The Parental Perspective of Perceived Benefits of Baby Sign Language In Preverbal Children
Laura M. Perrotta
Senior Honors Thesis School of Education
University of North Carolina at Chapel Hill 2017
Approved by:
Abstract
Previous research implies the benefits of using “baby sign language” include reduced frustration and increased parent-child bond. Additionally, some research proposes enhanced language development. Previous research analyzed benefits of using sign language with infants on language development and the parent-child bond in a highly controlled research setting. The present study surveyed parents who were currently using sign language with their babies at home in order to gain a parent’s perspective of the process of learning and using sign language and the perceived benefits. Thirty-two parents participated in the survey. Results of the study found that parents primarily used baby sign language as a tool for earlier communication in order to reduce frustration. Most parents had a positive experience, and over half of the participants did not spend any money on this process; however, many participants spoke of the difficulty in learning sign language. This information is helpful to parents of infants, as sign language could serve as a supportive tool used for earlier communication between parent and child. Parents in need of extra support could learn and implement sign language in order to facilitate the parent-child bond.
Table of Contents
Abstract 2
Introduction 4
Literature Review 10
Methodology 31
Results 35
Discussion 54
References 65
Appendix A 68
Appendix B 69
Appendix C 70
The Parental Perspective of Perceived Benefits of Baby Sign Language In Preverbal Children Using American Sign Language (ASL) to sign with hearing babies, or baby sign, has become a new trend among parents and caregivers working with young children (Nelson, White & Grewe, 2012, Seal & DePaolis, 2014). Between the ages of seven months and ten months, a baby can understand the gestures that adults make, while also attempting to make sounds themselves (Centers for Disease Control and Prevention, 2016). While this development is typical, parents often look for a different tool of communication to use with their child before he/she can speak. Communication is made up of expressive language, which is communicating one’s thoughts and desires, as well as receptive language, which is the ability to understand what others communicate (Nelson, White & Grewe, 2012).
ASL, as well as other gesturing techniques, could provide an additional tool for
expressive and receptive communication for these parents. What, exactly are the benefits? How feasible is this mode of communication for parents to learn and use on a daily basis? What babies, if any, does this method of communication benefit the most? The answers to these questions could lead to a new, innovative way to communicate with a preverbal child, and save many parents frustration and confusion in the first year and half of parenting. Parents and those promoting baby sign claim many benefits, such as earlier communication of needs and thoughts, increased language and speech development, improved literacy, increased IQ and cognitive skills, reduced frustration, tantrums, and emotional outburst, increased parent-child bonding and increased self-esteem (Meuller & Sepulveda, 2013).
processes, which is the communication and exchange between the contexts surrounding the child, the child’s development will be affected over time. The closest system to the child, the microsystem, is composed of the individuals and contexts that have the most immediate effect on the child (Bronfenbrenner and Evans, 2000). In addition, for the child to have positive outcome of development, it is imperative for him or her to form an attachment with the systems
surrounding their development. This means attaching to family and friends, as well as the larger social context including neighborhoods, schools, and the larger community’s ideals and beliefs (Bronfenbrenner and Evans, 2000). As seen in Appendix A, the bioecological model is
composed of four main systems outside of the individual; the microsystem, mesosystem, exosystem, and macrosystem. Each system is composed of different contexts in which the child is affected by, and the systems themselves interact through proximal processes (Brofenbrenner and Evans, 2000).
This theory supports the notion that it is important and necessary for parents to make a bond with their child in order to facilitate positive development. The present study will focus on language development and parent-child bonding as potential outcomes after teaching a preverbal infant sign language, and will answer the questions: 1. What are the parents’ perceived benefits of sign language? and 2. How feasible is it to learn and implement sign language?
From the literature collected and through analysis of Bronfenbrenner’s theory, the following hypotheses are proposed: (1) parents will report that sign language has supported their
Gesturing
Gesturing is the use of a symbol that represents a referent, or represents the referent’s function (Acredolo, Goodwyn & Brown, 2000, Mueller and Sepulveda, 2013). This function serves to communicate with a child what something means (i.e. flapping one’s arms to represent “bird”). Sign Language, on the other hand, is a linguistically constructed language containing semantics, intonation, syntax, lexical categories and rules just like any spoken language (Mueller and Sepulveda, 2013). Though the two are different, parents often use a hybrid of these two ways of communication to sign with their babies.
The interest in baby sign language, that is using sign language to communicate with a preverbal baby, began primarily with Acredolo and Goodwyn’s first study in 1988 exploring symbolic gesturing in typically developing children. This study, with thirty-six 16-18 month-old infants, explored how frequently infants used gesturing to communicate. Finding that many of the gestures had a purpose, rather than just spontaneously occurring, they found that there was a correlation between gesturing and communication goals (Acredolo & Goodwyn, 1988).
Following this study, the researchers were interested in exploring how purposeful
Language Development
Language development encompasses many abilities that a child acquires over time. It is defined as reaching word milestones (Seal & DePaolis, 2014), vocabulary, expressive and receptive language testing (Kirk, Howlett, Pine, & Fletcher, 2012, Goodwyn, Acredolo, &
Brown, 2000, Nelson, White & Grewe, 2012), their phonemic abilities in making and articulating sounds (Goodwyn, Acredolo, & Brown, 2000), and finally their ability to hear and respond to a story (Kirk et al., 2012). These cognitive abilities allow a child to not only speak, but also hold a conversation.
Though many studies suggest a correlation with language development and signing, there are external factors that could be attributing to this quick development; parents who sign with their children seem to be more affluent, with college educations, and thus creating a more linguistically rich environment in addition to the sign language (Seal & DePaolis, 2014). Many studies could not prove a significant difference in language development between those who sign, versus those who do not (Kirk et al., 2012, Seal and DePaolis, 2014), though they could find a trend that favored the signing group. In addition, Nelson, White, and Grewe (2012) explored the research behind the claims that encourage baby sign on the Internet. After
researching, they found that 90% of claims were either biased, or written by the website itself. In addition, though they could find effects of sign language on communication, larger vocabulary and increased parent- child bonding, many of the studies were not of high quality in that they were not longitudinal, as well as they lacked random assignment of participants.
that parents felt more “in tune” with their child when in the sign language training group, for they could see their children respond with a physical, visual cue (Cowell, Memmott, & Meeker- Miller, 2013). In addition, parents commented at the end of their experience that signing
provided them a tool for communication that lessened their frustration with their child, allowing them to form the one-to-one connection they would not have otherwise had. The children in the sign language intervention group also had an increase in vocalization from before the training to after, indicating that they were experimenting with their voices earlier than the other two groups (Cowell, Memmott, & Meeker- Miller, 2013).
In addition to the above study, Vallotton (2012) investigated the effect of symbolic gesturing for preverbal children in low-income families. Vallotton found that when children were introduced to a rich gestural environment, they were able to learn dozens of gestures before their transition to speech. Symbolic gestures fade as children acquire speech, but it allowed mothers to become more attuned to their children’s affect before this transition. Mothers claimed during this study that they viewed their own children more positively, and felt a reduction in parenting- related stress.
