Decoding Motor Signals From the Pediatric Cortex:
Implications for Brain-Computer Interfaces in Children
WHAT’S KNOWN ON THIS SUBJECT: A brain-computer interface is a system that decodes a signal from the brain and uses it for control of a desired machine output. These systems have been widely studied for use in restoring function in adults with motor disabilities.
WHAT THIS STUDY ADDS: Before this study, neuroprosthetic capabilities in children were unknown. The results of this study show that pediatric brain signals can be decoded and applied similarly to adult brain signals, which thus expands
neuroprosthetic horizons to children.
abstract
OBJECTIVE:To demonstrate the decodable nature of pediatric brain signals for the purpose of neuroprosthetic control. We hypothesized that children would achieve levels of brain-derived computer control comparable to performance previously reported for adults.
PATIENTS AND METHODS:Six pediatric patients with intractable epi-lepsy who were invasively monitored underwent screening for electro-cortical control signals associated with specific motor or phoneme articulation tasks. Subsequently, patients received visual feedback as they used these associated electrocortical signals to direct one dimen-sional cursor movement to a target on a screen.
RESULTS:All patients achieved accuracies between 70% and 99% within 9 minutes of training using the same screened motor and artic-ulation tasks. Two subjects went on to achieve maximum accuracies of 73% and 100% using imagined actions alone. Average mean and maximum performance for the 6 pediatric patients was comparable to that of 5 adults. The mean accuracy of the pediatric group was 81% (95% confi-dence interval [CI]: 71.5–90.5) over a mean training time of 11.6 minutes, whereas the adult group had a mean accuracy of 72% (95% CI: 61.2– 84.3) over a mean training time of 12.5 minutes. Maximum performance was also similar between the pediatric and adult groups (89.6% [95% CI: 83– 96.3] and 88.5% [95% CI: 77.1–99.8], respectively).
CONCLUSIONS:Similarly to adult brain signals, pediatric brain signals can be decoded and used for BCI operation. Therefore, BCI systems developed for adults likely hold similar promise for children with mo-tor disabilities.Pediatrics2011;128:e160–e168
AUTHORS:Jonathan D. Breshears, BS,aCharles M. Gaona,
MS,bJarod L. Roland, BS,cMohit Sharma, BS,bNicholas R.
Anderson, MS,bDavid T. Bundy, BS,bZachary V.
Freudenburg, MS,dMatthew D. Smyth, MD,cJohn Zempel,
MD, PhD,eDavid D. Limbrick, MD, PhD,cWilliam D. Smart,
PhD,dEric C. Leuthardt, MDb,c
aSchool of Medicine and Departments ofbBiomedical
Engineering,cNeurological Surgery,dComputer Science and
Engineering, andeNeurology, Washington University School of
Medicine, St Louis, Missouri
KEY WORDS
brain-computer interface, electrocorticography, cerebral palsy, motor disability
ABBREVIATIONS
BCI—brain-computer interface ALS—amyotrophic lateral sclerosis ECoG—electrocorticography EEG—electroencephalography CI—confidence interval
www.pediatrics.org/cgi/doi/10.1542/peds.2010-1519
doi:10.1542/peds.2010-1519
Accepted for publication Mar 9, 2011
Address correspondence to Eric C. Leuthardt, MD, Department of Neurosurgery, Washington University, School of Medicine, Campus Box 8057, 660 S Euclid Ave, St Louis, MO 63130. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
A brain-computer interface (BCI) is a system that decodes a signal from the brain and uses it for control of a de-sired output, such as a robotic arm or a computer cursor.1 Such systems
have been widely studied in adults and represent a potential means of restor-ing function and communication in cases in which the normal flow and ex-ecution of motor commands from the brain to the peripheral muscles has been interrupted. Spinal cord injury, amyotrophic lateral sclerosis (ALS), and brainstem stroke are just a few examples of adult conditions in which function can be partially restored by BCI systems.2,3 Although BCI systems
may also hold potential for function restoration in pediatric patients with motor disability, work in this group has been limited. Known differences in cortical maturation and motor electro-physiology exist between children and adults.4,5 Therefore establishment of
the decodability of children’s brain sig-nals, as has been shown only in adults, is critical to the application of ad-vances in BCI technology to the pediat-ric population. In addition, pediatpediat-ric motor disability is caused by patho-logic conditions that are more promi-nent in pediatric age groups, such as muscular dystrophies and cerebral palsy, and may potentially require dif-ferent considerations and neuropros-thetic approaches. Patients with such disorders would stand to benefit from BCI systems capable of bypassing neu-ral dysfunction to carry out the user’s intentions.
