Ramesh Kumaresan et al., J. Sci. Res. Phar. 2013, 2(2), 7-18
J
ournal of
S
cientific
R
esearch in
P
harmacy
Review Article
Available online thr oug h
ISSN: 2277-9469
www.jsrponline.com
Nifedipine-Induced Gingival Overgrowth: A Report of Six Cases and Comprehensive Review of the
Literature with Recent Advances
Priyadarshini Karthikeyan1, Ramesh Kumaresan2*, Arishiya Thapasum Fairozekhan3, Faraz Mohammed4 1Post Graduate Student, Department of Oral Medicine and Radiology, Sri Balaji Dental College & Hospital, Chennai, India.
2Lecturer, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, AIMST University, Malaysia.
3Assistant Professor, Department of Oral Medicine and Radiology, Dr.Syamala Reddy Dental College Hospital & Research centre, India 4Assistant Professor, Department of Oral and Maxillofacial Pathology, Dr.Syamala Reddy Dental College Hospital & Research centre, India.
Received on: 30-04-2013; Revised and Accepted on: 16-05-2013
ABSTRACT
Gingival enlargement, an over-exuberant response to a range of local and systemic conditions, is a common finding in a routine dental practice. A greater part of such enlargements, however, occurs as an unwanted side effect of medications used mainly for systemic treatment for which the gingival tissue is not the projected target organ. An increasing number of medications are recently associated with gi ngival enlargement. Among those medications, gingival enlargement induced by nifedipine has been extensively reported. Although frequently reported, nifedipine -induced gingival enlargement remains a perpetual topic of discussion due to its several obscure features. This review summarizes the importance of gingival overgrowth as a clinical problem following systemic medication of nifedipine, and highlights recent advances that lead to an enhanced understanding of the biological mechanism underlying the overgrowth. A simple flowchart summari zing the various treatment options have been proposed. We also report a series of s ix patients with this condition.
Key words: Nifedipine, gingival-overgrowth, calcium channel blockers, side-effect.
INTRODUCTION
Clinically apparent gingival overgrowth (GO) is a common finding in otherwise healthy humans[1]. Being one of the most important
clinical features of any gingival pathology, GO represents an over-exuberant response to a variety of local and systemic conditions and has been associated with multiple etiological factors which includes inflammation, hereditary, neoplastic conditions, those resulting from adverse drug effects and is of idiopathic origin [2-5]. The mainstream of
cases, however, occurs as a side-effect of systemic medications [5]. The
medication-induced GO occurs as an undesirable side effect of drugs used mainly for systemi c treatment for which the gingival tissue is not the projected target organ [6]. An increasing number of medications are
recently associated with gingival enlargement. Currently, more than 20 prescription medications are associated with gingival enlargement [7].
These medication-related conditions are previously labeled as gingival hyperplasia or gingival hypertrophy. But these terms do not truly reflect our present understanding of the macroscopically enlarged and histologically altered gingiva, which is not merely due to increase in number of cells or the size but is due to an inflammatory component. Hence the term gingival enlargement or overgrow th is preferred [6, 8-10].
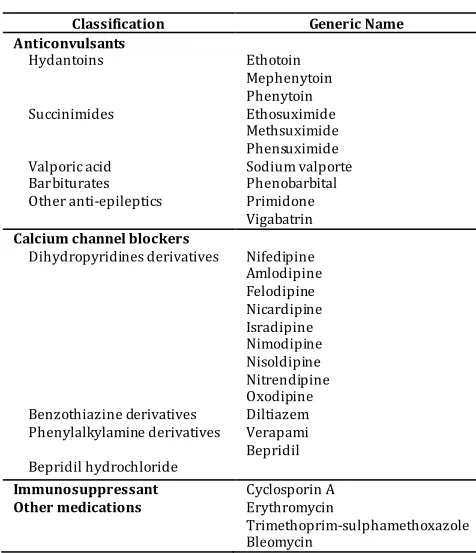
Drugs associated with GO can be broadly categorized in to three groups according to their therapeutic actions, namely anticonvulsants, calcium channel blockers (CCB) and immunosuppressants (Table 1). Although these drugs have different pharmacologic effects and are primarily directed towards various target tissues, all of them appear to act similarly on a secondary target tissue, that is, the gingival connective tissue, causing alike clinical and histopathological findings [2, 8].
The present review summarizes the importance of GO as a clinical problem following systemic medication of nifedipine, a calcium channel blocker and, highlights recent advances that lead to an enhanced understanding of the biological mechanism underlying the overgrowth. A straightforward flowchart summarizing the various treatment options have been proposed. We also report a series of six patients encountered with nifedipine-induced gingival overgrowth (NIGO).
