Erectile Dysfunction
Tina K.Thethi, MD; Nana O. Asafu-Adjaye, MPH; and Vivian A. Fonseca, MD
E
rectile dysfunction (ED) affects about 30 million men in the United States to some extent.1–3 It may indicate the presence of a seri-ous underlying medical condition, such as cardiovascular disease (CVD), dia-betes, or depression. It compromises multiple aspects of a patient’s life, including overall quality of life and interpersonal relationships.ED is common among men with diabetes. Its incidence increases with advancing age, and it occurs at an earli-er stage than age-matched countearli-erparts without diabetes. The etiology of ED in the diabetic population is multifactorial. In order to ensure the best possible out-comes in managing this problem, clini-cians need to be aware of the underlying pathophysiology.
Patients with diabetes respond to phosphodiesterase type 5 (PDE-5) inhibitors, but the response is lower than in those without diabetes. Coexistence of hypertension, CVD, and poor glycemic control worsens ED. A multi-disciplinary approach should be consid-ered to deal with the different comor-bidities, including psychiatric,
endocrine, cardiovascular, and urologi-cal issues.
PREVALENCE OF ED IN DIABETES
It is estimated that 35–75% of men with diabetes have ED. Compared to age-matched control subjects, men with diabetes develop ED ~ 5–10 years earli-er.4In a cross-sectional survey of 541 men with diabetes at a community-based clinic, the prevalence of ED increased progressively with age. The
prevalence was 6% in the age group 20–24 years and 52% in the age group 55–59 years. After the age of 60 years, 55–95% of men with diabetes were affected by ED, compared to ~ 50% in an unselected population in the Massachusetts Aging Male Survey.5,6In another cohort of patients having type 1 diabetes for at least 10 years, ED was reported in 1.1% of men in the age group 21–30 years, 55% of men in the age group 50–60 years, and 75% of men > 60 years of age.7
ED in men with diabetes is correlat-ed with hemoglobin A1c(A1C). The
presence of peripheral neuropathy increases the risk of ED, possibly because of underlying autonomic neu-ropathy. Almost 100% of patients with diabetic neuropathy will have ED. Endothelial dysfunction is a major etio-logical factor that is common to dia-betes, ED, and CVD.
Management of ED has been dra-matically altered by the introduction of PDE-5 inhibitors. Data suggest that patients with diabetes do not respond to treatment as well as patients without diabetes.7–9Alternative therapies may be needed to overcome this problem. This
review focuses on the evaluation, man-agement, and significance of ED in patients with diabetes.
PATHOPHYSIOLOGY OF ED
ED in men is multifactorial in origin. Diabetes is associated with accelerated large vessel atherosclerosis, microvas-cular arterial disease, autonomic neu-ropathy, dyslipidemia, concomitant hypertension, and prominent endothe-lial dysfunction. All of these conditions contribute to ED. It is the combination of impairments in nearly every step responsible for the production of penile erection (Table 1). Clinicians must take these etiological factors into considera-tion when treating ED in men with dia-betes. In addition to the listed causes (Table 2), a comprehensive evaluation should include assessment of gonadal function, medications, and drug history, along with psychological and marital status.7
ENDOTHELIAL DYSFUNCTION
The endothelium is vital to the mainte-nance of vascular health. It is a critical determinant of vascular tone and paten-cy, reactivity, inflammation, vascular remodeling, and blood fluidity.7,10
Nitric oxide (NO) is the most potent vasodilator and is secreted by the endothelium. It is synthesized from L
-arginine by the endothelial enzyme NO synthase (eNOS) (Figure 1). NO released in response to sexual stimula-tion relaxes penile vascular smooth muscle by increasing intracellular cyclic 3', 5'- guanosine monophosphate (cGMP) concentration. Vasodilatation of erectile tissues allows the sinusoidal Erectile dysfunction affects ~ 30
mil-lion men in the United States to some extent. It may indicate the presence of a serious underlying medical con-dition, such as cardiovascular disease, diabetes, or depression. It compro-mises multiple aspects of a patient’s life, including overall quality of life and interpersonal relationships.
Table 2. Modifiable Risk Factors for ED and Their Management
Risk Factor
Sedentary lifestyle Depression Diabetes Alcohol Tobacco Hypogonadism Overweight or obesity
(BMI > 26.9 kg/m2)
Strategy
Increase physical activity Treatment of depression Improved control Abstinence from alcohol Quit smoking/use of patch Testosterone replacement Weight loss
Figure 1: Production and action of NO. GTP, guanosine triphosphate; 5 GMP, 5'-guanosine monophosphate; sol GC, soluble guanylate cyclase; O2, oxygen. Cholinergic stimulation causes release of ACh. ACh activates eNOS to produce NO from L-arginine. NO in the smooth muscle cells activates solGC. This converts GTP to cGMP. cGMP causes Ca2+ efflux, which leads to relaxation of the smooth mus-cle. cGMP is degraded to 5 GMP via PDE-5, thus providing a therapeutic target to prolong the action of cGMP.