The majority of human BCIs derive their control signals from the electro-physiologic activity of the brain. These signals can take the form of oscillating electrical potentials acquired at the scalp by electroencephalography (EEG) or at the cortical surface by elec-trocorticography (ECoG). Oscillations of the cortical electrical potential rep-resent larger scale neural phenomena
and occur in separable frequency ranges, which can be used for control. Sensorimotor cortex oscillations in the range of 8 to 30 Hz arise from thalamo-cortical circuits and exhibit power de-creases during motor movements.6–8
Higher frequencies (⬎30 Hz), known as␥rhythms, are associated with the activity of cortical neural ensembles and exhibit highly localized power in-creases associated with motor move-ments and speech.9–11 BCIs based on
EEG and ECoG can use power changes in these different frequency bands as the independent signals for device control.
Invasive monitoring of pediatric epi-lepsy patients provides a unique op-portunity to test ECoG brain signals in children to determine the decodability of the brain signals and the feasibility of BCI application. In this study we tested multiple motor paradigms to assess the feasibility of the application of BCI in younger patient populations. In addition, to establish that the elec-trical signals from children’s brains can be successfully decoded and used for control just as those in adults, we compared our data on the perfor-mance of our cohort with data ac-quired from adult studies. Our results demonstrate that with very little training time, pediatric epilepsy pa-tients with clinical ECoG grid im-plants are able to achieve rapid and effective control of a simple com-puter task. Performance made possi-ble by this control in children is com-parable to that in adults. These findings provide the first evidence of the potential utility of neuropros-thetic approaches in children.
PATIENTS AND METHODS
Patients
This study included 6 pediatric pa-tients (aged 9 –15 years) with intracta-ble epilepsy who underwent place-ment of a subdural electrode array (3
right, 3 left). The study was approved by the human studies committee of the Washington University Medical Center. Before patient inclusion in the study, the patient’s legal guardians gave their written informed consent and the child also provided assent. A craniot-omy was performed to place the elec-trode array according to clinical criteria (Fig 1 A and B). Patients were then moved to a 24-hour video-monitoring unit for⬃1 week, during which exper-imental data were collected. Patients had no previous training on a BCI sys-tem. Demographic and clinical infor-mation is shown in Table 1.
Signal Acquisition
Electrode arrays (AdTech, Racine, WI) consisted of 48 to 64 electrodes (6⫻8, 8⫻8) spaced 10 mm apart, with an exposed surface with a diameter of 2.43 mm. Using g.tech biosignal ampli-fiers (Graz, Austria), electrocortical signals were digitized at 1200 Hz. A Dell computer running BCI2000 software was used to acquire, process, and store the data.12The amount of data
collected from each patient varied de-pending on the patient’s physical health after the craniotomy, and will-ingness to continue.
periods of repetitive verbal expression of 1 of 4 phonemes (oo, ah, eh, and ee) or rest. Cues were presented as words on a screen. Active cues were pre-sented in random order for a period of
2 to 3 seconds, during which the pa-tient repeatedly performed the speci-fied action. During intervals between cued activity, patients were cued to “rest,” or remain inactive. For
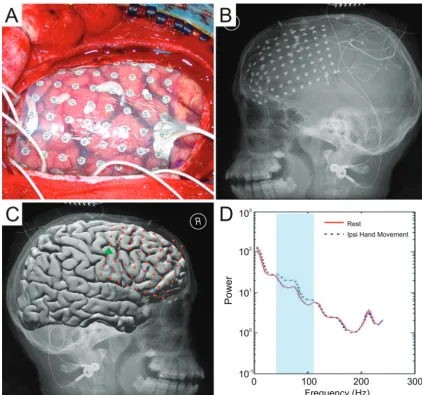
experi-ments in which imagined actions were used as the control task, the initial screening was the same except that subjects were instructed to imagine performing the given task rather than FIGURE 1
Electrode implantation, localization, and control-feature determination (from subject 2). A, Intraoperative photograph during grid implantation. B, Postop-erative radiograph. C, Electrode locations shown on a standard Montreal Neurological Institute brain. The green triangle indicates an electrode that shows significant spectral power changes in the frequency range of 40 to 110 Hz with ipsilateral hand movement (D).