Parent-Child Bond
Maternal- mindedness is defined as the parent’s ability to respond and recognize their children’s cues (Kirk, Howlett, Pine & Fletcher, 2012). Gestures can draw a greater
responsiveness from adults; they see a child’s gesture, and they respond accordingly. With more gestures, children can elicit a more responsive environment for themselves (Vallotton, 2012). This ability, compatible with the parent attention, affects the parent- child bond. This is
Given the past research, many of the studies have been on affluent mothers and their children in the lab. A missing piece in the literature, however, is why it is so alluring for parents to partake in sign language with their children, how feasible it really is for parents of all socio-economic statuses, and what benefits the parents actually see. In many studies, as mentioned above, there is not a group statistical difference. What Kirk et al. (2012) recognized during their study, however, is that there can be individual benefits for certain children using sign. In the children who registered as “low-ability”, meaning they were linguistically behind their peers in word milestones and expressive and receptive language, they showed a large increase in ability after signing. This change in score could be attributed to the gestures benefitting those with weaker language skills, rather than all toddlers as a whole.
Present Study
Literature Review
Two of the main benefits that many different sites/organizations claim to come from teaching sign language to preverbal children include spoken language benefits and child-parent bond enhancement. This portion of the literature review will discuss the literature currently circulating about the benefits of sign language benefits, and in turn provide the background for the current study about feasibility of teaching sign language, and parental views of baby sign language.
Presence Language Benefits
Baby sign language has been implemented in many families across the U.S. due to many claimed benefits of teaching sign language or a similar gesture system; one of them including more rapid language development, or increased vocabulary (Nelson, White, & Grewe, 2012). Some studies have found evidence that teaching sign language during the early months of life, and later implementing it in learning vocabulary, enhances spoken language later on (Cowell, Memmott, & Meeker- Miller, 2013; Goodwyn, Acredolo, & Brown, 2000, Acredolo & Goodwyn, 1988).
There were thirty-eight 16-18 month old infants involved in this study; 21 were male and 17 were female. The babies were located by postings in a local newspaper of birth
announcements, and the families were contacted to participate in the study through an
introductory letter to the study (Acredolo & Goodwyn, 1988). The primary study included an interview of the parents to explore how often and what kind of gestures their children were using. The interviewers probed the mothers, asking what kind of symbolic actions their children were using. When the mother identified a gesture, the researchers would follow up with
questions regarding its frequency of use, context, age of onset and at what age the child began to accompany the gesture with speech. Following these questions, the mothers were asked how many words the children already said, and this was their way of measuring what type of vocabulary the infant already developed with the gestures they were using.
In order to categorize the data, Acredolo and Goodwyn (1988) made sure that two researchers reviewed each example provided by the mothers, and only considered the example a gesture if the gesture occurred multiple times within the same context and if the gesture was used in order to refer to something that is non-audible (i.e., an object or action, not a sound). From this categorization, researchers went further to separate object gestures (with the referent as an
object) and request gestures (with the purpose to elicit an action).
on a scale of 1-10 based on their number of words estimated in their vocabulary; 1=10-19 words, 2= 20-29 words, etc. (Acredolo & Goodwyn, 1988). Following this measurement, the researchers compared the children’s scores to how many signs they used and computed Pearson’s r
measurement to describe the relationship between type of gesture and number of vocabulary words. They found that children that used more object signs also had a larger vocabulary, meaning that object gestures could be linked with verbal development.
In order to see if it was another variable rather than gesturing that contributed to this vocabulary increase, researchers decided to conduct hierarchical multiple regression analyses, with the covariates including sibling status, mother’s education, sex, object signs and request signs. Results indicated that sex and sibling status were related to vocabulary, as well as object signs. They found that 28% of variance of 18-month vocabulary was due to the covariates, and 11% was accounted for by object sign presence (Acredolo & Goodwyn, 1988). From this, they concluded that it seemed Werner and Kaplan’s prediction that sensorimotor behaviors were use in the service of the representative function of verbal words seemed correct; however, in order to create a more reliable and valid study (since this one was mostly based on maternal memory and they could not monitor verbal development step by step), they created a longitudinal study to follow.
To proceed with this study, Acredolo and Goodwyn recruited 16 11-month-old infants, in which six were male and ten were females. This was a middle class sample, since 94% of
also a space for parents to record any new verbal words that were produced, with word
constituting “a sound used consistently to refer to a referent or class of referents” (Acredolo & Goodwyn, 1988, p. 458). Researchers included both the definition for “word” and for “symbolic gesture” in the beginning of each diary in order to keep all mothers recording in a similar way. At 17 months old, all infants were seen in the experimenters’ research facility and assessed for individual differences in ability to imitate and use gestures. During these video taped sessions, researchers presented a gesture in one of four categories: familiar gestures with objects (for example, putting an arm through a ring), unfamiliar gestures with objects (such as drinking from a shoe), visible gestures without objects (such as wiggling finger), and invisible gestures without objects (for example, poking puffed cheeks) (Acredolo & Goodwyn, 1988). 12 gestures in total were at random shown to the child three times, with ten seconds in between each representation. If the child was able to imitate the gesture in some way, they received credit for doing the gesture. At 20 months old, the infants were assessed for an estimate of their verbal vocabulary size and the mothers were interviewed in order to clear up any confusion researchers had about the weekly reports in regards to the infants’ signing behavior in addition to filling out a
questionnaire about current vocabulary and which words were acquired at that point.
At 24 months, the researchers took the final estimate of verbal vocabulary size, Mean Length of Utterance (MLU) was measured, and each infant was given the Mental Development Inventory (MDI) and the Bayley Scales of Infant Development in order to assess cognitive development as a whole (Acredolo & Goodwyn, 1988). This assessment was taken at the
found. For example, only 32% of object gestures occurred during interactive routines, as opposed to the 59% claimed during the interview with the mothers; however, 68% occurred outside of interactive routines compared to the 41% in the interview. The average age of acquisition of these signs differed among the gestural categories; for Object gestures, 15.59 months, for
Request gestures, 14.16 months and for Attribute gestures, 15.27 months (Acredolo & Goodwyn, 1988).
In relation to verbal development, researchers discovered that often children either had the gesture for the word, or had the verbal component for the words; they did not occur
simultaneously. This leads to the question of which comes first- the gesture or the word? To analyze this data, they organized the children’s vocabularies into five categories: 0 words, 1-10 words, 10-25 words, 25-50 words, or 50+ words, and then organized the age of gesture onset in relation to these categories. They found that 80% of the children acquired their gestures before the 25- word stage, with 71% of children acquiring Object gestures somewhere in between 0 and 25 words. This led the researchers to believe that gestures come prematurely to verbal
development, which could suggest that gestural intervention affects language development (Acredolo & Goodwyn, 1988).
