Long-Term Outcomes After Laparoscopy-Assisted Gastrectomy for
Advanced Gastric Cancer: Analysis of Consecutive 106 Experiences
JUNHYUN LEE,MD ANDWOOK KIM,MD,PhD*
Department of Surgery, College of Medicine, The Catholic University of Korea, Seoul, South Korea
Background and Objectives:The purpose of this retrospective study is to suggest the possibility of laparoscopy-assisted gastrectomy (LAG) for advanced gastric cancer (AGC) through long-term outcomes.
Methods:Of 283 patients with gastric cancer who underwent LAG with extraperigastric (D2) lymphadenectomy between January 2004 and February 2009, 106 were pathologically confirmed with AGC and analyzed.
Results:There were 75 men and 31 women, with a mean age of 61.411.7 years. There were 32 total gastrectomies and 74 distal gastrectomies with D2 lymphadenectomy. The mean tumor size was 4.82.6 cm. The mean numbers of retrieved and metastatic lymph nodes were 34.315.3 and 5.48.7, respectively. There was no lymph node metastasis in 44 patients (41.5%), and there were 35 grade T2a, 51 T2b, and 20 T3 lesions. There were 10 operation-related morbidities (9.4%) and one postoperative death (0.9%) from hepatic failure. The overall and disease-free survival rates were 81.4% and 72.4%, respectively. Tumors recurred in 17 patients (16.0%) during the follow-up periods (median 21.5 months; range 2–60).
Conclusions:LAG for AGC might be considered as a minimally invasive treatment in selected cases, but further study comparing it with open gastrectomy will be needed.
J. Surg. Oncol. 2009;100:693–698. ß2009 Wiley-Liss, Inc.
K
EYW
ORDS: laparoscopy; D2 lymph node dissection; recurrence; overall and disease-free survival rates
INTRODUCTION
Since laparoscopy-assisted distal gastrectomy (LADG) for early gastric cancer (EGC) was first reported in 1994 by Kitano et al. [1], the application of this procedure has been increasing rapidly in countries such as Korea and Japan, which have a high prevalence of EGC. Many authors have reported their experience with minimally invasive surgery of the stomach, reporting the adequacy of resection margins and nodal clearance rates [2–5]. There are potential benefits of laparoscopy-assisted gastrectomy (LAG) for treating patients with EGC and infrequent lymph node metastases compared with the conventional open procedure, including less postoperative pain, faster recovery and shorter hospital stays [2,3]. However, there remain controversies in terms of its oncological benefits. Moreover, application of LAG for the treatment of patients with AGC remains controversial because of the technical difficulty of carrying out D2 lymphadenectomy and insufficient data related to the procedure’s oncological adequacy. Notably, LAG for treating patients with AGC must overcome problems associated with incomplete D2 lymphadenectomy resulting from the difficult anatomical approach via a laparoscopic view. Despite recent innovative progress in laparoscopic tools and improvements in surgical experience, only a few reports have addressed the application of a laparoscopic procedure to patients with AGC in terms of oncological benefits or risks. In the present study, we describe our experience with LAG in the treatment of patients with AGC and evaluate its safety in terms of clinicopathological characteristics, surgical outcomes and long-term follow-up results.
MATERIALS AND METHODS
Patients
Between January 2004 and February 2009, 283 patients with gastric cancer underwent LAG, which was performed by one surgeon with permission of our institutional review board. Among these patients,
106 were pathologically confirmed with AGC and enrolled in this study. The indication for LAG was confined initially to patients with EGC but, after the surgeon had overcome a learning curve (40 LADGs), it was extended gradually to tumors graded clinically T2N1M0 on the UICC classification scheme. Clinical grading was preferentially performed by gastrofiberscopy and high-resolution multi-directional computed tomography with air-filling of the stomach (CT gastrography), and then endoscopic ultrasound was performed if not clearly graded by former studies. However, conversion to an open procedure was carried out when there was obvious intraoperative evidence of serosal invasion during the LAG procedure. Laparoscopic D2 lymphadenectomy was routinely performed in all cases. All patients except one perioperaive mortality were followed up pros-pectively for survival analysis. We reviewed the oncological feasibility of LAG for AGC in terms of clinicopathological characteristics, morbidity, and recurrence and survival rates. All procedures were based strictly on the patient’s individual decision after obtaining informed consent, following advice concerning the surgical and oncological risks. Postoperatively, six cycles of adjuvant chemo-therapy with intravenous 5-fluorouracil (5-FU) and cisplatinum was introduced in patients with T3 tumor or lymph node metastasis. Follow-up data were obtained from office records, and computed tomography scans, gastrofiberscopy and assays for serologic tumor markers were performed on patients every 6 months after surgery.
