Decreasing Colectomy Rate for Ulcerative Colitis in the United
States Between 2007 and 2016: A Time Trend Analysis
Edward L. Barnes, MD, MPH,
*
,†,‡Yue Jiang,
§Michael D. Kappelman, MD, MPH,
†,‡,¶Millie D. Long, MD, MPH,
*
,†,‡Robert S. Sandler, MD, MPH,
*
,‡Alan C. Kinlaw, PhD,
‖,**,aand Hans H. Herfarth, MD, PhD
*
,†,‡,aBackground: Improved treatment approaches for ulcerative colitis (UC), including novel medications, might reduce the need for colectomy. We performed a retrospective cohort study of adult patients (age 18–64) with UC in the United States to examine time trends for colectomy and biologic use from 2007 to 2016.
Methods: We estimated quarterly rates for colectomy and biologic use using the IQVIA Legacy PharMetrics Adjudicated Claims Database. We used interrupted time series methods with segmented regression to assess time trends with 95% confidence intervals (CIs) for biologic use and colectomy before and after the emergence of newly available biologic therapies in 2014.
Results: Among 93,930 patients with UC, 2275 (2.4%) underwent colectomy from 2007 to 2016. Biologic use rates increased significantly from 2007 to 2016, from 131 per 1000 person-years in 2007 (95% CI, 121 to 140) to 589 per 1000 person-years in 2016 (95% CI, 575 to 604; P < 0.001). Colectomy rates decreased significantly between 2007 and 2016, from 7.8 per 1000 person-years (95% CI, 7.4 to 8.2) to 4.2 per 1000 person-years in 2016 (95% CI, 3.2 to 5.1; P < 0.001). An interruption in 2014 was associated with a positive trend deflection for biologic use (+72 treatments per 1000 person-years per year (95% CI, 61 to 83) and a negative trend deflection for colectomy (–0.76 per 1000 person-years per year; 95% CI, –1.47 to –0.05).
Conclusions: Among commercially insured patients in the United States from 2007 to 2016, biologic use rates increased, colectomy rates de-creased, and both trends were impacted by the interruption in 2014. These findings suggest that new biologic therapies may have contributed to decreased colectomy rates.
Key Words: ulcerative colitis, inflammatory bowel diseases, interrupted time series, administrative claims, colectomy
INTRODUCTION
In the past 15 years, the number of medications avail-able for the treatment of ulcerative colitis (UC) has increased significantly. These new therapies act through multiple mech-anisms, and biologic therapies in particular are being utilized earlier in the disease course than in prior eras of treatment for UC. If these new approaches are effective in altering the clin-ical course of disease, the need for colectomy may decrease or be delayed.
applyparastyle "fig//caption/p[1]" parastyle "FigCapt"
Received for publications September 10, 2019; Editorial Decision September 18, 2019. From the *Division of Gastroenterology and Hepatology, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA; †Multidisciplinary Center for Inflammatory Bowel Diseases, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA; ‡Center for Gastrointestinal Biology and Disease, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA; §Department of Biostatistics, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA; ¶Division of Pediatric Gastroenterology and Hepatology, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA; ‖Division of Pharmaceutical Outcomes and Policy, Eshelman School of Pharmacy, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA; **Cecil G. Sheps Center for Health Services Research, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA
aEqual contribution
Supported by: This work was supported by the Nickolas Bunn Boddie, Sr., and Lucy Mayo Boddie Foundation (to E.L.B.), the Crohn’s and Colitis Foundation (grant number 567497 to E.L.B.), and the National Institutes of Health (P30DK034987).
Population-based estimates of the frequency of colec-tomy among patients with UC have varied considerably over time.1 Although early reports of the frequency of colectomy
ranged as high as 20%–45% in patients up to 25 years after diagnosis,1 in other population-based or prospectively enrolled
cohort studies, the risk of colectomy reported was lower.2–4
A recent meta-analysis estimated that the 10-year risk of sur-gery among patients with UC was 15.6%.5 Additionally, the
indication for colectomy appears to have changed over time,
Conflicts of interest: E.L.B.: speaking for AbbVie, Inc.; Y.J.: no disclosures; M.D.K.: consulting for AbbVie, Inc., Eli Lilly; M.D.L.: consulting for Pfizer, AbbVie, Takeda, Janssen, Salix, Valeant, Target Pharmasolutions, Prometheus, UCB; R.S.S.: no disclosures; A.C.K.: no disclosures; H.H.H.: consulting for Alivio, AMAG, Finch, Gilead, Merck, Pfizer, Celltrion, Lycera, Boehringer-Ingelheim, Seres, and Otsuka and research support from Pfizer and Artizan.
