ARTICLE
Decade of Experience With Vascular Rings at a
Single Institution
Carrie Humphrey, MDa, Kim Duncan, MD, FACSb, Scott Fletcher, MD, FAAP, FACCc
aDepartment of Pediatrics andcDepartment of Pediatrics and Radiology, Joint Division of Pediatric Cardiology, Department of Cardiovascular Magnetic Resonance Imaging-Children’s Hospital, Creighton University/University of Nebraska Medical Center/Children’s Hospital, Omaha, Nebraska;bDepartment of Surgery, Section of Cardiothoracic Surgery, Nebraska Medical Center, Omaha, Nebraska
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.Over the past decade, the diagnostic workup of vascular rings has changed at our institution. Despite surgical intervention, we have observed long-term aerodigestive issues in some patients. In an effort to better characterize these pre-and postoperative issues, we reviewed a decade of experience at our institution.
METHODS.We performed a complete chart review of all patients identified as having surgical intervention for vascular ring between January 1993 and December 2003. A questionnaire was mailed to the family of each patient to ascertain a subjective assessment of long-term postoperative issues.
RESULTS.Thirty-eight patients were reviewed and categorized as to specific arch anomaly. Associated cardiac anomalies were present in 29% of patients. Chronic feeding difficulties persisted in 18% of patients, and airway issues remained in nearly half of the patients. Patients with underlying genetic syndromes had less resolution of symptoms compared with nonsyndromic children. Chronic respira-tory symptoms were present in 80% of patients operated ⬍6 months, 15% if operated between 6 months and 3 years, and 42% of patients operated after 3 years of age.
CONCLUSIONS.Aerodigestive issues may persist after vascular ring division despite initial improvement. Accurate preoperative anatomic imaging is imperative to surgical planning.
www.pediatrics.org/cgi/doi/10.1542/ peds.2005-1674
doi:10.1542/peds.2005-1674
Key Words
vascular ring, imaging, chronic symptoms
Abbreviations
DAA— double aortic arch
RALL—right aortic arch with persistent left ligament
ASA/RDA—aberrant right subclavian artery/left aortic arch with right descending aorta
RA/RLIA—right arch with a retroesophageal left innominate artery MRA—magnetic resonance angiography CT— computed tomography
Accepted for publication Nov 4, 2005
Address correspondence to Scott Fletcher, MD, FAAP, FACC, Department of Pediatrics and Radiology, Joint Division of Pediatric Cardiology, Cardiovascular Magnetic Resonance Imaging-Children’s Hospital, Creighton University/University of Nebraska Medical Center/Children’s Hospital, 8200 Dodge St, Omaha, NE 68114-4113. E-mail: sfl[email protected]
C
ONGENITAL DEFECTS OFthe aortic arch, also known as vascular rings, constitute a set of anomalies that can cause compression of the esophagus and/or trachea. The compression can result in symptoms characterized by upper airway symptoms or dysphagia. Vascular rings are classified according to embryologic, pathologic, and radiographic criteria.There is a wide range in the presentation of patients with vascular rings from severe respiratory distress after birth or completely asymptomatic for life. The most com-mon presenting symptoms are inspiratory stridor, dys-phagia, wheezing, dyspnea, cough, and recurrent respi-ratory tract infections.1 Because of the nonspecific nature and high prevalence of these symptoms in the pediatric population and the relatively rare incidence of a vascular ring, the diagnosis is often overlooked. It is important for the general pediatrician to be familiar with the condition and the appropriate diagnostic workup. Little data are published regarding the long-term status of patients after repair/division of vascular rings.
We performed a retrospective study of 38 children with true vascular rings to analyze their presenting symptoms, diagnostic procedures, and outcomes. The purpose of this study was to describe the clinical presen-tation of children with vascular rings, the use of different diagnostic techniques, and the follow-up of children af-ter surgical inaf-tervention.
