Copyrightc 2010 Wolters Kluwer Health|Lippincott Williams & Wilkins
Improving Timeliness
and Efficiency in the
Referral Process for Safety
Net Providers
Application of the Lean Six Sigma
Methodology
Gloria J. Deckard, PhD; Nancy Borkowski, DBA;
Deisell Diaz, PhD; Carlos Sanchez, MBA;
Serge A. Boisette, MHSA
Abstract:Designated primary care clinics largely serve low-income and uninsured patients who present a disproportionate number of chronic illnesses and face great difficulty in obtaining the medical care they need, particularly the access to specialty physicians. With limited capacity for providing specialty care, these primary care clinics generally refer patients to safety net hospitals’ specialty ambulatory care clinics. A large public safety net health system successfully improved the effectiveness and efficiency of the specialty clinic referral process through application of Lean Six Sigma, an advanced process-improvement methodology and set of tools driven by statistics and engineering concepts.Key words:access,ambulatory care,process improvement,Six Sigma,
specialty referral
Author Affiliations: Decision Sciences and Information Systems, College of Business Administration, Florida International University, Miami (Dr Deckard); Health Care Management Programs, College of Business Administration, Florida International University (Dr Borkowski); Six Sigma Master Black Belt, Devin Consulting Group, Miami, Florida (Dr Diaz) and Six Sigma Black Belt, Deivin Consulting Group, Miami, Florida (Mr Sanchez); and Six Sigma Green Belt, Ambulatory Managed Care & Quality, Jackson Health System, Miami,Florida (Mr Boisette).
The authors thank the members of the Six Sigma team from Jackson Health System, Miami, Florida: Dr Yolangel Hernandez-Suarez, Associate Chief Med-ical Officer; Dr Angela Burrafato, MedMed-ical Director, Ambulatory Care Center; Dr Thresia Gambon, Medical Director, Primary Care Centers; Dr Lenworth Anglin, Medical Director, Quality and Managed Care; Mary-Keen Robinson, ARNP, Quality Manager, Ambulatory Services Division; Ester Eisler, Director, Ambulatory Ser-vices; Elaine Perdue, RN, Associate Director of Patient Care Services; Kevin Lynch, Director of Applications and Information Technology; Dr Suzanne Minor, Primary Care Physician; Marta Garcia, RN, Clinical Care Coor-dinator, Referral Services; Conchita Freitag, RN, Clinical Educator; and Debbie Turbert, RN, Director of Patient Care Services, Ambulatory Care Center.
E
STIMATES SUGGEST that communityhealth centers (CHCs) and designated low income primary care clinics (PCCs) serve more than 18 million individuals annually (National Association of Community Health Centers [NACHC], 2009a). These safety net providers largely serve low-income members of racial and ethnic minorities, who are unin-sured or publicly inunin-sured; present a dispropor-tionate number of chronic illnesses (NACHC, 2009a,b; Robert Wood Johnson Foundation, 2005); and face great difficulty in obtaining the medical care they need, particularly ac-cess to specialty physicians. Although PCCs and CHCs serve as the medical home, these centers have limited capacity for providing
Corresponding Author:Gloria J. Deckard, PhD, Deci-sion Sciences and Information Systems, College of Busi-ness, Florida International University, 11200 SW 8th St, Miami, FL 33199 ([email protected]).
Improving Timeliness and Efficiency in the Referral Process for Safety Net Providers 125 specialty care and face difficulties in referrals
as fewer private physicians, academic medi-cal centers, and community hospitals are will-ing to provide specialty care to the unin-sured (Felt-Lisk et al., 2002). Safety net hospi-tals through specialty ambulatory care clinics have become the providers of last resort for specialty care services for the increasing num-ber of uninsured and other vulnerable pop-ulations. Evidence suggests ever-lengthening wait times for the uninsured, especially adults with chronic illnesses, to obtain specialty care appointments, with the first available appoint-ment being in 6 months to a year (Felt-Lisk et al., 2002). In addition, healthcare processes (eg, referral systems) created and/or changed on an ad hoc basis over time may become unnecessarily complex (Kaplan et al., 2009). Referral processes that are unstructured and complex create inefficiencies in the system and delay the provision of specialty care.