*Corresponding author:
Dr. Ramesh KumaresanLecturer, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, AIMST University, Malaysia. Ph: +60-16-4672921.
*E-Mail: [email protected]
Table No. 1: Drugs associated with GO
Classification Generic Name
Anticonvulsants
Hydantoins Ethotoin Mephenytoin Phenytoin Succinimides Ethosuximide
Methsuximide Phensuximide Valporic acid Sodium valporte Barbiturates Phenobarbital Other anti-epileptics Primidone Vigabatrin
Calcium channel blockers
Dihydropyridines derivatives Nifedipine Amlodipine Felodipine Nicardipine Isradipine Nimodipine Nisoldipine Nitrendipine Oxodipine Benzothiazine derivatives Diltiazem Phenylalkylamine derivatives Verapami Bepridil hydrochloride Bepridil
Immunosuppressant Cyclosporin A
Other medications Erythromycin
Trimethoprim-sulphamethoxazole Bleomycin
Case reports:
Case 1:
Fig. 1a: Case 1: Inflamed overgrowth of anterior papillary and marginal gingival
Fig. 1b: Case 1: Inflamed and ulcerated gingival overgrowth in molar region
Case 2:
A 57-year old male was taking nifedipine (60 mg/day) for 5 months as a treatment to control his hypertension. The patient complained of GO, three months after initiation of therapy. Examination revealed a generalized fibrous overgrowth confined to the papillary gingiva. There were no signs of inflammation (Fig. 2a, 2b).
Fig. 2a: Case 2: Fibrous overgrowth confined to the papillary gingival
Fig. 2b: Case 2: Papillary overgrowth covering the middle third of the anatomical crown
Case 3:
This relates to a 60-year old female who was on nifedipine (40 mg/day) for past 5 years. The patient complained of generalized GO for past ten months with localized pus discharge. Examination revealed a generalized gingival enlargement involving papillary and marginal gingiva with gingival pocket and pus discharge noted from mandibular left premolar region. The pathologic area was severely inflamed with bleeding on probing (Fig. 3a, 3b).
Fig. 3a: Case 3: Severe generalized inflamed gingival overgrowth
Fig. 3b: Case 3: Inflamed gingival enlargement in the lower arch
Case 4:
The patient is a 36-year old female who was treated with nifedipine (20 mg/day) for past 8 months. The chief complaint of the patient was generalized overgrowth of gingiva for past 3 months. Examination revealed generalized inflamed papillary GO with bleeding on probing (Fig. 4).
Fig. 4: Case 4: Generalized gingival overgrowth
Case 5:
Fig. 5a: Case 5: Severe generalized fibrous and lobulated gingival enlargement
Fig. 5b: Case 5: Microscopic view of excised overgrowth
Fig. 5c: Case 5: Recurrence of gingival overgrowth after six months of surgical excision
Case 6:
This relates to a 49-year old male, who was prescribed nifedipine (40 mg/day) to control his hypertensive condition for the past 2 years. The patient noticed mild swelling over his gums which developed over the past 12 months. Intraoral examination revealed a generalized GO involving papillary and marginal gingiva with pseudo-gingival pocket and bleeding on probing (Fig. 6).
Fig. 6: Case 6: Generalized inflamed gingival papillary overgrowth
DISCUSSION
Calcium channel blockers:
Edentulousness is declining as an oral condition in most countries. Older individuals continue to comprise an over larger fraction of our population and are keeping their teeth throughout their lifetime[1].
Such older individuals regularly take various medications for the treatment of the cardiovascular problems, and today the most extensively and widely used antihypertensive compounds are CCB.
Calcium has a central role in cellular physiology. It mediates contraction of cardiac, skeletal and smooth muscles, act as an intracellular signal regulating key enzymes in metabolism, neurotransmission and hormone release, controls cellular differentiation and growth, and plays a significant role in the host immune response [11].
Calcium entry into the cell is regulated by receptor-mediated calcium specific channels in plasma membrane and this movement of extracellular calcium ions into the cardiac and vascular smooth muscles through specific ion channels is essential for their contractile process [1 , 12].
CCB exert their action by inhibiting calcium ion influx across the cell membrane of cardiac and smooth muscle cells, without changing the serum calcium level, there by interfering or blocking mobilization of calcium in to the cell [13, 14]. As a result they cause prolonged dilatation of
coronary arteries and arterioles, in addition to decreased myocardial contractility and oxygen utilization by the myocardium, and slow atrio-ventricular conduction [14, 15]. Hence CCB are extensively used for the
management of several cardiovascular conditions, including hypertension, angina pectoris, coronary artery spasm and cardiac arrhythmia – i.e., supra-ventricular tachycardia. CCB are also prescribed for idiopathic (or primary) pulmonary hypertension where their potent vasodilating effect improves the oxygen supply to the myocardium, while simultaneously decrease the oxygen demand by the heart, hence they lower both the pulmonary artery pressure and pulmonary vascular resistance, to increase cardiac output and improves exercise tolerance
[16].
