LEABHARLANN CHOLAISTE NA TRIONOIDE, BAILE ATHA CLIATH TRINITY COLLEGE LIBRARY DUBLIN
OUscoil Atha Cliath The University of Dublin
Terms and Conditions of Use of Digitised Theses from Trinity College Library Dublin Copyright statement
All material supplied by Trinity College Library is protected by copyright (under the Copyright and Related Rights Act, 2000 as amended) and other relevant Intellectual Property Rights. By accessing and using a Digitised Thesis from Trinity College Library you acknowledge that all Intellectual Property Rights in any Works supplied are the sole and exclusive property of the copyright and/or other I PR holder. Specific copyright holders may not be explicitly identified. Use of materials from other sources within a thesis should not be construed as a claim over them.
A non-exclusive, non-transferable licence is hereby granted to those using or reproducing, in whole or in part, the material for valid purposes, providing the copyright owners are acknowledged using the normal conventions. Where specific permission to use material is required, this is identified and such permission must be sought from the copyright holder or agency cited.
Liability statement
By using a Digitised Thesis, I accept that Trinity College Dublin bears no legal responsibility for the accuracy, legality or comprehensiveness of materials contained within the thesis, and that Trinity College Dublin accepts no liability for indirect, consequential, or incidental, damages or losses arising from use of the thesis for whatever reason. Information located in a thesis may be subject to specific use constraints, details of which may not be explicitly described. It is the responsibility of potential and actual users to be aware of such constraints and to abide by them. By making use of material from a digitised thesis, you accept these copyright and disclaimer provisions. Where it is brought to the attention of Trinity College Library that there may be a breach of copyright or other restraint, it is the policy to withdraw or take down access to a thesis while the issue is being resolved.
Access Agreement
By using a Digitised Thesis from Trinity College Library you are bound by the following Terms & Conditions. Please read them carefully.
Effect of Surface Contamination on
Re-osseointegration of dental implants surrounded by
circumferential bone defects
A thesis submitted in partial fulfilment of Doctorate in Dental Surgery
(D. Ch. Dent.) Periodontology
Seif Mohamed
Department of Restorative Dentistry and Periodontology
School of Dental Science
Trinity College
Dublin
DECLARATION
I declare that the present work has not been submitted as an exercise for the degree at
any university. It consists o f my work, except where reference indicates otherwise.
The library o f Trinity College Dublin may lend or copy this thesis on request.
DEDICATION
To my wife, Nuha for her patience and continuous support over the last three years.
To my children. Nasr, Nafissa and Mugtaba.
Acknowledgements
To Professor N oel C laffey, for his trust, encouragem ent, guidance and continuous
support.
To Dr. loannis Polyzois for his huge help, support and patience over the last three
years.
To Dr. Osam a O m er for his continuous support, help and guidance.
To all Libyan post-graduate students in Dublin D ental School & H ospital for their
help.
To Jan W alker for her help.
To Peter N ow lan for his help.
To peter O ’Reilly for his help.
SUMMARY
AIM OF THE STUDY:
This study was designed to evaluate the effect o f surface
contamination
on
re-osseointegration
o f dental
implants
surrounded
by
circumferential bone defect and to compare osseointegration around Osseotite
TMimplants (Biomet 31, Palm Beach Gardens, USA ) with that around Nanotite
implants ( Biomet 31, Palm Beach Gardens, USA ) in beagle dogs.
MATERIALS AND METHODS:
Four adult beagle dogs and 16 dental implants,
eight commercially pure titanium 3.25mm x 13mm Osseotite® implants ( Biomet 31,
Palm Beach Gardens, USA ) and eight commercially pure titanium 3.25 x 13mm
Nanotite™ implants ( Biomet 31. Palm Beach Gardens, USA ) were used. The lower
premolars (P I, P2. P3 and P4) were extracted. Following 3 months o f healing, bucccal
and lingual mucoperiosteal flaps were raised and 4 implants (Two Osseotite and two
Nanotite™) were partially inserted in the left side o f the mandible in each dog.
Following five weeks o f healing period, the implants were removed from the left
sides, decontaminated by tooth brush and saline and placed into freshly prepared sites
to the full implant length on the right side o f each mandible. The coronal 5 mm o f
each implant was surrounded by 1.0 mm circumferential bone defect. Following 12
weeks o f healing period, the dogs were sacrificed and the mandibles on experimental
sides were harvested.
Hard tissue ground sections were prepared o f biopsies taken at the end o f the study
and histometric measurements were obtained.
RESULTS:
The mean percentage o f bone in direct contact with the implant surface
(part 2) and the part that encased by bone (part 3) respectively. The m ean percentage
o f BIC for part 1 was significantly low er than part 2 and part 3 (p = 0.0001). The
m ean percentage o f the bone area w ithin threads for part 1, part 2 and part 3 was 55%,
80% and 79% respectively. Part 1 show ed significantly low er percentage o f bone area
w ithin threads than part 2 and part 3 (p = 0.0007). The m ean percentage o f BIC for
Osseotite® im plant (type 1) and Nanotite"^"* im plant (type 2) was 72% and 65%
respectively. The difference was not statistically significant (p = 0.23). The m ean
percentage o f bone area w ithin threads for type 1 and type 2 was 65% and 78%
respectively. The mean percentage o f bone area w ithin threads was found to be
significantly higher for type 2 im plant than type 1 im plant (p = 0.0299).
C onclusions: The result dem onstrated that osseointegration can occur to the im plants
surfaces that were previously contam inated and surrounded by bone defects.
Nanotite® im plants showed significantly greater bone area w ithin threads than
Osseotite^” implants.
CONTENTS
Declaration.
Dedication.
Acknowledgement.
Summary.
Contents.
Index of figures.
List of tables.
Introduction Chapter 1.
Literature Review Chapter 2.
2.1 O sseointegration.
2.2 Im plant surface.
2.3 The Criteria for im plant success.
2.4 Peri-im plantitis and treatm ent methods.
2.4.1 Clinical, M icrobiological and H istopathological features.
2.4.2 Treatm ent o f peri-im plantitis in humans.
2.4.3 Treatm ent o f peri-im plantitis in animal models.
M aterials and M ethods C hapter 3. 46
3.1 im plants. 47
3.2 A nim als and A naesthesia. 47
3.3 Extractions. 47
3.4 Experim ental Procedures.
47
3.4.1 Experim ental procedure 1. 47
3.4.2 Experim ental procedure 2. 48
3.5 A ntibiotic and Follow up. 50
3.6 Specim en Preparation. 50
3.7 H istological Preparation. 50
3.8 M easurem ent M ethod. 50
3.9 H istom etric Exam ination. 51
3.10 Data A nalysis. 51
Results Chapter 4. 59
4.1 A nalysis at im plant level.
M easurem ent 1. 60
M easurem ent 2. 63
4.2 A nalysis at dog level. 67
4.3 H istological observation. 70
Discussion C hapter 5. 74
References Chapter 6.
Page
53 53 54 54 55 55 56 56 57 57 58 58 61 62 62 63 6566
66
67 70 71Index of figures
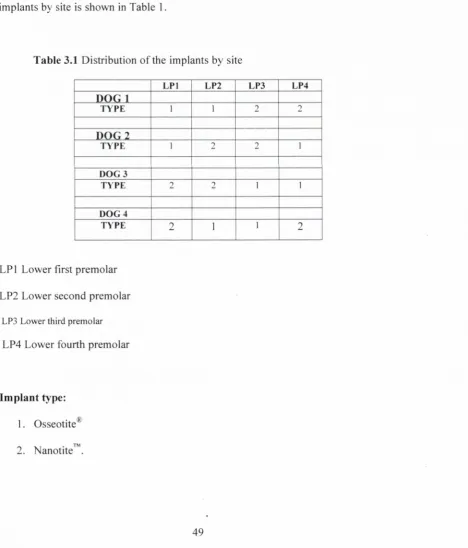
Edentulous prem olar areas prior to surgery. The ridge follow ing flap elevation.
