Direct Detection and Identification of
Bacterial Pathogens from Urine with
Optimized Specimen Processing and
Enhanced Testing Algorithm
Bin Huang,a,bLei Zhang,dWeizheng Zhang,e,fKang Liao,aShihong Zhang,a Zhiquan Zhang,gXingyan Ma,aJialong Chen,hXiuhong Zhang,iPinghua Qu,e,f Shangwei Wu,dCha Chen,e,f Yi-Wei Tangb,c
Department of Laboratory Medicine, First Affiliated Hospital of Sun Yat-sen University, Guangzhou, Chinaa; Department of Laboratory Medicine, Memorial Sloan Kettering Cancer Center, New York, New York, USAb; Department of Pathology and Laboratory Medicine, Weill Medical College of Cornell University, New York, New York, USAc; KingMed Diagnostics, Guangzhou, Chinad; Department of Laboratory Medicine, Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Chinae; Department of Laboratory Medicine, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, Chinaf; Department of Laboratory Medicine, Second Affiliated Hospital of Guangzhou Medical University, Guangzhou, Chinag; Department of Laboratory Medicine, People's Hospital of Huangpu, Zhongshan, Chinah; Department of Laboratory Medicine, People's Hospital of Huidong, Huizhou, Chinai
ABSTRACT Rapid and accurate detection and identification of microbial pathogens causing urinary tract infections allow prompt and specific treatment. We optimized specimen processing to maximize the limit of detection (LOD) by matrix-assisted la-ser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS) and evaluated the capacity of combination of MALDI-TOF MS and urine analysis (UA) for direct detection and identification of bacterial pathogens from urine samples. The optimal volumes of processed urine, formic acid/acetonitrile, and supernatant spot-ted onto the target plate were 15 ml, 3l, and 3l, respectively, yielding a LOD of 1.0⫻105CFU/ml. Among a total of 1,167 urine specimens collected from three
hos-pital centers, 612 (52.4%) and 351 (30.1%) were, respectively, positive by UA and urine culture. Compared with a reference method comprised of urine culture and 16S rRNA gene sequencing, the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of MALDI-TOF MS alone and MALDI-TOF MS coupled with UA were 86.6% versus 93.4% (2 ⫽ 8.93; P ⬍ 0.01), 91.5% versus
96.3% (2⫽ 7.06;P⬍ 0.01), 81.5% versus 96.4% (2 ⫽37.32;P⬍ 0.01), and 94.1%
versus 93.1% (2 ⫽ 0.40; P⬎ 0.05), respectively. No significant performance
differ-ences were revealed among the three sites, while specificity and NPV of MALDI-TOF MS for males were significantly higher than those for females (specificity, 94.3% versus 77.3%,2⫽44.90,P⬍0.01; NPV, 95.5% versus 86.1%,2⫽18.85,P⬍0.01).
Our results indicated that the optimization of specimen processing significantly en-hanced analytical sensitivity and that the combination of UA and MALDI-TOF MS provided an accurate and rapid detection and identification of bacterial pathogens directly from urine.
KEYWORDS identification, urine, pathogen, MALDI-TOF MS, urine analysis
U
rinary tract infections (UTIs) are among the most common bacterial infections seen in women. The initial treatment of UTI is mostly empirical, and immediately initiating therapy avoids serious complications and shortens the time of patient dis-comfort (1, 2). Diagnosis of UTI is currently based on the following three criteria: (i) clinical symptoms, (ii) detection of signs of infection in the urine, and (iii) detection andReceived28 December 2016Returned for modification24 January 2017 Accepted17 February 2017
Accepted manuscript posted online1 March 2017
CitationHuang B, Zhang L, Zhang W, Liao K, Zhang S, Zhang Z, Ma X, Chen J, Zhang X, Qu P, Wu S, Chen C, Tang Y-W. 2017. Direct detection and identification of bacterial pathogens from urine with optimized specimen processing and enhanced testing algorithm. J Clin Microbiol
55:1488 –1495.https://doi.org/10.1128/
JCM.02549-16.
EditorRobin Patel, Mayo Clinic
Copyright© 2017 American Society for
Microbiology.All Rights Reserved.
Address correspondence to Cha Chen, [email protected], or Yi-Wei Tang, [email protected].
B.H. and L.Z. contributed equally to this article.
crossm
on May 16, 2020 by guest
http://jcm.asm.org/
identification of bacteria in the urine. The gold standard for the diagnosis of UTIs, conventional urine culture and identification, usually takes 2 to 5 days, which delays evidence-based treatment (1, 3). Rapid detection and identification of urinary patho-gens without providing antimicrobial susceptibility testing may provide useful infor-mation for patients when promptly treated empirically with a single agent selected from a relatively small and select group of antimicrobial agents (sulfamethoxazole-trimethoprim, nitrofurantoin, or ciprofloxacin) (2). Rapid identification would reveal any unexpected pathogen for which susceptibility testing for additional agents would become important (2).