These CCB are grouped as dihydrophyridine derivatives (nifedipine, felodipine, amlodipine) and benzothiazine derivatives (diltiazem). Of these, nifedipine, though introduced in 1972, was not approved by the Food and Drug Administration for use in the United States until 1982 [17, 18]. But since its approval it has become increasingly
popular due to its widespread usage for the treatment of acute and chronic cardiac insufficiencies, including essential hypertension and chronic stable angina [18, 19]. Side effects of this drug are perhaps rare, but
include head aches, dizziness, nausea and tiredness, hypotension, muscle cramps, flushing, tremor, joint stiffness, peripheral oedema, dermatitis, pruritus and urticaria [18, 20, 21]. It was in 1984, a report from an Israeli
research team [22] demonstrated in five human subjects that GO could
occur as a side effect subsequent to a chronic regimen of nifedipine. Subsequently, authenticating reports have appeared [15, 23-27],
significantly increasing consciousness of this undesirable side effect in the dental community.
Nifedipine-induced gingival overgrowth:
Among CCB, GO has been most frequently reported subsequent to administration of nifedipine. The incidence of GO associated with nifedipine therapy is highly controversial. Since prescription of nifedipine is relatively common, it is difficult to determine the true incidence of its GO [2]. However the reported
incidence rate ranges from 0.5% to 85%.[4, 28-31] (Table 2) Few authors
criticized that this wide range of incidence may be attributed to the methods used to assess GO or the population sampling technique [32]. In
many of these incidence studies, the samples were based upon hospital patients who were attending either a cardiac clinic or a dental clinic. While such a sampling technique will produce an adequate sample of patients who are taking CCB, it is not a true representation of the population prescribed with these drugs. In addition, the sample of patients examined in these studies were small [32]. However, the overall
prevalence of NIGO appears to be approximately 38% [29].
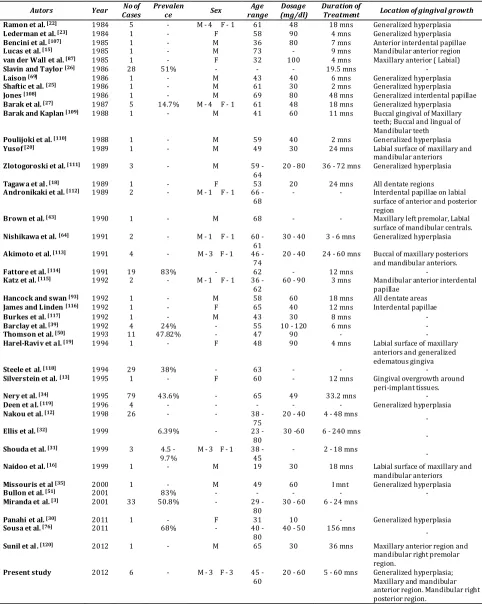
Table No. 2: Compilation of NIGO cases reported in literature
Autors Year Cases No of Prevalence Sex range Age (mg/dl) Dosage Duration of Treatment Location of gingival growth
Ramon et al. [22] 1984 5 - M - 4 F - 1 61 48 18 mns Generalized hyperplasia
Lederman et al. [23] 1984 1 - F 58 90 4 mns Generalized hyperplasia
Bencini et al. [107] 1985 1 - M 36 80 7 mns Anterior interdental papillae
Lucas et al. [15] 1985 1 - M 73 - 9 mns Mandibular anterior region
van der Wall et al. [87] 1985 1 - F 32 100 4 mns Maxillary anterior ( Labial)
Slavin and Taylor [26] 1986 28 51% - - - 19.5 mns -
Laison [69] 1986 1 - M 43 40 6 mns Generalized hyperplasia
Shaftic et al. [25] 1986 1 - M 61 30 2 mns Generalized hyperplasia
Jones [108] 1986 1 - M 69 80 48 mns Generalized interdental papillae
Barak et al. [27] 1987 5 14.7% M - 4 F - 1 61 48 18 mns Generalized hyperplasia
Barak and Kaplan [109] 1988 1 - M 41 60 11 mns Buccal gingival of Maxillary
teeth; Buccal and lingual of Mandibular teeth
Poulijoki et al. [110] 1988 1 - M 59 40 2 mns Generalized hyperplasia
Yusof [20] 1989 1 - M 49 30 24 mns Labial surface of maxillary and
mandibular anteriors
Zlotogoroski et al. [111] 1989 3 - M 59 -
64
20 - 80 36 - 72 mns Generalized hyperplasia
Tagawa et al. [18] 1989 1 - F 53 20 24 mns All dentate regions
Andronikaki et al. [112] 1989 2 - M - 1 F - 1 66 -
68 - - Interdental papillae on labial surface of anterior and posterior region
Brown et al. [43] 1990 1 - M 68 - - Maxillary left premolar, Labial
surface of mandibular centrals.
