Haşim Boyacı
1, A, Kübra Gacar
2, B, C, Serap Argun Barış
1, D,
Ilknur Başyiğit
1, E, Füsun Yıldız
1, FPositive Airway Pressure Device Compliance
of the Patients with Obstructive Sleep Apnea Syndrome
Wspomaganie oddechu stałym dodatnim ciśnieniem
u chorych na obturacyjny bezdech senny
1 Department of Pulmonary Disease, Kocaeli University, Medical Faculty, Turkey 2 Department of Pulmonary Disease, Sakarya Yenikent Government Hospital, Turkey
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Objectives. The aim of this study was to evaluate factors affecting the usage of continuous positive airway pressure (CPAP) device in patients with obstructive sleep apnea syndrome (OSAS).
Material and Methods. This study included 47 patients with OSAS who were suggested to use CPAP device at home and expected to use the device for at least 6 months. The compliance of CPAP device was determined by 2 different methods. In subjective evaluation, total time for usage of the device was recorded according to patients’ declaration. In objective evaluation, total time of usage was recorded from the counter on device and it was divided into the number of days passed from the beginning of the treatment and at least 4 h of usage in a day was accepted as an effective usage. Data of compliant and non-compliant patients were compared in order to determine the fac-tors affecting CPAP treatment.
Results. Ten patients were female, 37 of them were male and mean age was 52.98 ± 20.4 years. Mean Apnea Hypopnea Index (AHI) was 54.4 ± 20, mean oxygen saturation (SO2) was 87.3 ± 4.6 and mean CPAP pressure was 7.4 ± 1.9 in the whole study population. The compliance of CPAP treatment was found to be 48.9% according to objective evaluation whereas it was 80.9% according to subjective evaluation. Five of 8 patients (62.5%) who did not use the device stated the problems about the device mentioning the mask as a reason for their non-compliance. Treatment compliance was better in the patients with high Epworth sleepiness scale (16.5 ± 5.5 vs. 11.8 ± 4.1, p < 0.05). Epworth sleepiness scale of the patients who were compliant to the treatment was significantly decreased after the treat-ment both in subjective and objective evaluation. Treattreat-ment compliance wasn’t different between male and female patients, however it was significantly lower in active smokers compared to non-smokers and ex-smokers.
Conclusions. It was concluded that the most important factor associated with compliance to CPAP treatment in the patients with OSAS was Epworth sleepiness scale while mask related side effects might be a reason of treatment withdrawal and all these issues should be addressed carefully in order to increase compliance (Adv Clin Exp Med 2013, 22, 6, 809–815).
Key words: OSAS, CPAP treatment, compliance.
Adv Clin Exp Med 2013, 22, 6, 809–815 ISSN 1899–5276
ORIGINAL PAPERS
© Copyright by Wroclaw Medical University
Obstructive sleep apnea syndrome (OSAS) is a syndrome with repeated apneic events and oxy-gen desaturation episodes which affects multiple systems [1, 2]. Continuous positive airway pres-sure (CPAP) ventilation is the standard first-line therapy for the most of the patients with
moder-ate to severe OSAS [3]. When used properly and
limited by variable adherence to prescribed thera-py [6–13]. Many patients refuse the offer of CPAP therapy, do not tolerate it, or fail to use the porta-ble machine properly [14]. These patients remain essentially untreated and receive little or no bene-fit from the device. In addition, patients common-ly fail to fulcommon-ly compcommon-ly with CPAP use, either us-ing the device for only part of the night or only on some nights. There are many reasons why patients do not comply with CPAP therapy including, dis-comfort with the mask or tubing; nasal congestion; poor mask fit with either leakage of air, skin irri-tation, or claustrophobia; the complexity of ma-chines, their noise, and the general inconvenience of their use [15, 16].
The aim of this study was to evaluate the fac-tors affecting the usage of CPAP device in patients with obstructive sleep apnea syndrome (OSAS).
Material and Methods
Study Population
The study included 47 patients who agreed to take part in the study out of 114 patients who were diagnosed with obstructive sleep apnea syndrome and were advised to use a CPAP therapy at least 6 months. OSAS was diagnosed with whole night polisomnography (PSG) at the Sleep Laboratory of Kocaeli University, Faculty of Medicine. The se-verity of OSAS was classified based on AHI values as mild (AHI 5–15), moderate (AHI 15–30) and severe (AHI > 30). The CPAP was prescribed to patients with moderate to severe OSAS. The ade-quate CPAP pressure was determined after 2nd night of PSG recording, CPAP titration was made manually and the pressure was increased until ob-structive respiratory events such as apneas, hypop-neas, arousals and snoring eliminated or the
rec-ommended maximum CPAP (20 cm H2O) was
reached. All patients were advised to use nasal CPAP treatment without humidification.