The researchers recruited 103 infants, 58 were boys and 45 were girls, form a
predominately middle-class area. All children in this experiment were eleven months old, and 90% of them were Caucasian. The researchers designed this experiment with three different groups: the sign- training group (ST), the verbal training group (VT) and the non-intervention control group (NI). The ST group included 32 infants and all parents were instructed to do the gesture themselves and to always pair the gesture with the verbal word. The VT group was instructed to pay special attention to words they use in everyday life without using gestures. This was to prove that it was not the verbal words themselves that was affecting the language of the children, but rather the gesture. Finally, the NC group was not involved in any training and was not aware of the researchers’ special interest in language; this group was primarily used to compare those in the experimental groups to a child who was developing language normally (Goodwyn, Acredolo, & Brown, 2000).
Before beginning the experiment, the researchers took baseline measures through a maternal report of verbal vocabulary the infants already have, and through a measure of how frequently the toddlers vocalized during a 15-minute play interaction. For the experiment,
researchers hoped to gain insight about which signs were used more frequently than others and how the child was using them.
Along with the maternal interviews, researchers tested the children’s receptive and expressive language at 11, 15, 19, 24, 30 and 36 months of age. Many tests were used during this process, including the MacArthur Communicative Development Inventory (CID), which
evaluated several aspects of expressive vocabulary, the Sequenced Inventory of Communicative Development (SICD), which assesses both expressive and receptive language abilities in infants 4-48 months old, Receptive- and Expressive-One-Word-Picture-Vocabulary Tests (ROWPVT, EOWPVT), which also provide receptive and expressive language measures, Mean Length of Utterance (MLU), which researchers record the infants’ mean words spoken per utterance during a free play period, and finally the researchers conducted a Phonemic Discrimination Task: 21 pairs of one-syllable words that differed from each other in only one sound were presented to the child and they were tested to see if they caught the verbal difference (for those children in the ST group) (Goodwyn, Acredolo & Brown, 2000).
They conducted one of the overall scores at 15 months old because parents were, for the most part, still verbally labeling at this time.
Results showed that the ST group outperformed the infants in the NI groups in the verbal language testing overall; however, at 30 and 36 months individually, there was no longer a significant difference between the test scores. In addition, the VT group did not differ from the NI group, which suggests that signing could possibly be the component that affected the greater verbal language scores. Acredolo, Goodwyn, and Brown (2000) accredited this difference to either joint attention, child directed speech, emphasis on context while speaking to a child, as well as the signing itself. The results from this study may indicate that sign language in addition to verbal prompting encourages greater language benefits; however, these benefits may not be long lasting.
In another study, researchers analyzed how a music intervention versus a sign language intervention affected both the child’s communication efforts and the parent-child relationship (Colwell, Memmott, & Meeker-Miller, 2013). In this study, researchers compared across three different groups of children: a sign language group, a music group, and a sign language and music group, with ten dyads of caregiver and child in each group. Each group met weekly for four weeks and followed detailed plans for intervention; each session was videotaped and led by the same music therapist in order to ensure consistency among the groups. The mean age of the Music group was 12.3 months, 12.9 months for the Sign Language group, and 12.4 months for the Music and Sign Language group.
addition, they were sent home with worksheets after each session with a review of the signs, and given a copy of Baby Sing and Sign after the posttest.
For the music intervention, parents used song material from Clap your Hands: Play-Filled Songs for Little Children (Miller, 2004 as cited in Colwell, Memmott & Meeker- Miller, 2013) and Baby Sign and Sing, (Miller, 2007 as cited in Colwell, Memmott & Meeker- Miller, 2013) as well as thematic material taken from the board book My World (Brown, 2001 as cited in Colwell, Memmott & Meeker- Miller, 2013). A sheet of targeted words that were used in lessons was sent home each week. The sessions for this were broken up into four different centers in which the children took part: music (books and songs), centers (vestibular, textile, etc.), music review, and goodbye lullaby.
The Music and Sign Language group used Baby Sing and Sign, the music CD, and My World, as primary thematic material. During these sessions, participants were exposed to sign language that was both thematic (such as a book), and functional (such as “more”). Sessions were divided into the same four centers as the Music alone group. Parents were sent home with weekly worksheets, as well as the music materials after the first week and the board book after the posttest (Colwell, Memmott, & Meeker-Miller, 2013).
Pre- and post-tests were conducted using two measures: The Early Communication Indicator (ECI) and the Indicator of Parent-Child Interaction (IPCI). Both rounds of assessments were held in the same room by the same researchers and videotaped in order to maintain
consistency. ECI measures infants’ communication in the way in which they express wants and needs (for example, vocalizations, gestures, words, and sentences to convey utterances).
Memmott, & Meeker-Miller, 2013). ICPI measured how often parents respond to their child in ways that promote positive emotional behavior; these measurements were taken during four activities including free play, looking at books, distraction task and dressing. Each activity was rated on a 4-point scale (never, rarely, sometimes, and often) in ten- minute intervals of play.
Concluding this study, researchers found that results from the ECI had higher
vocalizations for the sign language alone group, and the ICPI reveal that parent-child interactions increased and there was an increase in child engagement for both the sign language group and the Music and sign language group. This could have also been attributed to the structured play in which parents were taught how to interact with their child both verbally and nonverbally. Parents reported during an informal interview after the assessments that they felt more in tune with their child using sign language because it facilitated the one-on-one relationship. The ICPI also
revealed a decrease in parental interruption and child distress as the sign functioned as a “tool” to communicate and decrease frustration (Colwell, Memmott & Meeker-Miller, 2013).
Lack of Language Benefits
Nelson, White and Grewe (2012) sought out to identify the credibility of the 33 websites claiming that preverbal sign language yielded language benefits. They used content analysis, which combines objective, quantitative and systematic review of the message that was
Though the outcomes were consistent across websites, the researchers wanted to assess the credibility of the journal articles, book chapters, books, newspapers, articles, etc. that were cited as evidence for these outcomes. Out of the 82 pieces of evidence that were cited on the website, only eight of them were research articles, with five of them written by Acredolo and Goodwyn (1985, 1990, 2000), and three of them written by Daniels (1996 & 2004) (Nelson, White & Grewe, 2012). Through this analysis of evidence, the researchers found that even when the research was found in peer-reviewed journals, they often analyzed research that either taught gestural information to the infants or relied on parent recall for the study. They also found that the studies sampled a small population, making the study less reliable. From this analysis, the researchers were able to identify that the websites claims were not reliable and that they could not successfully claim that it was sign language that was the cause of any increased language ability or early communication (Nelson, White & Grewe, 2012). This study found a lack of quality evidence for the support of language benefits.
hours, number of infants, and information about the fathers’ work and education). The mothers in the VT group were told to model the target words as they used them in interactions in order to control for the fact that mothers in both the SG group and the BSL group were both using the target word as well as some sort of gesture during their interactions. By giving all of the experimental groups the same target words they could directly compare the verbal or manual adoption that resulted between the groups (Kirk et al., 2012). In all conditions, the frequency of use of the gesture and/or target use was monitored and recorded.