Table 1. Pathophysiology and Factors Complicating Diabetic ED
• Increasing age and hyperglycemia leading to glycation of elastic fibers with failure of relaxation of the corpora cavernosa11,24 • Peripheral vascular disease causing reduced arterial and arteriolar inflow11,56
• Advanced glycation end products leading to increase in reactive oxidizing substances and reduced NO production11,26,57 • Failed neural signal transmission to and from the spinal cord due to diabetic neuropathy11,58and reduced production of
neu-ronal NO synthase11,59
causing reduced levels of neuronal NO release to the cavernosal smooth muscle
• Endothelial dysfunction of the sinusoidal endothelial cells resulting in a decrease in NO release and impaired vasodilatation • Hypogonadotrophic hypogonadism11,50,52
• Multiple drug regimens • Dyslipidemia
spaces to fill with blood resulting in the attainment and maintenance of an erec-tion. This process is reversed by PDE-5, the major PDE in penile cavernosal smooth muscle that is responsible for cGMP degradation. The bioavailability of NO can be decreased by various mechanisms, such as decreased pro-duction of eNOS, enhanced NO break-down due to increased oxidative stress, or both.
There is increasing evidence that ED correlates with the level of glycemic control. In animal experi-ments, elevated A1C significantly impairs endothelial NO-mediated cor-pus cavernosal relaxation in vitro. A retrospective analysis of a cohort of men with type 2 diabetes4 demonstrat-ed that A1C was an independent pre-dictor of erectile function score. An inverse relationship between severity of ED assessed by the International Index of Erectile Function (IIEF) score and A1C has also been demonstrated.11The IIEF, a multidimensional scale for assessment of ED, provides a broad measure of sexual function (Table 3).12
dis-International Index of Erectile Function
Precede all questions listed below with the phrase, “Over the past 4 weeks, . . .” Use the scale below each question in determining response.
Q1.How often were you able to get an erection during sexual activity?
Q2.When you had erections with sexual stimulation, how often were your erections hard enough for penetration?
0 = No sexual activity; 1 = Almost never/never; 2 = A few times (much less than half the time); 3 = Sometimes (about half the time); 4 = Most times (much more than half the time); 5 = Almost always/always
Q3.When you attempted sexual intercourse, how often were you able to penetrate (enter) your partner?
Q4.During sexual intercourse, how often were you able to maintain your erection after you had penetrated (entered) your partner? 0 = Did not attempt intercourse; 1 = Almost never/never; 2 = A few times (much less than half the time); 3 = Sometimes (about half the time); 4 = Most times (much more than half the time); 5 = Almost always/always
Q5.During sexual intercourse, how difficult was it to maintain your erection to completion of intercourse?
0 = Did not attempt intercourse; 1 = Extremely difficult; 2 = Very difficult; 3 = Difficult; 4 = Slightly difficult; 5 = Not difficult
Q6.How many times have you attempted sexual intercourse?
0 = No attempts; 1 = One to two attempts; 2 = Three to four attempts; 3 = Five to six attempts; 4 = Seven to 10 attempts; 5 = More than 11 attempts
Q7.When you attempted sexual intercourse, how often was it satisfactory to you?
0 = Did not attempt intercourse; 1 = Almost never/never; 2 = A few times (much less than half the time); 3 = Sometimes (about half the time); 4 = Most times (much more than half the time); 5 = Almost always/always
Q8.How much have you enjoyed sexual intercourse?
0 = No intercourse; 1 = No enjoyment; 2 = Not very enjoyable; 3 = Fairly enjoyable; 4 = Highly enjoyable; 5 = Very highly enjoyable
Q9.When you had sexual stimulation or intercourse, how often did you ejaculate?
Q10.When you had sexual stimulation or intercourse, how often did you have the feeling of orgasm or climax? 0 = No sexual stimulation/intercourse; 1 = Almost never/never; 2 = A few times (much less than half the time); 3 = Sometimes (about half the time); 4 = Most times (much more than half the time); 5 = Almost always/always
Q11.How often have you felt sexual desire?
1 = Almost never; 2 = A few times (much less than half the time); 3 = Sometimes (about half the time); 4 = Most times (much more than half the time); 5 = Almost always/always
Q12.How would you rate your level of sexual desire?
1 = Very low/none at all; 2 = Low; 3 = Moderate; 4 = High; 5 = Very high
Q13.How satisfied have you been with your overall sex life?
Q14.How satisfied have you been with your sexual relationship with your partner?
