. The purpose of this paper was to consider how different health statuses may affect the level of housing opportunities for
formerly incarcerated individuals. Race was also taken into consideration, which opened the possibility for an interaction between race and health that also may alter housing
opportunities. I collected first-hand data by sending emails to housing providers using fictious testers who exhibited different characteristics between race and health status. Email responses were compiled and categorized as positive or negative, and were then analyzed between the six
auditors to address the research question. My initial expectations were that the signaling of either mental or physical health conditions would lead to lower levels of housing opportunities
for individuals with a felony record. I also hypothesized that race would be another dimension of differential treatment, in which the Black auditors would receive a lower amount of total and positive response rates.
Contrary to my initial expectations, the results indicated no significant differences between some or no health status on the level of housing opportunities received. Nor did the results
point towards significant differences in housing opportunities between auditors reporting asthma and mental illness. In fact, some of the total and positive response rates for those reporting some health condition were marginally higher than the response rates for those
reporting no health condition, as found in Figure 1. When examining the response rates for those reporting either mental illness or asthma, it appeared that those reporting mental illness
had slightly higher response rates than those reporting asthma. However, the differences mentioned are very slight and none are statistically different. These results addressed whether health statues alone played a role in potentially affecting the level of housing opportunities for
What was apparent throughout this study were differences in the response rates for
auditors on the basis of race. The overall difference in housing opportunities here shows a significant disparity in response rates before taking health into consideration, as shown in
Figure 3. The same goes for the set of analyses taking health status into consideration, although the results do not indicate an interactional effect between race and health status. Figures 4, 5, and 6 all present similar trends in response rates compared to the overall racial differences.
The auditor that received the lowest positive response rate among the six auditors was the Black auditor reporting mental illness, but only by a slight margin compared to the other two
Black auditors. When comparing the auditors of the same health category across race, the study indicates significant differences in response rates. What the results illustrated in Figures 3-6 suggest is that housing opportunities are affected by race, but with no significant
interactions with health status.
The analysis of the response rates within the three most populated CSAs do not suggest any
significant variation between the categories of some or no health condition. Small sample sizes largely contributed to a lack of statistical differences, especially with the case of the Charlotte-Concord CSA. The results here reflect the initial finding that health status does not play a role
in causing housing discrimination for formerly incarcerated individuals. Since the CSAs reflect the three most populated areas and cities in North Carolina, this lack of variation may
potentially be due to the similarities that underlie these areas. If CSAs with different characteristics were analyzed – perhaps in income level or in their population of formerly incarcerated individuals – there may have been more potential for differential treatment.
The central research question of this study asks whether formerly incarcerated individuals with a mental or physical illness receive different levels of housing opportunities than those
who are healthy. Based by the results addressing this question, the paper gives no significant evidence that a health problem affects the accessibility for housing. While it appears that health status does not affect the behavior of housing organizations, there are multiple possibilities as
to why these results were reached. The initial inference here is that housing organizations are not swayed by the potential risks that a tenant with a health condition may bring, especially in
their offer of housing based on a health problem may in fact be discriminatory, making the
housing opportunities unaffected. These results may also be caused by the overarching stake that housing organizations place on a criminal record in whether or not they would be willing
to take on a tenant. Perhaps the health concerns fall out of focus when these organizations are faced with a criminal record, given the current knowledge of housing discrimination and criminal backgrounds.
Audit studies on the collateral consequences of a criminal record have detected racial discrimination in which minorities face additional challenges in securing needs like
employment and housing (Pager, 2003; Hanson & Hawley, 2011). This study is able to add to this literature by providing evidence of differential treatment on the basis of race in the housing market for formerly incarcerated individuals. While the focus on this study was to
analyze the effect of health conditions, the area in which the paper does successfully capture discrimination is on the basis of race alone. Differential treatment is evidenced in each analysis
comparing the auditors of each race regardless of the health status being analyzed, consistent with preceding literature. However, the detection of racial discrimination in the housing market for formerly incarcerated individuals is not unanimous among previous audit studies
(Helfgott, 1997; Thacher, 2008; Evans et al., 2019). The results of this study suggest that a formerly incarcerated Black individual experiences more challenges in attaining rental housing
than a White individual with the same background. Given that findings from previous studies have suggested both none and some cases of differential treatment on the basis of race, this study contributes new evidence for the presence of racial discrimination in housing for
formerly incarcerated individuals.