There were two sets of targets, the first including object signs (such as drink or hat) and non- object signs (such as where or all gone). The second target set was chosen based off of what mothers thought they would use most often (such as shoe, dog and biscuit). In order to collect data about the frequency of signing and interactions, mothers were interviewed twice a month (Kirk et al., 2012). During this interview, mothers were also asked if they thought their child was able to understand the word and/ or sign. Researchers visited mothers in all groups to model the sign language and to teach them what to do, and they all received a pack of materials that had illustrations.
Researchers found that over time, mothers signed less and less with their child. Mothers were signing the most frequently with their child at 16 months of age; however, at 20 months of age, this modeling started to decline. This is more than likely due to the emergence of consistent language. All toddlers were able to acquire at least two signs, while some were able to acquire up to 20 signs by 20 months of age. Results revealed that between groups, gesturing along side the target words did not accelerate acquisition of first words. There was no significant difference in receptive and productive vocabulary, nor in auditory comprehension or expressive
significant differences among groups, this possibly was not the case for individuals within the group.
To identify individual gains, researchers ranked the infants within each condition from one to four, one being the lowest in ability in the pre-intervention and four being the highest in ability. The dependent variable for this test was the change in mean rank from pre-intervention to post-intervention. For males, the mean rank of low ability increased when exposed to the gesture condition and expressive communication also increased for those individuals that ranked as low ability it the pre-intervention test. This suggests that for individuals who are scored as having low linguistic ability to begin with, sign language or symbolic gesturing may affect their
language abilities; however, overall, no evidence proved significant that overall gesturing or sign language increased the language ability of the toddlers.
This controversy over the effects (or lack thereof) of sign language on language
were not able to obtain information about parent signing (such as frequency or accuracy) or sign selection.
They studied 40 tapes of children exposed to BS and 38 tapes of non-signing children. They used data from the York lab data (the previous study they were using the video sets from) that documented when each child demonstrated 4, 10, and 25 words in the video sessions in order to determine which videos contained this information. By determining the number of days that had passed since their birthdays at the time of the milestone videos, they were able to figure out the age of onset of each milestone. In order to analyze each video, Speech Language
Pathology graduate students coded the manual activity from segments of vocal productions throughout the sessions. They coded and transcribed the manual activities with the ELAN software by marking where the vocal activities were as well as where the manual activities were, and seeing if they corresponded. By looking at vocal and manual activities separately, they were able to reduce the expectations of observing the manual production with the vocal production accompanying it. Seal & DePaolis (2014) defined manual activity as all visible hand movements when both hands were visible, and vocal activity as any babbling or vocal productions. The graduate students were trained to identify and code based on right and left hand configurations basked on the Stokoe hand shape notation, whether or not the configuration involved an object, a description of the manual activity, and whether the hand shape occurred by itself or in a
The researchers found that both groups had the same amount of manual productions paired with verbal productions, and all infants in both groups reached the 4-word milestone by or before 18 months of age (all but one of the NS group). They found that five infants in the NS reached the 10-word milestone and all eight infants in the BS reached the same milestone; this difference, however, was not found to be statistically significant. Four in the NS group and six in the BS group reached the 25-word point by the end of investigation, but again this difference was not statistically different. The researchers conducted 2 ANOVA tests to measure the sign status’ effect on word points and sign status’ effect on age of completion, but neither was found to be statistically significant. From this study, the researchers concluded that the abundance of manual activity with vocal activity suggests that though the results favor the signing group, none of the differences between the groups were significantly different. While manual activity does seem to support vocal activity, it does not seem that baby signing alone causes greater language
development.
Parent-Child Bond Benefits
The effect of baby sign on enhancement of the parent- child bond, and the ability it gives parents to be more responsive to their children constitutes as another perceived benefit of those who are proponents of baby sign language (Kirk et al., 2012, Nelson, White, & Grewe, 2012, Zammit & Atkinson, 2016, Mueller & Sepulveda, 2013).
inappropriate mind- related comments, encouraging autonomy, imitation, responding to change in infant object- directed action/gaze, and other (Kirk et al., 2012). A second coder coded 8 of the 72 video taped sessions at each age of assessment in order to ensure equal sampling from both groups and both genders.
The mother’s encouraging maternal mind- mindedness scores were computed by
summing the proportion of maternal utterances that were categorized as mind-related comments, imitations, encouraging autonomy, and responding to changes in infant object- directed
action/gaze. From these scores, researchers computed that mothers in the gesture condition produced a higher proportion of encouraging comments than mothers in the control condition. There was no significant difference in change in maternal MM overall, but there were subtle differences associated with positive changes in a mother’s interactions with her infant with gesture training. The increase usage of positive comments in the gesture condition, however, suggests that by revealing some of their internal thoughts through gesture, infants gave their mothers’ greater insight into their abilities and were more involved in the interaction (Kirk et al., 2012). Since the sample only consisted of 18 infants, generalizability is not recommended.
researchers were able to compare the relationship between choice of child activity and maternal MM and comparing the development of kids’ vocabularies. In addition, by including a group participating in a different activity, researchers would be able to better say that it was the sign language itself that led to the differences in vocabulary and maternal MM (if there were differences) (Zammit & Atkinson, 2016). The researchers allowed mothers to choose which group they would like to participate in in order to support the notion that mothers who choose to sign with their children are more or less sensitive to their child than those who do not choose to partake.
Participants were recruited via baby sign classes, toddler groups and by word of mouth/posters placed around university campuses in England. The baby sign group had 15 participants (6 boys and 9 girls) ages 11.5-26.3 months, and the non- sign group had 19
participants (8 boys and 11 girls) ages 14.5-28.3 months (for a total of 34 participants). In order to measure the vocabulary of the children, researchers used the MacArthur Communicative Development Inventory (CDI) for mothers to complete in order to provide a snapshot of total vocal and gestural vocabulary. Maternal MM was measured using the Meins and Fernyhough’s brief interview protocol and associated coding scheme. Mothers were asked open-ended
questions and responses’ content was categorized into four categories: mental attributes
(children’s thoughts, feelings, etc), physical attributes (child’s appearance), behavioral attributes (ex: she’s very cuddly) and general attributes (Zammit & Atkinson, 2016). Researchers contacted the child activity groups and gained permission from the instructor so that they could be present during the groups’ meetings. All mothers were visited at their home or at the university
Maternal age, maternal education, child age, time spent in daycare, siblings, and child gender were tested prior to the experiment in order to determine if they should control for those factors. None of them were found to be significantly different. In both groups, 75% of mothers had achieved at least a degree- level education. They found from their study that there was no significant effect between the groups on CDI scores of receptive and expressive vocabulary. They did find, however, that the maternal MM scores were significantly higher for the baby sign group than the non- baby sign group. Though this supports the notion that mothers attending baby sign classes have a higher MM than other mothers, it does not support that MM leads to communicative ability. There are two explanations for this data: either mothers that attend baby sign classes have a higher MM and seek out a communication tool, or that attending baby sign classes may have improved maternal MM (Zammit & Atkinson, 2016). Either way, the mothers in the baby sign group had higher maternal MM scores, and thus were more responsive to their babies.