Nishikawa et al. [64] 1991 2 - M - 1 F - 1 60 -
61
30 - 40 3 - 6 mns Generalized hyperplasia
Akimoto et al. [113] 1991 4 - M - 3 F - 1 46 -
74
20 - 40 24 - 60 mns Buccal of maxillary posteriors and mandibular anteriors.
Fattore et al. [114] 1991 19 83% - 62 - 12 mns -
Katz et al. [115] 1992 2 - M - 1 F - 1 36 -
62 60 - 90 3 mns Mandibular anterior interdental papillae
Hancock and swan [93] 1992 1 - M 58 60 18 mns All dentate areas
James and Linden [116] 1992 1 - F 65 40 12 mns Interdental papillae
Burkes et al. [117] 1992 1 - M 43 30 8 mns -
Barclay et al. [39] 1992 4 24% - 55 10 - 120 6 mns -
Thomson et al. [50] 1993 11 47.82% - 47 90 - -
Harel-Raviv et al. [19] 1994 1 - F 48 90 4 mns Labial surface of maxillary
anteriors and generalized edematous gingiva
Steele et al. [118] 1994 29 38% - 63 - - -
Silverstein et al. [13] 1995 1 - F 60 - 12 mns Gingival overgrowth around
peri-implant tissues.
Nery et al. [34] 1995 79 43.6% - 65 49 33.2 mns -
Deen et al. [119] 1996 4 - - - - - Generalized hyperplasia
Nakou et al. [12] 1998 26 - - 38 -
75 20 - 40 4 - 48 mns -
Ellis et al. [32] 1999 6.39% - 23 -
80 30 -60 6 - 240 mns -
Shouda et al. [31] 1999 3 4.5 -
9.7% M - 3 F - 1 38 - 45 - 2 - 18 mns -
Naidoo et al. [16] 1999 1 - M 19 30 18 mns Labial surface of maxillary and
mandibular anteriors
Missouris et al [35] 2000 1 - M 49 60 I mnt Generalized hyperplasia
Bullon et al. [51] 2001 83% - - - - -
Miranda et al. [3] 2001 33 50.8% - 29
-80 30 - 60 6 - 24 mns
Panahi et al. [30] 2011 1 - F 31 10 - Generalized hyperplasia
Sousa et al. [76] 2011 68% - 40 -
80
40 - 50 156 mns -
Sunil et al. [120] 2012 1 - M 65 30 36 mns Maxillary anterior region and
mandibular right premolar region.
Present study 2012 6 - M - 3 F - 3 45 -
60 20 - 60 5 - 60 mns Generalized hyperplasia; Maxillary and mandibular anterior region. Mandibular right posterior region.
Clinical features:
Clinical manifestation of gingival enlargement usually appears within 1 to 3 months after initiation of nifedipine therapy [8, 18, 19]. In our case series, the earliest appearance of gingival enlargement
was 5 months in two patients. Though GO may occur around any natural teeth and may also involve dental implants in certain susceptible individuals, it frequently occur in the anterior labial gingiva in the presence of bacterial accumulation and gingival inflammation, while edentulous areas are usually not affected [13, 15, 18, 22, 28, 33] (Table 2).
However, Nerg et al., reported that 10.3% of edentulous patient in their study developed overgrowth in the mucosal region [35]. It usually
commences as a papillary enlargement which increases and coalesce with adjacent interdental papillae, giving the gingival tissues a lobulated or nodular appearance [2, 28, 35] (Fig. 5a). The fibrotic enlargement is
generally confined to the attached gingiva but may extend coronally and interfere with occlusion, masticati on and speech [2, 3, 8, 14, 28, 35].
factors inducing inflammation [28]. This may favor the appearance of
clinical symptoms and signs that include pain, friability of the tissue, abnormal movement of the teeth, changes of appearance, phonetics and occlusion, as well as the appearance of dental caries and other periodontal disorders [3, 36, 37].