Unnecessary complexities in the referral process exacerbate delays in the receipt of ser-vices and impact patient quality of care. The Institute of Medicine (IOM, 2001) suggests that overly complex delivery processes that require numerous steps and patient “hand-offs” slow down care, decrease safety, and
waste resources.Crossing the Quality Chasm
(IOM, 2001) identified timeliness—reducing
waits and sometimes harmful delays—for both those who receive and those who give
care and efficiency—avoiding waste,
includ-ing waste of equipment, supplies, ideas, and energy—as aims or goals for improvement of the US healthcare system. Providing timely and appropriate care to the uninsured and other vulnerable populations is a national con-cern that can be addressed, at least in part, by improving the PCC/CHC to specialty referral process through performance-improvement strategies such as Lean Six Sigma.
PROCESS IMPROVEMENT BY USING LEAN SIX SIGMA
Process improvementis the act of analyzing a process (macro or micro) to determine how it can be done better and proceed to make the necessary changes to improve outcomes
(Diaz, 2008). There are 2 paths to process improvement: unstructured and structured. Unstructured process improvement does not provide an organized method and, thus, can result in ad hoc changes. Lacking a stan-dard methodology, improvement relies on in-dividual expertise rather than on measures or metrics to guide the process and set goals. Structured process improvement, on the other hand, provides a standard, organized method to guide improvements for change that is based on measures and responsibilities. Kaplan et al. (2009) note that intentionally designed (structured) process-improvement strategies are more likely to yield efficient and effective processes.
Six Sigma is a tested and commonly known structured method that utilizes comprehen-sive data-driven tools supported by statis-tical analysis to improve process perfor-mance (Diaz, 2008). The Six Sigma method includes 5 phases: define-measure-analyze-improve-control, commonly referred to as the DMAIC technique. These phases are used to improve existing processes to improve overall performance. The DMAIC methodology has a proven data drill-down capability that is based on statistical analysis. This helps achieve the goal within Six Sigma: reduce variation.
Lean provides a set of transitional tools that identify valuable and invaluable activities with events or activities (steps). The Lean analysis pinpoints specific improvements by eliminat-ing steps that incur costs but are not valu-able to the desired end result. Lean and Six Sigma combined dramatically reduce varia-tion, unpredictability, and potential negative outcomes while minimizing costs.
Six Sigma was originally developed by Motorola as a quality improvement method-ology, and its use was expanded by other companies such as General Electric and Al-lied Signal/Honeywell (Black & Revere, 2006). A review of Six Sigma applications across a variety of healthcare processes (Vest & Gamm, 2009) demonstrates the effectiveness of Six Sigma methodology for healthcare or-ganizations. The array of processes exam-ined by Vest and Gamm (2009) included surgery turnaround time, clinic appointment
access, hand hygiene, antibiotic prophylaxis in surgery, scheduling radiology procedures, and meeting Centers for Medicare and Medi-caid Services cardiac indicators. Earlier work by Gamm et al., (2007) suggested the use-fulness of Six Sigma in addressing the IOM “quality chasm.” Lean Six Sigma provides a structured, systematic approach to improving healthcare processes and meeting the chal-lenges of quality improvement.
APPLICATION OF LEAN SIX SIGMA AND DMAIC TO A SPECIALTY REFERRAL PROCESS
Recognizing the value of both Lean and Six Sigma approaches, the Jackson Health System (JHS) in Miami-Dade County, Florida, sought to improve the effectiveness and efficiency of referrals for specialty care through application of Lean Six Sigma methodology. Two specialty clinics were identified to participate in the project: (1) genitourinary (GU) and (2) gyne-cology (GYN). A multidisciplinary team was identified and, with the assistance of 2 Sigma Black Belt mentors, the project followed the DMAIC approach (Diaz, 2008):
DEFINE the project’s purpose and scope and obtain background on the current pro-cess and the customers’ perspectives;
MEASURE data that pinpoint problem loca-tion or occurrence; focus the improvement ef-fort by gathering baseline information on the current situation;
ANALYZE data to identify and confirm root causes; set goals for performance;
IMPROVE process by implementing
planned solutions; eliminate or reduce the impact of the identified root causes; and
CONTROL the gains by standardizing pro-cesses; use data to evaluate the solutions; an-ticipate next steps.