There is an emphasis on sensitive and attuned parting during the first months of life in order to promote stable relationships within families that do not falter as greatly in times of stress (Oldbury & Adams, 2015). A study reviewed 20 pieces of literature in order to explore the impact of infant crying on parents. They used databases including CINAHL, Psychinfo, PubMed, SCOPUS, and Summon in order to find articles published between 2003 and 2013 about infant crying. Nine of these studies identified the impact of infant crying on the parent-infant
Oldbury and Adams’ (2015) analysis revealed difficulties and delays in parent bonding with their baby due to the infant crying; this is a significant concern because the impact of poor attachment and parent responsiveness is great on overall child development. Contemporary attachment theory states that the importance of good quality close relationships is incredible when related to promoting the child’s emotional and social development. Interruptions in this process can be critical (Oldbury & Adams, 2015). It is crucial to identify parents who are experiencing difficulties in coping with infant crying and provide services and ways to cope. In addition, it is important for professionals who are working with new parents to allow them to feel supported in discussing their feelings of frustration and to allow them to have the intervention opportunities that are needed (Oldbury & Adams, 2015). This study indicates the importance of parents having some sort of way to communicate with their child earlier on (though, not every parent may need that), and one of the possible ways could include sign language in order to allow parents to connect with their child earlier on.
children and to understand the impact that baby signs have on the parent-child interactions. Low SES parents often do not understand the importance of talking to their infants, so often children from low- SES families are less likely to be exposed to as long of utterances and rich vocabulary (Hoff, 2003). The workshop took place at a university SLP clinic. Initially, a traditional
classroom setting was used, but eventually changed to a circle of chairs with a rug in the center to facilitate interaction among the parents, children, and researchers (Mueller & Sepulveda, 2013).
The first 35 signs that emerge for Deaf children were used in this experiment. Parents were encouraged to use sign naturally in the context of their daily routines and to just use the signs that felt natural to the daily parent-child interactions. Researchers and the ASL teacher reassured parents that sign is separate from spoken language (Mueller & Sepulveda, 2013). During each session, the first 30-45 minutes was spent with just the parents discussing their challenges of the week, their progress with sign language, and any confusion they were having with the signs. This allowed the parents to have a debrief session with each other and the researchers on the study. Each week, a binder was given out with handouts about the signs that were introduced that week. The children were brought in after each workshop and the families practiced with their child with books, etc. Concluding each session, parents asked last minute questions. The first week was an introduction to signs, the second week was food items and related verbs, the third week was toys and animals, the fourth week was emotions and routines, and the final week was miscellaneous signs that parents had requested throughout the workshop.
their child was not stressful at all. The one parent who reported it was stressful responded that they were stressed at first, because she felt as though her baby was not paying attention; however, she reported that after the researchers assured her this was normal, the process was totally comfortable (Mueller & Sepulveda, 2013). Parents enjoyed having a time to interact with their child and to ask questions to learn more sign language. Parents’ most observed changes in child language and communication was increased eye contact, more focus and attention to hands and an increase in vocalization and use of sign. Researchers recognized that during this study, there were 4 researchers to about 9 parents, so it was easier for parents to feel more supported. Parents felt a sense of belonging and communication with their child during this process, and they felt as though they had more time to spend with their child (Mueller & Sepulveda, 2013).
Methodology
The methods section outlines the design of the study that aimed to investigate parental perspective about teaching baby sign language, their perspective of the learning process, and the overall feasibility of learning and using sign language. This section will additionally outline the survey process of recruiting participants through convenience sampling and will describe the instrumentation of the data collection. The survey participants will also be outlined.
While previous studies addressed the benefits of using signs with infants in laboratory settings, this study surveyed parents who chose to learn sign on their own and aimed to
understand why parents started learning sign, and what method they used to incorporate this into their everyday lives. In addition, this study aimed to collect information about parents’
perception of the process, retrospectively, and the resources they used to learn and execute baby sign language. With this research, findings will provide insight about how parents learned sign language, their perception of this early communication tool, and how feasible it is to incorporate into everyday life as a new parent.
Research Design
Survey Participants and Setting
The owner of a local Speech- Language clinic in Chapel Hill, NC who teaches sign language to parents to use with their babies offered to send the survey to participants. The owner sent the link to the survey out to her email list, as well as through her Facebook page that she uses to keep contact with present and previous clients. This method of recruitment led to approximately 800 contacted people. In order to complete the survey, participants’ only qualification was to be a parent teaching sign language to an infant before the age of language onset. Clicking the link to the survey brought participants to a consent letter that included intent of the study. The participants continue to the survey after reading and clicking “next,” which indicated their consent to participate. No identifying demographic information was asked
(including name, birthdate or any other information). Once the participant began the survey, they could choose to stop the survey at any point.
Twenty-eight responses were collected following the first email (as seen in Appendix B) and the Facebook post. These responses came in from mid-May to mid-August. After submitting an addendum to the original IRB application, a second email was sent to parents. This email was exactly the same as the first email. It served as a reminder about the study and to let parents know that the survey was still open for responses. The survey was open for two more weeks after the reminder email was sent. Four additional responses were collected following the second email. The coding process began with these data from these 32 responses
Obtaining Institutional Review Board Approval
Training Initiative’s Group 2 Social and Behavioral Research training in addition to the requisite conflict of interest disclosures prior to the beginning of the study. The collected data did not include name, birth date, or any other personal information that could identify the participants. All data were stored in Qualtrics’ HIPPA-compliant secure database.
An addendum was added to the IRB application on August 9, 2017 and was reviewed and approved on August 25, 2017. This addendum stated that there would be a reminder email sent to parents in order to collect additional responses to the survey that was initially distributed. The information was stored through the same Qualtrics survey database for the second round of responses.
Data Collection Procedure
The survey was designed using Qualtrics. The survey consisted of ten qualitative
questions and eight quantitative questions that collected demographic information including age, gender, race, occupation, and number of children. The survey can be viewed in Appendix C. The qualitative portion of the survey collected information about the parents’ experience using and learning sign language with their baby, as well as advice for parents who aspire to use sign language with their children. The survey could only be accessed after reading the consent letter attached in Appendix D.
Data Coding Procedures
Data coding procedures included using the CSV file uploaded to Microsoft Excel from Qualtrics to code the results. Prior to beginning the coding process, the researcher examined the theory that originally derived the hypothesis. Bronfenbrenner theorized that a child’s
bond with the child. Given the literature, and the amount of time that the parents would spend focused on the child to increase the amount of signs used by the child, the researcher
Results
Data were analyzed from the 32 parents (.04 response rate) teaching sign language to their children who responded to the survey. Both qualitative and quantitative results are
presented. Additionally, included are the themes identified in the qualitative data inquiring about the child’s response to signing, parental perspective, and feasibility.