PATIENTS AND METHODS
Clinical records of 38 patients diagnosed with a vascular ring between January 1993 and December 2003 were examined retrospectively. Presenting symptoms in-cluded a history of inspiratory stridor, wheezing, dys-pnea, cough, dysphagia, and recurrent respiratory tract infections. Diagnostic procedures performed as part of the workup were quite varied and were “dependent” on the physician subspecialty evaluating the patient. Tests included chest radiograph, echocardiography, barium swallow, angiography, bronchoscopy, computed tomog-raphy (CT) scan, and cardiovascular MRI. Associated anomalies, treatment, and postoperative follow-up were also recorded.
The vascular rings in our study were classified accord-ing to Weinberg2 with the following categories repre-sented in our study population:
1. Double aortic arch (DAA): both right and left arches are present with variations, including both arches widely patent, hypoplasia of 1 arch (usually the left), and atresia of 1 arch (usually the left). In addition, a ductus arteriosus or ligamentum may be present.
2. Right aortic arch with persistent left ligament (RALL): right arch with diverticulum of Kommerell with sev-eral variations, including (a) mirror image branching; or b) first branch: the left carotid artery, second branch: the right carotid artery, third branch: the
right subclavian artery, and fourth branch: a retroe-sophageal left subclavian artery. The left ductus arte-riosus or ligamentum arteriosum connects from the diverticulum to the pulmonary artery, producing a vascular ring.
3. Aberrant right subclavian artery/left aortic arch with right descending aorta (ASA/RDA): the brachioce-phalic branches are first, the right carotid artery; sec-ond, the left carotid; third, the left subclavian; and fourth, a retroesophageal right subclavian artery aris-ing from the distal aortic arch. Ductus ligamentum connects the thoracic aorta to the proximal right pul-monary artery.
4. Right arch with a retroesophageal left innominate artery (RA/RLIA): the sequence of brachiocephalic vessels is right carotid, right subclavian, and retroe-sophageal left innominate artery. The ductus arterio-sus or ligamentum arteriosum completes a vascular ring as it connects the left pulmonary artery with the innominate artery.
RESULTS
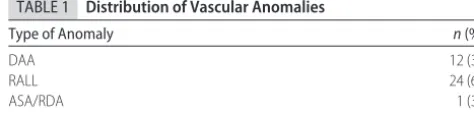
Data from chart review of 14 girls and 24 boys were studied. The male to female ratio was 1.7 to 1. The age at the time of operation ranged from 1 week to 19 years (median age, 14.5 months). The types of vascular rings are shown in Table 1. The presenting symptoms are shown in Table 2. Respiratory symptoms were variably described in symptomatic patients but present in every patient with aerodigestive symptoms. Right aortic arch with a left-sided patent ductus or a ductus ligamentum was the most common type of vascular ring followed by DAA. If an atretic segment of DAA was present, this was uniformly distal to the left subclavian artery. Only 2 patients were initially asymptomatic; one had a RA/ RLIA and the other had a RALL. Esophageal symptoms were present in 50% of patients but never presented independent of respiratory symptoms.
Associated anomalies were found in 18 (47%) of 38 patients as shown in Table 3. In total, 18 associated anomalies were found of which the majority were car-diac anomalies (11 of 38 [29%]) as shown in Table 3. The noncardiac anomalies included a tracheoesophageal fistula and syndromes or associations such as DiGeorge, Down, CHARGE (coloboma, congenital heart disease, choanal atresia, mental and growth retardation, genital anomalies, and ear malformations and hearing loss), PHACE (posterior fossa malformations, hemangiomas,
TABLE 1 Distribution of Vascular Anomalies
Type of Anomaly n(%)
DAA 12 (31)
RALL 24 (63)
ASA/RDA 1 (3)
arterial anomalies, coarctation of the aorta and cardiac defects, eye abnormalities, and sternal defects), and ve-locardiofacial. After surgical ring division, all patients received immediate improvement in aerodigestive symptoms; however, 41% had chronic respiratory diffi-culties, including noisy breathing with exertion or chronically prescribed “asthma medication.” Three pa-tients with chronic respiratory symptoms had a BMI ⬎95% for age and this may have contributed to respi-ratory symptoms. No patient had severe exercise intol-erance that prompted additional intervention. Chronic feeding difficulties persisted in 16% of patients, 1 with a tracheoesophageal fistula experienced dysphagia and 2 syndromic children had gastroesophageal reflux. Late repair (⬎3 years of age) was associated with persistent symptoms in 50% of patients. Early repair (⬍6 months of age) of the vascular ring was associated with chronic respiratory issues in 80% of patients.