1 = Very dissatisfied; 2 = Moderately dissatisfied; 3 = About equally satisfied and dissatisfied; 4 = Moderately satisfied; 5 = Very satisfied
Q15.How do you rate your confidence that you could get and keep an erection? 1 = Very low; 2 = Low; 3 = Moderate; 4 = High; 5 = Very high
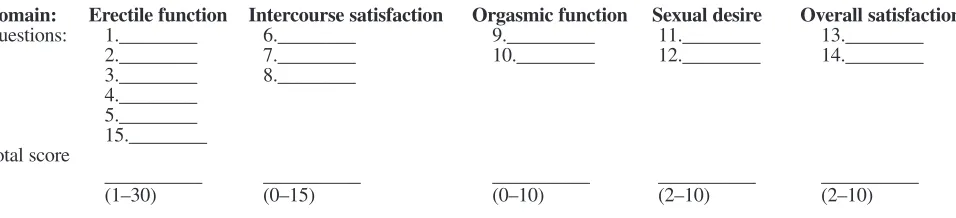
SCORING
Domain: Erectile function Intercourse satisfaction Orgasmic function Sexual desire Overall satisfaction
Questions: 1.________ 6.________ 9._________ 11.________ 13.________ 2.________ 7.________ 10.________ 12.________ 14.________ 3.________ 8.________
4.________ 5.________ 15.________ Total score
__________ __________ __________ __________ __________
Table 4. Evaluation and Management Strategies
Medication History:It is extremely important to consider side effects and drug interactions
• Antihypertensives:especially
♦ -Blockers: consider ACE inhibitor/angiotensin receptor blocker/calcium channel blocker
♦ Thiazide diuretics: consider switching to furosemide
• Agents acting on the centraol nervous system:tricyclic antidepressant drugs, selective serotonin reuptake inhibitors, phenothiazines, butyrophenones, atypical antidepressants: consider switching to trazodone
• Agents affecting the endocrine system:Antiandrogens, gonadotropin-releasing hormone agonists and antagonists, estrogens, cimetidine, metoclopramide, fibric acid derivatives,
alcohol, marijuana
Hormonal Status:
• Leutinizing hormone, follicle-stimulating hormone, prolactin • Testosterone level
• Ferritin (to evaluate for hemochromatosis)
Autonomic Neuropathy:
• ECG (R-R variability), heart rate variability • Orthostatic blood pressure readings • Tilt table testing
Vascular Disease:
• Doppler studies of penile blood flow
• Pharmacodynamic testing using vasoactive compounds • Pudendal angiography and cavernosometry
Psychosocial Assessment:
• Combine with nocturnal penile tumescence test • Marital counseling
ease.13The presence of peripheral neu-ropathy also increases the risk of ED, possibly because of undiagnosed auto-nomic neuropathy; almost 100% of patients with diabetic autonomic neu-ropathy will have ED. The interaction between endothelial dysfunction and autonomic neuropathy results in an inability to increase blood flow under conditions of stress or increased demands, such as during an erection.
SIGNIFICANCE OF ED IN PATIENTS WITH DIABETES
Many of the risk factors of ED are the same as those for CVD, which in patients with diabetes may be asympto-matic (Table 2). ED may be the first warning sign of underlying cardiovas-cular problems.
Gazzaruso et al.14evaluated the prevalence of ED in 133 diabetic men without apparent complications but with angiographically verified silent coronary artery disease (CAD) and in 127 diabetic men without myocardial ischemia at exercise electrocardiogram (ECG), 48-hour ambulatory ECG, and stress echocardiography. The preva-lence of ED was significantly higher in patients with silent CAD compared to those without silent CAD (33.8 vs. 4.7%). Multiple logistic regression showed that apolipoprotein(a) poly-morphism, smoking, microalbumin-uria, HDL cholesterol, and LDL cho-lesterol were significantly associated with silent CAD. Among the various factors, ED appeared to be the most efficient predictor of silent CAD. Thus, there may be a strong and inde-pendent association between ED and silent CAD in apparently uncomplicat-ed type 2 diabetic patients. ED may also be a potential marker to identify diabetic patients to screen for silent CAD.
Billups et al.15examined the rela-tionship between traditional and emerg-ing risk factors for CVD and the severi-ty of penile vascular disease in 137 men with ED and without clinical CAD. Plasma hs-C reactive protein levels
cor-related significantly with increasing severity of penile vascular disease as measured by penile Doppler.
ED may be an early sign or symp-tom of CVD. The same vascular/ endothelial injuries that occur in the coronary arteries likely occur in the cav-ernosal arteries, the primary vessels supplying the penile erectile tissue.16
MANAGEMENT OF ED
Management of ED includes a full clin-ical evaluation and a careful assessment of medications and other etiological factors in ED. Examination should include determination of the testes size and the secondary sexual characteristics for hypogonadism. Laboratory investi-gations should include levels of
testos-terone, prolactin, and ferritin, among others (Table 4).