Define
Over time, the process of specialty referral from primary care physicians (PCPs) at PCCs and CHCs to the JHS ambulatory care spe-cialty clinics (ACSC) had grown cumbersome and fragmented impacting the efficiency of the process. In addition, the effectiveness of
the system varied. A Pareto chart (ie, a type of bar chart that aligns categorical data) was con-structed to graph the problems across refer-ring entities. This analysis demonstrated that PCCs’ consult requests took twice as long as other services and that PCCs were less suc-cessful at converting consult requests to spe-cialty appointments than were other services. Thus, the PCCs were identified as the focus for the initial project.
A fishbone diagram (Fig 1) was developed to obtain background and understand the current referral process for PCCs. Reviewing this diagram, the team discovered inefficien-cies and developed the following problem de-scription: “The referral process from PCP to the Patient Clinical Care Coordinator (PCCC) for review is not efficient and the time lag between Appointment Made to Day of Ap-pointment is excessive.” The objective of the project then became restructuring the sys-tem for consults to improve quality and timeli-ness of communication between primary care physicians, primary care coordinating center, and specialty physicians. Specifically, the aim for improvement was to reduce turnaround time.
The next step in the process was to dia-gram a process map detailing the steps in the process from the PCP determining the need for a referral/consultation through the con-sult process (review, approval, and service) and the returned referral/consult to the PCP. This process map followed a standard SIPOC (supplier, inputs, process, outputs, and cus-tomers) analysis and provided the tools to identify appropriate measures and steps of value/nonvalue activities.
Measures
Data were collected to pinpoint the prob-lems and focus the improvement effort. At this phase, the Critical to Quality (CTQ) was iden-tified as “turnaround time for consult” (refer-ral). CTQs are core customer-focused require-ments that provide a measure to determine whether the objectives are being met, that is, the referrals are processed and appoint-ments are made in a timely fashion. Timely fashion was then quantified; specifically, if the
Improving Timeliness and Efficiency in the Referral Process for Safety Net Providers 127
Figure 1. Fishbone diagram outlining background of specialty referral process. PCP indicates primary care physician.
process takes more than 30 days (4 weeks), it does not meet the criteria.
Analyze
The analysis phase utilized several steps to identify and confirm root causes of ineffi-ciency (ie, delays in making appointments) to address process improvement. All paper re-ferrals for GU and GYN were collected and reviewed; all approved appointments for GU and GYN were collected and reviewed; and pathways were identified and analyzed. The outcomes for all referrals (ie, incomplete, in-appropriate, approved) were documented in a database.
Drill-down analysis revealed delays in the referral process due to the following:
1. Incompleteness of referrals,
2. Inadequate staffing in making appoint-ments,
3. Lack of staff access to available specialty care appointment slots, and
4. Inadequate number of specialty care ap-pointment slots (eg, insufficient clinical capacity).
These delays resulted in extra steps in the process, which could be removed through process improvement and standardization.
Improve
To improve the specialty referral process, all PCP/PCCs referrals/consults were:
1. Sent to a central area, 2. Entered into a database, and
3. Reviewed for completeness, appropri-ateness (based on InterQual evidence-based clinical decision support criteria) and timeliness.
Referrals that were
• incomplete were logged and returned to
the originator for proper completion with needed actions noted;
• determined to possibly be
inappropri-ate were reviewed by the medical direc-tor using InterQual criteria, and who, if needed, performed a literature review for current best practices (ie, evidence-based medicine);