Urine analysis (UA), including urine dry chemistry and urinary sediment micros-copy, has been widely used as a preliminary screening urine test (4). Patients with UTIs usually present with positive leukocyte esterase and nitrate reduction as well as bacteria in urine. Nitrite and leukocyte esterase in urine were reported to independently predict UTIs caused by Enterobacteriaceae with a sensitivity and specificity of 77% and 79%, respectively (5). Nitrite lacks adequate sensitivity for the detection of non-Enterobacteriaceaeinfections, so negative results should be inter-preted with caution (6). The determination of bacteriuria by direct microscopy was reported to be reliable when the levels of bacteriuria were over 105CFU/ml (7).
Matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS) has emerged as a convenient, fast, and accurate method for bacterial and yeast identification on purified isolates (3, 8, 9). Direct analysis of clinical samples further increased the usefulness of this method by eliminating the time required for microor-ganism growth and isolation. Several studies have applied the technique to detect and identify microbial pathogens directly from urine (10–13) and have revealed that clini-cians would receive therapeutically helpful information for 96.1% of samples in less than 1 h (10, 14).
Much effort has been spent to improve urine processing and to enhance the identification capability of MALDI-TOF MS by coupling it with rapid urine analysis (4, 10, 12, 14–16). This study aimed to establish and optimize a urine processing method to improve the analytical sensitivity and specificity of MALDI-TOF MS. In addition, we explored the performance of the combination of MALDI-TOF MS and UA for detection and identification of bacterial pathogens directly from urine samples.
RESULTS
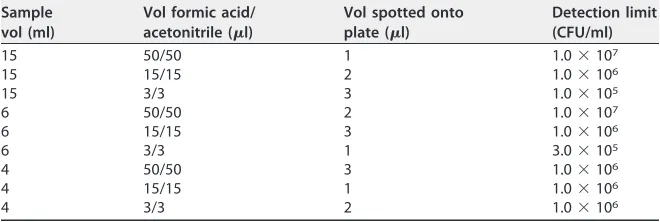
We first optimized the volumes of urine, formic acid, and acetonitrile and that of the supernatant spotted onto the target plate and determined the limit of detection (LOD) of Escherichia coli, Klebsiella pneumoniae, and Enterococcus faecalis (Table 1). The optimal LOD (1.0⫻105CFU/ml) was achieved by using 15 ml of urine, 3l of formic
acid, and 3l of acetonitrile in the sample preprocessing step and spotting 3l of supernatant onto the target plate as shown in Table 1. Using this optimized combina-tion, the LOD values of the MALDI-TOF MS were 1.0⫻105, 4.0⫻105, and 1.5⫻105
CFU/ml forE. coli,K. pneumoniae, andE. faecalis, respectively.
[image:2.585.41.371.84.195.2]During the study period, a total of 1,167 urine specimens with sufficient residual volumes from the three sites were collected. Among them, 532 (45.6%), 367 (31.4%), TABLE 1Optimization of sample preprocess for MALDI-TOF MS
Sample vol (ml)
Vol formic acid/ acetonitrile (l)
Vol spotted onto plate (l)
Detection limit (CFU/ml)
15 50/50 1 1.0⫻107
15 15/15 2 1.0⫻106
15 3/3 3 1.0⫻105
6 50/50 2 1.0⫻107
6 15/15 3 1.0⫻106
6 3/3 1 3.0⫻105
4 50/50 3 1.0⫻106
4 15/15 1 1.0⫻106
4 3/3 2 1.0⫻106
on May 16, 2020 by guest
http://jcm.asm.org/
and 268 (23.0%) were from the First Affiliated Hospital of Sun Yat-sen University (FAH), the Second Affiliated Hospital of Guangzhou University of Chinese Medicine (SAH), and KingMed Diagnostics (KMD), respectively. Of the patients tested, 525 (45.0%) were male and 642 (55.0%) were female (Table 2).
For the urine cultures, 351 (30.1%) out of 1,167 urine samples were positive. Among the 351 positive specimens, there were 342 with one colony morphology and 298 with colony counts that were greater than 1.0 ⫻105 CFU/ml and 44 with colony counts
between 1.0⫻104CFU/ml and 1.0⫻105CFU/ml. In addition, nine specimens showed
two colony morphologies with colony counts that were greater than 1.0⫻105CFU/ml.