Lafzi et al., has categorized DIGO in to vertical enlargement and outgrowth (horizontal) enlargement and postulated that pocket/pseudo pocket formation is associated with gingival inflammation and hence TGF-β1 and other factors responsible for the production of a fibrous scaffold may be essential for the vertical growth
of gingival-pseudo pocket development. Also the formation of periodontal pocket necessitates the inflammatory degradation of the periodontal tissues and as an alternative, periodontal pocket formati on may precede the inflammation [4].
Pathogenesis:
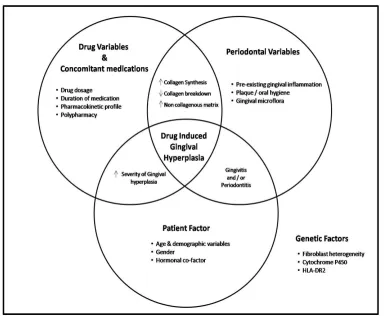
Despite extensive studies, the pathophysiology and the exact cause of NIGO has not been effusively identified. However, several theories have been suggested (Fig. 7).
Fig. 7: Pathogenesis of NIGO
Hassell and Cooper [38] proposed the “cell subpopulation
theory” to explain the pathogenesis of phenytoin-induced gingival overgrowth, which holds good with nifedipine also. They suggested that, there are phenotypically distinct and functionally different subpopulations of morphologically similar gingival fibroblasts, some of which are “responders” and others “non-responders”. The responder fibroblasts are characterized by an increased cell proliferation rate, DNA synthesis and collagen synthesis and in some way induced to become the predominant cell in GO and hence termed “key cells” [39, 40].
Studies have also confirmed that patients developing GO have high frequency of particular HLA antigens and genetic markers (cytochrome P450, HLA-DR2) and this appears to be related to a genetic predisposition for this pathology. This explains why GO does not develop in all patients taking nifedipine.
Vander Wall et al. and Barclay et al., proposed that the synthesis of collagen and collagenase are calcium dependent cellular events [24, 39]. Nifedipine interferes with calcium transport, reducing
cytosolic calcium levels in gingival fibroblasts (due to alteration in calcium-sodium exchange), thus interfering with activation and collagen synthesis by gingival fibroblasts [39]. The fibroblasts from patient treated
with nifedipine may produce an inactive form of collagenase, which would obviously reduce the collagen breakdown. This mechanism along
with over production of collagen and extracellular ground substance leads to GO.
Recent studies afforded two main pathways as most probable mechanism of NIGO; inflammatory pathway and non inflammatory pathway.
(i) Inflammatory pathway:
a. Decreased uptake of folic acid:
Vogel [41] hypothesized that DIGO may be due to a decrease in
intracellular calcium influx which causes a decrease in cellular folic acid uptake, producing a localized folate deficiency thus, limiting the production of the collagenase-activating enzyme deficiency, which is the active form of collagenase. Folic acid deficiency could also lead the gingival tissues susceptible to inflammation by causing degenerative changes in the gingival sulcular epithelium. Since the presence of inflammation causes proliferative increase in connective tissue, the catabolic ability of collagenase is saturated, and the inhibited degradation of the extra cellular matrix causes a localized accumulation of this matrix leading to GO [42, 43].
b. Androgen metabolism:
Sooriyamoorthy et al., explained in their report that circulating androgen levels were increased in patients treated with nifedipine, cyclosporine and phenytoin [44]. They also recognized the interaction
readily metabolize 5α-dihydrotestosterone and the active metabolite could act on subpopulation of gingival fibroblasts and cause either an increase in collagen synthesis and/or a decrease in collagenase activity aiding in GO [45].
(ii) Inflammatory pathway:
a. Role of inflammatory mediators:
Considerable epidemiological evidence substantiates that plaque-induced gingival inflammation exacerbates the expression of drug-induced gingival enlargement [32, 46-52]. Though exclusive studies on
inflammatory changes in NIGO are scarce, similar studies in phenytoin and cyclosporine-induced gingival overgrowth provides us some simultaneous evidence. It has been hypothesized that all these drugs reduce cytosolic free calcium in recruited T-lymphocytes. Such an action will interfere with T-cell proliferation and activation, leading to impaired collagen resorption [39]. Hence, it was suggested that drug-induced
changes in T-cell function together with the elevated number of macrophages in susceptible gingival tissues may be instrumental in initiating a fibrous hyperplastic response [53]. This mechanism is also
confirmed by a comparative study by Dahllof et al., who found a substantially more mononuclear cells in phenytoin-induced gingival overgrowth tissues than healthy or inflamed gingival [54]. The number of
langerhans cells also increased in gingival epithelium in patients with phenytoin-induced gingival overgrowth [55]. It has also been shown that
an increase in interleukin-1 is related to an increase in Langerhans cells in clinically inflamed gingival [56]. Interleukin-1 can stimulate fibroblast
proliferation in the presence of primary growth factors, thus leading to GO .