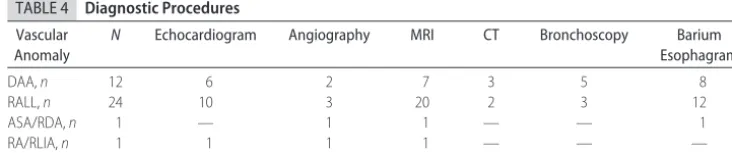
Diagnostic Procedures
The diagnostic procedures performed on the patients are shown in Table 4. The 2 most preferred studies for documenting the presence of a vascular anomaly were cardiovascular MRI (75%) and barium swallow (58%). Barium swallow was often used as an initial screening method followed by cardiovascular MRI or
echocardio-gram for additional delineation of the vascular anomaly and identification of additional congenital heart abnor-malities.
CT scans were performed on an ultrafast single-slice Philips Secura system (Eindhoven, Netherlands) with scan time ranging from 25 to 40 seconds. Four of 5 CT scans were done before full establishment of our insti-tution’s cardiac MRI program. The average radiation dose for CT scans was roughly 6 mSv per slice with enough slices to cover the thorax (range: 30 –50 slices). MRI/magnetic resonance angiography (MRA) scans were performed on a 1.5-Tesla Philips Intera system with a cardiac package. In patients ⬍6 years of age, cardiac MRI required sedation. Sedation was 50 mg/kg chloral hydrate for infants, 75 mg/kg for children 1 to 3 years of age, and 5 mg/kg oral pentobarbital for children 3 to 6 years. The same sedation regime was used in the 4 young patients undergoing CT scan; the fifth CT pa-tient did not require sedation. When sedation was ad-ministered for MRI, a registered nurse and the director of cardiovascular MRI, who is certified in sedation manage-ment was present in the MRI suite. Patients had contin-uous pulse oximetry and electrocardiographic monitor-ing. Sedated CT patients were monitored by a registered nurse. When “possible vascular ring” was the study in-dication for a cardiovascular MRI, a standard spin echo
TABLE 2 Distribution of Symptoms
Vascular Anomaly
N No
Symptoms
Wheezing Stridor Dyspnea Cough Dysphagia Recurrent Respiratory Tract Infection
DAA,n 12 — 4 4 2 — 9 6
RALL,n 24 1 3 11 7 3 9 5
ASA/RDA,n 1 — — — 1 — 1 —
RA/RLIA,n 1 1 — — — — — —
Total,n(%) 38 2 (6) 7 (19) 15 (42) 10 (28) 3 (8) 19 (50) 11 (31)
TABLE 3 Associated Anomalies: Relative Occurrence of Congenital Anomalies per Vascular Anomaly
Vascular Anomaly
N VSD TOF CoA ASD PDA TGA Noncardiac Total,
n(%)
DAA,n 12 — — — — — — 2 2 (5)
RALL,n 24 5 1 — — 4 — 4 14 (36)
ASA/RDA,n 1 — — — — — — 1 1 (3)
RA/RLIA,n 1 — — 1 — — — — 1 (3)
Total,n(%) 38 5 (14) 1 (3) 1 (3) — 4 (10) — 7 (18) 18 (47)
VSD indicates ventricular septal defect; TOF, tetralogy of Fallot; CoA, coarctation of the aorta; ASD, atrial septal defect; PDA, patent ductus arteriosus; TGA, transposition of the great arteries.