TABLE 1 Demographic and Clinical Information for the 6 Subjects
Patient Age, y Gender Cognitive Capacity
Motor Capacity Age at Seizure Onset, y
Seizure Type Seizure Focus
1 15 Male Normal Normal 3 Complex partial Left medial frontal lobe 2 11 Male Normal Normal 7 Drop attacks, complex partial Right frontal lobe 3 15 Female Normal Normal 12 Complex partial Left temporal lobe 4 9 Male Normal Mildly impaired 8 Complex partial, generalized tonic-clonic,
staring spells, auras
Right postcentral gyrus
5 12 Male Normal Mildly impaired 8 Complex partial Mesial left frontal
6 13 Male Normal Normal 7 Complex partial Right medial anterior frontal lobe
actually performing it, and were mon-itored for compliance.
The signal tracings were inspected be-fore, during, and after the experiment to ensure that there was no interictal activity during the course of the exper-iment. The screening data were then converted to the frequency domain by autoregressive spectral estimation in 2-hz bins ranging from 0 to 250 Hz. For each electrode and frequency bin, power increases or decreases in the significant task-related spectral power were identified by calculating ther2value between the baseline, or
rest, sprectra and the activity spec-tra for each of the active tasks. Those features (ie, electrodes and fre-quency bins) with the highest degree of power variance accounted for by the specific task, as indicated by their relatively higherr2values, were chosen
as the control features for the subse-quent closed-loop control experiments (Fig 1 C and D).
Skull radiographs were used in con-junction with the getLOC MATLAB
pack-age (Mathworks, Natick, MA) to deter-mine the Talairach coordinates of the electrodes,13which were then used to
approximate the cortical location (⫾1 cm) and appropriateness of a given control feature (ie, an electrode iden-tified as having significant activations with hand movements was indeed lo-cated near motor areas).
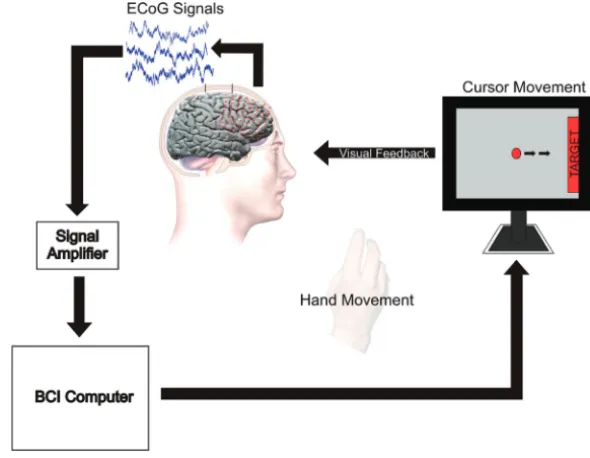
Closed-Loop Control Experiments Using the identified control features and their associated tasks, the pa-tients participated in closed-loop con-trol experiments (Fig 2) during which the patients’ objective was, by per-forming the particular motor or pho-neme articulation task, to move a cur-sor on a screen along 1 dimension to hit a presented target on either side of the screen. Cursor movement was determined by the output of a real-time translational algorithm based on the weighted, linear summation of the identified control features (ie, the power in a particular frequency bin from particular electrodes). Cursor
movement occurred every 40 millisec-onds and was based on signals ac-quired over the previous 280 millisec-onds. Control features showing power increases with a particular task were assigned positive weights, and those showing power decreases were as-signed negative weights, such that per-forming the task would move the cur-sor 1 direction and not performing the task would move the cursor in the op-posite direction. After an initial 1-minute parameter initialization pe-riod, the sliding window adaptation feature of BCI2000 was turned off and all parameters remained constant throughout the sessions.