The identification results showed that 263 (73.1%) specimens contained Gram-negative bacilli and 97 (26.9%) contained Gram-positive cocci. The most commonly isolated microorganisms wereE. coli(157, 43.6%), followed byK. pneumoniae(31, 8.6%) andP. aeruginosa(21, 5.8%).
For the urine analysis, 612 (52.4%) out of 1,167 samples were positive. Among them, 317 were positive by culture, 214 of them with colony counts that were greater than 1.0⫻105CFU/ml and 34 of them with colony counts between 1.0⫻104and 1.0⫻105
CFU/ml. Among the 555 urine samples with negative urine analysis results, 34 were positive by culture, and the omission ratio was 2.9% (34/1,167) (Table 3).
For the MS analysis, 373 (32.0%) out of 1,167 samples were identified successfully by Vitek MS. Forty-seven positive samples that were detected by urine culture were unidentified by MALDI-TOF MS (Table 3). Among them, 44 samples were positive by culture with colony counts between 1.0⫻104and 1.0⫻105CFU/ml and 3 samples
were positive by culture with colony counts of 1.0 ⫻ 105 CFU/ml (identified as K.
[image:3.585.38.552.84.162.2]pneumoniae [n ⫽ 2] and E. faecalis [n ⫽ 1], respectively). The nine samples with discrepant results between MALDI-TOF MS and culture identification were analyzed by 16S rRNA gene amplification and sequencing (Table 4). In addition, nine sample
TABLE 2Comparison of the results stratified by gender of MALDI-TOF MS between males and females
Test
Group or statistical value
No. of patients
No. of specimens with indicated resulta
Sensitivity (%) Specificity (%) PPV (%) NPV (%) SⴙTⴙ SⴙTⴚ SⴚTⴙ SⴚTⴚ
MALDI-TOF MS Male 525 105 18 23 379 85.4 94.3 82.0 95.5
Female 642 281 40 73 248 87.5 77.3 79.4 86.1
2value 0.37 44.90 0.42 18.85
Pvalue ⬎0.05 ⬍0.01 ⬎0.05 ⬍0.01
aUC, urine culture; S, standard (urine culture plus 16S rRNA sequencing); T, test.
TABLE 3Performance of urine analysis, MALDI-TOF MS, and MALDI-TOF MS coupled with urine analysisa
Test(s)
Institute or statistical value
No. of specimens with indicated result
Sensitivity (%) Specificity (%) PPV (%) NPV (%) SⴙTⴙ SⴙTⴚ SⴚTⴙ SⴚTⴚ
UA only Total 317 34 295 521 90.3 63.8 51.8 93.9
FAH 138 18 116 260 88.5 69.1 54.3 93.5
SAH 103 10 98 156 91.2 61.4 51.2 93.9
KMD 76 6 81 105 92.7 56.5 48.4 94.6
MALDI-TOF MS only Total 304 47 69 747 86.6 91.5 81.5 94.1
FAH 122 17 24 369 87.8 93.9 83.6 95.6
SAH 111 15 27 214 88.1 88.8 80.4 93.4
KMD 71 15 18 164 82.6 90.1 79.8 91.6
UA⫹MALDI-TOF MS Total 296 21 11 284 93.4b 96.3b 96.4b 93.1
2value 8.93 7.06 37.32 0.40
FAH 119 9 5 133 93.0 96.4 96.0 93.7
SAH 105 7 5 108 93.8 95.6 95.5 93.9
KMD 72 4 2 43 94.7 95.6 97.3 91.5
aUC, urine culture; UA, urine analysis; FAH, First Affiliated Hospital of Sun Yat-sen University; SAH, Second Affiliated Hospital of Guangzhou University of Chinese
Medicine; KMD, KingMed Diagnostics; S, standard (urine culture plus 16S rRNA sequencing); T, test.
bCompared with MALDI-TOF MS only (P⬍0.01).
on May 16, 2020 by guest
http://jcm.asm.org/
[image:3.585.43.543.539.712.2]cultures resulted in two colony morphologies with colony counts that were greater than 1.0⫻105CFU/ml. However, just one type of bacterium was correctly identified by
MALDI-TOF MS among them (Table 5).
Compared with the reference standard comprised of urine culture and 16S rRNA gene sequencing, the sensitivity, specificity, positive predictive value (PPV), and nega-tive predicnega-tive value (NPV) of MALDI-TOF MS alone were 86.6%, 91.5%, 81.5%, and 94.1%, respectively. When coupling MALDI-TOF MS with UA, the sensitivity, specificity, PPV, and NPV were 93.4%, 96.3%, 96.4%, and 93.1%, respectively. Significant improve-ments in sensitivity (2⫽8.93;P⬍0.01), specificity (2⫽7.06;P⬍0.01), and PPV (2⫽
37.32;P⬍0.01) were revealed (Table 3). No significant performance differences were revealed among the three sites (Table 3) while the specificity and NPV of MALDI-TOF MS for males were significantly higher than those for females (specificity, 94.3% versus 77.3%,2⫽44.90,P⬍0.01; NPV, 95.5% versus 86.1%,2⫽18.85,P⬍0.01) (Table 2).