Several therapeutic strategies including lifestyle changes have been shown to improve endothelial function in patients with type 2 diabetes. Epi-demiological studies have identified sedentary lifestyle as a potential modifi-able risk factor in men with ED and provide moderate support for the bene-ficial role of increasing exercise.5,17–20 Recent studies also have shown marked improvement in erectile function with exercise and weight loss in a group of obese men with moderate ED and no overt symptoms of CVD as compared to the control group.19,21
was a discontinuation rate from 5 to 17%, primarily due to insufficient clini-cal response.9
With tadalafil, 76% of men with diabetes taking the 20-mg dose had improved erections. Of the total number of patients in the group, 58% had erec-tions satisfactory to complete inter-course. Comparatively, in nondiabetic men the rates were 81 and 75%, respec-tively.29Use of vardenafil led to improved erections in 71–75% of non-diabetic men with 5-, 10-, and 20-mg doses. In men with diabetes, the response rates were comparatively low-er at 57% with the 10-mg dose and 72% with the 20-mg dose.30It is possible that this lower response rate in men with diabetes is related to their more severely impaired endothelial function.23
Taking into consideration the preva-lence of CVD in patients with ED, con-cerns regarding the risk of sexual activi-ty triggering acute cardiovascular events and potential risks of adverse or unan-ticipated drug interactions were addressed by the Princeton Consensus Panel. Patients were stratified into low-, intermediate-, or high-risk categories (Table 5).19
Exercise training after acute myocardial infarction (MI) improves cardiovascular efficiency and reduces myocardial oxygen consumption during regular activities, including sexual activity.17,31,32Cardiac rehabilitation exercise programs are helpful in reduc-ing coital symptoms and coital heart rates.17,19,32Patients whose cardiac con-dition is uncertain and those with multi-ple risk factors require further testing or evaluation before resuming sexual activ-ity.19Patients at high risk should be sta-bilized by cardiological treatment before resumption of sexual activity is considered or treatment of sexual dys-function is recommended.
The relative risk of a coitus-induced coronary event is not greater in patients with established CAD than in those without documented cardiac disease.19 Clinical studies of the PDE-5 inhibitors demonstrated no increase in MI or death diabetes who are often on multiple
drugs to treat hypertension, dyslipi-demia, depression, glaucoma, neuro-pathic pain, and diabetes itself. The major medications responsible for ED are antihypertensives, especially nonse-lective -blockers, sympathyolytics, and diuretics. The main problem in diabetes is that often these medications cannot be replaced; -blocker therapy is essen-tial in patients with coronary heart dis-ease or heart failure. Equally important are treatments for patients who suffer from conditions such as pain and depression. These problems are real to patients and, if not adequately treated, are likely to exacerbate ED. Physicians should try and optimize therapy with agents that are less likely to cause ED (Table 4). ACE inhibitors, angiotensin II receptor blockers (ARBs), statins, and thiazolidinediones should theoretically improve erectile function as they either enhance NO levels or block production of oxygen radicals, which deplete NO and prevent vasodilatation.22–27
PDE-5 Inhibitors
The Food and Drug Administration approved three drugs of the PDE-5 cate-gory for clinical use in the treatment of ED. Sildenafil was the first drug in this class, followed by the newer agents tadalafil and vardenafil. These drugs are potent and selective inhibitors of cGMP-specific PDE-5. They prevent the break-down of cGMP and prolong and improve smooth muscle relaxation. PDE-5 is the isoform of the enzyme highly expressed in cavernosal tissue. Hence, vasodilata-tion is greater in this tissue.
A meta-analysis of 11 randomized, double-blind, placebo-controlled trials of sildenafil citrate in patients with dia-betes reported improved erections in 59% of those with type 1 diabetes and 63% of those with type 2 diabetes.8 Improvement was noted regardless of age, race, ED severity and duration, or presence of various comorbities.28 Patients with diabetes experienced a decreased response rate as compared to those without diabetes (83%). There
rates in men compared to expected rates.19,33–35Patients with known CAD or heart failure receiving PDE-5 inhibitors did not exhibit worsening ischemia, coronary vasoconstriction, or hemodynamics on exercise testing or cardiac catheterization.19,36–40However, the use of nitrates is absolutely con-traindicated in patients taking PDE-5 inhibitors for ED.19-Blockers are con-traindicated with sildenafil and varden-fil. The PDE-5 inhibitors have a mini-mal effect on QTc interval.19,41 Vardenafil in one study was shown to increase the QTc interval by 6–9 mil-liseconds. It is not recommended in patients taking type IA antiarrhythmics, such as quinidine or procainamide, or type III antiarrhythmics, such as sotalol and amiodarone, or in patients with con-genital prolonged QT syndrome.19 Sta-tistically significant QTc interval changes have not been observed with either sildenafil or tadalafil.19
Intracavernosal Therapy
Several vasoactive substances can be used to stimulate the erectile process. These substances can be delivered directly into the corpora cavernosa by injection. Papaverine is a nonspecific PDE, and alprostadil is a prostaglandin E1 derivative. These two drugs, when given via the intracavernosal route, relax the smooth muscle of the corpora cavernosa. Another agent in use is phentolamine. Phenotolamine is a com-petitive inhibitor of -adrenergic recep-tors, which reduces sympathetic tone. Some practitioners use a combination of these agents, although very few large clinical trials of these combinations have been carried out.
Alprostadil is a synthetic
Intraurethral Prostaglandin Therapy
An intraurethral alprostadil supposito-ry system was developed in an attempt to avoid the problems and issues relat-ed to injection therapy.42Although it avoids the side effects of injection therapy, it may cause urethral pain in ~ 30% of the users. It has not been effective in those who have failed injection therapy. In a large study, 70% of men with diabetes were able to achieve an erection satisfactory for reported satisfactory sexual function.
The 31% of the men who did not com-plete the study complained of pain at the injection site and lack of efficacy. Of all the studies, 50% of the men partici-pating complained of pain at injection sites.