Four implants partially inserted. Four im plants after flap sutured back.
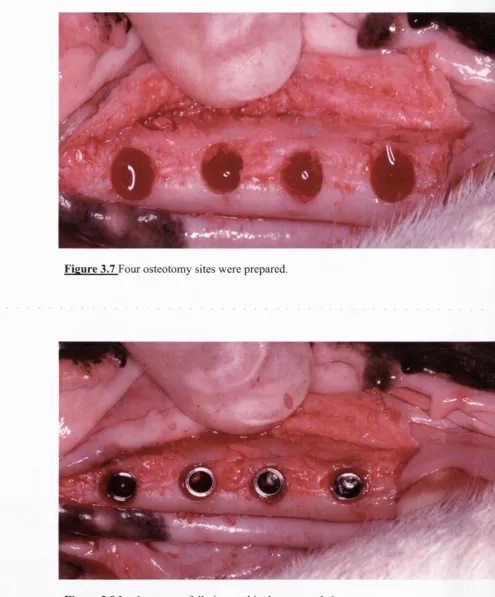
Four im plants contam inated with bacterial plaque. Im plants cleaned w ith saline and tooth brush. Four osteotom y sites w ere prepared.
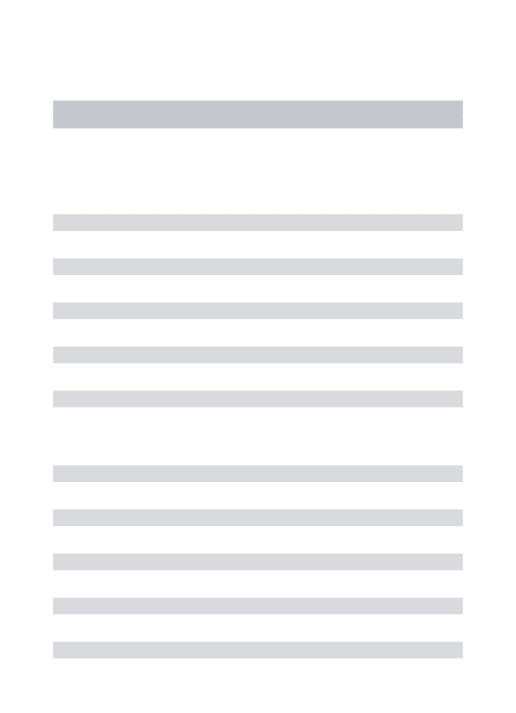
Implants were fully inserted in prepared sites. Cover screws w ere placed.
Flap sutured back.
M achined used for sectioning the implants. Sectioning o f the im plant.
M eans for percentage o f bone in direct contact with the im plant surface (BIC) by im plant site.
M eans for percentage o f bone in direct contact w ith the im plant surface (BIC) by im plant type.
M eans for percentage o f bone in direct contact with the im plant surface (BIC) by im plant part.
Least square m eans for types broken down by parts.
M eans for the percentage o f bone area w ithin threads by im plant site.
M eans for the percentage o f bone area within threads by im plant type.
M eans for percentage o f bone area w ithin threads by im plant part. Least square m eans for types broken down by parts.
M esio-distal section o f Nanotite^” im plant dog 1 x 3"^^* premolar. M esio-distal section o f N anotite’^” im plant dog 2 x second premolar.
Figure 4.3.3
H igher m agnification o f the previously contam inated part for the im plant illustrated in figure 4.3.2. [image:13.522.40.488.77.806.2]71
Figure 4.3.4
M esio-distal section o f Osseotite® im plant dog 2 x fourth prem olar. 72Figure 4.3.5
M esio-distal section o f Osseotite® im plant dog 3 third prem olar. 73Figure 4.3.6
H igher m agnification o f the previously contam inated part for the im plant illustrated in figure 4.3.5.page 39 42 49 52 60 60 61 61 64 64 64 65
68
68
69List of tables
H um an studies for treatm ent o f peri-im plantitis.
A nim al studies for treatm ent o f peri-im plantitis.
D istribution o f the implants by site.
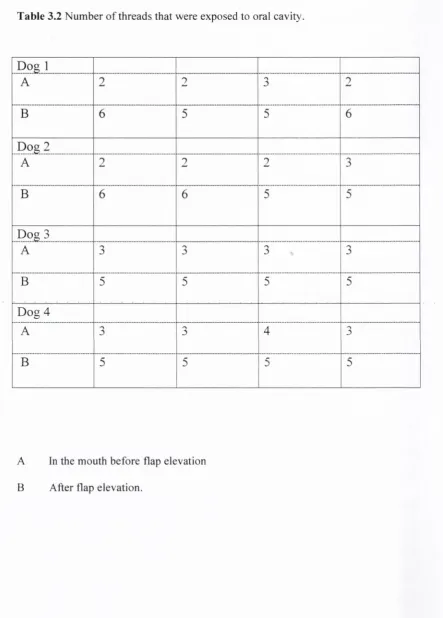
N um ber o f threads exposed to oral cavity.
Effect tests for im plant site, type and part.
M eans and standard deviations for percentage o f bone in direct contact with im plant surface by im plant site.
M eans and standard deviations for percentage o f bone in direct contact with im plant surface by im plant type.
M eans and standard deviations for percentage o f bone in direct contact with im plant surface by im plant part.
Effect tests for im plant site, type and part.
M eans and standard deviations for m easurem ent o f percentage o f bone w ithin threads by im plant site.
M eans and standard deviations for m easurem ent o f percentage o f bone w ithin threads by im plant type.
M eans and standard deviations for m easurem ent percentage o f bone w ithin threads by im plant part.
M eans and 95% confidence intervals for the tw o im plant types and for the part o f im plant that was previously contam inated and surrounded by bone defect.
M eans and 95% confidence intervals for the tw o im plant types and for the part o f im plant that was previously surrounded by soft tissues alone.
M eans and 95% confidence intervals for the tw o im plant types and for the part o f im plant that was encased by bone.
CHAPTER 1
The use o f osseointegrated im plants in the rehabilitation o f partial or complete
edentulism is becom ing a com m on treatm ent procedure. For the last 30 years,
favourable long-term results o f im plant-supported and implant-retained prostheses
have been reported in com plete and partially edentulous patients. (Adell et a/,1981, Albrektsson e? <3/. 1988).
Occasionally how ever, im plant threads becom e exposed as a result o f bacterial-
induced peri-im plant destruction. This destruction has been termed peri-im plantitis
and the objective o f therapy for this condition is to regain integration o f the implant
with bone.
Various treatm ent m odalities have been used to treat peri-im plantitis in humans and
animal m odels including debridem ent & decontam ination o f the exposed implant
surface, access flap procedures, use o f adjunctive anti-m icrobial agents and
regenerative procedures with m em branes/grafts. (Singh et al. 1993, Griinder et al. 1993, Jovanovic et al. 1993, Persson et al. 1996, W etzel et al. 1999) Although all o f these treatm ent m odalities were found to be effective in cleaning titanium surfaces
and to allow for soft tissue healing and bone re-fill in the defects, only limited re-
osseointegration occurred.
Failure o f re-osseointegration follow ing induced peri-im plantitis has been attributed to
m any factors including contam ination o f im plant surface, bony defects surrounding
the im plants and other factors such as clot adhesion/stability and cellular
m igration/differentiation.
R e-o sse o in teg ratio n to su rfaces th a t w e re plaque co n tam in ated w as co n sid ered to be
e ith e r ex tre m ely d ifficu lt or im p o ssib le to obtain. (G ru n d er et a/. 1993, E ricsson et a/. 1996, P ersson et al. 1996, 1999, 2 0 0 1 , W etzel et al. 1999).