DISCUSSION
MALDI-TOF MS has emerged and shown high stability, accuracy, and rapidity in identification of pathogens directly from clinical samples. This allows clinically helpful results to be reported minutes after sample reception (8, 9). The Vitek MS identification system consists of a MALDI-TOF mass spectrometer (Shimadzu, Japan) and anin vitro diagnostic (IVD) database (bioMérieux), which has been cleared under regulatory guidelines for the identification of bacterial and yeast organisms from purified colonies. In our study, we optimized specimen processing to maximize LOD by Vitek MS and evaluated the capacity of the combination of Vitek MS and UA for detection and identification of bacterial pathogens directly from urine samples.
Initially, according to the method of Ferreira et al. (11), theE. colidetection limit of Vitek MS was demonstrated to be 1.5⫻106CFU/ml, which does not meet the clinical
[image:4.585.42.372.93.215.2]requirement, and showed a significant difference compared with the detection limits reported (11) using Autoflex III MALDI-TOF MS (Bruker Daltonics, Leipzig, Germany). Considering the differences between equipment and databases, orthogonal experi-mental design L9(34) was used to determine the most appropriate mixture of sample,
TABLE 416S rRNA sequencing of nine discrepant results between urine culture and MALDI-TOF MS
Urine culture identification
MALDI-TOF MS identification
16S rRNA sequencing identification
Escherichia coli Klebsiella pneumoniae Escherichia fergusonii
Escherichia coli Klebsiella pneumoniae Klebsiella pneumoniae
Escherichia coli Klebsiella pneumoniae Escherichia coli
Escherichia coli Citrobacter koseri Escherichia coli
Escherichia coli Klebsiella pneumoniae Klebsiella pneumoniae
Morganella morganii Citrobacter freundii Morganella morganii
Proteus mirabilis Enterobacter cloacae Enterobacter cloacae
Proteus mirabilis Klebsiella pneumoniae Klebsiella pneumoniae
Klebsiella pneumoniae subsp.pneumoniae
Enterobacter aerogenes Enterobacter aerogenes
TABLE 5The identification results of MALDI-TOF MS on samples with two species identified by urine culture
Conventional identification MALDI-TOF MS
Escherichia coli,Klebsiella pneumoniae Klebsiella pneumoniae
Escherichia coli,Enterococcus faecalis Escherichia coli
Escherichia coli,Pseudomonas aeruginosa Escherichia coli
Escherichia coli,Klebsiella pneumoniae Escherichia coli
Klebsiella pneumoniae,Morganella morganii Klebsiella pneumoniae Klebsiella pneumoniae,Enterococcus faecalis Klebsiella pneumoniae Enterococcus faecalis,Pseudomonas aeruginosa Enterococcus faecalis Enterococcus faecalis,Burkholderia cepacia Enterococcus faecalis
Enterococcus faecalis,Escherichia coli Enterococcus faecalis
on May 16, 2020 by guest
http://jcm.asm.org/
[image:4.585.42.371.637.739.2]formic acid, and acetonitrile and the optimal volume of supernatant spotted onto the target plate. The most appropriate volumes of the urine sample, formic acid, acetoni-trile (15 ml, 3l, and 3l, respectively) and 3l of supernatant spotted onto the target plate showed LODs of 1.0 ⫻ 105, 4.0 ⫻ 105, and 1.52 ⫻ 105 CFU/ml forE. coli, K.
pneumoniae, andE. faecalis, respectively, which were equivalent to those previously reported on the Bruker Biotyper system (17). Inigo et al. established 2 ml as the optimum volume, as it was easily manipulated in Eppendorf tubes and centrifuges (15). Zboromyrska et al. used 10 ml of urine for MALDI-TOF MS and obtained higher score values of direct identification (16). In order to improve the LOD, Sánchez-Juanes et al. added a pretreatment with SDS to enhance cell lysis and the release of microorganisms, and Veron et al. compared different methods, concluding that previous short-culture and dual-filtration methods provided the best results (18, 19). We suggest a starting volume of 15 ml, as conical tubes and centrifuges of this size are routinely available in clinical bacteriology laboratories.
In this study, MALDI-TOF MS missed 47 positive samples detected by urine culture. Among these, the colony count of 44 samples was below the LOD of MALDI-TOF MS. However, three samples with colony counts of 1.0⫻105CFU/ml were identified asK.