Study Plan
The patients were reached by phone to provide them with information about the study and were asked if they would take part in the study. The pre-treatment body mass index (BMI), Epworth Sleepi-ness Scale (ESS) and apnea hypopnea index (AHI) values of the patients who agreed to take part in the study were recorded from their files and they were invited to the sleep laboratory together with their CPAP devices. A short questionnaire was adminis-tered to the patients. In the questionnaire, besides their demographic characteristics the patients were
asked about their smoking habits, education sta-tuses, whether they used their CPAP devices, if yes, how many hours a day they used it on the average, if no, what was the reason, and whether they had any problems with the device and the mask. As in pre-treatment, all the patients’ post-treatment ESS was calculated.
Definition of the CPAP
Device Compliance
Patient compliance with CPAP treatment was evaluated through 2 different methods. In the 1st method, the average number of hours they used the device at night was recorded based on their own statements and device usage at least 4 h every night was accepted as effective usage. This method was called subjective evaluation. In the 2nd method, usage time was recorded from the meter on the device and this length of time was divided by the number of days elapsed from the baseline until that day; 4 h/day and values above this were ac-cepted as effective usage. This method was called objective evaluation.
In order to identify the factors that affect-ed compliance with the positive airway pressure treatment, the data of compliant and non-compli-ant patients were compared.
Statistical Analysis
Data analysis was performed in SPSS (Statis-tical Package for Social Sciences) for Windows, version 13.0. Numeric variables were expressed as
means ± standard deviation. The X2 test was used
for percentage values and qualitative variables. P < 0.05 was accepted as significant. Calculations for significant differences between different pa-tient groups were carried out using Student’s t test. Pearson’s correlation coefficient r was computed for comparing continuous variables.
Results
mean saturation was 87.3 ± 4.6 and mean CPAP pressure was 7.4 ± 1.9 in the whole study popula-tion. Based on severity classification according to AHI, 7 of the patients were defined as moderate (15%) and 40 of them were defined as severe (85%) OSAS. The demographic characteristics of the pa-tients are shown in Table 1.
Patient compliance with CPAP treatment was 48.9% according to objective evaluation and 80.9% according to subjective evaluation (Table 2). While 8 of the 9 patients who were found non-compliant in subjective evaluation stated that they never used the device, 1 reported that he used it for 3 h a night. It was observed that 11 of the 24 patients who were found non-compliant in objective evaluation either never used the device or used it less than 1 h/day on
the average, whereas device usage time ranged be-tween 1.75 h/day and 3.58 h/day in the remaining 13 patients, the average duration being 2.79 hours. The device usage times of the patients in objective evaluation are shown in Fig. 1. 5 of the 8 patients who said they never used the CPAP device report-ed that they did not use it because of the problems with the device (poor mask fit, skin irritation and nasal congestion) and the other 3 because they did not believe in its usefulness.
When the relationship of AHI, ESS, BMI and age with CPAP compliance was explored, patients with high ESS were found to have better treatment compliance (Table 3). Moreover, a significant de-crease was found in the ESS of compliant patients after the treatment. The ESS of the group assessed
Table 1. Demographic characteristics of the cases
Age (years) 52.98 ± 20.4
Gender Female
Male 1037
BMI (kg/m²) 31.038 ± 3.87
AHI 54.351 ± 20.4
Disease severity
(n) ModerateSevere 740
ESS 14 ± 5
Smoking status
n (%) Current smoker Former smoker Nonsmoker
13 (27.7) 16 (34.0) 18 (38.3) Education level
n (%) LiteratePrimary S. Secondary S. High-School University Total
2 (4.3) 18 (38.3) 5 (10.6) 8 (17.0) 14 (29.8) 47 (100)
Table 2. Treatment compliance according to objective and subjective evaluation
Compliant
n (%) Non- -compliant n (%)
Total time of usage (hours/night) Subjective 38 (80.9) 9 (19.1) 5.0 ± 2.7 Objective 23 (48.9) 24 (51.1) 3.5 ± 2.3
Fig. 1. Usage of CPAP device of the patients according to objective evaluation (hours/day)
0.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00 8.00
patients
hours/day
Table 3. The relationship between objective compliance to CPAP device and different variables
as non-compliant showed a statistically insignifi-cant decrease after the treatment (Table 4). There was no difference on mean prescribed CPAP pres-sure between the compliant and non-compli-ant group (7.58 ± 1.6 in non-complinon-compli-ant group vs. 7.26 ± 1.5 in compliant group).