b. Role of growth factors:
Current studies have elucidated a variety of growth factors which control connective tissue homeostasis. Drugs that cause GO obvi ously target these growth factors and their activation may have an important role in the pathogenesis of DIGO [53]. Few studies have focused on
interaction of phenytoin with epidermal growth factor and platelet derived growth factor which suggested an increase in epidermal growth factor receptors on the cell surface of gingival fibroblast obtained from responders and an increase in platelet derived growth factor secretion from macrophages and monocytes [57, 58].
c. Keratinocyte growth factor:
Daset al., demonstrated that NIGO upregulates both keratinocyte growth factor secreti on and gene activity in gingival fibroblasts [59].
Keratinocyte growth factor is the seventh member of the fibroblast growth factor family. It is produced by mesenchymal cells and its activity is specific for epithelial cells, controlling epithelial homeostasis and wound repair. Although keratinocyte growth factor has been implicated in a number of hyperplastic pathologies, its role in the molecular pathology of NIGO has been documented recently. The effect of nifedipine may occur directly on keratinocyte growth factor or indirectly mediated through other growth factors such as platelet derived growth factor and TGF β or certain cytokines which have been reported to be upregulated in DIGO [13, 30, 59].
Risk factors for NIGO:
Various risk factors have been identified for NIGO and have been systematically reviewed recently [45, 60]. These identifiable factors
can be concise under four issues; patient factor, drug variables, periodontal variables and genetic factors (Fig. 8).
Fig. 8: Risk factors for NIGO Patient factor:
(i) Age:
Age has been considered as an important risk factor for various DIGO s but i s not an applicable risk factor for the CCB since the use of these drugs is usually confined to the middle aged and elderly [45].
Correspondingly, all our patients were middle aged with age ranging from 45 to 60 years. A study by Ellis et al., on more than 800 patients medicated with CCB supports this statement that age was not identified as a significant risk factor for GO due to CCB [32].
However, age has been identified as a risk factor in patients medicated with a combination of nifedipine and cyclosporine where,
younger patients show a higher prevalence of overgrowth [61, 62]. This
may be an effect of drug association rather than the age of the patients.
(ii) Gender:
Many of the studies involving NIGO patients have a significant male bias, with males being 3.3 times more likely to develop overgrowth than females [32]. Various reasons have been quoted for this male bias.
Since use of CCB are comparatively higher in male as men have higher incidence of cardiovascular disease than women [63]. A link to hormonal
co-factor has also been suggested, since nifedipine is said to alter androgen metabolism [44, 45, 64]. Animal studies also support this finding,
female sex hormone, progesterone is found to suppress GO in rats as they decrease glycosaminoglycan synthesis by human gingival fibroblasts [64, 66]. It has been suggested that there exist a serum
threshold level of nifedipine above which GO occurs, and this level is higher in females than in males, although the maximum degree of GO is virtually the same in both [65].
Drug variable and concomitant medications:
There exist a considerable controversy concerning the relationship between the expression of GO and drug variables which include drug dosage, duration of therapy, serum and salivary concentration. Most would agree that a certain threshold concentration of the drug or its metabolite is necessary to initiate the gingival changes and such a threshold concentration may vary from individual to individual [45, 53]. However, Daley et al., suggested that increasing the
levels of the drug above this threshold did not increase the severity of the lesion [46]. But studies concluded that drug dosage to be a poor
predictor of the gingival changes [39, 67, 68]. It would be more appropriate
to correlate dose with the patient’s body weight to obtain a more meaningful interpretation of drug dose and its relationship to GO [45, 60].
Duration of appearance of GO after initiation of nifedipine therapy has been evaluated adequately in literature [3, 16, 18, 64]. The rate at
which the clinically noticeable GO occurred in response to nifedipine therapy varied from one month to 19 months with a mean of 9 months
[15, 23, 27, 69]. On an average initial gingival changes can occur within 3
months of dosage. The pattern of overgrowth development shows significant individual variation, but may reach a “state of equilibrium” often within the first year of commencing medication [53]. Longer
treatment periods did not result in further increase in the overgrow th, however changes in drug therapy, or systemi c illness may alter this state and lead to further gingival changes [53, 64]. On the other hand, regression
of overgrowth as early as one week to 3 months after withdrawal of the drug have also been documented [23].
An insight evaluation of various pharmacokinetic profile of nifedipine as a risk factor of GO has been carried [31, 45, 53, 64, 70]. Ellis et al.,
stated that those subject taking nifedipine appeared to be more at risk for developing GO that those taking other CCB (amlodipine) due to its different physio-chemical profile and pharmacokinetic variation [32].