This study has several limitations. First, the use of signaling mental illness as a whole does
not address the potential for differential treatment across the spectrum of psychological disorders. It may be possible that housing opportunities for formerly incarcerated individuals can be different for those reporting a severe disorder like schizophrenia as opposed to
depression or anxiety. The use of asthma as a way to signal physical illness also constrains the response rates from illustrating the housing opportunities available to formerly incarcerated
different, especially with other common illnesses within the formerly incarcerated population
like diabetes or HIV. This study also does not address the potential for differential treatment with respect to other races/ethnicities. Given that this study examines race by utilizing Black
and White names in the emails, the results do not include any race or ethnicity outside of these two, which may potentially lead to other significant results. Another limitation stems from the use of a static rent cap used to create the sample of housing organizations across North
Carolina. Every city has a different threshold of what is considered affordable housing. For instance, a listing in Charlotte for $900 a month likely provides a different living situation than
a $900 listing in a more impoverished areas in the state like Rocky Mount. Thus, the sample of housing organizations includes listings within various types of communities which could possibly contribute to differences in housing opportunities.
Future research should continue to explore the relationship between health status and the housing barrier by looking deeper into specific facets of health. Studies could look into housing
opportunities for formerly incarcerated individuals with a focus on various mental illnesses, such as the potential differences with disorders of varying levels of severity. The same could go for physical illnesses, as knowledge of housing opportunities for individuals with a variety of
physical health problems would be valuable to the literature. Examination into the common illnesses of formerly incarcerated individuals, such as diabetes, HIV, or high blood pressure,
and their effects on housing opportunities way expose cases of differential treatment that the present study did not address. Another topic of future research is further analysis on the effect of race & ethnicity on housing opportunities for reentering individuals. Studies could replicate
or take inspiration from previous audit studies examining criminal and racial discrimination in order to provide valuable knowledge on the topic of housing discrimination for the formerly
incarcerated. Further analysis can be conducted on the effect of different types of communities and cities on the level of housing opportunities for the reentry population. The sample of housing organizations can include locations with different levels of racial composition, the
formerly incarcerated population, or places with various levels of median income. With the limitations of the present study as well as the pressing situation of health in the formerly
Conclusion
Housing remains a top priority for individuals returning from incarceration. However, this
fundamental necessity is often out-of-reach for people who have been involved with the justice system due to the stigma of a criminal record. Preceding literature does not provide much evidence of whether or not health status plays a role in housing discrimination. Given the high
prevalence of physical and mental health conditions in the reentry population, this study asks the question of if health status does indeed play a role in the housing discrimination faced by
the formerly incarcerated population. I have been unable to demonstrate that health status plays a role in making housing less accessible for reentering individuals. However, the results highlight significant differences in the amount of housing opportunities received on the basis
of race. These differences suggest that formerly incarcerated Black individuals face more of a challenge in acquiring housing than White applicants with the same criminal and health
background. The racial disparity evidenced in this study is consistent with preceding literature on the collateral consequences of a criminal record, and furthers the discussion on the
presence of racial discrimination in the housing market for reentering individuals (Pager,
2003; Hanson & Hawley, 2011). The inaccessibility of housing for people with criminal records traps individuals within the justice system even after release, which contributes to high rates of
physical and psychological issues within this population (“Homelessness & Health,” 2019; Bronson & Berzofsky, 2017). Although this thesis does not provide evidence of lower housing opportunities for people with health problems and a criminal record, the current state of
References
Alexander, M. (2010). The New Jim Crow: Mass Incarceration in the Age of Colorblindness.
New Press.
Alper, M., Durose, M., & Markman, J. (2018). 2018 Update on Prisoner Recidivism: A 9-Year
Follow-up Period (2005-2014). Bureau of Justice Statistics; U.S. Department of Justice.
Retrieved from https://www.bjs.gov/content/pub/pdf/18upr9yfup0514.pdf
Bassuk, E., Rubin, L., & Lauriat, A. (1984). Is Homelessness a Mental Health Problem?. The
American Journal of Psychiatry, 141(12), 1546–1549.