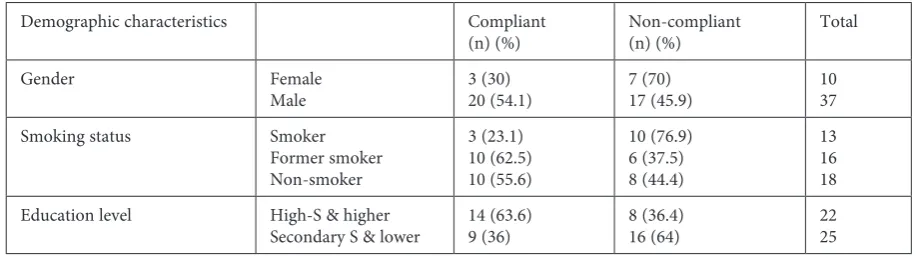
When the relationship between smoking ha-bit and compliance with treatment was explored, smokers’ compliance was observed to be signifi-cantly lower than that of both former smokers and non-smokers. When investigating the relationship between the patients’ education level and their compliance with CPAP, the patients were classi-fied as those who had education at high-school le-vel and higher and the others. Given this, although compliant patients seemed to have higher edu-cation level, this was not statistically significant. When the relationship between gender and CPAP compliance was explored, 30% of the female pa-tients and 54.1% of the male papa-tients were found compliant, but this difference was not statistically significant (Table 5).
Discussion
We found that the compliance of CPAP treat-ment was 48.9% according to objective evalua-tion whereas it was 80.9% according to subjective evaluation. ESS of the patients who were compli-ant to the treatment significcompli-antly decreased af-ter the treatment both in subjective and objective evaluation.
Objective data can be obtained from patients’ device information when evaluating patient com-pliance with positive airway pressure treatment by using the meter systems on the devices, smart cards, modems and a number of software. In the study made by Hui and associates with 112 pa-tients who were suggested to have CPAP therapy, outputs of usage times were obtained from the pa-tients’ devices and these objective data were
com-pared to the usage times subjectively reported by the patients. While the subjective usage time was found to be 6.5 ± 1.5 h/night in the 1st month, they were observed objectively to use the device 5.4 ± 1.6 h/night and it was demonstrated that there was a significant difference between the sub-jective and obsub-jective data. When the same evalu-ation was made for the 3rd month, the subjective time was similarly one hour longer than the objec-tive time [10]. Other similar studies also revealed that patients did not give correct information to the doctor about their device usage and they gen-erally used the device for a shorter time than what they reported [17–20]. The subjective usage time was also found longer than the objective usage time in our study. The patients’ objective usage time was calculated in our study by dividing the total usage time by the number of days that elapsed from the day they 1st started using the device un-til the day of checking. Since the days when the pa-tients did not use the device at all due to various reasons (traveling, upper respiratory tract infec-tion etc.) were also included in this total number of days, subjective usage naturally turned out to be shorter than objective usage. This result could al-so have been affected by the possibility that the pa-tients did not give correct information to the doc-tor about their device usage.