TABLE 4 Diagnostic Procedures
Vascular Anomaly
N Echocardiogram Angiography MRI CT Bronchoscopy Barium Esophagram
DAA,n 12 6 2 7 3 5 8
RALL,n 24 10 3 20 2 3 12
ASA/RDA,n 1 — 1 1 — — 1
RA/RLIA,n 1 1 1 1 — — —
technique was used for black blood imaging in 3 orthog-onal planes followed by gadolinium contrast-enhanced angiography with 3-dimensional reconstruction. An-giography performed in the catheterization laboratory was used in the initial study period but became obsolete since 1997 at our institution.
Treatment
Thirty-five of 38 patients underwent surgical division of the vascular ring through a left lateral muscle sparing thoracotomy. One patient with an RDA with the last brachiocephalic vessel arising the right subclavian artery and right sided ductal ligamentum required a right lat-eral thoracotomy. The patient with a RA/RLIA was re-paired with a midline sternotomy. A third patient, with bilateral ducts, had a right-sided ductus ligated through a right thoracotomy and the ring divided through a left thoracotomy at subsequent operation. Two patients who were diagnosed with vascular rings while asymptomatic underwent surgical repair as a result of development of mild symptoms of dysphagia in 1 patient, and the second patient had severe coarctation of the distal right aortic arch who received repair through a midline sternotomy. The median age of surgical repair was 14.5 months with a range from 1 week to 19 years. There was no intraop-erative mortality, and all symptomatic patients reported initial improvement in symptoms on postoperative fol-low-up within 4 to 6 weeks of surgery.
Postoperative Follow-up
A survey was sent in April 2004 by mail to the families of the 38 patients. Twenty-four responses were ob-tained. The questions in the survey were the following:
1. Did your child have any breathing difficulties before surgery?
2. Does your child have any current difficulties breath-ing?
3. Does your child use any respiratory medications such as inhalers?
4. Did your child have any feeding issues before sur-gery?
5. Does your child have any current feeding issues related to difficulty swallowing?
6. Is your child’s growth and development normal?
7. How would you rate your child’s exercise tolerance as: (a) poor, (b) fair, (c) average, or (d) exceptional?
8. What is the major limitation to your child’s exercise tolerance?
9. What are your child’s current age, height, and weight?
10. Does your child have any concerns about the scar at the site of the surgical incision?
Returned surveys (Table 5) revealed the majority of patients (94%) had breathing difficulties before surgery, whereas feeding problems were present in 50% of pa-tients before treatment. In general, the early results of surgical treatment were excellent. Survey results re-vealed slightly more than half of the patients with pre-operative breathing difficulties were now symptom-free. Just less than half of the patients were still having respi-ratory problems, but all were described as improved over preoperative status. Thirteen percent remained on inhal-ers for presumed “reactive airway disease.” Approxi-mately two thirds of patients with preoperative feeding issues were relieved of symptoms after surgery. Interest-ingly, of the 7 patients with additional noncardiac anom-alies, including tracheoesophageal fistula and syndromes or associations such as DiGeorge, Down, PHACE, velo-cardiofacial, and CHARGE, only 1 patient with Down syndrome had complete resolution of symptoms after surgery. Exercise tolerance was subjectively average or above in all patients without a syndrome.
DISCUSSION
The branchial arch system provides 6 pairs of primitive aortic arches that develop into the aortic arch and its branches and the pulmonary system during fetal life. Vascular rings are caused by abnormal regression of the branchial system and may result in encirclement and compression of the trachea, esophagus, or both. Symp-tomatic vascular rings are often diagnosed early in life. Traditional teaching has been the greater the delay be-tween the first presentation of symptoms and the time of diagnosis and treatment, the likely higher risk of tra-cheomalacia, esophageal dysmotility, and persistence of symptoms. The most common symptoms of a vascular ring are inspiratory stridor, dyspnea, cough, wheezing, dysphagia, and recurrent respiratory tract infections. These symptoms are common during early childhood, but their persistence should alert the general pediatri-cian to the possibility of a vascular ring.3–6 Other suspi-cious indicators are respiratory symptoms that are not transient and that do not respond to bronchodilators. We found chronic postoperative symptoms were related to age of operation with persistent symptoms in 80% of patients repaired before 6 months, 15% when operated
TABLE 5 Preoperative and Chronic Incidence of Respiratory and Feeding Difficulties (Survey Response)
Vascular Anomaly
N PRD CRD PFD CFD
DAA,n 6 6 5 6 1
RALL,n 18 16 5 7 3
ASA/RDA,n 1 1 1 1 —
RA/RLIA,n 1 — — — —
Total,n(%) 26 23 (88) 11 (42) 14 (54) 4 (15)
between 6 months and 3 years, and 42% when operated after age 3. We postulate that early surgery is performed in a substrate of worse pathology, whereas late repair is likely related to less reversibility of tracheobronchoma-lacia.