Address correspondence to: Edward L. Barnes, MD, MPH, Division of Gastroenterology and Hepatology, University of North Carolina at Chapel Hill, 130 Mason Farm Road, Bioinformatics Building, CB #7080, Chapel Hill, NC 27599-7080 ([email protected]).
with an increasing proportion of colectomies being performed for fulminant colitis or neoplasia compared with medically re-fractory disease.6
The therapeutic landscape for UC is rapidly evolving, with multiple new biologic and small molecule therapies ap-proved since 2014.7, 8 Recent guidelines for the management of
UC advocate for an evaluation of disease activity and an assess-ment of disease prognosis when choosing a therapy,9 perhaps
leading to earlier treatment with biologic therapy. Infliximab, the first biologic therapy to be approved for the treatment of UC, has been associated with decreased rates of colectomy in retrospective and placebo-controlled studies.10–12 It is unknown
whether overall colectomy rates in the United States have been meaningfully impacted by newer biologic therapies or the earlier introduction of biologic therapies into management al-gorithms for UC.13
The primary objective of this study was to evaluate the rates of colectomy for UC over time between 2007 and 2016 among commercially insured patients in the United States. Additionally, we examined trends over time in use of biologic therapies among patients with UC and the rate of colectomy performed for colorectal cancer.
METHODS
Data Source
For this study of colectomy rates in the UC popula-tion, we used the IQVIA Legacy PharMetrics Adjudicated Claims Database, which contains longitudinal, de-identified, individual-level administrative claims for medical, surgical, and prescription drug services in the United States from January 1, 2007, to June 1, 2016. Approximately 100 health plans are included in this data source, with a total of 27,800,023 de-identified individuals represented. In prior published liter-ature, this data source has been reported as representative of the commercially insured population in the United States on a variety of measures, including age, sex, geographic region, and health plan type.14, 15
Patient Selection
We identified adult patients age 18–64 with UC using pre-viously described criteria.15, 16 Briefly, we extracted all claims with
an International Classification of Diseases, 9th revision, Clinical Modification (ICD-9-CM) or ICD, 10th revision, Clinical Modification (ICD-10-CM) diagnosis code for UC (556.x for ICD-9-CM and K51.x for ICD-10-CM) and dispensing/ad-ministration of inflammatory bowel disease (IBD)–specific medications (mesalamine, olsalazine, balsalazide, sulfasala-zine, azathioprine, mercaptopurine, infliximab, adalimumab, certolizumab, golimumab, natalizumab, or vedolizumab). We identified claims for these medications by searching their ge-neric names and anatomical therapeutic chemical codes in the
National Drug Data File (NDDF Plus; First Databank; www.
firstdatabank.com) to ascertain National Drug Codes for
pre-scription dispensation claims and CPT or Healthcare Common Procedure Coding System (HCPCS) codes for biologic proce-dure claims. To classify as having a diagnosis of UC, patients were required to have at least 1 diagnosis code for UC at 3 dis-tinct health care encounters or at least 1 diagnosis code for UC with an accompanying claim for an IBD-specific medication.