In an ex p e rim en t in L ab rad o r dogs, p eri-im p lan titis lesions w e re treated by system ic
an tim ic ro b ial th era p y and local m e a su re s in cluding flap elev a tio n , cu rettag e and
ch e m ic al d ec o n ta m in a tio n o f the ex p o se d im plant su rface (E ricsso n et al. 1996). The ab u tm en t parts w ere rem oved, clean ed in am in o -a lc o h o l (1 % d elm o p in o l H C L ) and
au to cla v ed , w hile the fixture c o m p o n e n ts w ere clean ed th o ro u g h ly w ith the sam e
am in o -a lc o h o l. It w as observed th a t th is regim e w hen acco m p an ied by a careful
plaq u e control p rogram d uring h ealin g re su lted in th e elim in a tio n o f the in flam m ato rj'
lesions, but re-o sseo in teg ratio n failed to o c c u r to titan iu m su rfa ces p rev io u sly exposed
to plaq u e (E ricsson et al. 1996).A sim ila r result w as o b tain ed w hen the co n tam in ated ab u tm en ts w ere d iscarded, and p ristin e c o v e r screw s w e re p laced o v er the cleaned
fixtures, w hich w ere su bsequently su b m erg e d (P ersson e t al. 1996).
In an attem p t to avoid chem ical m an ip u latio n o f the fix tu re surface. P ersson et al. (1999) restricted the clean in g o f th e ex p o se d im plant to m ech a n ical m ean s using a
rotatin g brush and an abrasive (p u m ice ). T his tre a tm e n t resu lted in m arked bone
fo rm ation in the crater like defects and the e stab lish m en t o f a co n n e ctiv e tissue
capsule th at separated the new ly fo rm ed bone from m ost o f th e clean ed im plant
surface. T he auth o rs co ncluded th at n e ith e r chem ical n o r m ech a n ical tre a tm e n t o f the
co n tam in ated im plant surface estab lish ed co n d itio n s co n d u c iv e fo r re-
Persson et al. (2001a) used im plants com prised o f tw o parts, one apical and one coronal part that w ere joined w ith a connector. Such fixtures were first installed in the edentulous prem olar region o f L abrador dogs and peri-im plantitis was subsequently induced. During treatm ent o f the inflam m atory condition (system ic antibiotics and surgical granulation tissue rem oval), the upper part o f the fixture was rem oved and substituted with identical but pristine part. H ealing resulted not only in resolution o f inflamm ation but also in re-osseointegration o f the pristine fixture. The author concluded that “the quality o f the titanium surface is o f decisive im portance for both osseointegration and re-osseointegration’,'
Kolonidis et al. (2003) investigated the direct influence o f surface contam ination on re-osseointegration o f sm ooth surfaced dental im plants in Labrador dogs. Results dem onstrated that osseointegration can occur on surfaces that were plaque contam inated and cleaned by different m ethods. The findings o f K olonidis et al. (2003) were consistent with A lhag et al. (2008) who evaluated the effect o f surface contam ination on re-osseointegration o f rough surfaced dental im plants in beagle dogs.
It has also been dem onstrated in anim al m odels that osseointegration can occur when sterile implant surfaces are surrounded by bony defects. (Scipioni et a l.\9 9 1 , Paolantonio et al. 2001, Botticelli et al. 2003a, Polyzois et al. 2007, A bushahba et al. 2008).
A ccording to these results neither the implant surface contam ination nor the bony defect surrounding the im plant seem s to prevent re-osseointegration.
Titanium dental im plants have either m achined (turned) or rough (textured) surfaces. R ecently m achined surfaced im plants have been superseded by the rough surfaced im plants. M any different techniques have been used to m odify dental im plants surfaces such as titanium plasm a spray, grit-blasting, acid-etching, hydroxyapatite coating (HA) and anodization. One o f the m ost recent surface m odifications is the Discrete Crystalline Deposition (DCD) process as used in the Nanotite™ implants. This process involved deposition o f nano-stuctured calcium phosphate on the surface o f the dual acid-etched im plant resulting in discrete crystal deposits o f 20-100 nanom eters in length. The DCD process increases the m icro-surface area by 200% . There is lack o f studies regarding osseointegration o f the new ly introduced Nanotite™
(S) surface im plants in com parison to the other im plant surfaces such as Osseotite surface implants.
CHAPTER 2
2.1 Osseointegration
B ran e m a rk et al. (19 6 9 ) perfo rm ed anim al e x p e rim en ts and indicated th a t it w as p o ssib le to estab lish a d irec t bone anch o rag e to an im planted m etal d ev ice p rovided
th a t a n u m b er o f g u id elin es w ere follow ed. T his w as d o cum ented in the first clinical
re p o rt p u b lish ed som e y ea rs later (B ran em ark et al. 1977).
B ran e m a rk et al. (1977) d escrib ed this rela tio n sh ip b etw een the im plant su rface and bo n e for w hich th ey coin ed the term o sseo in teg ra tio n . T his has been d esc rib ed as “a
d irec t functional and structural connection b etw een living bone and th e su rface o f a
load carry in g im plant w ith persisten t stab ilitj' w h ere th ere is no p ro g ressiv e
m o v em en t".
In the 1970s th ere w ere no m ethods av a ila b le to section intact bone to m etal
sp ecim en s and hence the histo lo g ic evidence o f o sseo in teg ratio n re m ain ed indirect.
N e w ly d eveloped te ch n iq u e s w ere used to cut th ro u g h u ncalcified bone and im plant
w ith o u t p rev io u s separation o f an chorage and since then direct bo n e to im.plant
co n tac t w as proved beyond do u b t (S ch ro ed er et al 1981).
U n d e r light m icro sco p y o sseo in teg ratio n can be defin ed as the direct attac h m e n t o f
bo n e to an im plant surface w ith o u t an interposed soft tissu e layer (A lb rek tsso n et al.
1982 & 1983). H ow ever, at the electron m icro sco p ic level, bone has been show n to be
ap p ro x im a te ly 20 nm from the im plant surface, o r in co n tac t w ith the im p lan t surface
Zarb & A lbrektsson (1991) redefined osseointegration as “a process w here by clinically asym ptom atic rigid fixation o f alloplastic m aterials is achieved and m aintained in bone during functional loading” . This was based on stability instead o f histological criteria, as the exact degree o f bone attachm ent was difficult to identify.
A lbrektsson et al. (1981) presented a series o f factors that needed to be controlled in order for reliable osseointegration to ensue. These factors were refm ed by Adell et al (1985) and eventually sum m arized by A lbrektsson & Sennerby (1990) and they included the following:
1. B iocom patibility and inertness o f implants. 2. Im plants design,
3. Surface characteristics,
4. Host bone quality and quantity, 5. A traum atic surgical technique.
6. Loading o f im plant after sufficient healing periods.
M any factors that have been suggested to jeopardize or prevent O sseointegration include:
1. Im proper preparation o f the recipient site w hich results in undue hard tissue damage such as bone necrosis.
2. Bacterial contam ination and extensive inflam m ation o f the w ound. 3. Inadequate m echanical stability o f an im plant follow ing its insertion, 4. Prem ature loading o f im plant,
Bain and M oy (1993) review ed 2,194 Branemaric im plants over a 6 year period. They found that the percentage o f failure in sm okers w as 11.2% com pared to 4.7% for non- sm okers. A retrospective study by De Bruyn & C ollaert (1994) reported that failure before loading is 9% in sm okers com pared to 1% in non-sm okers. Recent system atic review s docum ented that sm oking interferes with the prognosis o f dental im plants and associated with com plications such as peri-im plantitis (Strietzel et al. 2007, Lindhe et al. 2008).