*Correspondence to: Wook Kim, MD, PhD, Division of GI Surgery, Department of Surgery, St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, #62 Youido-dong, Yeongdeungpo-gu, Seoul 150-713, South Korea. Fax: 82-2-786-0802.
E-mail: [email protected]
Received 31 May 2009; Accepted 24 July 2009 DOI 10.1002/jso.21400
Published online 3 September 2009 in Wiley InterScience (www.interscience.wiley.com).
Operative Procedure
Before operative procedure, all patients had worn pneumatic compressive stocking for preventing deep vein thrombosis. Immedi-ately after skin incision, prophylactic antibiotics was intravenously administered. Total omentectomy with D2 lymphadenectomy was performed for all patients according to the lymph node classification by the Japanese Gastric Cancer Association [6]. All patients were placed in the supine position and subjected to a 15–208reverse Trendelenberg position. An initial 10 mm trocar for a 308rigid electrolaparoscope was inserted through the infraumbilical area using an open technique. After establishing a pneumoperitoneum with carbon dioxide (CO2), two additional 12 and 5 mm trocars were introduced as main ports into the right side at 2 cm above the umbilicus and just below the costal margin, respectively. Then, a 10 mm trocar was inserted 4 cm below the xyphoid process for traction of the liver, and a 5 mm trocar was inserted in the left mid-clavicular line 2 cm above the umbilicus as an accessory port. The operator stood on the right side of the patient, and the CO2
pneumoperitoneum was maintained at 12–14 mmHg during the operation. First, a routine exploration of the abdominal cavity was carried out. The stomach and peritoneal cavity were examined carefully to exclude any serosal invasion and distant metastasis. Division of the greater omentum along the avascular plane, using ultrasonic-activated scissors (Laparoscopic Coagulation Shears [LCS1]; Ethicon Endo-Surgery, Cincinnati, OH), was started from the middle part of the transverse colon and extended up to the lower pole of the spleen. The left gastroepiploic vessels were divided to remove lymph node number 4sb. Then, the right side omentum was divided along the transverse colon and hepatic flexure. The dissection was continued towards the inferior border of the pancreas neck portion while identifying the middle colic vessels, and lymph nodes around the superior mesenteric vein (number 14v) were removed. The right gastroepiploic vessels were then exposed and divided at their origin with removal of lymph node number 6. After dissection of the anterior plane of the hepatoduodenal ligament, the right gastric artery was divided with double clips at its origin, and lymph node number 5 was removed. The duodenum was transected about 2 cm distal from the pylorus, using a 45 mm endoscopic stapling device. The common hepatic artery was then identified and skeletonized to dissect lymph nodes numbers 8a and 12a using laparoscopic dissectors and the LCS. The lymph node dissection was continued towards the celiac axis, and the left gastric vein and artery were identified and divided at their roots with removal of lymph nodes numbers 7 and 9. Then, the lymph nodes around the proximal splenic artery (number 11p) were dissected. During LATG, lymph nodes around the distal splenic artery (number 11d) and splenic hilum (number 10) were also dissected using vessel loops for traction of the splenic artery. Lymph nodes numbers 1 and 3 (including numbers 2 and 4sa during LATG) were approached along the upper portion of the lesser curvature of the stomach and dissected. Following these procedures, 4.5–5 cm vertical incision was made at the epigastrium in which 10 mm trocar located and a double-ring wound retractor (Alexis1, Applied Medical, Rancho Santa Margarita, CA) was inserted through the incision and rolled to protect and stretch it. Billroth-II or jejunal pouch interposition between the remnant stomach and duodenum (in LADG) and Roux-en-Y esophagojejunostomy (in LATG) were performed with a hand-sewing technique or using endo-scopic stapling devices via a mini-laparotomy at the upper abdomen.