Outcome Measures
The primary outcome of interest for this study was the rate of colectomy in patients with UC. We identified colec-tomy based on Current Procedural Terminology (CPT) codes for the first observed operation among 3 types of total colec-tomy procedures: total abdominal coleccolec-tomy (44150, 44151, 44210), total proctocolectomy (44155, 44156, 44212), and total proctocolectomy with ileal pouch–anal anastomosis (IPAA; 44157, 44158, 44211). Similar methods of identifying patients with UC undergoing colectomy have been utilized in prior studies evaluating administrative claims data.17
Second, we measured the rate at which the following bio-logic medications were used by patients with UC: adalimumab, certolizumab, golimumab, infliximab, natalizumab, or vedolizumab. We analyzed use of biologic medications among the entire population of patients with UC and in separate evalu-ations of patients who underwent colectomy and those who did not undergo colectomy during the study period. In the evalua-tion of biologic use among colectomy patients, we evaluated bi-ologic use in the quarter where colectomy occurred. Finally, we analyzed the annual and quarterly frequency of colectomy with a concomitant diagnosis of colorectal cancer during the study period. For the evaluation of colectomy for colorectal cancer among patients with UC, we identified patients with a diag-nosis code of colorectal cancer (ICD-9-CM 153.x-154.8, 230.3, 230.4; ICD-10-CM C18, C19, C20)18 within the 3 months
be-fore colectomy.
Covariates
Available patient demographics included age, sex, and US Census region. We also used the Deyo Modification of the Charlson Comorbidity Index to assess comorbidities that po-tentially influence the likelihood of undergoing colectomy as a therapy for UC.19
Statistical Analysis
diagnosis code. Patient follow-up accrued until disenrollment from a health plan in the database, loss of prescription drug coverage for >1 month, age 65, or June 1, 2016—whichever came first. Among patients who underwent colectomy, fol-low-up for both outcomes was terminated at the time of their colectomy. We excluded patients who had <3 months of contin-uous insurance enrollment after UC diagnosis.
To estimate time trends in rates of biologic use and colec-tomy and to assess how these may have been impacted by newly available biologics, we conducted an interrupted time series analysis. This is a common study design to assess changes in time trends that take place after well-defined population-level changes (eg, new policies or guidelines), when randomization is not possible.20, 21 Three new biologic therapies were approved
for the treatment of UC between 2012 and 2014 (adalimumab, golimumab, and vedolizumab). Given that vedolizumab was approved by the Food and Drug Administration (FDA) in May 2014, we allowed a 6-month lag until the fourth quarter of 2014 as the a priori “interruption” that would mark deflec-tions in trends for biologic use and colectomy. We hypothesized that changes in rates of biologic use and colectomy would be gradual, and therefore did not model discontinuities between segments.22, 23
We used ordinary least squares for segmented linear regres-sion models to estimate linear trends before and after the 2014 interruption, with 95% confidence intervals (CIs). We controlled for confounding by seasonality using a transformed cosine peri-odic function.24, 25 To account for autocorrelated error over time,
we used Durbin-Watson tests (α = 0.05) lagged up to 3 years.26
We performed all data management and analysis using R, version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria), and SAS, version 9.4 (SAS Institute, Cary, NC, USA), including the AUTOREG and MODEL (with %AR macro) procedures to implement segmented regression. The study pro-tocol was exempted by the Institutional Review Board at the University of North Carolina at Chapel Hill.
RESULTS
We identified 93,930 UC patients for this study. Clinical and demographic characteristics of the study population are re-ported in Table 1. Among all patients with UC, 51,393 (55%) were women with a median age of 55 years at the time of last follow-up [interquartile range (IQR) 44–63 years]. The median follow-up time for all patients with UC was 5.5 years (IQR 3.2–7.0 years).
Among 93,930 patients with UC, 2275 (2.4%) under-went colectomy during the study period; 1082 patients (48%) underwent a total abdominal colectomy, 375 (16%) underwent a total proctocolectomy, and 818 (36%) underwent a total proctocolectomy with IPAA. The quarterly rate of colectomy among UC patients decreased between 2007 and 2016, from a peak of 8.4 per 1000 person-years in quarter 4 (Q4)–2007 to a minimum of 4.1 per 1000 person-years in Q2-2016 (Fig. 1).