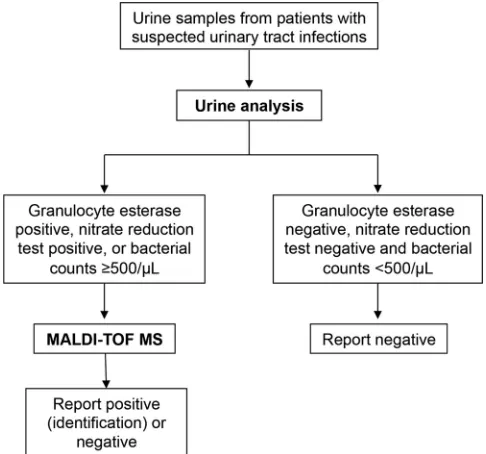
pneumoniaeandE. faecalis, which is regarded to be below the LOD of MALDI-TOF MS. Three studies have been reported to combine MALDI-TOF MS with rapid UA (4, 15, 16). In order to evaluate the performance of the combination of UA and MALDI-TOF MS, only samples that were granulocyte esterase positive or nitrate reduction test positive or had bacterial counts that were greater than 500/l were combined with MALDI-TOF MS. The improved sensitivity (93.4%), specificity (96.3%), and PPV (96.4%) (P⬍ 0.01) indicated that combining UA with MALDI-TOF MS can provide better results and rapid identification of microorganisms from urine samples directly. Among the 555 samples that were negative by urine analysis, 34 samples were positive by culture. The omission ratio was 2.9% (34/1,167). All false-negative samples were collected from middle-aged and elderly patients, which were mostly elderly females. Low immunity among these patients may lead to a low granulocyte esterase, which may result in the false-negative UA result. There were 11 false-positive samples with negative culture results. Most of these patients (9/11) suffered from kidney diseases. We speculated that there may be plenty of protein in these urine samples, especially from nephritis patients, which will influence the extraction of protein, possibly interfere with the detection of MALDI-TOF MS, and may result in misidentified results. Additional processing (e.g., additional centrifugal filters) for diafiltration may help reduce the unnecessary protein in these urine samples. Therefore, we suggest that an enhanced test algorithm as shown in Fig. 1 be used in clinical laboratories to detect and identify bacterial pathogens from urine samples rapidly and directly.
As reported previously by others, the analysis of polymicrobial cultures did not provide reliable results (15, 20). In our study, nine polymicrobial urine samples provided the correct identification of one microorganism, which is similar to Inigo et al. who showed that 75% of the polymicrobial urine samples provided invalid results (15). Wang et al. detected urine specimens containing two microorganisms in different ratios and demonstrated that only the dominant bacteria were detected in a mixture at a ratio of 1:9 (20). Identification of polymicrobial urine samples remains a challenge for rapid diagnosis using MALDI-TOF MS directly from urine samples.
Comparing the results of MALDI-TOF MS from different hospitals, there was no statistical difference in sensitivity, specificity, PPV, and NPV, which suggests that the source of the specimen has no influence on detection by MALDI-TOF MS. We noticed that transport times of urine specimens from KMD were 12 to 24 h longer than those of the two clinical laboratories within the hospital (FAH and SAH). Nevertheless, the results stratified by gender showed no statistical difference in sensitivity and PPV of MALDI-TOF MS. However, there were statistical differences in specificity (94.3% versus 77.3%,P⬍0.01) and NPV (95.5% versus 86.1%,P⬍0.01) between samples from males and females. This finding suggests the presence of additional interference factors, such
on May 16, 2020 by guest
http://jcm.asm.org/
as human proteins in the urine samples of females that may affect MALDI-TOF MS analysis.
In conclusion, the combination of UA and MALDI-TOF MS can provide preliminary and reliable identification from urine samples in 1 h, which allows timely and targeted treatment for patients. In accordance with other references, urine samples with a low bacterial count (less than 1.0⫻105CFU/ml) can currently not be reliably identified by
MALDI-TOF MS, which suggests that identifications will be obtained only when the colony counts are at least 1.0⫻105CFU/ml.
MATERIALS AND METHODS
Standard strains and urine samples.Escherichia coliATCC 25922 andPseudomonas aeruginosa
ATCC 27853 (American Type Culture Collection, Manassas, VA, USA) were used as controls for urine culture and identification. All ATCC strains were obtained from the National Center for Clinical Laboratory of China and maintained as described previously (3). Three clinical laboratories in the Guangzhou area participated in the study, including the First Affiliated Hospital of Sun Yat-sen University (FAH), the Second Affiliated Hospital of Guangzhou University of Chinese Medicine (SAH), and KingMed Diagnostics (KMD). Consecutive urine specimens with sufficient residual volume after urine culture were included in the study. Fresh urine specimens were tested immediately at FAH and SAH. The transport times of urine specimens sent to KMD were 12 to 24 h longer than those of urine specimens sent to the two hospital clinical laboratories (FAH and SAH). Urine specimens from KMD were stored at 4°C before testing during transportation. Each urine sample was divided into two aliquots, one for UA (including urine dry chemistry and urinary sediment microscopy) and the other for MALDI-TOF MS. Strains isolated from urine samples were stored at⫺80°C and used for 16S rRNA gene sequencing if discrepant results were revealed between MALDI-TOF MS and conventional culture and identification.