For ED, intracavernosal therapy has a success rate of ~ 80–90%. However, half of the men discontinue the use of intracavernosal injections due to pain, loss of effect, or lack of interest.
intercourse in 70% of their attempts. Only 2.4% of the men discontinued use because of pain.42
Vacuum-Constriction Devices
Vacuum tumescence devices work irre-spective of the underlying etiology of ED. Diabetic men with ED report a success rate of 75%. Most men find the technique acceptable, especially if they have tried and failed oral or injection therapy. Some individuals may find it cumbersome. It can also be added on to one of the other treatment modalities to enhance a partial response.
Surgery
With the availability of various newer treatment modalities, the use of penile prostheses has declined. However, there is an 86% success rate at 5 years, and 91% of erections are suitable for coitus.28Diabetes, however, poses a risk for prosthesis-associated infection and can often necessitate the removal of the prosthesis and possible worsen-ing of the primary problem. Rarely, severely compromised blood flow could lead to device failure.
Revascularization might help some of these patients, but it is difficult to select patients with a predictable good outcome. Also, revascularization is rel-atively contraindicated in men with diabetes.43In some patients, there could be venous incompetence, which can be improved by ligation of the deep dorsal vein and any incompetent circumflex veins.
The complexity of ED, the underly-ing endothelial dysfunction and neu-ropathy, and the extent of vascular dis-ease in patients with diabetes leads to less successful outcomes for these sur-gical procedures. Surgery should be reserved for clear-cut cases of vascular or venous insufficiency in young patients with recent-onset diabetes.
-Blockers
There are several over-the-counter herbal remedies but no adequate scien-tific data to support their efficacy or
Table 5. Risk Stratification for CVD and Management Recommendations
GRADE OF RISK CATEGORIES OF CVD MANAGEMENT
RECOMMENDATIONS
Low Risk • Asymptomatic, < 3 major • Primary care management risk factors for CAD • Consider all first-line • Controlled hypertension therapies
• Mild, previously evaluated • Reassess at regular angina intervals (6–12 months) • Post-successful coronary
revascularization • Uncomplicated past MI
(> 6–8 weeks) with negative stress test
• Mild valvular disease
• Congestive heart failure (New York Heart Association Class I)
Intermediate or • ≥3 major risk factors for • Specialized cardiovascular Indeterminate Risk CAD, excluding sex testing (e.g., exercise
• Moderate, stable angina tolerance test, • Recent MI or cardiovascular echocardiogram)
accident (< 6 weeks) • Restratification into high-• Left ventrical dysfunction/ or low-risk based on
congestive heart failure (New the results of
York Heart Association cardiovascular assessment Class II)
• Arrhthymia of unknown cause
High Risk • Unstable or refractory angina • Priority referral for • Uncontrolled hypertension specialized cardiovascular • Congestive heart failure (New managment
York Heart Association • Treatment for ED to be Class III, IV) deferred until cardiac • Recent MI (< 2 weeks), condition stabilized and
cardiovascular accident dependent on specialist • High-risk arrhythmias recommendations • Hypertrophic and other
cardiomyopathies • Moderate/severe valvular
ed, 33 patients regained adequate erec-tile function.52
Of note also is that serum testos-terone concentration is inversely associ-ated with carotid atherosclerosis in men with type 2 diabetes.53Vascular cells contain sex steroid hormone receptors.49 Testosterone can exert its effect on the vascular wall, either directly or through aromatization to estrogen.54It is uncer-tain if any of these etiologies contribute to ED. However, they must be consid-ered and, if severe, treated with androgen replacement. There has been a poor yield of results when testosterone is used as monotherapy for treatment of ED, how-ever. In a study of 78 obese men with type 2 diabetes, only 17% reported improved long-term sexual function when placed on testosterone enanthate.
The use of testosterone in men with normal testosterone levels is not advo-cated. Replacement therapy should be reserved for those who are androgen deficient, especially if they are contem-plating the use of a PDE-5 inhibitor. This is because neural NO production is androgen dependent, and PDE-5 inhibitors require the presence of NO to be effective.
CONCLUSION
The etiology of ED is multifactorial. Workups of patients for ED must include a detailed medication history because medication regimens are quite often the culprit. Astute physicians must try to make appropriate therapeutic exchanges when possible. It is important to stress lifestyle changes in addition to pharma-cological treatments. There are many therapeutic options for treating ED.