Statistical Analysis
All statistical analyses were performed using the Statistical Package for the Social Science (SPSS1) version 12.0 for Windows (SPSS, Chicago, IL). Patient’s survival data was analyzed using the Kaplan–Meier method. All continuous values are presented as the meanstandard deviation.
RESULTS
Of 283 patients who underwent LAG with extraperigastric (D2) lymphadenectomy, 106 consecutive patients were pathologically proven as AGC and others were EGC. Initially, 112 patients were listed for LAG, 106 consecutive cases were eventually included after excluding six conversions for inclusion criteria (obvious serosal invasion). The demographic and clinicopathological characteristics of the patients are presented in Table I. There were 32 total gastrectomies and 74 distal gastrectomies with D2 lymphadenectomy, and all LAG had achieved R0 resection. The mean tumor size was 4.82.6 cm and there were 35 graded T2a lesions, 51 T2b lesions, and 20 T3 lesions. The numbers of retrieved and metastatic lymph nodes were 34.315.3 and 5.48.7, respectively. There was no lymph node metastasis in 44 patients (41.5%). For all 106 patients, the mean operation time was 293.063.3 min, and the mean blood loss was 346.6104.7 ml. The times to first flatus and commencing eating soft meals were 3.21.1 and 4.41.0 days, respectively, and the mean postoperative hospital stay was 11.94.1 days. There were 10 operation-related morbidities (9.4%). Adverse intraoperative events included two cases of splenic injury in LATG that led to combined splenectomy and one thermal injury to the left bile duct by LCS. In postoperative morbidities within a 30-day period, events related with surgery included duodenal stump leakage (four cases), intraluminal bleeding from the rupture of a pseudoaneurysm of the gastroduodenal artery (one case) and delayed diaphragmatic hernia (one case) and pneumonia (one case) was an only medical complication. There was no wound problem. One patient died postoperatively (0.9%) from hepatic failure (Table II). Tumor recurrence was detected in 17 cases (16.0%) during the follow-up periods (median 21.5 months, range 2–60). The main sites of recurrence were the peritoneum (five cases), the liver (five), the remnant stomach (three), para-aortic lymph nodes (two), bone (one), and the duodenal stump (one). Four patients with recurrence underwent a reoperation: one liver resection, two extended total gastrectomies for remnant gastric cancer and one pancreatico-duodenectomy for duodenal stump recurrence.
The respective overall and disease-free survival rates were 81.4% and 72.4% (Fig. 1a,b). Among patients with 86 T2 tumors, they were 89.8% and 81.0%. And according to the subclassification for depth of
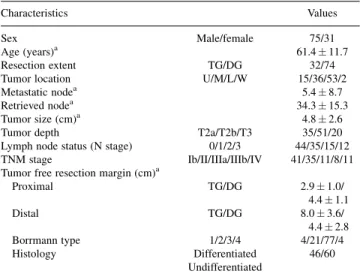
TABLE I. Clinicopathologic Characteristics in Patients With Advanced Gastric Cancer Who Underwent Laparoscopy-Assisted Gastrectomy (LAG) With D2 Lymphadenectomy
Characteristics Values
Sex Male/female 75/31
Age (years)a 61.411.7
Resection extent TG/DG 32/74
Tumor location U/M/L/W 15/36/53/2
Metastatic nodea 5.48.7
Retrieved nodea 34.315.3
Tumor size (cm)a 4.82.6
Tumor depth T2a/T2b/T3 35/51/20
Lymph node status (N stage) 0/1/2/3 44/35/15/12
TNM stage Ib/II/IIIa/IIIb/IV 41/35/11/8/11
Tumor free resection margin (cm)a
Proximal TG/DG 2.91.0/ 4.41.1 Distal TG/DG 8.03.6/ 4.42.8 Borrmann type 1/2/3/4 4/21/77/4 Histology Differentiated 46/60 Undifferentiated
TG, total gastrectomy; DG, distal gastrectomy; U, upper; M, middle; L, low; W, whole; T2a, muscularis propria; T2b, subserosa; T3, serosa exposure.