Since amlodipine is more polar than nifedipine, with a pKa value of 8.7, the drug may not pass through cell membranes without an active transport mechanism, By contrast, nifedipine is extremely liphophilic and will dissolve readily within the cell membrane and pass in to the cytoplasma, which enhances the drug/cellular interaction within the gingival tissues. Similarly, amlodipine has a long half-life (t½=34 hrs) and a high volume of distribution (21 litres/Kg) but the corresponding figures for nifedipine are 7.5 hrs and 0.78 l/kg respectively. These dissimilarities entail that majority of amlodipine will be tissue bound and hence inactive rather than circulating freely in blood. With its long half-life, and steady plasma state, amlodipine rarely achieve a threshold plasma state to cause GO but nifedipine tends to exhibit pronounced peak plasma levels [31, 32].
Local concentration of nifedipine in gingival crevicular fluid has provided some useful insight in to local tissue activity [70]. Ellis et al.,
with an ultrasensitive assay, measured the pharmacokinetics of nifedipine in plasma and gingival crevicular fluid and found that the concentration of nifedipine was 105 times greater in gingival crevicular fluid than in plasma of patients who developed overgrowth and hence proposed that gingival tissues sequestrate nifedipine. This high concentration appears to be related to the degree of gingival inflammation thus predisposes the tissue to overgrowth [53, 70].
Considerable evidence suggests that the combination of nifedipine with cyclosporine in organ transplant patients produce more GO [50, 71-75]. However, it has also been suggested that combined therapy
may increase the prevalence (51% compared with 8%) of the condition but not the severity [26]. They also concluded that local factors and
pharmacological parameters were unrelated to overgrowth and
indicated a trend for HLA A19-positive patients to show signs of inflammation, suggesting an underlying genetic susceptibility. Nevertheless, few researchers also documented that overgrowth was not potentiated by concomitant medication [48, 49].
Periodontal Variables:
Plaque score and gingival inflammation are considered an important risk factor in the expression of GO correlated to nifedipine use
[49, 50, 67, 68, 70, 76]. Most of the evidence to support this relationship has
been derived from cross-sectional studies, and it is impossi ble to determine the true sequence of events with respect to the role of gingival inflammation in the development of overgrowth as whether plaque is a contributing factor or a consequence of the gingival changes [32, 39].
A patient’s existing gingival condition, that is, the extent of inflammation present prior to dosing may also be a significant risk factor for overgrow th. Nakou et al., isolated Gram-negative anaerobic bacteria in high numbers from nifedipine-induced enlarged gingival indicating the development of an anaerobic environment [12]. It seems that the
enlarged gingiva influence the subgingival ecosystem by creating the appropriate environment of a niche with a low redox potential consequently leading to a shift in the composition of the microflora favoring the growth of strictly anaerobic and capnophilic species. These bacteria may indirectly enhance the inflammatory process to a certain extent [12]. With continuing debate as to the role of plaque and gingival
inflammation in DIGO, there still remain a cohort of patients who develop over growth irrespective of their oral hygiene or periodontal condition [77]. In such patients, other risk factors may be more significant.
Various indices to score DIGOand their reliability:
A wide range of methods have been employed to determine the severity of GO. Most of these methods rely on descriptive scales that use subjective terms such as minimal, moderate and severe to define the various grades of gingival enlargement [78-82]. In spite of the ease in using
of such scales their lack of reproducibility and a non-continuous scale for subsequent statistical analysis makes them inefficient for large scale epidemiological studies (Table 3). Objective scales that relate the overgrowth tissue to tooth crown have also been proposed [83, 84] (Table
4).
Seymour proposed a method of measuring the GO using a stone model. The method assessed both horizontal and vertical components, focusing on the upper and lower anterior teeth (canine to canine), since the overgrowth is more likely to occur in these areas, and a cumulative percentage overgrowth score obtained (Table 5). The system recognizes the continuous nature of GO from the smallest (1%) to the largest (100%) change and thereby offers a degree of sensitivity not seen in conventional ordinal scales, (net grading) Patient with a GO score >30% were regarded as responders with clinically significant overgrowth, i.e. a level of overgrowth that warrants surgical intervention. Though this method has been used extensively it is time consuming, complicated and expensive [85].
Photographic methods have also been proposed to assess GO
[82]. Standardized photographic view of patient can be assessed against a
reference set of photographs that define various degree of overgrow th. Such photographic methods have high advantages for large-scale epidemiological studies as it does not require any special facilities other than the camera itself. Patient does not have to undergo any invasive procedures, such as impression taking. However such methods have a largely subjective component. To overcome such disadvantages Ellis et.al. proposed a photographic grading method using the assessment of vertical component described by Seymour et.al. This method also provides a continuous scale of gingival changes for subsequent statisti cal analysis [82].