Parents could choose to skip whichever questions they were not comfortable answering, therefore each question has a different total of responses. The number of respondents per
question can be seen in Table 4.1 below. A copy of the survey is also included in Appendix B for reference.
Table 4.1 Number of Respondents per Survey Question
Question n % Total
1a Gender 31 96.88%
1b Age 32 100%
1c Occupation 32 100%
1d Race 31 96.88%
1e Education Level 32 100%
1f Total # of Children 31 96.88%
1g # Children Signed With 31 96.88%
2 Why did you start signing 23 71.88%
2a Age of child when started 23 71.88%
2b When did child sign back 23 71.88%
3 How did child respond 23 71.88%
5 Like least about signing 18 56.25%
6 Describe learning sign 20 62.50%
7 Wish to be different 17 53.13%
8 Did you spend money 21 65.23%
9 What method of signing 22 68.75%
10 Advice to other parents 20 62.50%
Participants Demographics
The participants were asked several questions related to their demographics. This included their gender, age, occupation, race and education level. The participants were also requested to give the total number of children they had and the number of children with whom they introduced signing.
Gender. Thirty- two participants completed the survey. Thirty-one of the 32 participants
included their information about gender. One participant was male (3%), while thirty participants (93.8%) were female, and there was one non-respondent (3%).
Age. The ages of the participants ranged from 27 to 46, with most of participants in the
30-34 range. Six participants were over the age of 40 (19%), 10 participants were between 35 and 39 (31%), 14 participants were between 30 and 34 (44%) and 2 were under 30 (6%). In addition, parents were asked to report their career status.
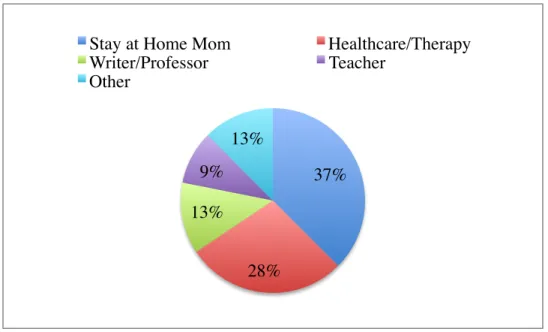
Occupation. Parents were asked to report their career status. Most of the parents reported
teachers (9%), and other (13%), including professions such as preschool trainer and security guard.
These results can be seen in figure 4.1, 4.2 and 4.3, respectively, below. Figure 4.1 Gender of Participants
Figure 4.2 Age of Participants
6 10 14 2 0 2 4 6 8 10 12 14 16
40+ 35-39 30-34 <30
N u mb er of P ar ti ci p an ts Age (years) 1 30 1 0 5 10 15 20 25 30 35
male female No response
Figure 4.3 Occupations
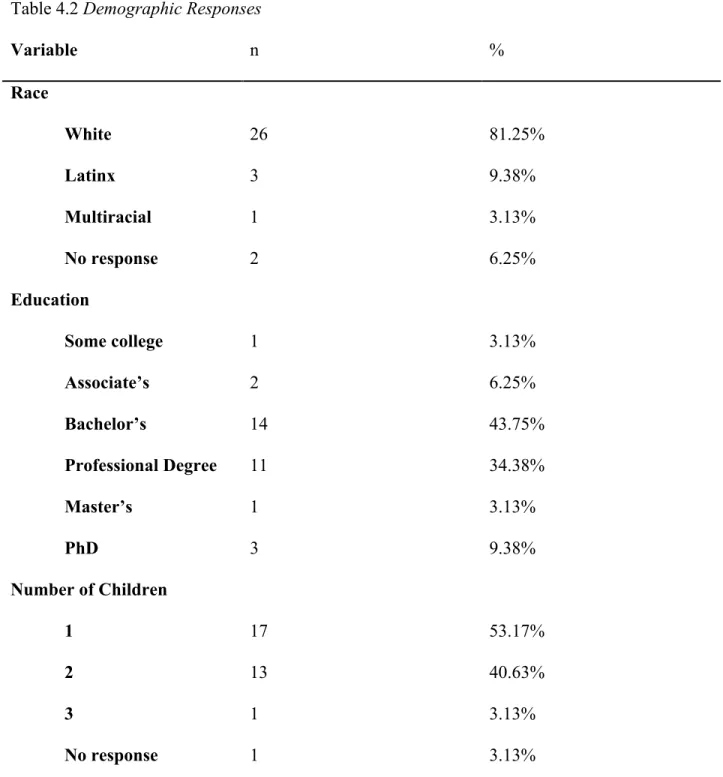
Race. Thirty- one participants answered the question revealing their racial identification.
Twenty-six participants identified as white (81.25%), 3 participants identified as Latinx (9.38%), 1 participant identified as multiracial (3.13%), and 2 participants chose not to answer this
question (6.25%).
College level. All of the participants of this study indicated that they completed some
portion of college; 1 participant indicated starting college (3.13%), 2 achieved an Associate’s Degree (6.25%), 14 achieved a 4-year degree (43.75%), 11 achieved a professional degree (34.38%), 3 achieved their PhD (9.38%) and 1 completed their Master’s (3.13%). This indicated that all parents (100%) completing this survey who used sign language were educated beyond a high school level. A professional degree constitutes a degree of higher learning that does not constitute as a Master’s degree.
Number of Children. When asked how many children they had, 17 participants
indicated having one child (53.17%), 13 indicated having two children (40.63%), and 1 indicated having three children (3.13%). There was 1 non-respondent (3.13%).
37%
28% 13%
9% 13%
Stay at Home Mom Healthcare/Therapy
Writer/Professor Teacher
Number of children parents signed with. Twenty participants signed with one child
(62.5%), 10 signed with two children (31.25%), and 1 signed with three children (3.13%). There was 1 non-respondent (3.13%).
All of these results can be viewed in Table 4.2. Table 4.2 Demographic Responses
Variable n %
Race
White 26 81.25%
Latinx 3 9.38%
Multiracial 1 3.13%
No response 2 6.25%
Education
Some college 1 3.13%
Associate’s 2 6.25%
Bachelor’s 14 43.75%
Professional Degree 11 34.38%
Master’s 1 3.13%
PhD 3 9.38%
Number of Children
1 17 53.17%
2 13 40.63%
3 1 3.13%
Number of signing children
1 20 62.5%
2 10 31.25%
3 1 3.13%
No response 1 3.13%
Children’s Response to Learning Sign Language
This section includes the results to the questions that pertained to the way in which the child responded to signing with the parent. Parents were asked four questions pertaining to how their children responded, when they responded, when they started signing with their children, and why the parent began signing with the child in the first place. Responses were coded based on themes of early communication, frustration reduction, observation and initial failures.
How did child respond. The first question parents were asked about their child’s
response to signing was “How did your children respond to your signing? Feel free to share an example.” To this, parents’ responses followed four themes: earlier communication, lowered frustration levels, observation, and failure to respond.