Bronson, J., & Berzofsky, M. (2017). Indicators of Mental Health Problems Reported by
Prisoners and Jail Inmates, 2011-12. Bureau of Justice Statistics; U.S. Department of
Justice. Retrieved from https://www.bjs.gov/content/pub/pdf/imhprpji1112.pdf
Cain, H. L. (2003) Housing our criminals: Finding housing for the formerly incarcerated
individual in the twenty-first century. Golden Gate University Law Review, 33, 131–171.
Carey, C. (2005). No Second Chance: People with Criminal Records Denied Access to Public
Housing. University of Toledo Law Review, 36(3), 545-594
Couloute, L. (2018). Nowhere to Go: Homelessness among formerly incarcerated people. Prison
Policy Initiative. Retrieved from https://www.prisonpolicy.org/reports/housing.html
Crabtree, C. (2018). An Introduction to Conducting Email Audit Studies. Audit Studies:
Behind the Scenes with Theory, Method, and Nuance, 103-117
Criminalization of Homelessness. (n.d.) National Coalition of the Homeless. Retrieved from
https://nationalhomeless.org/issues/civil-rights/
Crowe, C., Hardill K. (1993) Nursing research and political change: the street health report.
Don’t Count on It: How the HUD Point-in-Time Count Underestimates the Homelessness Crisis
in America. (2017). National Law Center on Homelessness and Poverty. Retrieved from
https://nlchp.org/wp-content/uploads/2018/10/HUD-PIT-report2017.pdf
Evans, D., Blount-Hill, KL., Cubellis, M. (2019) Examining housing discrimination across race,
gender and felony history. Housing Studies, 34(5), 761-778
Evans, G., Wells, N., & Moch, A. (2003). Housing and Mental Health: A Review of the
Evidence and a Methodological and Conceptual Critique. Journal of Social Issues, 59(3),
475–500.
Felony Disenfranchisement: A Primer. (2016). The Sentencing Project. Retrieved from
https://www.sentencingproject.org/wp-content/uploads/2015/08/Felony-Disenfranchisement-Primer.pdf
Fontaine, J., & Biess, J. (2012). Housing as a Platform for Formerly Incarcerated Persons. What
Works Collaborative; Urban Institute. Retrieved from
https://www.issuelab.org/resources/12966/12966.pdf
Formerly Incarcerated People Are Nearly 10 Times More Likely to be Homeless. National Low
Income Housing Coalition. (2018). Retrieved from
https://nlihc.org/resource/formerly-incarcerated-people-are-nearly-10-times-more-likely-be-homeless
Gaddis, S. (2018). An Introduction to Audit Studies in the Social Sciences. Audit Studies:
Behind the Scenes with Theory, Method, and Nuance, 3-44.
Garland, B., Wodahl, E. J., & Mayfield, J. (2010). Prisoner reentry in a small metropolitan
community: Obstacles and policy recommendations. Criminal Justice Policy Review, 22,
Geller, A. and Franklin, A.W. (2014). Paternal Incarceration and the Housing Security of
Urban Mothers. Journal of Marriage and Family, 76(2), 411-427.
Goff, A., Rose, E., Rose, S., Purves, D. (2007) Does PTSD Occur in Sentenced Prison
Populations? A Systematic Literature View. Criminal Behavior and Mental Health, 17,
152-162
Greenburg, G.A., Rosenheck, R.A. (2008) Jail Incarceration, Homelessness, and Mental Health:
A National Study. Psychiatric Services, 59(2), 170-177.
Hammett, T. M., Roberts, C., & Kennedy, S. (2001). Health-Related Issues in Prisoner Reentry.
Crime & Delinquency, 47(3), 390–409.
Hanson, A. & Hawley, Z. (2011) Do landlords discriminate in the rental housing market?
Evidence from an internet field experiment in US cities. Journal of Urban Economics,
70(2–3), 99–114.
Helfgott, J. (1997). Ex-offender needs versus community opportunity in Seattle, Washington.
Federal Probation, 61, 12–24.
Hill, G., & Hill, K. (2002). The People’s Law Dictionary: Taking the Mystery out of Legal
Language. MFJ Books.
Hogan, B. & Berry, B. (2011) Racial and ethnic biases in rental housing: An audit study of
online apartment listings. City & Community, 10(4), 351–372.