It is known that various risk factors increase vulnerability to OSAS. It was reported that OSAS was seen in the 40–65 age group most frequent-ly and its prevalence decreased after 65 years of age [21]. The mean age of the cases in our study
Table 4. The relationship between compliance and Epworth sleepiness scale before and after treatment
ESS Before treat-ment
ESS After treat-ment
p
Compliant 16.5 ± 5.5 2.9 ± 3.3 p < 0.05 Non-
-compliant 11.8 ± 4.1 6.6 ± 5.8 p > 0.05
Table 5. Relationship between CPAP compliance and demographic characteristics
Demographic characteristics Compliant
(n) (%) Non-compliant(n) (%) Total
Gender Female
Male 3 (30)20 (54.1) 7 (70)17 (45.9) 1037
Smoking status Smoker
Former smoker Non-smoker
3 (23.1) 10 (62.5) 10 (55.6)
10 (76.9) 6 (37.5) 8 (44.4)
13 16 18 Education level High-S & higher
was also found to be 52.98 ± 20.4, which was con-sidered consistent with the literature. Male gender is also an important risk factor for OSAS. Accu-mulation of fat especially in the neck region due to androgenic fat distribution in men increases the risk of OSAS. In a screening study conducted by Nieto and associates on 6132 people, it was report-ed that 63% of the cases who were diagnosreport-ed with OSAS were men [22]. In our study, 94 (82.5%) of the 114 cases who were advised to have CPAP due to their diagnosis of OSAS and 37 (78.7%) of the cases who took part in the study were men. When the role of gender in compliance with CPAP treat-ment was investigated, some studies reported that women used their CPAP devices more efficient-ly than men [12, 17], while Mc Ardle and asso-ciates reported that the percentage of women ac-cepting a CPAP treatment was lower [23]. Weaver and associates, on the other hand, reported that there was not any relationship between treatment compliance and gender [6]. Although effective us-age was found in our study in 3 of the female cas-es (30%) and 20 of the male cascas-es (54.1%) in ob-jective terms, no statistically significant difference was observed. The number of female cases being limited in our study could have prevented obtain-ing a statistically significant difference.
It is known that smoking is another risk fac-tor in developing OSAS [24]. Not very much da-ta could be found about the relationship between smoking and CPAP compliance. Lin and associates reported in their study including 131 OSAS patients that there was not any relationship between smok-ing and CPAP compliance [25]. In our study, only 3 (23.1%) of the 13 active smokers and 58.8% of the non-smokers and former smokers were compliant with the treatment. The fact that those who con-tinue to smoke although the harm of smoking on health is very well known have very low treatment compliance shows that the extent of compliance people exercise for their treatment is proportional to the importance they attribute to their health.
In our study, 9 (36%) of the 25 cases whose ed-ucation was at secondary school level or lower and 14 (63.6%) of the 22 cases whose education was at high-school level or higher were found to be com-pliant with the treatment. Although this result sug-gests that treatment compliance increases with the level of education, it was not found statistically sig-nificant. However, a more correct evaluation can be made if the number of cases is increased. It was also demonstrated in a similar way in the study made by Uyar and associates that compliance with device usage was not associated with the level of education [26].
One of the most important symptoms that adversely affect the social lives of the patients
diagnosed with obstructive sleep apnea syndrome is excessive sleepiness in daytime. It was evidenced that alleviating daytime sleepiness through CPAP treatment increased compliance with the treat-ment. It was also reported that those OSAS patients who had no daytime sleepiness according to ESS had poor compliance with their CPAP treatment and did not use their devices in an efficient way, which showed that there was a positive correlation between treatment compliance and ESS [27, 28]. It was observed in our study that the pre-treatment mean ESS was 16.5 ± 5.5 in compliant patients and 11.8 ± 4.1 in non-compliant patients. These results were also found consistent with the literature.
The criterion that is used for both the diag-nosis and severity of OSAS is AHI that is found as a result of a polysomnographic study. It was observed in a study made with 71 patients diag-nosed with obstructive sleep apnea syndrome that the cases with high AHIs had higher CPAP compliance [28]. The study of Galetke and asso-ciates demonstrated that usage of a CPAP device was correlated with the AHI value at baseline [29]. Although there are studies showing in a similar way that AHI is correlated with CPAP compli-ance [9, 10, 23], there are also studies showing that there is no significant relationship between AHI and CPAP compliance [18, 30–32]. The mean AHI of the cases included in our study was 54.4 ± 20.4 and no significant relationship was found between AHI and CPAP compliance, but the fact that the majority of the cases in our study (82.9%) had se-vere OSAS might have prevented us from revealing such a relationship.
Despite the technological improvements in the devices used in positive airway pressure treat-ment, treatment-related side effects can be seen in many patients. It was reported that the side effects associated with the mask in particular could affect patients’ compliance with the treatment negative-ly [33]. For this reason, all patients should be called to regular checks for side effects and practical ap-proaches should be offered to eliminate these. Al-though mask-related side effects were seen in more than half of the patients in the study of Gülcü and associates, no significant relationship was found between the side effects and efficient use of the CPAP device [34]. In our study, 5 (62.5%) of the 8 cases, who stated that they did not use the device, mentioned about problems related to the device and the mask as their reason and this showed that the problems associated with the device was one of the important factors affecting CPAP usage.
found that patients without co-existing disease as well as patients with more than 2 comorbid con-dition tended to withdraw CPAP treatment more frequently [29]. However, there were no doctor di-agnosed comorbidities in our study population, so it was not possible to determine the impact of co-morbidities on treatment compliance.