tumors, the survival and disease-free survival rates were both 100% in patients with T2a tumors, however, they were 84.1% and 71.6%, respectively, in patients with T2b tumors. In T3 tumors, they were 39.0% and 32.7%, respectively (Fig. 2a,b).
DISCUSSION
Curative resection for gastric cancer essentially requires an adequate extent of lymphadenectomy as well as gastric resection to improve therapeutic outcomes [6–8]. The general surgical community has concerns about limited lymphadenectomy for laparoscopic procedures, although several prospective clinical trials have demon-strated LADG to be superior to an open procedure because it results in less postoperative pain, faster recovery and better cosmetic results [2,3]. For distal AGC, the Japanese Gastric Cancer Association has presented complete D2 lymphadenectomy including lymph nodes numbers 11p, 12a, and 14v as the standard therapy and LADG observing this guideline necessitates a lot of experience, skill, efforts and times [6,8]. As a result, most surgeons only perform LADG for cases of EGCs, in which the rate of lymph node metastasis is not as high as in AGC and limited lymphadectomy is enough to oncological demands. However, laparoscopic tools and surgeon’s skill has been improving as time passed and Hyung et al. reported that patients with some EGCs, especially those with submucosal cancers and vascular
invasion, should undergo D2 lymphadenectomy, even if LADG with limited lymphadenectomy has an adequacy as surgical modality for EGCs [9]. Consequently, several surgeons abundantly experienced in laparoscopic procedures have attempted or accomplished laparoscopic D2 lymphadenectomy during LADG and few studies had reported the possibility of applying LADG with D2 lymphadenectomy for patients with AGC [9–11]. Since Uyama et al. first reported laparoscopy-assisted total gastrectomy with D2 lymphadenectomy and distal pancreaticosplenectomy for advanced upper-third gastric cancers in 1999, there have been several studies to determine the technical feasibility of D2 lymphadenectomy in patients with AGC [4,5,10–14]. However, there is no study showing the availability of LAG with D2 lymphadenectomy for treating patients with AGC in terms of surgical results such as morbidity, recurrence and survival rate, and this raises doubts about its suitability. Under these circumstances, we made effort to find out whether LAG with D2 lymphadenectomy had a feasibility and oncological propriety for AGC as a treatment modality.