Patients received visual feedback and performed consecutive trials of at-tempting to move the cursor to the tar-get. Trials began with the appearance of a target randomly at the left or right side of the screen. After a 1-second de-lay, a cursor appeared in the middle of the screen with its one-dimensional left or right movement driven by the patient’s ECoG signals as described above. The patient would perform or imagine the particular task or rest to move the cursor toward the target on the left or right of the screen, respec-tively. Each trial ended with either suc-cess (cursor hit the target), failure (cursor hit side of the screen opposite the target), or a time-out (time ran out before success or failure occurred). Trials were grouped into runs of up to 3 minutes, separated by rest periods of⬃1 minute. Accuracy, calculated as number of successes divided by the number of successes plus failures, was assessed after each block.
Per-formance curves were assessed
over the entire duration of training (multiple runs) with a particular task and associated set of control features. Performance at the level of chance was conservatively assumed to be 50%. To cultivate participant engagement in the research, less FIGURE 2
constrained tasks involving video game play and control of a robotic hand (Shadow Robot Company, Lon-don, United Kingdom) were also done with 3 of the 6 children.
To assess whether pediatric perfor-mance was similar to that of adults in the same one-dimensional cursor con-trol tasks, previously reported data from 5 adult patients, aged 23 to 46 years, was used.14,15The average (with
95% confidence interval [CI]) mean and maximum accuracy during the overt control experiments were calcu-lated for both groups and compared.
RESULTS
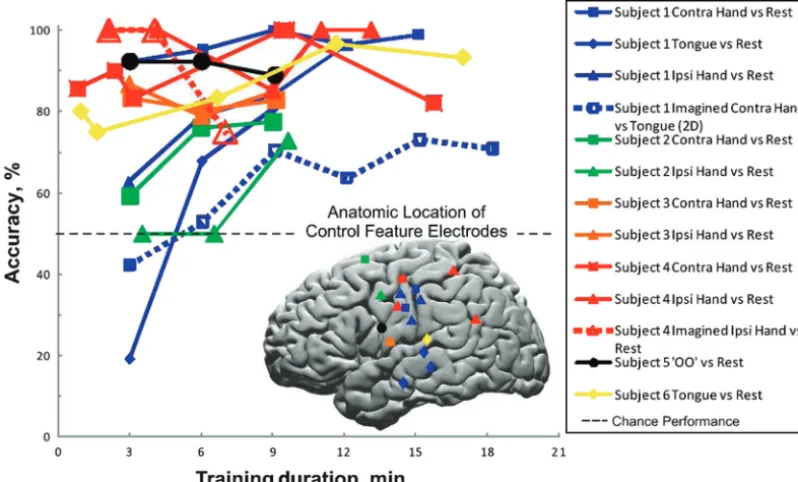
The performance curves and cortical locations of the corresponding control features used are shown in Fig 3. Final target accuracies for all patients were between 70% and 99% (chance perfor-mance⫽50%). Training times ranged from 9 to 18 minutes, during which 5 participants achieved⬎80% accuracy. Of note, 4 of the 6 subjects started with accuracies⬎70%. Table 2 summarizes the tasks performed, control features
used, and final accuracies achieved by the subjects during each of the control experiments. Four subjects were able to get control based on both
contralat-eral and ipsilatcontralat-eral hand movements, with control signals identified primar-ily in motor and premotor areas at classic (15– 40 Hz) and ␥ (60 –130 Hz) frequency ranges. Two subjects
at-tained control based on tongue move-ments, with control features identified at high␥ (107.5–155 Hz) frequencies primarily on the posterior superior temporal lobe. A single subject was
able to achieve a final accuracy of 88.8% based on articulating the pho-neme “oo.” This control was based on 77.5– 82.5 Hz signals from the left hemisphere near the face motor area.
In addition to the described BCI control tasks, 3 of the 6 patients also partici-pated in less constrained BCI control
tasks intended to engage the partici-pants. With 2 patients, control features as selected for the one-dimensional cursor task were used to control as-pects of video game play for Space
In-vaders, Pac-Man, and/or Raiden X (Fig 4 A andSupplemental Movie 1). A third patient’s control features were ap-plied to the opening and closing of a
robotic hand (Fig 4 B and Supplemen-tal Movie 2). Importantly, after minimal training, patients 1 and 4 were able to exert BCI control based on imagination of the appropriate task rather than overt
performance of the task (Fig 3, dashed lines). Of note, these 2 subjects toler-ated the craniotomy procedure better than the other children, and thus also participated in more experiments.