• determined not to be appropriate were
returned to the originator with an expla-nation of the reason for the determina-tion;
• appropriate and complete requests,
specialty appointments were generated; and
• outcomes of all referrals were entered
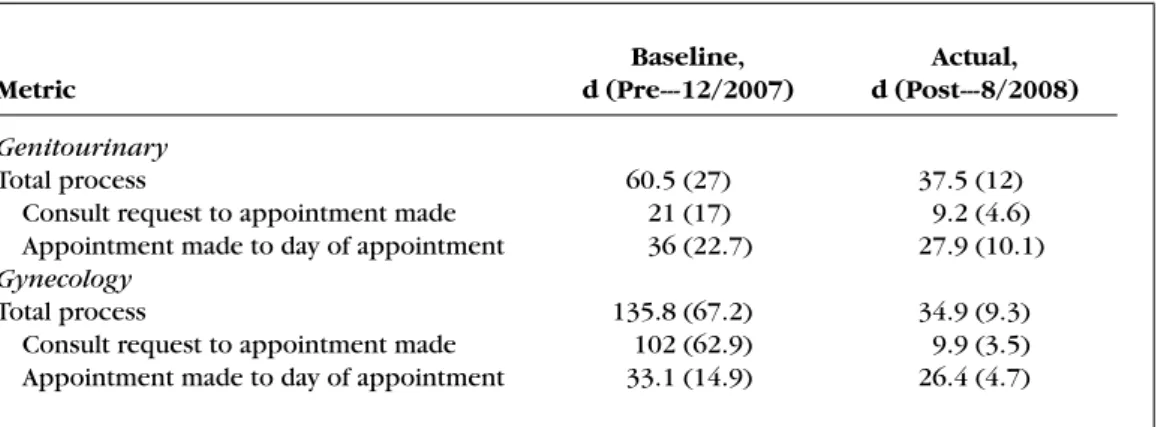
Table 1. Pre- and Postmetrics for specialty referral process measuresa
Baseline, Actual,
Metric d (Pre---12/2007) d (Post---8/2008)
Genitourinary
Total process 60.5 (27) 37.5 (12)
Consult request to appointment made 21 (17) 9.2 (4.6) Appointment made to day of appointment 36 (22.7) 27.9 (10.1)
Gynecology
Total process 135.8 (67.2) 34.9 (9.3)
Consult request to appointment made 102 (62.9) 9.9 (3.5) Appointment made to day of appointment 33.1 (14.9) 26.4 (4.7)
aValues are presented as mean (SD).
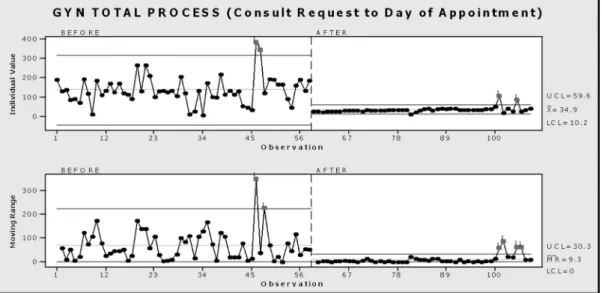
The statistical data analysis demonstrated improvements in the referral process for the 3 metrics: total process (number of days that elapsed between initiation of the referral and the date of the appointment), consult request to appointment made (number of days that elapsed between initiation of the referral and the date the appointment is made), and ap-pointment made to day of apap-pointment (num-ber of days that elapsed between the date the appointment is made and the date of the appointment). Table 1 provides the pre-and postmeasures for both GU pre-and GYN on the 3 metrics. Linear graphing of the values and ranges for the total specialty referral pro-cess before, during, and after the Six Sigma improve phase/process (implementation of change) are displayed in Figure 2 for GU and Figure 3 for GYN.
The overall process time was substantially reduced as were the intervening steps of the process. The referral process was reduced in GU from 60.5 to 37.5 days and in GYN from 135 to 34.9 days.
Control
Standardizing improved processes incorpo-rates the Deming Plan-Do-Check-Act Cycle (Deming, 2000). The monitoring, data analy-sis, and actions are performed by the ACSC administrative department. The database is updated each time there is a new referral/ consult. In the Plan-Do cycles, the follow-ing metrics are captured: appointment
re-quest date, appointment made date, and appointment day date. A report is generated from this database monthly. The Check cycle utilizes control charts from quarterly data to identify any undesirable patterns or trends. If an undesirable pattern or trend is identified, the ACSC administration does the following (Act cycle): establish data collection plan to zoom (drill down) on the problem area, im-prove breakdown in process and communica-tion, and continue monitoring to ensure sus-tainability.
CONCLUSIONS
Data reported here demonstrate the suc-cess of the Lean Six Sigma application to a spe-cialty referral process in ambulatory care. As noted earlier, the total referral process was re-duced, as well as the days elapsed, in both the components of the process—initiation of re-quest to appointment made and appointment made to day of appointment. Application of Lean Six Sigma structured methodology to the referral process improved both efficiency and timeliness, reducing the total process time by 23 days (38%) in GU and by 100 days (74%) in GYN. The aim defined by the team—to reduce the turnaround time—was met; how-ever, the quantitative measure of 30 days (4 weeks) was not met. Given the substantial re-ductions in days from pre- to post process measures, the interventions set a direction for a continuing improvement process. The re-duction in times in the total process and wait
Improving Timeliness and Efficiency in the Referral Process for Safety Net Providers 129
Figure 2. Variability and range values for GU: Before, during, and after improvement process implemen-tation. GU indicates genital urinary.
times for appointment dates improved ser-vice to the patients, PCPs, PCCs, and, poten-tially, the quality of care. Undoubtedly, Lean Six Sigma provided a successful means to ad-dress the IOM aims of efficiency and timeli-ness in this study.