2.2 Implant surface
Titanium dental im plants have either m achined (turned) or rough (textured) surfaces. Smooth surfaced im plants have been used successfully for m ore than 30 years in treatm ent o f partially dentate and fully edentulous patients (Adell et al. 1981, A lbrektsson & Sennerby 1990). Recently m achined surfaced im plants have been superseded by the rough surfaced im plants. M any different techniques that have been used to m odify dental im plants surfaces such as titanium plasm a spray, grit-blasting, acid-etching, hydroxyapatite coating (HA) and anodization. Descriptive histological or histom orphom etric experim ents in hum ans & anim al m odels have shown that rough surfaced im plants have a greater bone-im plant contact area than do im plants w ith sm oother surfaces (B user et al. 1991, G odfredsen et al. 1992, Cochran et al.
1998, W ennerberg et a/. 1998, Ivanoff et al. 2001).
shown that m achined and m edium blasted im plants dem onstrated the lowest percentage o f bone-im plant contact (mean from 20-25% ). Large sandblasted
and TPS im plant surfaces had a m ean o f 30-40% bone-im plant contact area, and large sandblasted and acid-etched (SLA ) had a m ean o f 50-60% o f bone-im plant contact area. This result indicated that the extent o f bone-im plant interface was positively correlated with an increasing im plant surface roughness.
Ivanoff et al. (2001) in a study on hum an volunteers com pared the smooth surfaced im plants with sandblasted rough surfaced im plants regarding bone-im plant contact area. M icro-sized type im plants w ere placed in m axilla & m andible and allow ed to heal for 6 m onths and 4 m onths respectively. H istological exam ination revealed that rough surfaced im plants dem onstrated significantly larger am ount o f bone-im plant contact area than the smooth surfaced implants.
In another hum an experim ent Lazzara et a l (1999) com pared therm al dual acid- etched O sseotite® im plants (B iom et 3L Palm Beach Gardens, USA) with m achined im plant surface regarding bone-im plant contact. A fter a healing period o f 6 m onths, results showed that rough surfaced im plants dem onstrated tw ice the am ount o f bone- im plant contact area com pared to m achine surfaced.
Biom echanical studies assessing rem oval torque values have shown that rough surfaced im plants require higher forces to be rem oved from the bone than do im plants w ith smooth surface (W ilke et al. 1992, C arr et al. 2001).
C arr et al. (2001) com pared torque failure levels o f com m ercially pure titanium , titanium alloy and H A -coated im plants in baboons. A fter a healing period o f 3-4
m onths results showed that H A -coated im plants dem onstrated significantly greater torque rem oval values when com pared to smooth surfaced im plants.
O ne o f the m ost recent surface m odifications is the D iscrete Crystalline D eposition (D C D ) process. This process involved deposition o f nano-stuctured calcium phosphate on the surface o f the dual acid-etched im plant resulting in discrete crystal deposits o f 20-100 nanom eters in length. The DCD process increases the m icro surface area by 200%"
Orsini et al. (2007), in a random ized controlled double-blind study, evaluated im plants w ith N anom eter-scale calcium phosphate added to the dual acid-etched surface in the hum an posterior m axilla. One 2 x 1 0 mm site evaluation im plant (SEI) with nanom eter calcium phosphate added to the dual acid-etched surface (test) and one SEl dual acid-etched surface w ithout treatm ent (control) w ere placed in posterior m axilla o f 15 patients. A fter 2 m onths o f healing, histologic and histom orphom etric analysis revealed that im plants w ith the treated surface (test) dem onstrated significantly greater bone-im plant contact area than the control. The authors concluded that the nanom etric deposition o f calcium phosphate crj'Stal to the dual acid-etched surface implants can be clinically advantageous for shortening the im plant healing period, providing earlier fixation and m inim izing m icrom otion, thus allow ing earlier loading and restoration o f function for im plants placed in areas with low- density o f bone..
The possible m echanism s by which rough surfaced im plants produce greater bone- im plant contact area than smooth surfaced include:
2- Retention o f fibrin clot at the interface zone and osteoconductive activity for osteoprogenitor cell m igration tow ards the im plant surface (D avies et al. 1998).
3- Rough surface enhances m echanical interlocking betw een im plant m acrom olecules and the bone at the bone-im plant interface ( W ennerberg et al. 1996, 1997).
Suggested clinical advantages o f rough surfaced im plants include: a- Shorter healing period.
b- The use o f shorter im plants w here vertical bone dim ensions are lim ited (e. g. posterior m andible & m axilla),
c- By using shorter im plants invasive surgical procedures can be avoided (e. g. sinus floor lift and nerve transposition),
d- The reduction o f dental im plants num ber,
e- The lack o f necessity o f biocortical im plants anchorage.
2.3 The Criteria for Implant Success
Studies have shown that the placem ent o f endosseous im plants is a predictable procedure. Several criteria have been proposed for determ ining the long-term success o f functioning dental im plants (Schnitm an & Shulm an 1979, C ranin et al. 1982 M cK inney e /a /. 1984, A lbrektsson et al. 1986, Smith 1989).
Schnitm an & Shulm an (1976) described the follow ing criteria for dental im plant success:
1. M obility less than 1 mm in any direction.
2. Bone loss no greater than one third the vertical height o f the bone.
3. Gingival inflam m ation am enable to treatm ent; absence o f sym ptom s and infection, absence o f dam age to adjacent teeth, absence o f paraesthesia and
anaesthesia or violation o f the m andibular canal, m axillary sinus, or floor o f
the nasal passage.
4. Functional service for five years in 75% o f patients.
5. R adiologically observed radiolucency graded but no success criterion defined.
Cranian et al. (1982) proposed the follow ing criteria: 1. In place 60 m onths or more.
2. Freedom from haem orrhage according to M uhlem an’s Index.
3. Lack o f m obility.
4. A bsence o f pain or percussive tenderness.
5. N o peri-cervical granulom atosis or gingival hyperplasia.
6. N o evidence o f a w idening peri-im plant space on radiograph.
M cK inney et al. (1984) described the follow ing criteria: (a) Subjective criteria
1. A dequate function.
2. A bsence o f discom fort.
3. Patient b e lie f that aesthetics and em otional and psychological attitude
are im proved.
(b) O bjective criteria
1. G ood occlusal balance and vertical dim ension.
2. Bone loss no greater than one third o f the vertical height o f the
im plant, absence o f sym ptom s and functionally stable for five years.
3. G ingival inflam m ation am enable to treatm ent.
5. A bsence o f damage to adjacent tooth or teeth and their supporting structures.
6. A bsence o f paraesthesia or violation o f m andibular canal, m axillary sinus, or floor o f nasal passage.
7. H ealthy collagenous tissue without polym orphnuclear infiltration. (c) Success criteria
1. Provide functional service for 5 years in 75% o f patients.
Albrektsson et al. (1986) described the follow ing criteria for dental im plant success: 1. Individual unattached im plant that is imm obile w hen tested clinically.
2. Radiograph that does not dem onstrate evidence o f peri-im plant radiolucency.
3. Bone loss that is les than 0.2 mm annually after the im p lan t's first year service.
4. Individual im plant perform ance that is characterized by an absence o f persistent and /or irreversible signs and sym ptom s o f pain, neuropathies, paraesthesia, anaesthesia, or violation o f the m andibular canal.
In the context o f the criteria m entioned a success rate o f 85% at the end o f a 5-year observation period and 80% at the end o f 10-year observation period are m inim um criteria for success.
Smith et al. (1989; suggested the follow ing criteria for success:
1. The individual unattached im plant is im m obile w hen tested clinically.
2. No evidence o f peri-im plant radiolucency is present as assessed on an undistorted radiograph.
3. The mean vertical bone loss is less than 0.2 mm annually after the first year o f service.
4. No persistent pain, discomfort, or infection attributed to the implant.
5. The implant design does not preclude placement o f a crown or prosthesis with an appearance that satisfactory to the patient and dentist.