A comparison of pediatric and adult BCI performance based on overt control tasks is shown in Fig 5. The mean
accu-racy of the pediatric group was 81% (95% CI: 71.5–90.5) over a mean train-ing time of 11.6 minutes, whereas the adult group had a mean accuracy of 72% (95% CI: 61.2– 84.3) over a mean
training time of 12.5 minutes. Maximum performance was also similar between the pediatric and adult groups (89.6% [95% CI: 83–96.3]) and 88.5% [95% CI: 77.1–99.8], respectively).
FIGURE 3
DISCUSSION
This is the first study of an ECoG BCI in a pediatric population. Our results show that prepubescent and peripubescent children are able to rapidly and effec-tively achieve control of a computer cur-sor using a multitude of different cogni-tive modalities and their associated cortical physiologies. In addition, the subjects showed levels of performance comparable to those reported for adults
by this group and others.16This
inaugu-ral demonstration of the decodability of pediatric brain signals has important implications for the future extension of the BCI work done in adults to children with motor disabilities.
To date, BCIs have been studied exten-sively in adult populations as a means of augmenting function in victims of spinal cord injury, ALS, or locked-in syndrome.3,17–22 In addition to spinal
cord injury, pediatric motor disability is also commonly caused by cerebral palsy, perinatal stroke,
myelomeningo-celes, traumatic brain injury, and mus-cular dystrophies. With spinal cord dysfunction and peripheral muscular dystrophies the approaches for func-tional augmentation would be similar to previous approaches, namely, ac-quire signals from an intact brain to enable control of a device to facilitate
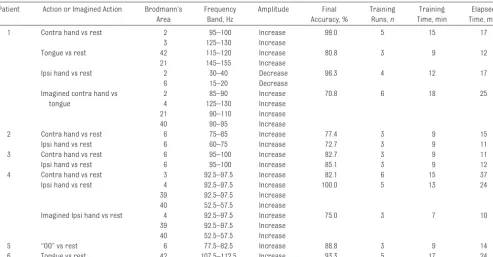
TABLE 2 Summary of Tasks Performed, Control Features, and Final Accuracy for Each BCI Control Experiment
Patient Action or Imagined Action Brodmann’s Area
Frequency Band, Hz
Amplitude Final Accuracy, %
Training Runs,n
Training Time, min
Elapsed Time, min
1 Contra hand vs rest 2 95–100 Increase 99.0 5 15 17
3 125–130 Increase
Tongue vs rest 42 115–120 Increase 80.8 3 9 12
21 145–155 Increase
Ipsi hand vs rest 2 30–40 Decrease 96.3 4 12 17
6 15–20 Decrease
Imagined contra hand vs tongue
2 85–90 Increase 70.8 6 18 25
4 125–130 Increase 21 90–110 Increase 40 90–95 Increase
2 Contra hand vs rest 6 75–85 Increase 77.4 3 9 15
Ipsi hand vs rest 6 60–75 Increase 72.7 3 9 11
3 Contra hand vs rest 6 95–100 Increase 82.7 3 9 11
Ipsi hand vs rest 6 95–100 Increase 85.1 3 9 12
4 Contra hand vs rest 3 92.5–97.5 Increase 82.1 6 15 37
Ipsi hand vs rest 4 92.5–97.5 Increase 100.0 5 13 24
39 92.5–97.5 Increase 40 52.5–57.5 Increase
Imagined Ipsi hand vs rest 4 92.5–97.5 Increase 75.0 3 7 10
39 92.5–97.5 Increase 40 52.5–57.5 Increase
5 “OO” vs rest 6 77.5–82.5 Increase 88.8 3 9 14
6 Tongue vs rest 42 107.5–112.5 Increase 93.3 5 17 24
Elapsed time indicates duration of sessions during which all training runs were performed. It does not include equipment-setup time (10 –20 minutes).
FIGURE 4
communication and environmental control. The central causes of motor disability more common in children, however, require different strate-gies for neural restoration. In partic-ular, if a certain part of the brain is not functioning to achieve a func-tional motor output, as in the case of spastic hemiplegia, in which 1 hemi-sphere is affected; the use of an al-ternate cortical location of motor in-tention may be required. Thus the demonstration of ipsilateral motor movements as a generator of effec-tive control signals by 4 of our pedi-atric subjects, as has been re-ported,14is particularly exciting.