Impact of Newly Available Biologics for
Ulcerative Colitis
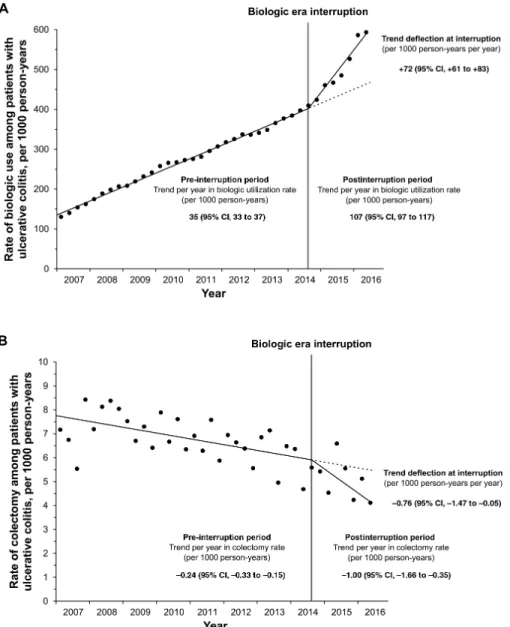
The rates of (A) biologic use and (B) colectomy in pa-tients with UC are presented in Figure 2, along with seasonality-adjusted trend estimates from our interrupted time series analysis. In patients with UC, the rate of biologic use increased over time from 2007 (131 per 1000 person-years; 95% CI, 121 to 140) until the interruption in 2014 (402 per 1000 person-years; 95% CI, 393 to 411). During this pre-interruption period, the increasing trend for biologic use rates was 35 per 1000 person-years per year (95% CI, 33 to 37; P < 0.001). The interruption in 2014 was associated with a further positive trend deflec-tion of +72 per 1000 person-years per year (95% CI, 61 to 83; P < 0.001; null impact of interruption would be 0 deflection). As a result, the postinterruption trend was 107 per 1000 person-years per year (95% CI, 97 to 117; P < 0.001). By 2016, the biologic use rate had reached 589 per 1000 person-years (95% CI, 575 to 604).
The colectomy rate in UC patients decreased by 24% from 2007 (7.8 per 1000 person-years; 95% CI, 7.4 to 8.2) until the interruption in 2014 (5.9 per 1000 person-years; 95% CI, 5.5 to 6.3). During this pre-interruption period, the decreasing trend for colectomy rates was –0.24 per 1000 person-years per year (95% CI, –0.33 to –0.15; P < 0.001). The interruption in 2014 was associated with a further negative trend deflection of –0.76 per 1000 person-years per year (95% CI, –1.47 to –0.05; P = 0.044; null association would be 0 deflection). As a result,
TABLE 1.
Demographic and Clinical Characteristics
of Patients with Ulcerative Colitis in the United States,
IQVIA Legacy PharMetrics Adjudicated Claims Database,
2007–2016
Patients With UC (n = 93,930)
Median IQR
Age at last follow-up, y 55 (44–63) Person-years of follow-up 5.5 (3.2–7.0)
No. %
Male sex 42,537 45.3
Census region
East 23,301 24.8
Midwest 26,599 28.3
South 28,638 30.5
West 15,392 16.4
Charlson Comorbidity Index
0 69,312 73.8
1 16,725 17.8
2 4103 4.4
the postinterruption trend was –1.00 per 1000 person-years per year (95% CI, –1.66 to –0.35; P = 0.005). By 2016, the colec-tomy rate had reached its nadir, at 4.2 per 1000 person-years (95% CI, 3.2 to 5.1). In a subanalysis of patients with UC undergoing colectomy, there was no significant difference in the rate of colectomy performed for colorectal cancer during the study period (Supplementary Fig. 1).
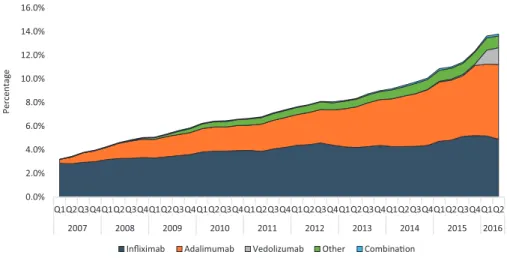
Figure 3 shows the quarterly proportion of patients
with UC who used each biologic. From 2007 to 2016, use of infliximab increased from 2.9% to 4.9% among patients with UC, whereas use of adalimumab increased from 0.3% in 2007 to 2.6% in 2012 to 6.3% in 2016. After FDA approval of vedolizumab in 2014, the proportion of patients with claims for vedolizumab reached a maximum of 1.4% of patients with UC by 2016. Among patients undergoing colectomy, the percentage of patients with a biologic claim in the same quarter increased by a mean of 0.23 absolute percentage points per quarter (linear trend test, P = 0.024) during the study period, whereas the per-centage of patients who did not undergo colectomy with a bi-ologic claim increased by 0.24 absolute percentage points per quarter (linear trend test, P < 0.001) during the study period.