The most important problem in CPAP treat-ment, which is the most effective treatment meth-od in treating OSAS tmeth-oday, is patient compliance. Although it was suggested that a wide range of fac-tors affected this compliance, it was concluded in
this study that the most important factor that in-creased compliance was the extent of excessive day-time sleepiness in patients and a high ESS result as the indicator of this. Despite the technological im-provements in the devices used, it was observed that device-related side effects affected compliance negatively. Therefore, all patients should be given adequate training on their disease and the device, they should regularly be called to checks for side effects and practical approaches should be offered to eliminate these and in this way efforts should be continued to increase compliance.
References
[1] Olson EJ, Park JG, Morgenthaler TI: Obstructive sleep apnea hypopnea syndrome. Prim Care 2005, 32, 329–359.
[2] Park JG, Ramar K, Olson EJ: Updates on definition, consequences, and management of obstructive sleep apnea: Mayo Clin Proc 2011, 86, 549–554.
[3] Loube DI, Gay PC, Strohl KP, Pack Al, White DP, Collop NA: Indications for positive airway pressure treatment of adult obstructive sleep apnea patients: a consensus statement. Chest 1999, 115, 863–866.
[4] Vitulano N, Di Marco Berardino A, Re A, Riccioni G, Perna F, Mormile F, Valente S, Belocci F: Obstructive sleep apnea and heart disease: the biomarkers point of view. Front Biosci (Schol Ed) 2013, 1, 588–599.
[5] Doherty LS, Kiely JL, Swan V, Mc Nicholas WT: Long-term effects of nasal continuous positive airway pressure therapy on cardiovascular outcomes in sleep apnea syndrome. Chest 2005, 127, 2076–2084.
[6] Weaver TE, Grunstein RR: Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc 2008, 5, 173–178.
[7] Gay P, Weaver T, Loube D, Iber C: Evaluation of positive airway pressure treatment for sleep related breathing disorders in adults. Sleep 2006, 29, 381–401.
[8] Rauscher H, Formanek D, Popp W, Zwick H: Self-reported vs. measured compliance with nasal CPAP for obstructive sleep apnea. Chest 1993, 103, 1675–1680.
[9] Meurice JC, Dore P, Paquereau J, Neau JP, Ingrand P, Chavagnat JJ, Patte F: Predictive factors of long-term compliance with nasal continuous positive airway pressure treatment in sleep apnea syndrome. Chest 1994, 105, 429–433.
[10] Hui DS, Choy DK, Li TS, Ko FW, Wong KK, Chan JK, Lai CK: Determinants of continuous positive airway pres-sure compliance in a group of Chinese patients with obstructive sleep apnea. Chest 2001, 120, 170–176.
[11] Russo-Magno P, O’Brien A, Panciera T, Rounds S: Compliance with CPAP therapy in older men with obstruc-tive sleep apnea. J Am Geriatr Soc 2001, 49, 1205–1211.
[12] Sin DD, Mayers I, Man GC, Pawluk L: Long-term compliance rates to continuous positive airway pressure in obstructive sleep apnea: a population-based study. Chest 2002, 121, 430–435.
[13] Lindberg E, Berne C, Elmasry A, Hedner J, Janson C: CPAP treatment of a population-based sample: what are the benefits and the treatment compliance? Sleep Med 2006, 7, 553–560.
[14] Veasey SC, Guilleminault C, Strohl KP, Sanders MH, Ballard RD, Magalang UJ: Medical therapy for obstructive sleep apnea: a review by the Medical Therapy for Obstructive Sleep Apnea Task Force of the Standards of Practice Committee of the American Academy of Sleep Medicine. Sleep 2006, 29, 1036–1044.
[15] Parthasarathy S, Haynes PL, Budhiraja R, Habib MP, Quan SF: A national survey of the effect of sleep medicine specialists and American Academy of Sleep Medicine Accreditation on management of obstructive sleep apnea. J Clin Sleep Med 2006, 2, 133–142.
[16] Chasens ER, Pack AI, Maislin G, Dinges DF, Weaver TE: Claustrophobia and adherence to CPAP treatment. West J Nurs Res 2005, 27, 307–321.