In addition to the multiple cognitive modalities that were used, all the sub-jects had a high level of performance. In this study the participants demon-strated that final accuracies of 70% to 99% in a one-dimensional control task could be achieved with training times ranging from 9 to 18 minutes. Control was achieved from both contralateral and ipsilateral motor signals gener-ated by hand and tongue movements, as well as from phoneme articulation. Of note, 5 subjects started with
perfor-mance⬎80% based solely on the con-trol features chosen during screening and with no training at all. This reflects the robust decodable nature of signals derived from surface cortical physiol-ogy, which enable early and rapid con-trol. It is also important to note that although neurofeedback on brain sig-nals has been used before in children, this use has been primarily for diag-nostic and therapeutic purposes, rather than for the express purpose of control alone.23Moreover, when
high-frequency ␥ rhythms are used this control occurs within minutes, versus
⬎3 hours required when slow cortical potentials are used as described by Strehl et al23
ECoG’s superior frequency range is at-tributable to 2 factors. First, the capac-itance of cell membranes of the overly-ing tissue combined with their intrinsic electrical resistance consti-tutes a low-pass (resistor– capacitor) filter that largely eliminates higher fre-quencies from being recorded with EEG.24Second, higher frequencies tend
to be produced by smaller cortical as-semblies. Thus, they are more promi-nent at electrodes that are closer to the cortex.24Thus the ECoG offers
sub-stantial advantages over EEG in spatial resolution (millimeters versus centi-meters), noise reduction, and the abil-ity to detect changes in high-frequency oscillations not measurable at the scalp.24–26 In addition, for a future
clinical neuroprosthetic, an ECoG implant– based BCI offers enhanced stability and durability of control sig-nals compared with external EEG-based systems, which would require a higher level of technical support for daily electrode cap placement, recur-rent control feature localization (ow-ing to signal nonstationarity), and in-terface maintenance (eg, ensuring appropriate electrode contact with gels). Finally, because ECoG detects a more information-rich signal from the
cortex than EEG does from the scalp, there is the potential for more complex device control with simultaneous ac-cess of a smaller area of cortex with a microgrid implant.27 Given its
en-hanced signal properties over EEG, ECoG is an optimal emerging platform for BCI systems.15,28
When the pediatric subjects’ screening and performance are considered in a context relative to adult performance, another fundamental research link is provided. The ability of the children in our study to identify and use control features similarly to adults demon-strates that other ongoing neuropros-thetic findings and advances found in adult populations (in whom the major-ity of research is being performed) may also have implications for chil-dren. In addition, although our sample population was not large, the demon-stration that these control features can be accomplished by using covert intentions (without the need for actual movements for screening or control) further supports the possibility that these signals can be used in actual populations with motor disabilities. Fi-nally, as an example, although applica-tion of simple BCI control to video games and robotics had the intended the effect of enhancing the children’s engagement in the research, these promising demonstrations are also suggestive of future neuroprosthetic possibilities for BCI systems in chil-dren with severe motor disabilities.
It is important to note some potential limitations and considerations. The study patients had epilepsy, and al-though we could not explicitly disprove that seizure activity may in some way have contributed to the control fea-tures used in this paradigm, it is highly unlikely for several reasons. Mac-roscale␥band power increases have also been closely correlated with other modalities that localize functional fo-cal cortifo-cal activity, including multiunit FIGURE 5
action potential firing29 and
task-related activation in blood-oxygen-level dependent functional magnetic resonance imaging.30 Although
previ-ous investigators have looked at fast ripples and their relationship to sei-zures, these typically demonstrate more random stochastic activity and would be poorly correlated with pro-longed behaviorally associated corti-cal activations.31 In addition, the
fre-quency bands chosen as cognitive correlates and used for device control were narrow bands within the␥
spec-trum. These narrow bands have been shown to have a close correlation with distinguishing cognitive tasks.32
CONCLUSIONS
We report the first demonstration of the decodable nature of pediatric ECoG signals for use in a BCI application. Pe-diatric ECoG provided robust control signals that enabled a high level of con-trol with only minutes of training. The comparability of this performance in children to that of adults indicates that recent advances in
neuropros-thetic research being performed in adult populations will also have an impact on neuroprosthetics for chil-dren. By enabling children with per-manent motor disabilities to circum-vent sites of neurologic dysfunction, such systems may allow these chil-dren to function and communicate effectively.