Figure 3. Variability and range values for GYN: Before, during, and after improvement process implemen-tation. GYN indicates gynecology.
NEXT STEPS
Further improvements in the referral pro-cess are planned. Currently, the system con-tinues to rely on paper referrals and ap-provals. To achieve increased efficiency and
reach the 30-day target, the safety net sys-tem for Miami-Dade County is joining together to implement a Web-based referral system. Partners in this endeavor include the Miami-Dade County Health Department, the Health Council of South Florida, PCCs, CHCs, JHS, and researchers from Florida International University.
Vest and Gamm (2009) suggest the need for more stringent attention to research mea-sures as well as sustainability in documenting the effectiveness of Six Sigma. Future analy-sis will study specialty clinics referrals not in-cluded in this study, to compare changes or
improvements in the referral process without structured intervention, and will review the effectiveness of specialty consults/referrals from CHCs that were not part of this study. Both groups will provide “control” data to empirically test and eliminate alternative hy-potheses that may explain the improvement gained through Six Sigma. Although the pre-/ posttest findings of this Six Sigma applica-tion demonstrated effectiveness and provided substantial support for the expansion of this process-improvement methodology in health-care, the controlled studies will answer any questions on the limitations of this design.
REFERENCES
Black, K., & Revere, L. (2006). Six Sigma arises from the
ashes of TQM with a twist.International Journal of
Health Care Quality Assurance Incorporating Lead-ership in Health Services,19(2/3), 259–266.
Deming, W. E. (2000).Out of Crisis.Cambridge, MA: MIT
Press.
Diaz, D. M. (2008).Simple Lean Six Sigma: Global
or-ganizational Lean Six Sigma training for systematic improvement: Driving organizational excellence us-ing Lean and Six Sigma.Miami, FL: Deivin. Felt-Lisk, McHugh, M., & Howell, E. (2002). Monitoring
local safety-net providers: Do they have adequate
ca-pacity?Health Affairs,21(5), 277–283.
Gamm, L., Kash, B., & Bolin, J. (2007). Organiza-tional technologies for transforming care: Measures
and strategies for pursuit of IOM quality aims.
Jour-nal of Ambulatory Care Management, 30(4), 291– 301.
Gilmer, T., & Kronick, R. (2005). It’s the premiums, stupid: Projections of the uninsured through 2013
[Web exclusive].Health Affairs. doi: 10.1377/hlthaff.
W5.143. Retrieved July 31, 2009, from http://content. healthaffairs.org/cgi/reprint/hlthaff.w5.143v1
Institute of Medicine. (2001). Crossing the quality
chasm: A new health system for the 21st century.
Washington, DC: National Academies Press.
Kaplan, S., Bisgaard, S., Truesdell, D., & Zetterholm, S. (2009). Design for Six Sigma in healthcare: Developing
an employee influenza vaccination process.Journal of
Healthcare Quality,31(3), 36–43.
National Association of Community Health Centers.
(2009a). America’s health centers. Retrieved July
31, 2009, from http://www.nachc.com/client/
documents/America’s Health Centers updated 3.09. pdf
National Association of Community Health Centers.
(2009b). Primary care access: An essential
build-ing block of health care reform. Retrieved July
31, 2009, from http://www.nachc.com/client/
documents/pressreleases/PrimaryCareAccessRPT.pdf
Robert Wood Johnson Foundation. (2005). Uninsured
Americans with chronic health conditions: Key find-ings from the National Health Interview Survey. Re-trieved July 31, 2009, from http://www.rwjf.org/files/ research/Urban2005.pdf
Vest, J. R., & Gamm, L. D. (2009). A critical review of re-search literature on Six Sigma, Lean and StuderGroup’s Hardwiring Excellence in the United States: The need to demonstrate and communicate the
effective-ness of transformation strategies in healthcare.
Imple-mentation Science,4,35. doi:10.1186/1748-5908-4-35.