Homelessness - What We Know. (n.d.). Reentry and Housing Coalition. Retrieved from
http://www.reentryandhousing.org/public-housing
Homelessness & Health: What’s the Connection? (2019). National Health Care for the
Homelessness Council. Retrieved from
Hwang, S. (2001). Homelessness and health. Canadian Medical Association Journal, 164(2),
229–233.
Kreiger, J., & Higgins, D. (2002). Housing and Health: Time Again for Public Health Action.
American Journal of Public Health, 92, 758–768.
Kulkarni, S.P., Baldwin, S., Lightstone, A.S. et al. (2010) Is Incarceration a Contributor to
Health Disparities? Access to Care of Formerly Incarcerated Adults. Journal of
Community Health, 35,268–274.
La Vigne, N. G., Thomson, G. L., Visher, C., Kachnowski, V. & Travis, J. (2003). A portrait of
prisoner reentry in Ohio. Urban Institute. Retrieved from http://www.urban.
org/sites/default/files/alfresco/publication-pdfs/410891-A-Portrait-of-Prisoner-Reentry-in-Ohio.PDF.
Leasure, P., Martin, T., (2017). Criminal records and housing: an experimental study. Journal
of Experimental Criminology, 13, 527-535
Lee, B. A., Tyler, K. A. & Wright, J. D. (2010) The new homelessness revisited, Annual Review
of Sociology. 36, 501–521.
Link, N, Ward, J, Stansfield, R. (2019). Consequences of mental and physical health for
reentry and recidivism: Toward a health-based model of desistance. Criminology, 57(3),
544– 573.
Mallik-Kane, K., & Visher, C. (2008). Health and Prisoner Reentry: How Physical, Mental, and
Substance Abuse Conditions Shape the Process of Reintegration. Urban Institute Justice
https://www.urban.org/sites/default/files/publication/31491/411617-Health-and-Prisoner-Reentry.PDF
Mallik-Kane, K., Paddock, E., & Jannetta, J. (2018). Health Care after Incarceration: How Do
Formerly Incarcerated Men Choose Where and When to Access Physical and Behavioral
Health Services? Urban Institute; National Institute of Corrections. Retrieved from
https://www.urban.org/sites/default/files/publication/96386/health_care_after_incarcer
ation.ppd
McKernan, P. (n.d.). Homelessness and Prisoner Re-Entry: Examining Barriers to Housing.
Volunteers of America. Retrieved from
https://www.voa.org/homelessness-and-prisoner-reentry
Middlemass, K. (2017). Convicted and Condemned: The Politics and Policies of Prisoner
Reentry. New York University Press. 81, 95-95
Munro, N., & Reason, C. (2018). Homelessness: why new statistics are probably underestimating
the problem. The Conversation. Retrieved from
https://theconversation.com/homelessness-why-new-statistics-are-probably-underestimating-the-problem-108840
No Second Chance: People with Criminal Records Denied Access to Public Housing. (2012)
Human Rights Watch. Retrieved from
https://www.hrw.org/report/2004/11/18/no-second-chance/people-criminal-records-denied-access-public-housing
O’Brien, P. (2001). “Just like baking a cake”: Women describe the necessary ingredients for
successful reentry after incarceration. Families in Society: The Journal of Contemporary
Social Services, 82, 287–295.
Pedersen, T. (2019). Ex-Prisoners Who Face Barriers to Re-Entry Prone to Poor Mental,
Physical health. PsychCentral. Retrieved from
https://psychcentral.com/news/2019/12/09/ex-prisoners-who-face-barriers-to-re-entry-prone-to-poor-mental-physical-health/152474.html
Prisoners and Prisoner Re-Entry. (n.d.). Office of Justice Programs; U.S. Department of
Justice. Retrieved from https://www.justice.gov/archive/fbci/progmenu_reentry.html
Rabuy, B., & Kopf , D. (2015). Prisons of Poverty: Uncovering the pre-incarceration incomes
of the imprisoned. Prison Policy Initiative. Retrieved from
https://www.prisonpolicy.org/reports/income.html
Roman, C. G. (2004) A roof is not enough: Successful prisoner reintegration requires
experimentation and collaboration. Criminology and Public Policy, 3(2), 161–168.