ACKNOWLEDGMENT
This work was made possible through the generous support of the Children’s Discovery Institute.
REFERENCES
1. Wolpaw JR, Birbaumer N, McFarland DJ, Pfurt-scheller G, Vaughan TM. Brain-computer inter-faces for communication and control.Clin Neu-rophysiol. 2002;113(6):767–791
2. Hochberg LR, Serruya MD, Friehs GM, et al. Neuronal ensemble control of prosthetic devices by a human with tetraplegia. Na-ture. 2006;442(7099):164 –171
3. Wolpaw JR, McFarland DJ. Control of a two-dimensional movement signal by a noninvasive brain-computer interface in humans.Proc Natl Acad Sci U S A. 2004;101(51):17849 –54
4. Gogtay N, Giedd JN, Lusk L, et al. Dynamic map-ping of human cortical development during childhood through early adulthood.Proc Natl Acad Sci U S A. 2004;101(21):8174 – 8179
5. Pangelinan MM, Kagerer FA, Momen B, Hat-field BD, Clark JE. Electrocortical dynamics reflect age-related differences in move-ment kinematics among children and adults.Cereb Cortex. 2011;21(4):737–747.
6. Crone NE, Miglioretti DL, Gordon B, et al. Func-tional mapping of human sensorimotor cortex with electrocorticographic spectral analysis. I. Alpha and beta event-related desynchronization. Brain. 1998;121(pt 12):2271–2299
7. Pfurtscheller G.Event-Related Desynchroniza-tion (ERD) and Event Related SynchronizaDesynchroniza-tion (ERS). Baltimore, MD: Williams and Wilkins; 1999 8. Pfurtscheller G, Graimann B, Huggins JE, Levine SP, Schuh LA. Spatiotemporal pat-terns of beta desynchronization and gamma synchronization in corticographic data during self-paced movement.Clin Neu-rophysiol. 2003;114(7):1226 –1236
9. Crone NE, Hao L, Hart J Jr, et al. Electrocor-ticographic gamma activity during word production in spoken and sign language. Neurology. 2001;57(11):2045–2053
10. Crone NE, Miglioretti DL, Gordon B, Lesser RP. Functional mapping of human
sensori-motor cortex with electrocorticographic spectral analysis. II. Event-related synchro-nization in the gamma band.Brain. 1998; 121(pt 12):2301–2315
11. Leuthardt EC, Miller, KJ, Anderson N, et al. Electrocorticographic frequency alteration mapping: a clinical technique for mapping the motor cortex.Neurosurgery. 2007;60(4 suppl 2):260 –270; discussion 270 –271
12. Schalk G, McFarland DJ, Hinterberger T, Birbaumer N, Wolpaw JR. BCI2000: a general-purpose brain-computer interface (BCI) system.IEEE Trans Biomed Eng. 2004; 51(6):1034 –1043
13. Miller KJ, Makeig S, Hebb AO, Rao RP, den-Nijs M, Ojemann JG. Cortical electrode local-ization from X-rays and simple mapping for electrocorticographic research: the “Loca-tion on Cortex” (LOC) package for MATLAB.J Neurosci Methods. 2007;162(1–2):303–308
14. Wisneski KJ, Anderson N, Schalk G, Smyth M, Moran D, Leuthardt EC. Unique cortical physiology associated with ipsilateral hand movements and neuroprosthetic implica-tions.Stroke. 2008;39(12):3351–3359
15. Leuthardt EC, Schalk G, Wolpaw JR, Ojemann JG, Moran DW. A brain-computer interface using electrocorticographic signals in hu-mans.J Neural Eng. 2004;1(2):63–71
16. Leuthardt EC, Miller KJ, Schalk G, Rao RN, Ojemann JG. Electrocorticography-based brain computer interface: the Seattle expe-rience.IEEE Trans Neural Syst Rehabil Eng. 2006;14(2):194 –198
17. Pfurtscheller G. Central beta rhythm during sen-sorimotor activities in man.Electroencephalogr Clin Neurophysiol. 1981;51(3):253–264
18. Pfurtscheller G. Functional topography dur-ing sensorimotor activation studied with event-related desynchronization mapping. J Clin Neurophysiol. 1989;6(1):75– 84