DISCUSSION
In this evaluation of health care claims from more than 90,000 commercially insured patients with UC in the United States, we observed a decrease over time in the rate of colec-tomy between 2007 and 2016. This decrease was demonstrated on multiple analyses, including segmented regression of inter-rupted time series data based on an interruption in 2014 repre-senting the emergence of newly available biologic medications.
During the same time period, rates of biologic use significantly increased among patients with UC. The decrease in colectomy rate during the study period represents one of the first evalu-ations of colectomy patterns in a commercially insured popula-tion in the United States during the current biologic era, when earlier and more aggressive biologic treatment regimens have been advocated.27
Although historically the lifetime risk of colectomy for an individual patient has been estimated to be ≥25% for patients with UC in population-based cohorts,1, 28 more recent analyses
have demonstrated a lower risk of colectomy at 10 years after diagnosis (~15%).5 Thus far, the impact of early and more
ag-gressive use of biologic therapy on long-term outcomes such as colectomy among patients with UC in the United States has not been well established. A prior study from Kaplan et al. demon-strated a decreased rate of elective colectomy among patients with UC in Alberta, Canada, from 1997 to 2009, along with a significant increase in thiopurine (1997–2009) and infliximab use (2005–2009).9 Although a decrease in early colectomy rates
was noted from 1998 to 2005 in a Dutch population-based co-hort when compared with previous years, there were no differ-ences in late colectomy rates between 1991 and 2010.2
In an evaluation from Ontario, Canada, using data from 1995 to 2012, the marketplace introduction of infliximab was not associated with a decrease in colectomy among patients with UC,29 whereas a study from Edmonton, Canada,
demon-strated a decrease in colectomy rate after 2005, which paralleled the increased use of infliximab.30 In our study of a more recent
decade (2007–2016), we have evaluated the early biologic era after the approval of infliximab for the treatment of UC and
FIGURE 1. Incidence rates of colectomy per 1000 person-years among patients with ulcerative colitis in the United States, IQVIA Legacy PharMetrics
the current biologic era, which includes additional anti-TNF therapies and a new mechanism of action in the form of anti-integrin therapy. Additionally, this more modern era of anal-ysis likely incorporates current practice patterns where earlier introduction of biologic therapy into the treatment paradigm is favored if not recommended.27, 31 A recent study from Japan
demonstrated a similar increase in anti-TNF therapy and calcineurin inhibitor use during a similar time period, along with a decrease in surgery rates for UC.32
Our segmented regression analyses demonstrated that colectomy rates decreased from 2007 until the interruption
in 2014, with an even more precipitous decrease noted after the interruption through the end of the study period in 2016. Biologic use rates were also meaningfully impacted by the in-terruption in 2014, after which the increasing trend in biologic use became even steeper. We identified this interruption a priori under the hypothesis that 2014 was a period of introduction and increased utilization of the newest biologic therapies for UC (adalimumab, golimumab, and vedolizumab). Prior studies utilizing administrative claims data from the United States have also demonstrated a consistent rise in biologic use for UC during this same time period.33 Changes in the pattern FIGURE 2. Segmented trends over calendar time for quarterly incidence rates of (A) biologic use and (B) colectomy per 1000 person-years among patients with ulcerative colitis in the United States, IQVIA Legacy PharMetrics Adjudicated Claims Database, 2007–2016. A, Biologic use:
pre-interruption period, P < 0.001; trend deflection at interruption, P < 0.001; postinterruption period, P < 0.001. B, Colectomy: pre-interruption period,
P < 0.001; trend deflection at interruption, P = 0.044; postinterruption period, P = 0.005. Pointwise quarterly rates (circles), pre- and postinterruption
of colectomies among inpatients in the United States during an early portion of this time period have been reported using the HCUP Nationwide Inpatient Sample13; however, this data
source lacks a mechanism to follow patients longitudinally and does not include medications. Whether the trends demon-strated in our study represent a significant shift in the natural history of UC or a temporary delay in surgery with a potential rebound in colectomy rates in the future is unknown. This ques-tion will require vigilant follow-up in future iteraques-tions of this data source and confirmation in other large, population-based longitudinal cohorts.