Roman, C. G. (2017). Community reintegration among prisoners with child support
obligations: An examination of debt, needs, and service receipt. Criminal Justice Policy
Review, 28(9), 896–917.
Roman, C. G. & Travis, J. (2004) Taking stock: Housing, homelessness, and prisoner reentry.
Urban Institute. Retrieved from
https://www.urban.org/sites/default/files/publication/58121/411096-Taking-Stock.PDF
Roth, D., & Bean, J. (1986). The Ohio study: A comprehensive look at
homelessness. Psychosocial Rehabilitation Journal, 9(4), 31–38.
Sawyer, W. (2017). Food for thought: Prison food is a public health problem. Prison Policy
Initiative . Retrieved from https://www.prisonpolicy.org/blog/2017/03/03/prison-food/
Sawyer, W., & Wagner, P. (2020). Mass Incarceration: The Whole Pie 2020. Prison Policy
Sokoloff, N., Schenck-Fontaine, A. (2017). College programs in prison and upon reentry for
men and women: a literature review. Contemporary Justice Review, 20(1), 95-114.
Stefancic, A., Tsemberis, S. (2007). Housing First for Long-Term Shelter Dwellers with
Psychiatric Disabilities in a Suburban County: A Four-Year Study of Housing Access
and Retention. The Journal of Primary Prevention, 28, 265–279.
Stewart, R., & Uggen, C. (2020). Criminal records and college admissions: A modified
experimental audit. Criminology, 58(1), 156–188.
Stuntz, W. (2001). The Pathological Politics of Criminal Law. Michigan Law Review, 7(2),
505-600
Sugie, N. F. (2018). Work as foraging: A smartphone study of job search and employment after
prison. American Journal of Sociology, 123(5), 1453–1491.
Temple, S. (2019). America’s 2019 Rental Market in Review: Did Renters Pay More? ABODO.
Retrieved from https://www.abodo.com/blog/2019-annual-rent-report/
Thacher, D. (2008). The rise of criminal background screening in rental housing. Law & Social
Inquiry, 33, 5–30.
Tress, W. (2009). Unintended Collateral Consequences: Defining Felony in the Early American
Republic. Cleveland State University Law Review, 57(3), 461-91
Wagner, P. (2012). Incarceration is not an equal opportunity punishment. Prison Policy
Initiative. Retrieved from https://www.prisonpolicy.org/articles/notequal.html
Wang, E.A., Green, J. (2010). Incarceration as a key variable in racial disparities of asthma
Wang, EA, Wildeman C. (2001) Studying Health Disparities by Including Incarcerated and
Formerly Incarcerated Individuals. Journal of the American Medical
Association. 305(16), 1708–1709.
Wheelock, D. (n.d.). Collateral Consequences and Racial Inequality: Felon Status Restrictions
as a System of Disadvantage. Journal of Contemporary Criminal Justice, 21(1), 82–90.
Widra, E. (2017). Incarceration shortens life expectancy. Prison Policy Initiative. Retrieved
from https://www.prisonpolicy.org/blog/2017/06/26/life_expectancy/
Wolff, N., Jacoby, J., Hartwell, S., & Duclos, C. (2005). Understanding community re-entry of
former prisoners with mental illness: a conceptual model to guide new research.
Behavioral Sciences & the Law, 23(5), 689–707.
Yahner, J., Visher, C. (2008) Illinois prisoners’ reentry success three years after release. Urban
Institute. Retreived from
Appendix
Appendix A – Emails sent
White mail auditor with no health condition:
Hello,
I’m writing because I’m interested in renting one of your apartments. Recently I have been released from prison, so I would like to clarify that I have a parole officer and a
case manager who may come into contact with you. Do you have a studio or one-bedroom apartment available to rent starting in the next few months? I’m currently staying with family and can be flexible about move-in dates.
Please let me know what you have available.
Thank you very much, Robert Walsh
White male auditor with a mental health condition:
Hello,
I’m writing because I’m interested in renting one of your apartments. Recently I have been released from prison, so I would like to clarify that I have a parole officer and a
case manager who may come into contact with you, both of whom are also responsible for my mental health treatment. Do you have a studio or one-bedroom apartment
available to rent starting in the next few months? I’m currently staying with family and can be flexible about move-in dates.
Please let me know what you have available.
Thank you very much,