19. Pfurtscheller G, Aranibar A. Event-related corti-cal desynchronization detected by power mea-surements of scalp EEG.Electroencephalogr Clin Neurophysiol. 1977;42(6):817– 826
20. Pfurtscheller G, Guger C, Muller G, Krausz G, Neuper C. Brain oscillations control hand orthosis in a tetraplegic. Neurosci Lett. 2000;292(3):211–214
21. Kübler A, Nijboer F, Mellinger J, et al. Pa-tients with ALS can use sensorimotor rhythms to operate a brain-computer inter-face.Neurology. 2005;64(10):1775–1777
22. Birbaumer N, Ghanayim N, Hinterberger T, et al. A spelling device for the paralysed. Nature. 1999;398(6725):297–298
23. Strehl U, Leins U, Goth G, Klinger C, Hinterberger T, Birbaumer N. Self-regulation of slow cortical potentials: a new treatment for children with attention-deficit/hyperactivity disorder. Pediat-rics. 2006;118(5). Available at: www.pediatrics. org/cgi/content/full/118/5/e1530
24. Srinivasan R, Nunez PL, Silberstein RB. Spa-tial filtering and neocortical dynamics: esti-mates of EEG coherence.IEEE Trans Biomed Eng. 1998;45(7):814 – 826
25. Freeman WJ, Holmes MD, Burke BC, Van-hatalo S. Spatial spectra of scalp EEG and EMG from awake humans. Clin Neuro-physiol. 2003;114(6):1053–1068
26. Boulton AA, Baker GB, Vanderwolf CH, eds. Neurophysiological Techniques: Applica-tions to Neural Systems. Totowa, NJ: Hu-mana Press; 1990
27. Leuthardt EC, Freudenberg Z, Bundy D, Ro-land J. Microscale recording from human motor cortex: implications for minimally inv a s i inv e e l e c t r o c o r t i c o g r a p h i c b r a i n -computer interfaces. Neurosurg Focus. 2009;27(1):E10
interfaces: going beyond classic motor physiology.Neurosurg Focus. 2009;27(1):E4
29. Whittingstall K, Logothetis NK. Frequency-band coupling in surface EEG reflects spik-ing activity in monkey visual cortex.Neuron. 2009;64(2):281–289
30. Brovelli A, Lachaux J-P, Kahane P,
Bous-saoud D. High gamma frequency oscillatory activity dissociates attention from intention in the human premotor cortex. Neuroim-age. 2005;28(1):154 –164
31. Zijlmans M, Jacobs J, Kahn YU, Zelmann R, Dubeau F, Gotman J. Ictal and interictal high frequency oscillations in patients with focal
epilepsy.Clin Neurophysiol. 2011;122(4): 664 – 671
DOI: 10.1542/peds.2010-1519 originally published online June 20, 2011;
2011;128;e160
Pediatrics
Zempel, David D. Limbrick, William D. Smart and Eric C. Leuthardt
R. Anderson, David T. Bundy, Zachary V. Freudenburg, Matthew D. Smyth, John
Jonathan D. Breshears, Charles M. Gaona, Jarod L. Roland, Mohit Sharma, Nicholas
Services
Updated Information &
http://pediatrics.aappublications.org/content/128/1/e160
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/128/1/e160#BIBL
This article cites 29 articles, 6 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neurology_sub
Neurology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2010-1519 originally published online June 20, 2011;
2011;128;e160
Pediatrics
Zempel, David D. Limbrick, William D. Smart and Eric C. Leuthardt
R. Anderson, David T. Bundy, Zachary V. Freudenburg, Matthew D. Smyth, John
Jonathan D. Breshears, Charles M. Gaona, Jarod L. Roland, Mohit Sharma, Nicholas
Brain-Computer Interfaces in Children
Decoding Motor Signals From the Pediatric Cortex: Implications for
http://pediatrics.aappublications.org/content/128/1/e160
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2011/06/13/peds.2010-1519.DC1
Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.