Sample preprocess optimization.A 0.5 McFarland standard suspension (approximately 1.5⫻108 CFU/ml) ofE. coliATCC 8739 was used to make six 10-fold serial dilutions ranging from 1.5⫻103to 1.5⫻ 108CFU/ml. Orthogonal experimental design L
9(34) was used to establish and optimize the appropriate volumes of urine samples, formic acid/acetonitrile, and mixture spotted onto the target plate. Each variable was set at three levels as shown in Table 1. Similarly, six 10-fold serial dilutions ofE. coliATCC 25922,K. pneumoniaeATCC 700603, andE. faecalisATCC 29212 were prepared to determine limit of detection (LOD).
Urine processing and extraction.Urine protein extraction for MS was performed as previously published with brief modifications (3). Strain suspensions and crude urine specimens were centrifuged at 2,000⫻gfor 30 s to remove leukocytes. Supernatants were centrifuged at 15,500⫻gfor 5 min, resuspended with 1 ml sterile water, and centrifuged at 15,500⫻gfor 2 min followed by two washes with sterile water. Supernatants were discarded, and pellets were air dried at room temperature. Seventy percent formic acid and 100% acetonitrile were added to resuspend pellets and centrifuged at 15,500⫻
g for 2 min. Finally, supernatants were spotted onto a target plate, and 1 l of matrix solution (2,5-dihydroxybenzoic acid [DHB]) was added and air dried at room temperature.
FIG 1Flowchart and test algorithm of rapid detection and identification of bacterial pathogens from urine samples.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:6.585.84.327.72.299.2]MALDI-TOF MS analysis.All standard strains and urine extracts were identified by the Vitek MS MALDI-TOF system (bioMérieux Inc., Durham, NC). Target plates were calibrated and quality controlled usingE. coliATCC 8739. Instrument calibration was performed using a TOF mix (bioMérieux). Following sample processing, specimens were analyzed with the Vitek MS at a laser frequency of 200 Hz, across the mass range of 2,000 to 20,000 Da. The resulting mass spectra were displayed as a graph of the ion intensities versus mass-to-charge (m/z) values. The spectra obtained were analyzed using the Vitek MS v2.0 database, and identification results were displayed by using Myla v3.2 middleware. A confidence value ofⱖ60% with the unique spectrum of a single organism indicated good species-level identification (8).
Urine culture and identification.A 10-l portion of urine was inoculated on a sheep blood agar plate and incubated aerobically only for 18 to 48 h at 37°C. Single colonies were counted to calculate the bacterial concentration of a urine sample, and identification was performed using GN or GP cards on the Vitek 2 system (bioMérieux, Marcy l’Etoile, France). If two types of colonies were present with counts of⬎1⫻104CFU/ml, both were identified and reported. Total colony counts of⬍1⫻104CFU/ml orⱖ3 colony types were considered negative or contaminated, respectively (3). Samples with counts ofⱖ3 colony types were excluded from analysis. If an anaerobe was identified, the result was considered invalid and excluded from analysis. For LOD determination, 100l of the lowest three 10-fold diluted suspen-sions was inoculated on blood agar plates in sextuplicate and incubated for 18 to 24 h at 37°C. The bacterial CFU per milliliter of specimens were calculated as follows: colonies per plate⫻10⫻dilution factor. The mean of six aliquots of each dilution was considered to be the final count for that aliquot.
Urine dry chemistry and urinary sediment microscopy.Urine specimens were analyzed using a urine dry chemistry analyzer (Aution Max AX-4280 urine analyzer; Arkray Inc., Kyoto, Japan) and a urine visible component analyzer (UF-1000i; Sysmex, Japan). Samples with positive leukocyte esterase and nitrate reduction tests as well as bacterial counts of⬎500/l were considered bacteriuria positive (4).