Of 106 patients with AGC, LATG was performed in 32 and LADG in 74 patients with D2 lymphadenectomy, which is performed on equal terms with the open procedure in our institution. In LAG with D2 lymphadenectomy, special attention was required to completely remove lymph node numbers 10, 11d, 12a, and 14v, though we accomplished this safely. During LADG, initially, we identified the gastrocolic vein and mid-colic vessels as landmarks for dissecting
Fig. 1. Kaplan–Meier survival curves in 105 patients with LAG.a: Cumulative overall survival.b: Cumulative overall disease free survival. TABLE II. Operation-Related Morbidity and Postoperative Mortality in Patients With Advanced Gastric
Cancer Who Underwent Laparoscopy-Assisted Gastrectomy (LAG) With D2 Lymphadenectomy
Site Number Results
Morbidity Surgical
Intra-operative
Bleeding Spleen 2 Splenectomy
Injury Left bile duct 1 T-tube choledochostomy
Post-operative
Leakage Duodenal stump 4 Percutaneous drainage
Bleeding Pseudoaneurysm 1 Endovascular coiling
Injury Left diaphragm 1 Laparoscopic primary closurea
Medical
Infection Pneumonia 1 Administration of antibiotics
Mortality
Hepatic failure 1 Perioperative death
lymph node number 14v. For lymph node 12a, meticulous dissection with traction of the major hepatic artery and bile ducts using vessel loops was occasionally necessary. In addition, the technique of encircling and pulling the splenic artery with vessel loops reported by Hur et al. helped us to complete dissection of lymph nodes around the distal splenic artery (number 11d) and splenic hilum (number 10) without distal pancreatectomy or splenectomy in LATG [14]. As a principle, a specimen including lymph nodes was removed with en block type through mini-laparotomy protected by a double-ring wound retractor. However, lymph nodes needing frozen section or mapping could be pushed out following method without spillage or fracture of those. First, a hollow cylinder longer than length of a trocar was inserted into 10 mm trocar. Second, laparoscopic instrument was introduced through it and pulled lymph node into it. Finally, a cylinder was removed from trocar. And we occasionally used endobag for large size lymph node. Many authors have reported no major differences between LAG and ODG procedures in terms of the number of retrieved lymph nodes [3,4,11]. The mean number of retrieved lymph nodes was 34.315.3 and this result did not show great difference from other reports [3,5,11,15]. To maintain a good operation field and avoid unnecessary manipulation or traction of the stomach during LAG procedure, smaller size of tumors might be more suitable according to our experience. The mean tumor size was 4.8 cm in this study.
Regarding the reported postoperative morbidity, most reports have concerned single-center experience and retrospective results. Post-operative morbidity rates ranging from 2.5% to 25.4% have been reported for patients undergoing LAG [16–19]. There was one postoperative death (0.9%) from hepatic failure and 10 operation-related morbidities (9.4%). Our laparoscopic series included three instances of major complications related to D2 lymphadenectomy although there was no minor complication. One was a left bile duct injury, which was repaired by a T-tube choledochostomy via a mini-laparotomy and eventually required biliary metallic stenting for stricture. The second case involved rupture of a pseudoaneurysm in the gastroduodenal artery. The final case was a left side diaphragmatic injury that led to herniation of transverse colon through the thoracic cavity. The treatment for this was delayed for 8 months postoperatively because the patient reported no symptoms. The authors assume that all of these injuries occurred accidentally through use of the LCS. These unintended complications including duodenal stump leakage might lengthen postoperative hospital stay in our series. Therefore, great attention is clearly needed when using the LCS to prevent thermal
injury, especially in lymph node dissection around major vessels and the hepatoduodenal ligament. These complicated laparoscopic proce-dures, when performed by an inexperienced surgeon, might contribute to longer operation times and yield poorer recovery from the operation when compared with open distal gastrectomy (ODG). Kim et al. [20] recently identified the independent risk factors associated with postoperative complications to be patient’s sex and age, comorbidity, type of resection and the surgeon’s experience. Among these, presence of comorbidity and the surgeon’s lack of experience were also identified as independent risk factors associated with requiring a reoperation and morbidity following LAG. Nevertheless, our complication rate was similar to other case-controlled studies for surgery on patients with EGC [21,22].
In the present study for treating patients with AGC, though a small number of cases were stratified for each stage, patients who had tumor invading into the serosa (T3) as well as into the subserosa (T2b) did not show worse survival or recurrence rates compared with other reports [23–25]. Especially, among 86 T2 tumors, the overall survival and disease-free survival rates were both 100% in patients with T2a tumors and they were 84.1% and 71.6% in patients with T2b tumors, respectively. These results might support that LAG for T2a and selective T2b tumors was a feasible and safe procedure for oncologic aspect. With regard to pT3 tumors in our study, there was no clear laparoscopic image of invasion of the serosa during operation, and this was later confirmed with focal penetration of tumors. They had mostly multiple lymph node metastasis (four with N0 grade tumors, four with N1, six with N2, and six with N3), which might be related to the poor outcomes (median follow-up periods: 18 months; range 8–49; overall survival rates: 39.0%; disease-free survival rates: 32.7%). However, for patients with T3 tumors, there was no recurrence and cancer-related death among the N0 cases, and half of the patients with lymph node metastasis were still alive without recurrence. Overall survival and disease-free survival rates of 283 patients with LAG were 87.0% and 70.0%.