[17] Amfilochiou A, Tsara V, Kolilekas L, Gizopoulou E, Maniou C, Bouros D, Polychronopoulos V: Determinants of continuous positive airway pressure compliance in a group of Greek patients with obstructive sleep apnea. Eur J Intern Med 2009, 20, 645–650.
[18] Reeves-Hoche MK, Meck R, Zwillich CW: Nasal CPAP: an objective evaluation of patient compliance. Am J Respir Crit Care Med 1994, 149, 149–154.
[19] Engleman H, Asgari-Jirhandeh N, Mc Leod AL, Ramsay CF, Deary IJ, Douglas NJ: Self reported use of CPAP and benefits of CPAP therapy. Chest 1996, 109, 1470–1476.
[20] Rauscher H, Formanek D, Popp W, Zwick H: Self-reported vs measured compliance with nasal CPAP for obstruc-tive sleep apnea. Chest 1993, 103, 1675–1680.
[21] WHO, prevention and management of global epidemic obesity. Report of WHO consultation on obesity 1997, Genova.
[23] McArdle N, Devereux G, Heidarnejad H, Engleman HM, Mackay TW, Douglas NJ: Long-term use of PAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med 1999, 159, 1108–1114.
[24] Young T, Finn L, Austin D, Peterson A: Menopausal status and sleep-disordered breathing in the Wisconsin Sleep Cohort Study. Am J Respir Crit Care Med 2003, 167, 1181–1185.
[25] Lin HS, Prasad AS, Pan CJ, Rowley JA: Factors associated with noncompliance to treatment with positive airway pressure. Arch Otolaryngol Head Neck Surg 2007, 133, 69–72.
[26] Uyar M, Elbek O, Mete A, Bayram N, Çiftçi N, Gündoğdu N, Dikensoy Ö: Factors influencing compliance with continuous positive airway pressure ventilation in obstructive sleep apnea syndrome. Tub Toraks 2012, 60, 47–51.
[27] Barbe F, Mayoralas LR, Duran J, Masa JF, Maimo A, Montserrat JM, Monasterio C, Bosch M, Ladaria A, Rubio M, Rubio R, Medinas M, Hernandez L, Vidal S, Douglas NJ, Agusti AG: Treatment with continuous positive airway pressure is not effective in patients with sleep apnea but no daytime sleepiness: a randomized, controlled trial. Ann Intern Med 2001, 134, 1015–1023.
[28] Yetkin O, Kunter E, Gunen H: PAP compliance in patients with obstructive sleep apnea syndrome. Sleep Breath 2008, 12, 365–367.
[29] Galetke W, Puzzo L, Priegnitz C, Anduleit N, Randerath WJ: Long-term therapy with continuous positive air-way pressure in obstructive sleep apnea: Adherence, side effects and predictors of withdrawal – a real life study. Respiration 2011, 82, 155–161.
[30] Sullivan CE, İssa FG, Berthon-Jones M, Eves L: Reversal of obstructive sleep apnea by continuous positive airway pressure applied through the nares. Lancet 1981, 1, 862–865.
[31] Sopkova Z, Dorkova Z, Tkacova R: Predictors of compliance with continuous positive airway pressure treatment in patients with obstructive sleep apnea and metabolic syndrome. Wien Klin Wochenschr 2009, 121, 398–404.
[32] Waldhorn RE, Herrick TW, Nguyen MC, O’Donnell AE, Sodero J, Potolicchio SJ: Long-term compliance with nasal continuous positive airway pressure therapy of obstructive sleep apnea. Chest 1990, 97, 33–38.
[33] Weaver TE: Adherence to positive airway pressure therapy. Curr Opin Pulm Med 2006, 12, 409–413.
[34] Gülcü A, İtil O, Öztura I,Sener G, Sahbaz S, Sevinç C, Kılınç O, İkiz AÖ, Çımrın AH, Uçan ES, Akkoçlu A:
Compliance, side effects and results of PAP therapy in cases with obstructive sleep apnea syndrome. Turkish Resp J 2005, 3, 135–138.
Address for correspondence:
Serap Argun Barış
Department of Pulmonary Disease, Kocaeli University Umuttepe, Kocaeli
Turkey
Tel.: 90 506 664 42 93
E-mail: [email protected] Conflict of interest: None declared Received: 21.12.2012