16S rRNA gene amplification and sequencing.Bacterial genomic DNA was extracted by a genomic DNA purification kit (TaKaRa, Dalian, China) according to manufacturer recommendations. Bacterial 16S rRNA genes were amplified using the universal primers 27f (5=-AGA GTT TGA TCC TGG CTC AG-3=) and 1492r (5=-GGT TAC CTT GTT ACG ACT T-3=). PCR was performed under the following conditions: 94°C for 5 min, 35 cycles of 94°C for 1 min, 55°C for 1 min, 72°C for 1 min, and a final annealing at 72°C for 7 min. Deionized water andE. coliATCC 25922 were used as negative and positive controls, respectively. The PCR products were sequenced by the Beijing Genomics Institute. All sequencing data analysis was carried out with the network service of the National Center for Biotechnology Information (http://www.ncbi .nlm.nih.gov) using BLAST homology analysis to confirm the bacterial genus. The 16S rRNA gene sequence of that bacterial genus was confirmed with the List of Prokaryotic Names with Standing in Nomenclature (LPSN) (http://www.bacterio.cict.fr/). To further confirm the bacterial species, we per-formed multiple sequence analysis with the BLAST algorithm. The results were interpreted according to Clinical and Laboratory Standards Institute (CLSI) document MM18-A (21).
Statistical analysis.Concordant results between MALDI-TOF MS and culture were accepted. Strains isolated from clinical specimens with discrepant results between MALDI-TOF MS and culture were tested by 16S rRNA gene sequencing. The concordant and resolved results were used as the reference standard. The minimal bacterial concentration allowing reliable MALDI-TOF MS identification was regarded as the LOD of MALDI-TOF MS. The mean of six aliquots of each standard strain dilution was considered to be the final count for that aliquot. Data analysis was carried out using SPSS v13.0 software. Attest was performed if the variances were equal. A chi-square test was used to compare the performance of UA, MALDI-TOF MS, and MALDI-TOF MS coupled with UA, including sensitivity, specificity, PPV, and NPV. Chi-square values were calculated, andPvalues ofⱕ0.05 were considered statistically significant.
ACKNOWLEDGMENTS
We thank David Pincus, Marc van Nuenen, Jonathan Jamison, and the clinical microbiology staff at the three sites for specimen collection and/or technical assistance. The study was supported in part by a research contract between the Memorial Sloan Kettering Cancer Center and bioMérieux, Inc. (SK2012-0595), an NIH/NCI Cancer Center support grant P30 (CA008748), the National Natural Science Foundation of China (81572058), the Guangdong Natural Science Foundation (2014A030313143), and the State Education Ministry Scientific Research Foundation for the Returned Overseas Chinese Scholars.
REFERENCES
1. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. 2015. Urinary tract infections: epidemiology, mechanisms of infection and treat-ment options. Nat Rev Microbiol 13:269 –284. https://doi.org/10 .1038/nrmicro3432.
2. Gupta K, Hooton TM, Naber KG, Wullt B, Colgan R, Miller LG, Moran GJ, Nicolle LE, Raz R, Schaeffer AJ, Soper DE. 2011. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and
Infectious Diseases. Clin Infect Dis 52:e103– e120. https://doi.org/10 .1093/cid/ciq257.
3. Yan Y, Meng S, Bian D, Quinn C, Li H, Stratton CW, Tang YW. 2011. Comparative evaluation of Bruker Biotyper and BD Phoenix systems for identification of bacterial pathogens associated with urinary tract infections. J Clin Microbiol 49:3936 –3939.https://doi.org/10.1128/JCM.05363-11. 4. Wang A, Nizran P, Malone MA, Riley T. 2013. Urinary tract infections. Prim
Care 40:687–706.https://doi.org/10.1016/j.pop.2013.06.005.
5. Little P, Turner S, Rumsby K, Warner G, Moore M, Lowes JA, Smith H,
on May 16, 2020 by guest
http://jcm.asm.org/
Hawke C, Mullee M. 2006. Developing clinical rules to predict urinary tract infection in primary care settings: sensitivity and specificity of near patient tests (dipsticks) and clinical scores. Br J Gen Pract 56:606 – 612. 6. Wilson ML, Gaido L. 2004. Laboratory diagnosis of urinary tract infections in adult patients. Clin Infect Dis 38:1150 –1158.https://doi.org/10.1086/ 383029.
7. Pappas PG. 1991. Laboratory in the diagnosis and management of urinary tract infections. Med Clin North Am 75:313–325.https://doi.org/ 10.1016/S0025-7125(16)30456-4.
8. Dubois D, Grare M, Prere MF, Segonds C, Marty N, Oswald E. 2012. Performances of the Vitek MS matrix-assisted laser desorption ionization-time of flight mass spectrometry system for rapid identifica-tion of bacteria in routine clinical microbiology. J Clin Microbiol 50: 2568 –2576.https://doi.org/10.1128/JCM.00343-12.