Given the prevalence of CVD in patients seeking medical attention for ED, the Princeton Consensus Confer-ence emphasized the importance of risk factor evaluation and risk stratification of patients into low-, intermediate-, and high-risk groups for management of ED. Clinical trial data provide support for the overall cardiac safety of PDE-5 inhibitors in patients with ED, even though a majority of these patients have safety.44Yohimbine and phentolamine
are -adrenergic blockers that have been shown to have modest efficacy in treating ED. However, they are not widely in use, especially in the United States. Side effects include palpitations and hypertension. In a recent study of 18 nonsmoker male subjects with ED, a 50% success rate (completion of inter-course) was reported in > 75% of the attempts. The patients who responded tended to have less severe ED.45A meta-analysis of yohimbine use found it to be more effective than placebo (odds ratio 3.85, 95% confidence inter-val 6.67–2.22).46Yohimbine has been advocated for more than a century as a treatment for ED.19,47However, results to date with yohimbine have been inconsistent, and adverse cardiovascular events have been observed in some studies.48
Androgen Therapy
Hypogonadism is being increasingly recognized as a comorbid condition associated with type 2 diabetes, meta-bolic syndrome, and other chronic ill-nesses.49Men who are obese and have type 2 diabetes are more prone to hypogonadotropic hypogonadism.50 This is attributed to elevated levels of estrone and estradiol produced by the aromatase enzyme in adipose tissue derived from adrenal (androstenedione) and testicular (testosterone) androgen. Aging is also associated with a pro-gressive decline in androgens.51
Workup of ED should always include a measured or calculated plasma free testosterone level. If this is low, a prolactin level should be checked to rule out a central problem. Screening serum testosterone levels of 105 consecutive patients with ED showed that 37 patients had previously unsuspected dis-orders of the hypothalamic-pituitary-gonadal axis. Twenty patients had hypogonadotropic hypogonadism, seven had hypergonadotrophic hypogonadism, eight had hyperprolactinemia, and two had occult hyperthyroidism. Once the specific condition was defined and
treat-cardiovascular risk factors. A number of investigators have even proposed poten-tial cardiovascular benefits of sexual activity and PDE-5 inhibitors.19,31,33,55
Follow-up at regular intervals and reassessment of all patients receiving treatment for ED is highly recommend-ed. Patients with ED should undergo evaluation of cardiovascular risk factors and assessment for subclinical CVD on a routine basis. Comprehensive evalua-tion and treatment of ED can lead to overall improved quality of life and well being for patients.
ACKNOWLEDGMENTS
Diabetes research and education at Tulane University Health Sciences Center is supported in part by the John C. Cudd Memorial Fund, the
Tullis–Tulane Alumni Chair in Diabetes, and the Susan Harling Robinson Fellowship in Diabetes Research.
REFERENCES
1NIH Consensus Conference: Impotence:
NIH Consensus Development Panel on Impo-tence. JAMA270:83–90, 1993
2Goldstein I, Lue TF, Padiabetesa-Nathan H,
Rosen RC, Steers WD, Wicker PA: Oral sildenafil in the treatment of erectile dysfunction. N Engl J Med338:1397–1404, 1998
3Shabsigh R, Klein LT, Seidiabetesan S,
Kaplan SA, Lehrhoff BJ, Ritter JS: Increased incidence of depressive symptoms in men with erectile dysfunction. Urology52:848–852, 1998
4Romeo JH, Seftel AD, Madhun ZT, Aron
DC: Sexual function in men with diabetes type 2: association with glycemic control. J Urol
163:788–791, 2000
5Feldiabetesan HA, Goldstein I, Hatzichristou
DG, Krane RJ, McKinlay JB: Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol
151:54–61, 1994
6Kaiser FE: Erectile dysfunction in the aging
man. Med Clin North Am83:1267–1278, 1999
7Richardson D, Vinik A: Etiology and
treat-ment of erectile failure in diabetes mellitus. Curr Diab Rep2:501–509, 2002
8Fink HA, Mac DR, Rutks IR, Nelson DB,
Wilt TJ: Sildenafil for male erectile dysfunction: a systematic review and meta-analysis. Arch Intern Med162:1349–1360, 2002
9Guay AT, Bansal S, Heatley GJ: Effect of
24Jiaan DB, Seftel AD, Fogarty J, Hampel N,
Cruz W, Pomerantz J, Zuik M, Monnier VM: Age-related increase in an advanced glycation end product in penile tissue. World J Urol