Under these criteria, a success rate o f 85% at the end o f a 5-year observation period and 80% at the end o f a 10-year period are minimum level for success.
However, according to the recent abundance o f data on marginal bone loss and a better understanding o f bone and soft tissue behaviour around the implant neck and body, these criteria are inaccurate for the wide variety o f implant systems. Schwartz et al. (2005) proposed guidelines for a novel approach to evaluate the long-term success o f implants regarding marginal bone loss. Four hypothetical marginal bone loss after the first year are suggested: Low-rate marginal bone loss over the years (A lbrektsson's pattern), low-rate marginal bone loss in the first few years followed by a rapid loss o f bone support, high-rate marginal bone loss in the first few years followed by almost no bone loss, and continuous high-rate marginal bone loss leading to a complete loss o f bone support. Correspondingly, universal success criteria should be revised.
2.4 Peri-implantitis and treatment methods
2.4.1 Clinical., M icrobiological and Histopathological features
Results from recent studies indicate that peri-im plantitis is a comm on disorder and the prevalence o f subjects with peri-im plantitis varied betw een 25-45% (Fransson et al. 2005, R oss-Jansaker et al. 2006b).
Clinical studies have docum ented that peri-im plantitis m ay lead to im plant failure and loss (Van Steenberge et al. 1993, Bragger et al. 2001). Clinical features o f peri- im plantitis as described by M om belli 1999 include the following:
1 - Radiographic evidence o f vertical destruction o f the crestal bone.
2- Form ation o f peri-im plant pocketing in association with radiographic bone loss.
3- Bleeding after gentle probing and possibly suppuration. 4- M ucosal sw elling and redness.
5- Typically no pain.
Bacterial dental plaque is the prim ary causative factor o f periodontal diseases, and this has stim ulated m uch research to investigate the role o f m icroorganism s in the developm ent and progression o f peri-im plantitis. Lindhe et al. (1992) evaluated the pattern o f ligature-induced periodontitis and peri-im plantitis in B eagle dogs. Radiographs obtained 6 w eeks after the experim ent revealed substantial am ount o f bone loss at the tooth and im plant sites. Bacterial sam ples dem onstrated that the plaque that form ed in pockets was sim ilar at tooth and implant sites and were dom inated by gram negative anaerobic bacteria. C om parable results w ere reported by M arinello et al. 1995, Ericson et al. 1996, Persson et al. 1996 and G otfredson et al. 2002 who used sim ilar m odels but allow ing different periods o f tissue breakdow n.
M om belli & Lang (1994) investigated the m icrobiota associated with unsuccessful
im plants. Sam ples w ere collected from 17 im plants o f various designs and analysed
by phase-m icroscopy and in part by transm ission electron m icroscopy. Thirteen o f
these im plants, with stabilised pockets not exceeding 5 mm, were considered
successful; 4 show ed advanced pocket form ation and were thus considered failures.
A lthough the sam ples from the successful im plants yielded a predom inantly coccoid
m icrobiota, the failed im plants showed significantly elevated levels o f spirochetes.
M om belli et al. (1995), in a study o f 10 patients with B ranem ark im plants and 10
patients w ith ITl im plants, sampled the deepest residual pockets and found P.
gingivalis P. intermedia, Fusohacterium , and Spirochetes in m any o f the implant-
associated deep pockets after three and six m onths. N one o f the im plants was
colonized by A. actinom ycetem com itans, but there was a sim ilar bacterial distribution
pattern for the ITI and Branem ark fixtures. However, a three-year study by Leonhardt
et al. (1993) o f 19 patients with osseointegrated im plants showed a subgingival flora
o f predom inantly P. gingivalis, and A. actinom ycetem com itans.
Studies have show n that the im plants in partially edentulous patients are m ore at risk
for peri-im plantitis than those in fully edentulous patients, perhaps due to the
pathogenic bacteria being transferring from the tooth pocket to the im plant crevice
(M effert et al. 1992, A spe et a l 1989, Quirynen & Listgarten 1990).
H istopathologically, peri-im plantitis lesions have features that are different from those
o f periodontitis. The histopathologic exam ination o f the biopsy samples from the dog
location o f the inflam m atory lesions o f the two sites. Thus, w hile the lesion in the periodontal sites was consistently separated from the alveolar bone by a zone, about 1mm high, o f non-inflam ed connective tissue, the lesion in the peri-im plant tissue in m ost situations extended into and involved the m arrow spaces o f the alveolar bone. This indicated that the pattern o f spread o f inflam m ation was different in periodontal and peri-im plant tissues. The lesions in plaque associated periodontitis w ere lim ited to the connective tissue, w hile in the peri-im plant tissues the lesions involved, in addition, the alveolar bone.
H istopathologic analyses o f tissues sam pled from peri-im plantitis sites in hum ans revealed the presence o f large inflam m atory cell infiltrate in the m ucosa. Sanz et al. (1991) analyzed soft tissue biopsies from six patients with peri-im plantitis and reported that 65% o f the connective tissue portion was occupied by an inflam m atory cell infiltrate. Berglundh et al. (2003) also observed that num erous PM N cells were present in the hum an peri-im plantitis lesions. Such cells occurred not only in the pocket epithelium and associated areas o f the lesions, but also in the peri-vascular com partm ents distant from the im plant surface.
2.4.2 Treatment of peri-im plantitis in humans
M om belli & Lang (1992) treated 9 lesions in 9 patients by closed debridem ent and
system ic antibiotic (O m idazole). R esults showed im provem ent in clinical and
m icrobiological param eters. R adiographs obtained 12 m onth post-operatively
revealed regrow th o f bone in som e patients.
M om belli et al. (2001) treated 30 lesions with closed m echanical debridem ent and placem ent o f tetracycline fibres. R esults also show ed im provem ent in clinical and
m icrobiological param eters. H ow ever, m icrobiological param eters rebounded during
the 12 m onth observation period. Two o f treated im plants were subsequently lost.
Karring et al. (2005) studied the efficacy o f closed debridem ent alone for treatm ent o f peri-im plantitis utilizing an ultrasonic device (V ector system , DUrr Dental.
Bietigheim -B issingen. G erm any) or carbon fibre curettes. Results showed no
statistically significant differences for the im plants treated either by ultrasonic device
or m anually between base line and 3 as well as 6 m onths, regarding bleeding on
probing, PPD and radiographic bone loss. The authors concluded that closed
debridem ent alone m ay not be adequate for the rem oval o f bacterial deposit w hen the
peri-im plant pocketing depth > 5mm.
Recently Renvert et al. (2006) com pared the com bination o f closed debridem ent and topical application o f m inocyline spheres with the com bination o f closed debridem ent
and 1% chlorhexidine topical application. Result obtained after follow -up period o f 12
m onths dem onstrated that m inocycline group showed significantly better outcom es in
term o f bleeding on probing and PPD reduction. In the chlorehexidine group only a
PPD rem ained unchanged. This result suggested that the topical application o f chlorhexidine provides limited or no adjunctive clinical im provem ent com pared w ith m echanical debridem ent alone.
Data for the effect o f open flap debridem ent alone in treatm ent o f peri-im plantitis in hum ans are scarce. In a case series report by Leonhardt et al. (2003) the long term outcom e o f access surgery w as evaluated. Resolution o f peri-im plant disease w as obtained in 58% o f the im plants. H ow ever, in spite o f treatm ent 7 o f 26 im plants w ere lost and disease progression occurred at an additional 4 implants.
In an attem pt to evaluate the adjunctive decontam ination effect o f laser to the surgical treatm ent o f peri-im plantitis, Deppe el al. (2007) com pared conventional decontam inated techniques with carbon dioxide laser assisted technique. Thirty tw o patients with 73 ailling im plants included. Patients w ere allocated into four treatm ent groups:
Group 1 conventional decontam ination + soft tissue resection.
