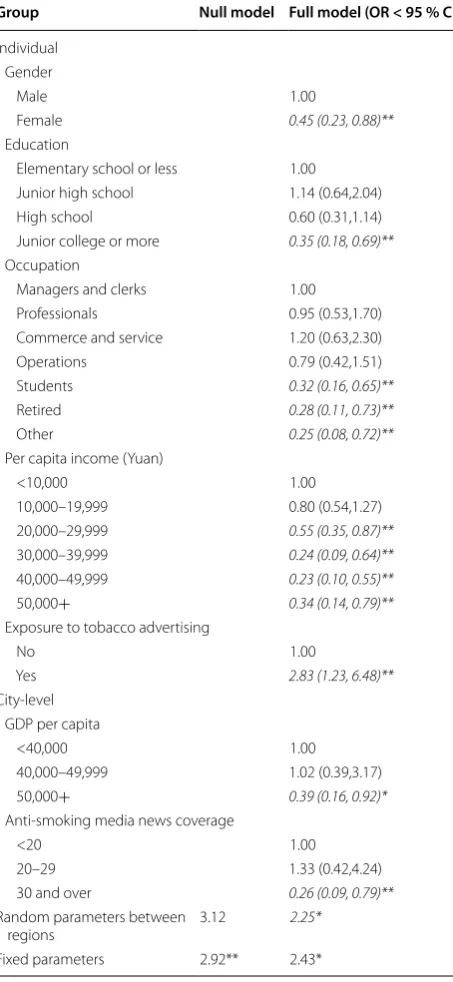
Individual and city-level determinants of secondhand smoke exposure in China
Full text
Figure

Related documents
Here, 8 incoming phone lines, and 16 outgoing stations are connected to a channel bank, which is connected to Asterisk using a T1 cross over cable.. (remember, in this diagram T1
To facilitate comparisons between our income poverty estimates and the income- based poverty rates from MOLISA, we adjust the income poverty line such that income poverty
Lisäksi on mahdollista, että tulevaisuudessa asuntojen ja autojen lisäksi vuokrataan myös tietoko- neita, kalusteita ja muita käyttötavaroita ostamisen sijaan (Kamppuri,
Jordi Rodón, Hospital Universitari Vall d’Hebrón (VHIO), Barcelona. Thursday 22 nd
Received: 2018.09.23 Revised: 2018.12.10 Accepted: 2019.02.12 Available online: 2019.02.. The changes in the initial maximum contact pressures p f max during one cycle of
With this view, some dioxomolybdenum(VI) complexes with general formula MoO2(mac)](acac)2, (where mac = tetraazamacrocyclic ligands derived from condensation of
In contrast, dynamic techniques called Dynamic Power Management (DPM) techniques are applied at runtime and these techniques are used to reduce power when systems are serving
6 – Effect of modifying time interval for defining secondary treatment on the number of patients for whom there was disagreement as to recurrent disease status between the Gold