In our evaluation of the rate of colectomy performed for colorectal cancer among patients with UC, there was no signif-icant change from 2007 to 2016. A recent evaluation of colec-tomy patterns in Helsinki demonstrated a similar decrease in colectomy rate during the current biologic era, without a sig-nificant difference in the percentage of colectomies performed for colorectal cancer or dysplasia.34 There have been several
recent changes in the approach to specific findings on surveil-lance colonoscopy among patients with UC, including recom-mendations from the SCENIC consensus statement,35 in which
surveillance colonoscopy is recommended over colectomy in multiple scenarios. Despite the overall decrease in colectomy rates for UC, the impact of these recommendations and other changes in practice patterns may not be fully captured in ad-ministrative claims data.
The findings of this study are ecological, and they may be influenced by other temporal changes in the clinical treatment of UC. They may be influenced by other temporal changes in clinical treatment of UC. Increased access to IBD specialist care may also improve long-term outcomes among patients with UC.36 This is particularly true when recognizing comorbid
conditions that might also increase the risk of colectomy such as cytomegalovirus infection or nontherapy interventions such as access to a nutritionist, social worker, psychologist, or other
resources. In addition to an overall use of biologic therapies, changes in how these biologic therapies are utilized may also significantly impact outcomes, including an increase in the use of combination therapy,37 treat-to-target strategies,38, 39 and
po-tentially therapeutic drug monitoring.40
This study has several strengths. Our interrupted time series analysis examined a critical 10-year period in the man-agement of UC, during which several new medications became available. We leveraged reliable administrative claims data to analyze a large sample of patients with UC using validated case-finding definitions, records of medication dispensing and infusion, and colectomies. However, it is recognized that di-sease extent influences risk of colectomy,41 and we were unable
to assess for disease extent or severity. Similarly, due to the re-strictions of administrative claims data, we were only able to evaluate those patients with a diagnosis of colorectal cancer be-fore colectomy. There are also limitations when analyzing bio-logic use using administrative claims. There may be incomplete capture of inpatient biologic utilization, given that bundling of inpatient costs may occur. Furthermore, if patients utilized manufacturer assistance programs, biologic use patterns would not be completely captured. Both of these measurement lim-itations would suggest that our estimates of sharp increasing trends for biologic use are underestimations, if they are indeed biased. When identifying patients with UC, we recognize that some patients will potentially continue to have documented di-agnosis codes for UC despite having previously undergone co-lectomy (potentially before enrollment). Although this likely represents a small subset of this population, this could inflate the total number of patients with UC while not representing true eligibility for colectomy. Due to the lack of granularity in this regard in the available claims data, we could not overcome this limitation for this study.
In conclusion, among a large, geographically diverse sample of patients with UC from the United States, we 0.0%
2.0% 4.0% 6.0% 8.0% 10.0% 12.0% 14.0% 16.0%
Q1Q2Q3Q4Q1Q2Q3Q4Q1Q2Q3Q4Q1Q2Q3Q4Q1Q2Q3Q4Q1Q2Q3Q4Q1Q2Q3Q4Q1Q2Q3Q4Q1Q2Q3Q4Q1Q2 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Infliximab Adalimumab Vedolizumab Other Combinaon
Percentag
e
demonstrated a significant decrease in the rate of colectomy from 2007 to 2016, which became more precipitous after the interruption in 2014. The use of biologics increased throughout the study period, and began to increase more rapidly in 2014. Although other nontherapy factors may have contributed to the decrease in colectomy rates, these data suggest that more widespread use of biologic therapy has reduced the rate of colectomy.
SUPPLEMENTARY DATA
Supplementary data are available at Inflammatory Bowel Diseases online.