Group 2 conventional decontam ination + bone augm entation with beta-tricalcium phosphate.
Group 3 conventional decontam ination + laser decontam ination + soft tissue resection.
Group 4 conventional decontam ination + laser decontam ination + bone augm entation with beta-tricalcium phosphate.
Results showed that carbon dioxide laser decontam ination produced better clinical outcom es than conventional decontam ination especially when com bined w ith soft tissue resection.
Several attem pts have been m ade to regenerate bone tissue and prom ote
osseointegration by the use o f barrier m em branes and/or grafts.
Jovanovic et al. (1993) treated 10 peri-im plantitis defects using expanded polytetrafluoroethylene m em branes (ePTFE) and system ic m etronidazole. Result
revealed significant reduction in probing depths and m ean bone fill 2.3 mm.
B ehneke et al. (2000) evaluated the effect o f autogenous bone grafts for treatm ent o f 25 peri-im plantitis lesions in 17 patients. Follow ing flap elevation and surgical
curettage o f the granulation tissues, fixture surfaces were cleaned by air-pow der and
saline and autogenous bone in the form o f bone chips or bone blocks were placed and
adjusted in the defects. Flaps were sutured back and the im plants left non-subm erged.
Patients received m etronidazole for 7 days. A fter 3 year observation period result
show ed im provem ent in clinical param eters and a mean radiographic bone fill o f 4.2
mm.
In an attem pt to investigate the com bined effects o f m em brane and graft. K houry &
Buchm ann (2001) treated 41 peri-im plantitis lesions using autogenous bone graft
alone or autogenous bone graft com bined w ith m em brane (e PTFE or collagen).
Results show ed no difference between the bone graft alone and the bone graft
com bined w ith either e PTFE or collagen m em brane. H ow ever, in 60% o f sites
A study by Schw arz et al. (2006b) evaluated the healing o f intra-bony peri-im plant defects follow ing application o f a nanocrystalline hydroxyapatite (N H A ) paste or Bio- Oss® in com bination with Bio-Guide®. Clinical param eters were reported at the base line and after 6 m onths. R esults show ed that both treatm ents resulted in im proved clinical conditions.
Recently, a study by Ross-Jansaker el al. (2007a) com pared tw o surgical techniques using a bone substitutes with or w ithout the use o f resorbable m em brane. The non submerged approach was used. As with K houry & Buchm an (2001) study, no significant differences w ere observed betw een the groups. It can be concluded that placement o f m em branes in addition to bone grafting does not provide any adjunctive effect.
Ross-Jansaker et al. (2007b) evaluated the effect o f subm erged approach for regenerative treatm ent o f peri-im plantitis. Sixteen im plants were treated in 12 patients. Follow ing flap elevation, granulation tissue w as rem oved and im plants surfaces were detoxified by hydrogen peroxide and irrigation with saline. Bone
(R)
substitute (A lgipore ) w as placed into each defect and covered by resorbable (R)
membrane (O sseoquest ). System ic antim icrobials (A m oxicillin 375 mg x 3 + m etronidazole 400 mg x 2) were given for 10 days starting 1 day before surgery'. Following 12 m onths period o f observation significant clinical and radiographical improvements w ere observed. M ean probing depth w as reduced by 4.2 mm and mean bone defect fill o f 2.3 m m was obtained. The authors concluded that regenerative technique using subm erged approach seem ed to produce more bone defect fill than non-subm erged approach by R oss-Jansaker et al. (2007a).
From the available literature the follow ing conclusions m ay be deduced regarding treatm ent o f peri-im plantitis in hum ans:
1- M ost o f the available studies are case reports and case series. 2- Closed debridem ent alone m ay not be adequate for the
rem oval o f bacterial load from the surfaces o f im plants with peri-im plant pockets > 5 mm.
3- Closed debridem ent com bined with system ic or topical antim icrobial agents can im prove the condition o f peri- im plantitis lesions at least on a short-term basis. How ever, failures have been reported.
4- No single m ethod o f surface decontam ination (chem ical agents, air abrasive and laser) was found to be superior. 5- So far it is not known if the adjunctive use o f system ic
antim icrobial agents is required for surgical treatm ent o f peri-im plantitis.
6- Regenerative procedures such as bone graft techniques with or w ithout the use o f barrier m em branes resulted in various degree o f success.
2 .4 .3 T reatm en t o f peri-im p lan titis in anim al m odels
In m ost o f the studies peri-im plantitis was induced by sub-m ucosal placem ent o f cotton ligature. The effectiveness o f ligature induction o f peri-im plantitis and the relative sim ilarity o f this induced lesion to naturally occurring peri-im plantitis in
hum an has been questioned. Schw arz et al. (2007) carried out a com parison betw een naturally occurring peri-im plantitis defects in 24 patients with m oderate to advanced peri-im plantitis and ligature-induced defects around 3 im plants placed bilaterally in
the m andible o f five beagle dogs. Follow ing placem ent o f the im plants in the dog m odel, 3 m onths integration tim e was allowed during which a plaque control program m e was im plem ented. Follow ing ligature placem ent apical to the gingival m argin around each im plant this oral hygiene was term inated. The ligature was replaced every three weeks until 30% o f the initial radiographic bone support w as lost. The defect configuration and size was then evaluated follow ing flap elevation by m easuring the vertical and horizontal dehiscence com ponents o f the defect, the circum ferential extent o f the defect from three points (m id-buccal, m esial, distal) and the intra and supra alveolar com ponents o f the defect. The results showed a sim ilarity betw een the configuration and size o f ligature induced peri-im plantitis and naturally occurring defects in hum ans. The circum ferential defect w ithout dehiscence o f the adjacent alveolar crest was the m ost com m on configuration in both groups (55.3% o f naturally occurring defects, 86.6% o f ligature induced defects). The authors concluded that ligature induced peri-im plantitis in beagle dog m odel is a valid representation o f naturally occurring defects in hum ans and can be used in experim ental studies investigating the treatm ent o f peri-im plantitis.
V arious m ethods have been used for decontam ination o f im plants surfaces e.g. air pow der abrasion, saline w ash, citric acid treatm ent, laser therapy, peroxide treatm ent,
ultrasonic and m anual debridem ent and application o f topical m edication. The various
options have associated advantages and disadvantages. M etal curettes and m etallic
ultrasonic tips have been shown to dam age the titanium im plant surface (Speelm an et al. 1992). Superpulse laser irradiation can have adverse effects on the surface prosperities o f lased im plants (D eppe et al. 2002). C ollectively studies indicate all m ethods o f surface decontam ination achieve resolution o f the inflam m atory lesion but
fail, in them selves, to achieve significant re-osseointegration along the previously
contam inated im plant surface (Ericsson et al. 1996, Persson et al. 1996, 1999, 2001, Shibli et al. 2003, Schw arz et al. 2006a).
Ericsson et al. (1996) treated 30 ligature-induced peri-im plantitis lesions in 5 L abrador dogs by open flap debridem ent com bined with system ic antibiotic.
Follow ing flap elevation and surgical curettage o f the granulation tissue in one side,
the fixture surfaces w ere decontam inated by delm opinol HCL and the flap sutured
back. The im plants w ere left non-subm erged and antim icrobials (A m oxicillin and
m etronidazole ) adm inistered for 3 weeks starting one w eek before surgery. The
results show ed resolution o f inflam m ation around the im plants treated by local
debridem ent, no resolution o f inflam m ation around untreated implants, and no bone
fill o f the defects and no re-osseointegration. These observations dem onstrated that a
treatm ent regim en restricted to system ic antim icrobials alone is not effective in the
m anagem ent o f peri-im plantitis and that their use should be com bined with
m eticulous rem oval o f the biofilm from the contam inated im plant surface.
implants. Result showed resolution o f peri-im plantitis and bone fill in adjacent bone defects. Further, while substantial re-osseointegration occurred to an im plant with rough surface (SLA), bone grow th on the previously exposed m achined surface was minimal.