Laparoscopic curative surgery for serosa-exposed (T3) AGC is not yet acceptable, because there could be peritoneal seeding of malignant cells in dealing with possible metastatic lymph nodes or gastric lesion, or there was a risk of port-site recurrence, as reported [26]. However, in our experience it is impossible to avoid touching the tumor or metastatic lymph node during conventional open procedures for T3 type AGC. Therefore, concern for the possibility of peritoneal seeding resulting from application of LAG for T3 case is not persuasive. We always minimized handling of the stomach and touched it far away Fig. 2. Kaplan–Meier survival curves according to different tumor stage (T) categories.a: Cumulative overall survival.b: Cumulative overall disease free survival.
from the tumor, regardless of gross appearance. These prudent manipulations might be helpful to prevent seeding of tumor cells if focal serosal invasion is suspected. In the present study, the peritoneal recurrence was not higher than in another report, and there was no port-site recurrence [23,24].
To date, several investigations have reported no differences in recurrence or survival following LAG and ODG for EGC [2,22,27]. In our LAG series, overall survival and disease-free survival rates of 177 patients with T1 were 98.1% and 97.0% and there were two cases of recurrences occurred in liver, and these results were similar with other reports. In particular, a recent randomized controlled trial of GC showed a similar curability rate for open and laparoscopic procedures after a mean follow-up of 21.5 months [27]. Our results regarding the recurrence pattern showed no difference from other open procedures, despite the small number of cases [24,28]. The peritoneum and liver were major site for recurrence, followed by remnant stomach, lymph nodes, bone and duodenal stump. Recurrence is the most intimidatory factor in patients with gastric cancer and unfortunately, most of it has multiple sites at the time of diagnosis. The standard treatment for recurrence has not been well established, but, on the other hand few studies had demonstrated that, in cases of localized recurrence, complete resection, when achievable, may be beneficial to the patient’s survival [29,30]. Interestingly, there were four cases of reoperation for localized recurrences. In case of duodenal stump recurrence, anemia had persisted by repetitive bleeding from a recurrent tumor and there was absence of any other metastatic lesions by positron emission tomography-computed tomography (PET-CT). Another patient with solitary liver recurrence at segment 2 had been preferentially treated with second line chemotherapy and there was no change for 1 year. For these reasons, reoperations were performed and there was no evidence of recurrence for 13 and 40 months, respectively. Three patients with tumor recurrences in the remnant stomach had well-demarcated tumors with adequate proximal tumor-free margin (>3 cm) and no other lesions in preoperative gastrofiberscopic examinations. However, they showed recurrences at 12, 13, and 31 months after operation. Although the causes of these recurrences were not clear, possibly these patients originally might have microscopic lesions that were undetected in the initial evaluation. Because these recurrences were regarded as gastric remnant cancer and it was reported that surgical resection was beneficial to survival [31–33], we recommended reoperation for those patients and two underwent a extended total gastrectomy. Of two patients with reoperation, one has no recurrence for 23 months and another had died 12 months after reoperation due to multiple metastasis. Among recurrence patterns, there were few meaningful findings. All the lymph node recurrences occurred beyond two-tier lymph nodes or at distant sites such as the para-aortic, inguinal or cervical areas. This finding suggests that our laparoscopic procedure for D2 lymphadenectomy was sufficient for locally advanced cancer. On the other hand, regarding the recurrence pattern,in vivostudies have shown that laparoscopy with CO2insufflation might stimulate the
growth of dormant tumor cells into overt liver metastases [34,35]. The pattern in our study might be consistent with the theory that laparoscopy with CO2insufflation might trigger the growth of dormant
tumor cells into overt liver metastases, however, further experimental studies and clinical data collection are necessary to confirm the different recurrence pattern for LAG.