Earlier communication. Most of the answers followed the theme of earlier
communication (58.33%). An example of a response in this category is as follows:
Parents also spoke to the slower onset of signing, but the aid to early communication that it served once their babies caught on:
“Sign recognition and usage took a few months but the results were astounding. I started around 5mo and signs from Lo (child’s name) came around 8mo. Most frequently used sign at first was 'milk' and helped ease frustration for both of us.”
In addition, one participant revealed the help that it served for her child before and after the onset of spoken communication: “She loved it! It facilitated her early communication ability greatly when she was preverbal and now she has advanced verbal skills, but still enjoys signing for fun!”
Lower frustration. Participants also discussed the frustration reduction that occurred after
learning and using the signs. Four out of 24 (16.66%) participants discussed their child’s use of sign in order to communicate prior to verbal language, and the way in which this tool reduced the frustration of not being able to communicate needs. One participant spoke to this:
“They both started signing back around 1 yr old. Once my oldest started speaking we dropped signing. Signing seemed to help with frustration levels for them and myself when trying to communicate with each other before they could verbally produce words.” The use of signs was very helpful to these parents in supporting their children’s communication in order to communicate what they needed.
Observation. Some children did not sign right away; rather, parents noticed that their
Initial failure. While many children did respond with signing, this was not a completely
effective tool of communication for every family that utilized this method. Three out of 24 (12.5%) participants reported failure with signing at first, or a lack of response from their child to their signing. One participant responded that “We just started a month ago, I find that I don't do it consistently. He doesn't really pay attention.” Another participant reported that they used basic signs with their child, but the child only really picked up on one sign, “more.” This participant reported that though their first child did not acquire many signs (though the one sign they did pick up was useful), they plan on trying with their newborn in a couple of weeks.
Why parent started signing. The next question about child response asked parents,
“Why did you start signing with your child?” Emergent themes are stated below.
Early communication. Responses varied, but nearly half of parents (11 out of 23,
47.83%) reported that they were interested in signing with their child in order to provide a tool for communication prior to their child’s ability to verbally communicate. One parent stated, “To help bridge the gap between when they started wanting to communicate but didn't have words yet,” which was similar to another parent who spoke to the desire “To give him the ability to communicate and begin to develop his expressive vocabulary. (The idea of reducing tantrums by giving him the ability to express his wants/needs was also appealing.)”
Previous experience. Some participants spoke to their experience with child development or someone else who used baby sign language prior to using it with their own child. Two of the 23 respondents (8.70%) explored the effects of sign language prior to using it with their own child, and decided to incorporate this intervention due to their experience or knowledge that they had about sign language. One participant specifically heard about baby sign language from his/her brother, who reported his success with sign language with his own child.
Decrease frustration. Parents also decided to incorporate sign language in order to reduce frustration that their child experienced due to the lack of ability to communicate. Three of 23 respondents (13.04%) spoke to the desire to reduce this frustration. One participant reported having twins, and was searching for anything that would make it easier with them. In addition, one participant wanted their child to use this method to increase language ability to then reduce frustration in the toddler years.
One participant reported the desire to allow their toddler to incorporate their body in engagement with the parent. This was the only response that spoke to the physical nature of sign language; in addition, it was the only response that cited the physical connection as the main reason for incorporating sign language into the family’s daily life.
Age child introduced to signs. Parents were asked when they started signing with their child. The most common age for introducing sign language was 6 months old. The average age that parents introduced sign language was around 5.12 months. The maximum age of
introduction was 12 months. The minimum age of introduction was birth (which was calculated as 0.5 in order to calculate all arithmetic measures). The results can be seen below in Table 4.3.
about 8.98 months. The maximum age of response was 18 months, and the minimum age of response was about 4 months old. For all responses that provided a range for both introducing and responding to signs, the smallest age was taken into account in order to calculate the above measures. In addition, there were 2 out of 25 participants who reported their child never started using signs, or has not yet. For results that were reported with both their first and second child’s data, they were reported as two separate responses, and calculated separately into the total. These results can be seen in Table 4.4.
Table 4.3 Ages of Introduction to Sign
Measure Age (months)
Minimum 0.5 (birth)
Maximum 12
Mode 6
Mean 5.12
Table 4.4 Ages of Response to Sign
Measure Age (months)
Minimum 4
Maximum 18
Mode 9
Mean 8.98
This section includes the results related to the parent’s perspective about their experience with the sign language. It incorporates their opinions of what went well, what did not go well, what they wish had been different about their experience and a description of learning sign language. The goal of this section is to report the overall themes that parents experienced during their sign language process with their child.
What did you like most. Parents were first asked, “What do you like most about signing
with your child?” Several themes emerged that are discussed below.
Increased communication. Eleven out of 23 (47.83%) responses were related to the
theme of communication. Parents reported that they enjoyed the use of signs in order to
communicate needs or wants before the child was able to use spoken language. One participant reported that they enjoyed “that I could respond to what they actually wanted instead of what I guessed they wanted. Even if we had only done 4 signs -- milk, eat, more, and all done -- those 4 alone were so helpful it would've been worth it.” In addition to this ease of communication, participants reported that the combination of spoken directions and signs increased their ability to communicate with their child successfully, in addition to allowing the child to communicate back. This participant stated, “Signs gave him a way to communicate and helped him understand my verbal directions when paired with a sign.”
Parent-child connection. Parents also reported the sense of pride that their children felt
after learning and executing a new sign, and how this facilitated a special bond between them. Seven out of 23 (30.43%) respondents spoke to this effect sign had on their child. One parent stated,
secret language that we can use without disrupting others or being rude, as well as in loud or busy settings without having to yell. For example signing "potty" versus yelling that when she needs to go. Also, I'm able to give her a stern look and sign "no," or "stop," from across the playground or at church.”
Another parent had a similar experience with his or her child: “Understanding needs before my child could ever verbalize. I feel our connection was stronger because we could understand each other, rather than just one-sided communication on my part.” This strengthening of the child to parent bond, and the child’s confidence was a poignant theme in the results.
Reduced frustration. Consistent with responses to other questions, parents also liked the lessening of frustration for their child that resulted from the use of sign language. Six of the 23 responses (26.08%) stated that their favorite part of signing was the ability to allow their child to communicate earlier, which in turn reduced their frustration. Parents stated that signing was useful in “understanding what they want which reduces crying/screaming/tantrums/frustration” as well as providing a tool to “be able to communicate across the room, and knowing what they need or want without them getting frustrated.”
What they like least. Parents were also asked what they like the least from signing with their child. Several themes emerged with this question.
Difficulty learning. Nine out of 18 (50%) participants responded that it was difficult for them to learn, remember and to use the signs. One participant stated that she/he felt “that I don't know what I'm doing and have no time or energy to devote to learning it ahead of them.”
consistency across caregivers, especially if the caregiver did not know enough sign language to also incorporate it into every day life for the child.