Regenerative procedures such as bone grafting with or w ithout m em branes have been investigated by different authors.
Jovanovic et al. (1993) studied the regenerative potential o f plaque-induced peri- im plant bone defects treated by subm erged m em brane technique in beagle dogs. Plaque accum ulation was achieved by tying silk ligature around the coronal im plant portion. Im plant surfaces were m achined, plasm a-sprayed or hydroxyapatite-coated. A fter 3 m onths o f plaque accum ulation and bone defect form ation, a total o f 21 im plants (7 o f each type o f im plant surface) form ed the experim ental group and 9 im plants served as controls. Test sites w ere treated with e PTFE m em brane over the defect and subm erged after the im plant surface was decontam inated using an air pow der abrasive unit and supersaturated citric acid. The result at the end o f the evaluation period (2-4.5 m onths) showed m inim al bone gain or rather fibrous soft tissue form ation in those im plants with m em brane exposure w hereas test sites in w hich a subm erged m em brane position w as m aintained, dem onstrated com plete regeneration o f the peri-im plant bone defect.. Som e re-osseointegration w as occurred in test sites but there w as no re-osseointegration in the control sites.
G runder et al. (1993) studied the effect o f guided bone regeneration in treatm ent o f experim entally induced peri-im plantitis in dogs. A fter flap elevation and surgical
curettage o f the granulation tissue, the im plant surfaces w ere cleaned by an air- pow der abrasive unit. Four groups o f treatm ent w ere random ly assigned:
- Subm erged im plants treated with open flap debridem ent alone. - Subm erged im plants treated with m em branes.
- N on-subm erged im plants treated w ith open flap debridem ent alone. - N on-subm erged im plants treated w ith m em branes.
The result showed m inimal bone fill or continued bone loss and there were no differences in outcom es betw een the four groups.
Persson et al. (1996) evaluated the effect o f guided bone regeneration in treatm ent o f experim entally induced peri-im plantitis in dogs. Follow ing flap elevation and surgical rem oval o f the granulation tissue in the left side o f the m andible, the exposed outer surface and the internal part o f the fixtures were carefully cleaned with delm opinol HCL. An e PTFE m em brane w as placed over each fixture and adjusted to cover the bone crater. N ew screw s were fitted through the m em brane to the cleaned fixture. The im plants were subm erged and the flaps sutured. In the right side o f the m andible no local treatm ent w as perform ed. The dogs were sacrificed after 4 m onths and biopsies prepared for histological exam ination. The results showed elim ination o f the inflam m atory process in the peri-im plant tissue and no re-osseointegration.
- D ebridem ent alone.
- D ebridem ent plus hydroxyapatite (HA)
- D ebridem ent plus canine dem ineralised freeze-dried bone (DFDB).
- D ebridem ent plus guided bone regeneration (GBR) using e PTFE m em brane. - D ebridem ent plus G B R and HA..
-D ebridem ent plus G B R and DFDB.
The implants w ere subm erged and m etronidazole w as adm inistered for 3 w eeks. A fter a healing period o f 4 m onths all sites were reopened for clinical m easurem ent and assessm ent o f bone regeneration. Result show ed better bone fill o f the defects with m em branes follow ed by grafts. Open flap debridem ent alone showed the least bone fill. However, there was no difference betw een m em brane use and m em brane plus bone grafts. H istom orphom etric analysis showed better re-osseointegration with m em branes follow ed by bone grafts followed debridem ent alone. M em branes com bined with grafts show ed significantly m ore re-osseointegration com pared to m em branes alone.
Schou et al. (2003a) studied the effects o f m em branes com bined w ith grafts for treatm ent o f experim entally induced peri-im plantitis in m onkeys. F ollow ing flap elevation and surgical curettage o f the granulation tissue, the implant surfaces were cleaned with cotton soaked alternately in chlorhexidine and saline. Four treatm ent groups were assigned as follow:
- D ebridem ent alone.
- D ebridem ent plus e PTFE m em brane. - D ebridem ent plus autogenous bone graft.
- D ebridem ent plus autogenous bone graft plus e PTFE m em brane.
The implants were non-submerged and metronidazole was administered for 12 days.
Sites treated with autogenous bone graft plus membrane resulted in significantly
better bone regeneration and re-osseointegration than the other techniques. Bone graft
alone and e PTFE alone were better than open flap debridement alone in respect of
bone fill and re-osseointegration.
The effect o f implant surfaces on bone regeneration and re-osseointegration had been
investigated by many authors.
Shibli el al. (2003) highlighted the influence o f different implant surfaces on bone regeneration and re-osseointegration when using expanded polytetrafluoroethylene (e
PTFE) membranes and found the greatest histological evidence o f regeneration
associated with Hydroxyapatite (HA) coated implants and the least for commercial
pure titanium implants (cpTi). Regarding re-osseointegration, the best result was seen
at titanium plasma sprayed (TSP) surfaces. Nevertheless, small sample size should be
considered.
Wetzel et al. (1999) evaluated the effects o f different implant surfaces on bone defect fill and re-osseointegration. Four types o f implant surfaces were investigated; titanium
plasma sprayed implants (TPS), TPS-furcation implants, sand-blasted acid etched
implants (SLA) and machined surface implants (M). Result showed a significant
differences in terms o f bone defect fill and re-osseointegration between different
implant surfaces with sand-blasted acid etched (SAL) being superior followed by TPS
Recently Persson et al. (2004) and Sennerby et al. (2005) both dem onstrated that
sand-blasted and acid etched im plants were superior to m achined surface im plants in term o f regeneration.
In an attem pt to com pare the surgical with non-surgical treatm ent Schw arz et al. (2006a) evaluated non-subm erged and subm erged healing o f ligature induced peri- im plantitis in dogs. Peri-im plantitis w as induced by ligature placem ent around 30 im plants in five beagle dogs. The defects were random ly and equally allocated in a split-m outh design to either closed treatm ent + non-subm erged healing (C N S) or open treatm ent + subm erged healing (OS) using an ER:Y A G laser (ERL), an ultrasonic device (VUS), or plastic curettes + local application o f m etronidazole gel (PCM ). The dogs were sacrificed after 3 m onths. All treatm ent procedures resulted in statistically significant im provem ent o f all clinical param eters. R adiological im provem ents were m erely observed at OS implants. H istom orphom etric analysis revealed that all CN S im plants exhibited com parable low am ount o f new bone to im plant contact (1.0- 1.2% ).W hile m ean bone to im plant contact was statistically significant higher in the respective OS groups (ERL 44% , PCN 14.8% and V U S 8.7% ). The authors concluded that open treatm ent with subm erged healing has better outcom e com pared to closed treatm ent w ith non-subm erged healing and ERL seem ed to be m ore suitable to prom ote re-osseointegration than PCN and VUS.
Surgical im plantation o f growth factors such as bone m orphogenetic protein-2 (BM P- 2) and platelets growth factors had been em erged as a possible treatm ent o f peri- im plantitis as well. Hanisch et al. (1997) evaluated bone form ation and re- osseointegration follow ing surgical im plantation o f recom binant hum an bone
m o rp h o g e n e tic p ro tein - 2 (rh B M B -2 ) in p eri-im p lan titis defects. H y d ro x y ap atite
c o a te d d ental im p la n ts w ere p laced b ilatera lly in m a n d ib u la r and m ax illary p re m o la r
are a o f 4 rh e su s m o n k ey s and w e re allow ed to o sseo in teg ra te for 1 year. P eri-
im p la n titis w as in duced by cotton lig atu re p lacem en t apical to the g ingival m arg in .