In conclusion, LAG with D2 lymphadenectomy was a feasible procedure for AGC, and the follow-up results demonstrated that it produced satisfactory surgical and oncological results, especially, for T2a and T2b. Consequently, LAG could be applied for locally advanced gastric cancer even though this might involve focal serosal exposure and perigastric lymph node metastases. However, longer follow-up studies as well as additional prospective clinical trials are needed to confirm the oncological security of LAG for patients with AGC.
ACKNOWLEDGMENTS
We have performed prospective randomized controlled trial for comparison laparoscopy-assisted distal gastrectomy with open con-ventional gastrectomy since August 25, 2008 with permission of our institutional review board and this trial was assigned at Clinicaltrials.gov (ID NCT00741676).
REFERENCES
1. Kitano S, Iso Y, Moriyama M, et al.: Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc 1994;4:146–148. 2. Huscher CG, Mingoli A, Sgarzini G, et al.: Laparoscopic versus
open subtotal gastrectomy for distal gastric cancer: Five-year results of a randomized prospective trial. Ann Surg 2005;241: 232–237.
3. Kitano S, Shiraishi N, Fujii K, et al.: A randomized controlled trial comparing open vs laparoscopy-assisted distal gastrectomy for the treatment of early gastric cancer: An interim report. Surgery 2002;131:S306–S311.
4. Noshiro H, Nagai E, Shimizu S, et al.: Laparoscopically assisted distal gastrectomy with standard radical lymph node dissection for gastric cancer. Surg Endosc 2005;19:1592–1596.
5. Song KY, Kim SN, Park CH: Laparoscopy-assisted distal gastrectomy with D2 lymph node dissection for gastric cancer: Technical and oncologic aspects. Surg Endosc 2008;22:655–659. 6. Japanese Gastric Cancer Association. Japanese Classification of Gastric Carcinoma—2nd English Edition. Gastric Cancer 1998;1: 10–24.
7. Kim JP: Current status of surgical treatment of gastric cancer. J Surg Oncol 2002;79:79–80.
8. Nakajima T: Gastric cancer treatment guidelines in Japan. Gastric Cancer 2002;5:1–5.
9. Hyung WJ, Cheong JH, Kim J, et al.: Application of minimally invasive treatment for early gastric cancer. J Surg Oncol 2004;85: 181–185.
10. Goh PM, Khan AZ, So JB, et al.: Early experience with laparoscopic radical gastrectomy for advanced gastric cancer. Surg Laparosc Endosc Percutan Tech 2001;11:83–87.
11. Ziqiang W, Feng Q, Zhimin C, et al.: Comparison of laparoscopi-cally assisted and open radical distal gastrectomy with extended lymphadenectomy for gastric cancer management. Surg Endosc 2006;20:1738–1743.
12. Uyama I, Sugioka A, Fujita J, et al.: Laparoscopic total gastrectomy with distal pancreatosplenectomy and D2 lympha-denectomy for advanced gastric cancer. Gastric Cancer 1999;2: 230–234.
13. Uyama I, Sugioka A, Matsui H, et al.: Laparoscopic D2 lymph node dissection for advanced gastric cancer located in the middle or lower third portion of the stomach. Gastric Cancer 2000;3:50– 55.
14. Hur H, Jeon HM, Kim W: Laparoscopic pancreas- and spleen-preserving D2 lymph node dissection in advanced (cT2) upper-third gastric cancer. J Surg Oncol 2008;97:169–172.
15. Tanimura S, Higashino M, Fukunaga Y, et al.: Laparoscopic gastrectomy with regional lymph node dissection for upper gastric cancer. Br J Surg 2007;94:204–207.
16. Kim MC, Kim HH, Jung GJ: Surgical outcome of laparoscopy-assisted gastrectomy with extraperigastric lymph node dissection for gastric cancer. Euro J Surg Oncol 2005;31:401–415. 17. Kitano S, Shiraishi N, Kakisako K, et al.: Laparoscopy-assisted
Billroth-I gastrectomy (LADG) for Cancer: Our 10 years’ experience. Surg Laparosc Endosc Percutan Tech 2002;12:204– 207.