It is also important to recognize that associated car-diac anomalies are not infrequent (29% of our cases), and therefore thorough cardiac evaluation is necessary. There are many diagnostic procedures that can be per-formed to make the diagnosis of a vascular ring, and it is important to determine the safest and most accurate. A chest radiograph can alert the pediatrician to the possi-bility of a vascular ring by finding a right-sided aortic arch and tracheal compression. Echocardiography is of-ten useful as a complementary procedure that helps clarify vascular anatomy preoperatively and evaluate for additional intracardiac anomalies. Bronchoscopy often is used to diagnose upper airway problems and can usually indicate the level of obstruction but is unable to define the precise vascular anatomy. (Bronchoscopy led to a MRI/MRA study in several patients that were found to have “innominate artery syndrome” secondary to late takeoff of the artery resulting in tracheomalacia. These patients were excluded from this review because this is not a true vascular ring.) Bronchoscopy is an invasive procedure and can temporarily worsen patients’ symp-toms by causing tracheal edema.
A widely used, noninvasive screening method for vascular rings is barium swallow.7The barium swallow demonstrates posterior indentation of the esophagus in all vascular anomalies except the rare pulmonary sling. A pulmonary sling produces an anterior indentation of the esophagus, and an increased space between the esophagus and trachea occurs at the same level on esophagram. However, the exact anatomy of the vascu-lar ring or any additional cardiac anomalies cannot be determined by esophagram. Several patients underwent a cardiac MRI/MRA to follow-up on “possible ring” in-terpretation by a pediatric radiologist and were found to have left aortic arch with ASA. These patients are not true vascular rings and were also excluded from our study.
Angiography was previously the gold standard for diagnosis, but it is an invasive procedure and carries risks resulting from ionizing radiation exposure and the use of iodinated contrast agents. At some institutions, CT screening is favored as detailed in a recent publication6; however, it also exposes the child to ionizing radiation with potential long-term consequences. We believe a single chest CT scan at our institution is roughly equiv-alent to 40 years of an annual chest radiograph evalua-tion. Although the CT technique can be modified to reduce radiation exposure for some applications, studies designed for vascular detail typically have high radiation exposure, and young infants may be more sensitive to the effects of radiation than older patients.8
The new gold standard at our institution and others9 has become cardiovascular thoracic MRI/MRA, which is noninvasive, uses no radiation, and is performed as a monitored outpatient procedure in most cases. In our experience, sedation with chloral hydrate or oral pento-barbital provides adequate and safe sedation for the young child. We have had no sedation-related problems, and it was effective in facilitating diagnostic images in all cases. The typical vascular ring study was completed in 30 minutes. MRI/MRA is not only able to accurately diagnose the vascular ring, but also define the relation-ship of the nonvascular structures such as the esophagus and trachea to the vessels. We believe MRI/MRA is superior to echocardiography in delineating the extra cardiothoracic vasculature and evaluating possible air-way compression. In addition to routine chest radio-graph, cardiovascular MRI was the only diagnostic pro-cedure used in 5 (13%) of 38 before surgical correction of the vascular ring and has become the authors’ recom-mended single modality of choice.