T h e p e ri-im p la n titis d efects w ere ra n d o m ly assig n ed to receiv e rh B M P -2 in
a b so rb a b le co llag e n ca rrier or a c a rrie r control. R esu lts show ed th at v ertical bone
g ain s as w ell as re -o sseo in teg ra tio n w e re g reater in rh B M P -2 d efects than in control
d efects. T he a u th o rs co n clu d ed th at rh B M P -2 has p o ten tial to p ro m o te bone fo rm ation
and re -o sse o in te g ra tio n in ad v an ced p eri-im p lan titis d efects in non h u m an p rim ate
m o d el.
R ece n tly , Y ou et al. (20 0 7 ) studied th e trea tm e n t o f ex p e rim en tal p eri-im p lan titis u sin g a u to g e n o u s bone grafts and p latelet-e n rich ed fibrin glue in dogs. T h irty -six
screw ty p e co m m ercially p u re titanium im plants w ith rough ac id -etch ed su rfaces w ere
in serted in six m o n g rel dogs 3 m o n th s a fte r ex tractio n o f m a n d ib u la r p rem olars. A fte r
3 m o n th s o f h ea lin g , p eri-im p lan titis w a s induced by p lacin g g au ze and w ire around
th e im p lan ts. T w o -fo u r m o n th s fo llo w in g ligature p lacem en t the resu lted bone defects
w e re assig n ed to th ree trea tm e n t g ro u p s as follow :
- O p en flap su rg e ry + co m b in atio n o f au to g en o u s bone grafts and p latelet-e n rich ed
fibrin glue.
- O p en flap su rg ery + a u to g en o u s bo n e g ra fts alone.
- O p en flap su rg ery alone (control).
S ix m o n th s a fte r healing, b io p sies o f th e im plant sites w ere taken and prepared for
an a ly sis. R esu lts rev ealed th at p eri-im p lan titis defects trea ted w ith co m b in ed
re-osseointegration com pared to the other 2 treatm ent procedures. A m ean bone-to-
im plant contact w as 50.1% , 19.3% and 6.5% for defects treated w ith the com bined
autogenous bone grafts and platelet-enriched fibrin glue, autogenous bone grafts alone
and surgery alone respectively. The authors concluded that surgical treatm ent
involving the com bined use o f autogenous bone grafts and platelet-enriched fibrin
glue m ight effectively prom ote re-osseointegration in lesions resulting from peri-
implantitis.
From the available literature the follow ing conclusions m ay be deduced regarding
treatm ent o f peri-im plantitis in anim al m odels:
1- Sub-m ucosal placem ent o f cotton ligature is the m ost com m on technique that used
to induce peri-im plantitis in anim als.
2- M ajority o f studies utilized primary' flap closure and post-operative subm erging o f
the treated defects/im plants.
3- Open debridem ent including surface decontam ination was m ore effective than
closed debridem ent in treatm ent o f peri-im plantitis.
4- Open flap debridem ent including surface decontam ination resolved peri-
im plantitis, enhanced bone defect fill and m ay result in re-osseointegration. H ow ever,
re-osseointegration was m ore pronounced on rough surfaces than on sm ooth surfaces
implants.
5- N o single m ethod o f surface decontam ination w as found to be superior.
6- Regenerative technique using bone grafting with or w ithout barrier m em branes
resulted in varying am ount o f bone defect fill and re-osseointegration.
2.5 Osseointegration of implants surrounded by bony defects
Bone loss associated w ith peri-im plantitis results in a gap betw een the im plant surface
and the surrounded bone. Such gap m ay influence re-osseointegration follow ing
treatm ent o f peri-im plantitis. The influence o f dim ension and configuration o f bone
defect at dental im plants regarding bone fill and osseointegration had been
investigated in different studies.
C arlsson et al. (1988) placed titanium rods o f varying w idths into tibias o f rabbits. A fter 6 and 12 w eeks o f healing, histologic evaluation revealed no direct bone-to-
im plant contact in 10 out o f 13 im plants when the initial gap betw een the bone and
im plant had been larger than 0.35 mm.
C audil & M effert (1991) studied the effect o f bony defects around dental im plants in
m ongrel dogs. Sim ulated extraction sockets were prepared on each side o f the
m andible. H ydroxyapatite-coated im plants w ere placed into the prepared sockets in
such a w ay that a 1 mm bony defect surrounded the coronal part o f each implant. H alf
o f the im plants received overlying barriers m em branes. A fter the 9 w eeks healing
period, the results dem onstrated that the apical “ intim ate f if ‘ portion o f each im plant
had osseointegrated at the light m icroscope level, while the coronal portions did not
have bone contacting the implant. The authors suggested that a possible cause o f
osseointegration failure at the coronal portion due to insufficient healing tim e and the
available vertical bone height allowed only h a lf o f the length o f the im plant in bone.
m andible o f each dog. One site on each side rem ained as control. The rem aining three
sites on each side were enlarged at their coronal 4 mm to create circum ferential
defects o f 0.5 mm, 1 mm and 2 mm. A fter 8 w eeks o f healing, the resuh show ed that
im plants surrounded by a gap o f 0.5 mm had values sim ilar to those o f the controls for
the level o f osseointegration and residual defect area. The im plants surrounded by
defects o f 1 mm or 2 mm dem onstrated m ore apical level o f osseointegration and
larger residual defect areas com pared to the controls. The authors concluded that
im plants surrounded by bony defects on their coronal portions can osseointegration;
how ever the level o f osseointegration is influenced by the width o f the bony defect.
Akim oto et al. (1999) evaluated the effect o f gap width on bone healing around implants placed into sim ulated extraction socket defects o f various w idths in dogs.
Four osteotom y sites. 2.7 mm wide and 10 mm long, were prepared in right and left
sides o f the m andible o f each dog. One site in each side rem ained as a control. Control
sites received 3.3 mm im plants. In the test sites, the coronal 6 mm portion was
enlarged to 4.3 mm, 5.25 mm and 6 m m. Test sites received 3.3 mm im plants. The
m odifications in the test sites created 0.5 m m, 1 mm and 1.4 mm gap around the
implants in the test sites. H istom orphom etric analysis revealed that for the coronal 6
mm o f the im plants the control sites dem onstrated the highest m ean percentage o f
bone-to-im plant contact (38.8% ), followed by the sites with 0.5 mm gaps (22.9% ), by
the sites with 1 mm gaps (11.1% ) and by the sites with 1.4 mm gaps (2.7% ). In the
apical 4 mm o f the im plants, no statistical differences in percentage o f bone-to-
im plant contact w ere found. The authors concluded that osseointegration at the
implant surface surrounded by bone defect is influenced by the w idth o f the bone
defect, with small diam eter defects show ing better osseointegration than larger
defects.
Botticelli et al. (2004) investigated bone healing at im plant sites with hard tissue defects o f varying dim ensions and configurations. Four Labrador dogs were used.
Three m onths after extraction o f all m andibular prem olars and first m olars five
im plants w ith sand blasted, large grit, and acid etched (SLA) surfaces were placed as
follow:
In the first prem olar sites the im plants w ere placed in intact bone, in the second
prem olar sites circum ferential gap 1 -1.25 mm wide was created at the coronal 5 mm
part o f each im plant, in the third prem olar sites circum ferential gap 1 -1.25 mm wide
w as created at the coronal 5 mm part o f each im plant and the buccal wall rem oved, in
the fourth prem olar sites circum ferential gap 2 -2.25 mm w ide was created at the
coronal 5 mm part o f each im plant and in the first m olar sites C ircum ferential gap 2 -
2.25 mm w ide w as created at the coronal 5 mm part o f each im plant and the buccal
w all rem oved. Results showed that four wall defects o f different dim ensions (1-2.25
mm wide) w ere resolve