13:369–375, 1995
25Plante GE: Vascular response to stress in
health and disease. Metabolism51 (Suppl. 1):25–30, 2002
26Seftel AD, Vaziri ND, Ni Z, Razmjouei K,
Fogarty J, Hampel N, Polak J, Wang RZ, Fergu-son K, Block C, Haas C: Advanced glycation end products in human penis: elevation in diabetic tis-sue, site of deposition, and possible effect through iNOS or eNOS. Urology50:1016–1026, 1997
27Xie Y, Garban H, Ng C, Rajfer J,
Gonzalez-Cadavid NF: Effect of long-term passive smoking on erectile function and penile nitric oxide syn-thase in the rat. J Urol157:1121–1126, 1997
28Carson CC, Mulcahy JJ, Govier FE:
Effica-cy, safety and patient satisfaction outcomes of the AMS 700CX inflatable penile prosthesis: results of a long-term multicenter study. J Urol
164:376–380, 2000
29Brock GB, McMahon CG, Chen KK,
Costi-gan T, Shen W, Watkins V, Anglin G, Whitaker S: Efficacy and safety of tadalafil for the treatment of erectile dysfunction: results of integrated analyses. J Urol168:1332–1336, 2002
30Porst H, Rosen R, Padma-Nathan H,
Gold-stein I, Giuliano F, Ulbrich E, Bandel T: The effi-cacy and tolerability of vardenafil, a new, oral, selective phosphodiesterase type 5 inhibitor, in patients with erectile dysfunction: the first at-home clinical trial. Int J Impot Res13:192–199, 2001
31Ebrahim S, May M, Ben Shlomo Y,
McCar-ron P, Frankel S, Yarnell J, Davey Smith G: Sexu-al intercourse and risk of ischaemic stroke and coronary heart disease: the Caerphilly study. J Epidemiol Community Health56:99–102, 2002
32Feldman HA, Johannes CB, Derby CA,
Kleinman KP, Mohr BA, Araujo AB, McKinlay JB: Erectile dysfunction and coronary risk fac-tors: prospective results from the Massachusetts male aging study. Prev Med30:328–338, 2000
33Kloner RA, Mitchell M, Emmick JT:
Car-diovascular effects of tadalafil. Am J Cardiol
92:37M–46M, 2003
34Mittleman MA, Glasser DB, Orazem J:
Clinical trials of sildenafil citrate (Viagra) demonstrate noincrease in risk of myocardial infarction and cardiovascular death compared to placebo. Int J Clin Pract57:597–600, 2003
35Padma-Nathan H: Sildenafil citrate (Viagra)
and erectile dysfunction: a comprehensive four year update on efficacy, safety, and management options. Urology60:1–90, 2002
36Arruda-Olson AM, Mahoney DW, Nehra A,
Leckel M, Pellikka PA: Cardiovascular effects of sildenafil during exercise in men with known or probable coronary artery disease: a randomized crossover trial. JAMA287:719–725, 2002
37Fox KM, Thadani U, Ma PT, Nash SD,
Keating Z, Czorniak MA, Gillies H, Keltai M, for the Clinical American and European Studies of Angina and Revascularization investigators: Sildenafil citrate does not reduce exercise toler-citrate. J Clin Endocrinol Metab80:3546–3552,
1995
10Calles-Escandon J, Cipolla M: Diabetes and
endothelial dysfunction: a clinical perspective.
Endocr Rev22:36–52, 2001
11Fonseca V, Seftel A, Denne J, Fredlund P:
Impact of diabetes mellitus on the severity of erectile dysfunction and response to treatment: analysis of data from tadalafil clinical trials. Dia-betologia47:1914–1923, 2004
12Rosen RC, Riley A, Wagner G, Osterloh IH,
Kirkpatrick J, Mishra A: The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction.
Urology49:822–830, 1997
13Veves A, Akbari CM, Primavera J,
Don-aghue VM, Zacharoulis D, Chrzan JS, DeGirola-mi U, LoGerfo FW, Freeman R: Endothelial dys-function and the expression of endothelial nitric oxide synthetase in diabetic neuropathy, vascular disease, and foot ulceration. Diabetes
47:457–463, 1998
14Gazzaruso C, Giordanetti S, De Amici E,
Bertone G, Falcone C, Geroldi D, Fratino P, Sol-erte SB, Garzaniti A: Relationship between erec-tile dysfunction and silent myocardial ischemia in apparently uncomplicated type 2 diabetic patients. Circulation110:22–26, 2004
15Billups KL, Kaiser DR, Kelly AS,
Wetter-ling RA, Tsai MY, Hanson N, Bank AJ: Relation of C-reactive protein and other cardiovascular risk factors to penile vascular disease in men with erectile dysfunction. Int J Impot Res15:231–236, 2003
16Levine LA, Kloner RA: Importance of
ask-ing questions about erectile dysfunction. Am J Cardiol86:1210–1213, 2000
17Bacon CG, Mittleman MA, Kawachi I,
Gio-vannucci E, Glasser DB, Rimm EB: Sexual func-tion in men older than 50 years of age: results from the health professionals follow-up study.