Finding time. Four of the 18 (22.22%) participants reported that sign language was difficult due to the amount of time it took their child to sign back or consistently sign. One participant stated that, “I wanted it to be more immediate and more in depth, but this was
developmental not a downside to sign language.” In addition, on participant said, “I know my 16 month old knows some signs but he refuses to use them.” This was not a strong theme in the results, but present. Four participants (22.22%) stated that there was nothing that they did not like from their experience using and teaching sign language to their child.
Other people’s comments. One participant (5.55%) reported that they did not like people’s comments about them using sign language with their child. They did not elaborate on the comments made, or the relationship they had with the people making the comments.
Description of the Learning Process. Parents were asked to describe their learning process of sign language. Additionally, they were asked to elaborate on the process and any difficulties while using sign language.
Structured system. One of the largest pieces of feedback from parents is the need for a class or structured system for learning sign language. Five out of 20 (25%) responses talked about the need for a class, or how the class was the main source of help for them during their time learning and using sign language. In addition, one participant discussed the helpfulness of adopting more than one method of learning:
DVDs (which my daughter absolutely loved/loves!!). It's easier to learn with repetition, relevant use, and I also like learning/teaching kids through song. In general, having multiple modalities to learn has helped solidify the learning experience for both my daughter and me.”
Previous experience. Many participants (25% of respondents) already had experience with American Sign Language (ASL) in some capacity, making the process of learning sign easier than it would have been with no experience. One parent also spoke to how their learning type aided them in learning and using ASL: “I had experience working with Deaf kids before I had my own so it was already second nature for me, which made signing with my kids easier.”
Lack of Experience. Parents without prior experience discussed the difficulty of
remembering the signs, as well as the difficulty of incorporating them into their everyday lives. Five out of 20 participants (25%) discussed this difficulty, but one participant discussed the way in which he or she found support:
Another respondent also discussed the importance of family support during the process they found difficult:
“We didn't use a ton of different signs, didn't want it to be overwhelming. That kept it easy for all family members to participate--I think we consistently used about 10 with her and she ended up using maybe 5 herself (eat, more, nursing, up & all done).”
Ease of online resources. Lastly, some parents discussed using online methods in order to train and learn ASL to use with their baby, reporting that it was easy to use and learn ASL. Three out of 20 participants (20%) utilized this method, and reported it to be successful and efficient for them to learn ASL. One participant found online methods to be more supportive than books: “Books could be difficult when motion was involved; I found YouTube to be the most helpful.”
What could be different. Parents were additionally asked, “What do you wish had been different about your experience with singing with your child/ren?” Some participants (23.5%) simply responded “nothing,” but the remaining emergent themes are included below.
Resources. Many parents reported that they think they would have benefited from more resources to aid them in learning and practicing sign language. One parent specifically wrote: “I wish there had been more ways to incorporate it into their lives without it all having to come just from me, a total novice. Like classes or exposure to other adults signing, etc.” Other parents that indicated a thirst for more resources included that more consistency through these resources would have benefited the child’s signing.
participants (17.64%) indicated that they had continued to use it, after verbal words were acquired. A participant stated, “I wish he still remembered some of them. Once he had a language growth spurt, his words were faster and easier and he never bothered signing again.”
Consistency. One out of 17 participants (5.88%) stated, “I wish I used it more. Also my childcare, since I work full time much time is with the nanny.” This need for consistency across all adults working with the child was a common theme among other questions as well.
Feasibility
This section will review the amount of money that parents spent in learning how to sign with their babies, which methods they used, and what advice they would offer to parents who are planning to sign with their babies. The purpose of these questions was to gauge the feasibility of signing with a child.
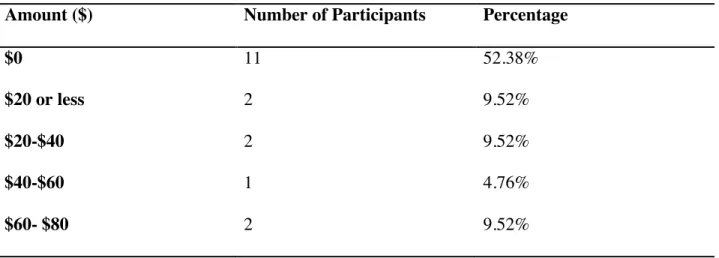
Money. Parents were asked “Did you have to spend any money to learn how to sign with your child? Please select around the amount of money you spent in learning and teaching sign language to your baby.” Results can be viewed below in Table 4.4. The majority of parents (52.83%) stated that they did not use any money during the process. The most any participant reported spending was between $100-$120. Results can be viewed below in Table 4.4. Table 4.4 Money used to learn and use sign language
Amount ($) Number of Participants Percentage
$0 11 52.38%
$20 or less 2 9.52%
$20-$40 2 9.52%
$40-$60 1 4.76%
$80-$100 2 9.52%
$100-$120 1 4.76%
Type of Sign. Parents were additionally asked which type of sign they used when teaching their baby sign language. Fourteen respondents (59.09%) indicated they utilized ASL. Three respondents (13.64%) utilized Baby Sign, 4 participants (18.18%) used a combination of gestures, Baby Sign and ASL, and 2 respondents (9.09%) utilized an alternative method of signing. The four that reported using a combination of signs used a combination of all three (but mostly ASL), Baby sign and ASL adapted to motor skills, or ASL and family specific signs. The two that reported “other” used signs that the parent learned in college, and some pidgin. The results can be seen below in Figure 4.4.
Figure 4.4 Methods of Signing
Future Advice. The final question that parents were asked was “What advice would you give to other parents who want to start signing with their babies?”
13 3 4 2 0 2 4 6 8 10 12 14
ASL Baby Sign Combination of two or more of
the above Other N u mb er of P ar ti ci p an ts
Do it/early introduction. Four out of 20 participants (20%) responded to “do it early,” meaning to start signing with the baby early on in development. Four out of 20 participants (20%) responded to simply do it. One participant stated: “Do it! The scientific benefits are vast, and hey, maybe they will be able to communicate with you.”
Consistency. Six out of 20 participants (30%) stated to stay consistent with the signing. One specifically stated,
“Stick with it! Sometimes it takes a while to see "results" but if you stick with it and do it consistently with lots of repetition, they will most likely sign back. There's this sort of hump you have to get over...at first it's hard to remember to sign at all, then you remember to do it but you forgot how to do the sign. As new parents there's lots going on, but it really will be well worth it if you stick with it!”
Relevant signs. Four out of 20 participants (20%) stated that it is easier when the parent picks the signs most relevant to their baby to learn and use in everyday life. One participant specifically stated that this practice relieves frustration with the child:
“Figure out where your child gets frustrated the most and add words that are related to that topic first. Mine got frustrated in demanding to be picked up and getting food. That's where I focused my time in learning signs so that there was an outlet for his
communication.”
Overall, the results to all of these questions indicated that parents were satisfied with their signing experience, and that it helped them communicate with their child earlier on.