REFERENCES
1. Fumery M, Singh S, Dulai PS, et al. Natural history of adult ulcerative colitis in population-based cohorts: a systematic review. Clin Gastroenterol Hepatol.
2018;16:343–356.e3.
2. Jeuring SF, Bours PH, Zeegers MP, et al. Disease outcome of ulcerative colitis in an era of changing treatment strategies: results from the Dutch population-based IBDSL cohort. J Crohns Colitis. 2015;9:837–845.
3. Eriksson C, Cao Y, Rundquist S, et al. Changes in medical management and co-lectomy rates: a population-based cohort study on the epidemiology and natural history of ulcerative colitis in Örebro, Sweden, 1963-2010. Aliment Pharmacol Ther. 2017;46:748–757.
4. Parragi L, Fournier N, Zeitz J, et al; Swiss IBD Cohort Study Group. Colectomy rates in ulcerative colitis are low and decreasing: 10-year follow-up data from the Swiss IBD Cohort Study. J Crohns Colitis. 2018;12:811–818.
5. Frolkis AD, Dykeman J, Negrón ME, et al. Risk of surgery for inflammatory bowel diseases has decreased over time: a systematic review and meta-analysis of population-based studies. Gastroenterology. 2013;145:996–1006.
6. Samuel S, Ingle SB, Dhillon S, et al. Cumulative incidence and risk factors for hospitalization and surgery in a population-based cohort of ulcerative colitis.
Inflamm Bowel Dis. 2013;19:1858–1866.
7. Feagan BG, Rutgeerts P, Sands BE, et al; GEMINI 1 Study Group. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med.
2013;369:699–710.
8. Sandborn WJ, Su C, Sands BE, et al; OCTAVE Induction 1, OCTAVE Induction 2, and OCTAVE Sustain Investigators. Tofacitinib as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2017;376:1723–1736.
9. Kaplan GG, Seow CH, Ghosh S, et al. Decreasing colectomy rates for ul-cerative colitis: a population-based time trend study. Am J Gastroenterol.
2012;107:1879–1887.
10. Sandborn WJ, Rutgeerts P, Feagan BG, et al. Colectomy rate comparison after treatment of ulcerative colitis with placebo or infliximab. Gastroenterology. 2009;137:1250–1260; quiz 1520.
11. Aratari A, Papi C, Clemente V, et al. Colectomy rate in acute severe ulcerative colitis in the infliximab era. Dig Liver Dis. 2008;40:821–826.
12. Clemente V, Aratari A, Papi C, Vernia P. Short term colectomy rate and mortality for severe ulcerative colitis in the last 40 years. Has something changed? Dig Liver Dis. 2016;48:371–375.
13. Geltzeiler CB, Lu KC, Diggs BS, et al. Initial surgical management of ulcerative colitis in the biologic era. Dis Colon Rectum. 2014;57:1358–1363.
14. Stempel DA, Mauskopf J, McLaughlin T, et al. Comparison of asthma costs in pa-tients starting fluticasone propionate compared to papa-tients starting montelukast.
Respir Med. 2001;95:227–234.
15. Kappelman MD, Rifas-Shiman SL, Kleinman K, et al. The prevalence and geo-graphic distribution of Crohn’s disease and ulcerative colitis in the United States.
Clin Gastroenterol Hepatol. 2007;5:1424–1429.
16. Bernstein CN, Blanchard JF, Rawsthorne P, Wajda A. Epidemiology of Crohn’s disease and ulcerative colitis in a central Canadian province: a population-based study. Am J Epidemiol. 1999;149:916–924.
17. Kulaylat AS, Kulaylat AN, Schaefer EW, et al. Association of preopera-tive anti-tumor necrosis factor therapy with adverse postoperapreopera-tive outcomes in patients undergoing abdominal surgery for ulcerative colitis. JAMA Surg.
2017;152:e171538.
18. Peery AF, Cools KS, Strassle PD, et al. Increasing rates of surgery for patients with nonmalignant colorectal polyps in the United States. Gastroenterology.
2018;154:1352–1360.e3.
19. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–619. 20. Shadish W, Cook T, Campbell D. Experimental and Quasi-Experimental Designs
for Generalized Causal Inference. 2nd ed. Boston: Houghton-Mifflin; 2001. 21. Wagner AK, Soumerai SB, Zhang F, Ross-Degnan D. Segmented regression
anal-ysis of interrupted time series studies in medication use research. J Clin Pharm Ther. 2002;27:299–309.
22. Gillings D, Makuc D, Siegel E. Analysis of interrupted time series mortality trends: an example to evaluate regionalized perinatal care. Am J Public Health.
1981;71:38–46.
23. Piegorsch W, Bailer J. Nonlinear Regression. 1st ed. Chichester, UK: John Wiley & Sons, Ltd; 2005.
24. Brookhart MA, Rothman KJ. Simple estimators of the intensity of seasonal oc-currence. BMC Med Res Methodol. 2008;8:67. doi:10.1186/1471-2288-8-67 25. Nam J-m. Efficient method for identification of cyclic trends in incidence. Comm
Statist Theory Methods. 1983;12:1053–1068.
26. DURBIN J, WATSON GS. Testing for serial correlation in least squares regres-sion. I. Biometrika. 1950;37:409–428.
27. Berg DR, Colombel JF, Ungaro R. The role of early biologic therapy in inflam-matory bowel disease. Inflamm Bowel Dis. 2019;15:1896–1905.
28. Langholz E, Munkholm P, Davidsen M, Binder V. Course of ulcerative colitis: analysis of changes in disease activity over years. Gastroenterology. 1994;107:3–11. 29. Murthy SK, Begum J, Benchimol EI, et al. Introduction of anti-TNF therapy has
not yielded expected declines in hospitalisation and intestinal resection rates in inflammatory bowel diseases: a population-based interrupted time series study.
Gut. In press.
30. Reich KM, Chang HJ, Rezaie A, et al. The incidence rate of colectomy for medi-cally refractory ulcerative colitis has declined in parallel with increasing anti-TNF use: a time-trend study. Aliment Pharmacol Ther. 2014;40:629–638.
31. Rubin DT, Ananthakrishnan AN, Siegel CA, et al. ACG clinical guideline: ulcer-ative colitis in adults. Am J Gastroenterol. 2019;114:384–413.
32. Uchino M, Ikeuchi H, Hata K, et al. Changes in the rate of and trends in colec-tomy for ulcerative colitis during the era of biologics and calcineurin inhibitors based on a Japanese nationwide cohort study. Surg Today. In press.
33. Yu H, MacIsaac D, Wong JJ, et al. Market share and costs of biologic ther-apies for inflammatory bowel disease in the USA. Aliment Pharmacol Ther.
2018;47:364–370.
34. Kolehmainen S, Lepisto A, Farkkila M. Impact of anti-TNF-alpha therapy on colectomy rate and indications for colectomy in ulcerative colitis: compar-ison of two patient cohorts from 2005 to 2007 and from 2014 to 2016. Scand J Gastroenterol. 2019;54:707–711.
35. Laine L, Kaltenbach T, Barkun A, et al; SCENIC Guideline Development Panel. SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology. 2015;148:639–651. e28.
36. Regueiro M, Click B, Anderson A, et al. Reduced unplanned care and disease activity and increased quality of life after patient enrollment in an inflammatory bowel disease medical home. Clin Gastroenterol Hepatol. 2018;16:1777–1785. 37. Panaccione R, Ghosh S, Middleton S, et al. Combination therapy with infliximab
and azathioprine is superior to monotherapy with either agent in ulcerative co-litis. Gastroenterology. 2014;146:392–400.e3.
38. Peyrin-Biroulet L, Sandborn W, Sands BE, et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): determining therapeutic goals for treat-to-target. Am J Gastroenterol. 2015;110:1324–1338.
39. Ungaro R, Colombel JF, Lissoos T, Peyrin-Biroulet L. A treat-to-target update in ulcerative colitis: a systematic review. Am J Gastroenterol. 2019;114:874–883. 40. Colombel JF, D’Haens G, Lee WJ, Petersson J, Panaccione R. Outcomes and
strategies to support a treat-to-target approach in inflammatory bowel disease: a systematic review. J Crohns Colitis. In press.