9. Seng P, Drancourt M, Gouriet F, La Scola B, Fournier PE, Rolain JM, Raoult D. 2009. Ongoing revolution in bacteriology: routine identification of bacteria by matrix-assisted laser desorption ionization time-of-flight mass spectrometry. Clin Infect Dis 49:543–551.https://doi.org/10.1086/ 600885.
10. Burillo A, Sanchez B, Ramiro A, Cercenado E, Rodriguez-Creixems M, Bouza E. 2014. Gram-stain plus MALDI-TOF MS (matrix-assisted laser desorption ionization-time of flight mass spectrometry) for a rapid diagnosis of urinary tract infection. PLoS One 9:e86915.https:// doi.org/10.1371/journal.pone.0086915.
11. Ferreira L, Sanchez-Juanes F, Gonzalez-Avila M, Cembrero-Fucinos D, Herrero-Hernandez A, Gonzalez-Buitrago JM, Munoz-Bellido JL. 2010. Direct identification of urinary tract pathogens from urine samples by matrix-assisted laser desorption ionization-time of flight mass spec-trometry. J Clin Microbiol 48:2110 –2115.https://doi.org/10.1128/JCM .02215-09.
12. Haiko J, Savolainen LE, Hilla R, Patari-Sampo A. 2016. Identification of urinary tract pathogens after 3-hours urine culture by MALDI-TOF mass spectrometry. J Microbiol Methods 129:81– 84.https://doi.org/10.1016/ j.mimet.2016.08.006.
13. Kim Y, Park KG, Lee K, Park YJ. 2015. Direct identification of urinary tract pathogens from urine samples using the Vitek MS system based on matrix-assisted laser desorption ionization-time of flight mass spectrom-etry. Ann Lab Med 35:416 – 422.https://doi.org/10.3343/alm.2015.35.4 .416.
14. Demarco ML, Burnham CA. 2014. Diafiltration MALDI-TOF mass spec-trometry method for culture-independent detection and identification of pathogens directly from urine specimens. Am J Clin Pathol 141: 204 –212.https://doi.org/10.1309/AJCPQYW3B6JLKILC.
15. Inigo M, Coello A, Fernandez-Rivas G, Rivaya B, Hidalgo J, Quesada MD, Ausina V. 2016. Direct identification of urinary tract pathogens from urine samples, combining urine screening methods and matrix-assisted laser desorption ionization-time of flight mass spectrometry. J Clin Microbiol 54:988 –993.https://doi.org/10.1128/JCM.02832-15.
16. Zboromyrska Y, Rubio E, Alejo I, Vergara A, Mons A, Campo I, Bosch J, Marco F, Vila J. 2016. Development of a new protocol for rapid bacterial identification and susceptibility testing directly from urine samples. Clin Microbiol Infect 22:561.e1–561.e6.https://doi.org/10.1016/j.cmi.2016.01 .025.
17. Cherkaoui A, Emonet S, Fernandez J, Schorderet D, Schrenzel J. 2011. Evaluation of matrix-assisted laser desorption ionization-time of flight mass spectrometry for rapid identification of beta-hemolytic streptococci. J Clin Microbiol 49:3004 –3005.https://doi.org/10.1128/ JCM.00240-11.
18. Sánchez-Juanes F, Siller Ruiz M, Moreno Obregon F, Criado Gonzalez M, Hernandez Egido S, de Frutos Serna M, Gonzalez-Buitrago JM, Munoz-Bellido JL. 2014. Pretreatment of urine samples with SDS improves direct identification of urinary tract pathogens with matrix-assisted laser de-sorption ionization-time of flight mass spectrometry. J Clin Microbiol 52:335–338.https://doi.org/10.1128/JCM.01881-13.
19. Veron L, Mailler S, Girard V, Muller BH, L’Hostis G, Ducruix C, Lesenne A, Richez A, Rostaing H, Lanet V, Ghirardi S, van Belkum A, Mallard F. 2015. Rapid urine preparation prior to identification of uropathogens by MALDI-TOF MS. Eur J Clin Microbiol Infect Dis 34:1787–1795.https://doi .org/10.1007/s10096-015-2413-y.
20. Wang XH, Zhang G, Fan YY, Yang X, Sui WJ, Lu XX. 2013. Direct identification of bacteria causing urinary tract infections by combining matrix-assisted laser desorption ionization-time of flight mass spectrometry with UF-1000i urine flow cytometry. J Microbiol Methods 92:231–235.https://doi.org/10 .1016/j.mimet.2012.12.016.
21. Clinical and Laboratory Standards Institute. 2008. Interpretive criteria for identification of bacteria and fungi by DNA target sequencing; approved guideline MM18-A. Clinical and Laboratory Standards In-stitute, Wayne, PA.