The imaging modality of choice should, however, depend on local expertise and equipment availability. When a right aortic arch is suspected on the chest radio-graph, the precise anatomy obtained by tomographic imaging with MRI/CT may potentially alter the surgical approach in some patients. In our study, MRI led to a right thoracotomy in 1 of our patients and a midline sternotomy in a second. A third premature syndromic infant with bilateral ducti and a small pressure-restric-tive membranous ventricular septal defect had bilateral thoracotomy. The patient’s left-sided ductus was not visualized by echo or MRI before surgically ligating a large right-sided ductus. The patient’s small size (⬍2 kg) may have contributed to this error or the left-sided duc-tus may have opened after the initial surgery.
Limitations
quite interesting and will now be considered in our long-term strategy.
CONCLUSIONS
Prolonged or recurrent respiratory difficulties and/or dysphagia should alert the pediatrician to the possibility of a vascular ring. When a vascular ring is suspected from history and physical examination, routine chest radiograph and barium swallow can be performed with a high yield for the presence of a ring. However, increas-ingly, cardiovascular MRI is being used to accurately delineate the specific vascular anatomy preoperatively and, in rare instances, MRI can alter the surgical ap-proach from the standard left minithoracotomy. All vas-cular rings that cause symptoms should be surgically corrected. Operative risks are relatively small. Intu-itively, early recognition and surgical treatment of symp-tomatic vascular rings may allow the greatest possibility of normal growth of the trachea, esophagus, and relief of aerodigestive symptoms; however, when severe early airway symptoms are present, this may be indicative of a worse pathology and patient substrate. Despite ring di-vision and improvement in symptoms, some patients with conventional ring division will have long-term is-sues of the aerodigestive tract.
REFERENCES
1. Bakker DAH, Berger RMF, Witsenburg M, et al. Vascular rings: a rare cause of common respiratory symptoms. Acta Paediatr.
1999;88:947–952.
2. Weinberg PM.Moss and Adams’ Heart Disease in Infants, Children, and Adolescents Including the Fetus and Young Adult.6th ed, Vol II. Philadelphia, PA: Lippincott Williams & Wilkins; 2001: 707–735 3. Woods RK, Sharp RJ, Holcomb GW, et al. Vascular anomalies and tracheoesophageal compression: a single institution’s 25-year experience.Ann Thorac Surg.2001;72:434 – 439
4. Longo-Santos LR, Maksoud-Filho JG, Tannuri U, et al. Vascular rings in childhood: diagnosis and treatment [in Portuguese].
J Pediatr (Rio J).2002;78:244 –250
5. Subramanyan R, Venugopalan P, Narayan R. Vascular rings: an important cause of persistent respiratory symptoms in infants and children.Indian Pediatr.2003;40:951–957
6. Backer CL, Mavroudis C, Rigsby CK, et al. Trends in vascular ring surgery.J Thorac Cardiovasc Surg.2005;129:1339 –1347 7. Backer CL, Ilbawi MN, Idriss FS, et al. Vascular anomalies
caus-ing tracheoesophageal compression. Review of experience in children.J Thorac Cardiovasc Surg.1989;97:725–731
8. Brenner DJ, Elliston DC, Hall EJ, et al. Estimated risks of radi-ation-induced fatal cancer from pediatric CT.AJR Am J Roentge-nol.2001;176:289 –296
DOI: 10.1542/peds.2005-1674 originally published online April 3, 2006;
2006;117;e903
Pediatrics
Carrie Humphrey, Kim Duncan and Scott Fletcher
Decade of Experience With Vascular Rings at a Single Institution
Services
Updated Information &
http://pediatrics.aappublications.org/content/117/5/e903 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/117/5/e903#BIBL This article cites 8 articles, 0 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/cardiology_sub
Cardiology
http://www.aappublications.org/cgi/collection/pulmonology_sub
Pulmonology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2005-1674 originally published online April 3, 2006;
2006;117;e903
Pediatrics
Carrie Humphrey, Kim Duncan and Scott Fletcher
Decade of Experience With Vascular Rings at a Single Institution
http://pediatrics.aappublications.org/content/117/5/e903
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.