18. Kim MC, Jung GJ, Kim HH: Morbidity and mortality of laparoscopy-assisted gastrectomy with extraperigastric lymph node dissection for gastric cancer. Dig Dis Sci 2007;52:543– 548.
19. Fujiwara M, Kodera Y, Kasai Y, et al.: Laparoscopy-assisted distal gastrectomy with systemic lymph node dissection for early gastric
carcinoma: A review of 43 cases. J Am Coll Surg 2003;196:75– 81.
20. Kim MC, Kim W, Kim HH, et al.: Risk factors associated with complication following laparoscopy-assisted gastrectomy for gastric cancer: A large-scale Korean multicenter study. Ann Surg Oncol 2008;15:2692–2700.
21. Huscher CG, Mingoli A, Sgarzini G, et al.: Videolaparoscopic total and subtotal gastrectomy with extended lymph node dissection for gastric cancer. Am J Surg 2004;188:728–735. 22. Mochiki E, Kamiyama Y, Aihara R, et al.: Laparoscopic assisted
distal gastrectomy for early gastric cancer: Five years’ experience. Surgery 2005;137:317–322.
23. Huscher CG, Mingoli A, Sgarzini G, et al.: Totally laparoscopic total and subtotal gastrectomy with extended lymph node dissection for early and advanced gastric cancer: Early and long-term result of a 100-patient series. Am J Surg 2007;194: 839–844.
24. Maruyama K, Kaminish M, Hayashi K, et al.: Gastric cancer treated in 1991 in Japan: Data analysis of nationwide registry. Gastric cancer 2006;9:51–66.
25. Hur H, Jeon HM, Kim W: Laparoscopy-assisted distal gastrec-tomy with D2 lymphadenecgastrec-tomy for T2b advanced gastric cancers: Three years’ experience. J Surg Oncol 2008;98:515– 519.
26. Lee YJ, Ha WS, Park ST, et al.: Port-site recurrence after laparoscopy-assisted gastrectomy: Report of the first case. J Laparoendosc Adv Surg Tech A 2007;17:455–457.
27. Kitano S, Shiraishi N, Uyama I, et al.: A multicenter study on oncologic outcome of laparoscopic gastrectomy for early cancer in Japan. Ann Surg 2007;245:68–72.
28. Koga S, Takebayashi M, Kaibara N, et al.: Pathological characteristics of gastric cancer that develop hematogenous recurrence, with special reference to the site of recurrence. J Surg Oncol 1987;36:239–242.
29. Song KY, Park SM, Kim SN, et al.: The role of surgery in the treatment of recurrent gastric cancer. Am J Surg 2008;196:19– 22.
30. Shchepotin I, Evans SR, Shabahang M, et al.: Radical treatment of locally recurrent gastric cancer. Am Surg 1995;6:371–376. 31. Sasako M, Maruyama K, Kinoshita T, et al.: Surgical treatment
of carcinoma of the gastric stump. Br J Surg 1991;78:822– 824.
32. Newman E, Brennan MF, Hochwald SN, et al.: Gastric remnant carcinoma: Just another proximal gastric cancer or a unique entity? Am J Surg 1997;173:292–297.
33. Isozaki H, Tanaka N, Fujii K, et al.: Surgical treatment for advanced carcinoma of the gastric remnant. Hepato-Gastro-enterology 1998;45:1896–1900.
34. Gutt CN, Riemer V, Kim ZG, et al.: Impact of laparoscopic surgery on experimental hepatic metastases. Br J Surg 2001;88: 371–375.
35. Kim ZG, Mehl C, Lorenz M, et al.: Impact of laparoscopic CO2-insufflation on tumor-associated molecules in cultured colorectal cancer cells. Surg Endosc 2002;16:1182–1186.