Ann Intern Med139:161–168, 2003
18Derby CA, Mohr BA, Goldstein I, Feldman
HA, Johannes CB, McKinlay JB: Modifiable risk factors and erectile dysfunction: can lifestyle changes modify risk? Urology56:302–306, 2000
19Kostis J, Jackson G, Rosen R, et al.: Sexual
dysfunction and cardiac risk: the 2nd Princeton Consensus Conference. Am J Cardiol.In press
20Nicolosi A, Glasser DB, Moreira ED, Villa
M: Prevalence of erectile dysfunction and associ-ated factors among men without concomitant dis-eaes: a population study.Int J Impot Res
15:253–257, 2003
21Esposito K, Giugliano F, Di Palo C,
Giugliano G, Marfella R, D’Andrea F, D’Armien-to M, Giugliano D: Effect of lifestyle changes on erectile dysfunction in obese men: a randomized controlled trial. JAMA291:2978–2984, 2004
22Colberg SR, Stansberry KB, McNitt PM,
Vinik AI: Chronic exercise is associated with enhanced cutaneous blood flow in type 2 dia-betes. J Diabetes Compl16:139–145, 2002
23De Angelis L, Marfella MA, Siniscalchi M,
Marino L, Nappo F, Giugliano F, De Lucia D, Giugliano D: Erectile and endothelial dysfunction in type II diabetes: a possible link. Diabetologia
44:1155–1160, 2001
ance in men with erectile dysfunction and chronic stable angina. Eur Heart J24:2206–2212, 2003
38Herrmann HC, Chang G, Klugherz BD,
Mahoney PD: Hemodynamic effects of sildenafil in men with severe coronary artery disease. N Engl J Med342:1622–1626, 2000
39Reffelmann T, Kloner RA: Effects of
silde-nafil on myocardial infarct size, microvascular function and acute ischemic left ventricular dila-tion. Cardiovasc Res59:441–449, 2003
40Thadani U, Smith W, Nash S, Bittar N,
Glasser S, Narayan P, Stein RA, Larkin S, Mazzu A, Tota R, Pomerantz K, Sundaresan P: The effect of vardenafil, a potent and highly selective phosphodiesterase-5 inhibitor for the treatment of erectile dysfunction, on the cardiovascular response to exercise in patients with coronary artery disease. J Am Coll Cardiol40:2006–2012, 2002
41Morganroth J, Ilson BE, Shaddinger BC,
Dabiri GA, Patel BR, Boyle DA, Sethuraman VS, Montague TH: Evaluation of vardenafil and silde-nafil on cardiac repolarization. Am J Cardiol
93:1378–1383, 2004
42Padma-Nathan H, Hellstrom WJ, Kaiser FE,
Labasky RF, Lue TF, Nolten WE, Norwood PC, Peterson CA, Shabsigh R, Tam PY: Treatment of men with erectile dysfunction with transurethral alprostadil. Medicated Urethral System for Erec-tion (MUSE) Study Group. N Engl J Med
336:1–7, 1997
43Benet AE, Sharaby JS, Melman A: Male
erectile dysfunction assessment and treatment options. Compr Ther20:669–673, 1994
44Moyad MA, Hathaway S, Ni HS:
Tradition-al Chinese medicine, acupuncture, and other alternative medicines for prostate cancer: an introduction and the need for more research. Sem Urol Oncol17:103–110, 1991
45Guay AT, Spark RF, Jacobson J, Murray FT,
Geisser ME: Yohimbine treatment of organic erectile dysfunction in a dose-escalation trial. Int J Impot Res14:25–31, 2002
46Ernst E, Pittler MH: Yohimbine for erectile
dysfunction: a systematic review and meta-analy-sis of randomized clinical trials. J Urol
159:433–436, 1998
47Morales A: Yohimbine in erectile
dysfunc-tion: the facts. Int J Impot Res12:570–574, 2001
48Ruck B, Shih RD, Marcus SM:
Hyperten-sive crisis from herbal treatment of impotence.
Am J Emerg Med17:317–318, 1999
49Zimmerman GA, McIntyre TM, Prescott
SM: Adhesion and signaling in vascular cell-cell interactions. J Clin Invest98:1699–1702, 1996
50Tan RS, Pu SJ: Impact of obesity on
hypog-onadism in the andropause. Int J Androl
25:195–201, 2002
51Leifke E, Gorenoi V, Wichers C, Von Zur
MA, Von Buren E, Brabant G: Age-related changes of serum sex hormones, insulin-like growth factor-1 and sex-hormone binding globu-lin levels in men: cross-sectional data from a healthy male cohort. Clin Endocrinol (Oxf)
53:689–695, 2000
52Spark RF, White RA, Connolly PB:
56Jevtich MJ, Edson M, Jarman WD, Herrera
HH: Vascular factor in erectile failure among dia-betics. Urology19:163–168, 1982
57Burchardt T, Burchardt M, Karden J,
Buttyan R, Shabsigh A, de la Taille A, Ng PY, Anastasiadis AG, Shabsigh R: Reduction of endothelial and smooth muscle density in the cor-pora cavernosa of the streptozotocin induced dia-betic rat. J Urol 164:1807–1811, 2000
58Bemelmans BL, Meuleman EJ, Doesburg
WH, Notermans SL, Debruyne FM: Erectile dys-function in diabetic men: the neurological factor revisited. J Urol151:884–889, 1994
59Vernet D, Cai L, Garban H, Babbitt ML,
Murray FT, Rajfer J, Gonzalez-Cadavid NF: Reduction of penile nitric oxide synthase in dia-betic BB/WORdp (type I) and BBZ/WORdp into hypothalamic-pituitary-gonadal dysfunction.
JAMA 243:750–755, 1980
53Fukui M, Kitagawa Y, Nakamura N, Kadono
M, Mogami S, Hirata C, Ichio N, Wada K, Hasegawa G, Yoshikawa T: Association between serum testosterone concentration and carotid ath-erosclerosis in men with type 2 diabetes. Dia-betes Care26:1869–1873, 2003
54Rhoden EL, Morgentaler A: Risks of
testos-terone-replacement therapy and recommenda-tions for monitoring. N Engl J Med350:482–492, 2004
55Reffelmann T, Kloner RA: Therapeutic
potential of phosphodiesterase 5 inhibition for cardiovascular disease. Circulation108:239–244, 2003
(type II) rats with erectile dysfunction.
Endocrinology 136:5709–5717, 1995