But for a complete grading of the GO, plaque index, gingival index, periodontal probing depth and papillary bleeding index should also be considered. Few scales which include all these details were also suggested [12, 32].
Table No. 3: Harris and Ewart’s GO grading
Grade Clinical Features
0 No overgrowth.
1 Early changes detectable, without encroachment on the tooth.
2 Moderate changes with increased enlargement of the interdental papillae and slight encroachment of the gingival tissue onto the tooth surfaces. (Fig 1a, 2a)
3 Marked changes with obvious encroachment of the gingival tissues onto the tooth surface. (Fig 2b, 3a, 3b)
Table No. 4: Angelopoulous and Goaz index modified by Miller and Damm
Grade Clinical Features
0 Normal gingiva.
1 Minimal enlargement (≤ 2mm in size, with gingiva covering the cervical third or less of the anatomic crown).
2 Moderate enlargement (2 - 4 mm in size and/or gingiva extending into the middle third of the anatomic crown). (Fig 1a, 2a)
3 Severe enlargement (nodular growth > 4mm and/or gingiva covering more than two-thirds of the tooth crown). (Fig 2b, 3a, 3b,5a)
Table No. 5: GO grading by Seymour
Horizontal Component: Measure the degree of gingival thickening labially and lingually by means of a 3 point scale. 0 Normal width
1 Thickening upto 2mm 2 Thickening more than 2mm
Vertical Component: Extent of encroachment of the gingival tissues on the labial and lingual aspects of adjacent tooth surface from a gingival unit.
0 No encroachment of interdental papilla onto tooth surface.
1 Mild encroachment of interdental papilla, producing a blunted appearance to papilla tip.
2 Moderate encroachment, involving lateral spread of papilla across buccal tooth surface of less than one quarter tooth width. (Fig 1a, 2b)
3 Marked encroachment of papilla i.e. more than one fourth tooth width, loss of normal papilla form. (Fig 2b, 3a, 3b, 5a)
Histological features of NIGO:
A well explained histopathologic study of NIGO was performed using Beagle model [86]. Few human studies observed a slight
to moderate hyperkeratosis and a marked epithelial acantosis with elongation of rete peg into the lamina propria and thickening of spinous layer [24, 87]. The connective tissue exhibited fibrous hyperplasia with
dense collagen formation and fibrosis. An increase in the number of capillaries with a perivascular inflammatory cell infiltrate is noted, mainly of lymphocytes and plasma cells [1, 8, 16]. Microscopic examination
of the excised specimen in our patient demonstrated the overlying keratinized irregular, hyperplastic epithelium of variable thickness along with the elongation of rete ridges penetrating the connective tissue. A highly vascular thick proliferative fibrous connective tissue with focal accumulation of inflammatory cells was evident (Fig. 5b). Correlating histopathological findings with the clinical presentation it was suggestive of drug induced gingival enlargement.
Few authors claimed that there was an increase in acid mucopolysaccharide production and the number of cytoplasmic secretary granules was also elevated. However, further studies with considerable number of specimens in controlled populations are needed for an in detail histopathologic features.
Treatment:
Despite our greatest understanding of the various aspect of NIGO, its treatment still remains a challenge for the periodontist. Various treatment options had been critically reviewed by Ellis et.al [88].
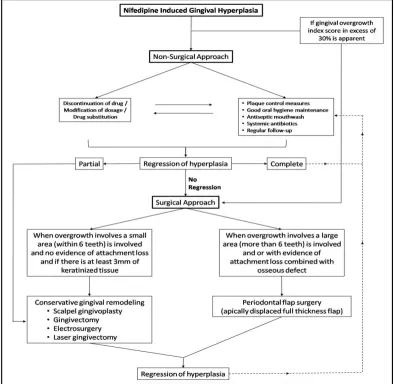
Treatment approach includes surgical and/or non-surgical options. Whenever it is possible, non-surgical treatment should always be adopted first, however, GO index scores suggested by Seymour can be extensively used to initiate the treatment. Researches have suggested surgical intervention is warranted when score in excess of 30% are apparent [89]. A concise model for treatment of NIGO has been
summarized in Fig. 9.
Non-Surgical approach:
The primary aim of non-surgical approach is to reduce the inflammatory component in the gingival tissues and to reduce or eliminate the concentration of the drug reaching the target tissues.
Drug discontinuation/substitution:
One obvious solution in the management of NIGO is to change the medication. Since nifedipine can be substituted by a greater range of alternative CCB which achieves the same therapeutic goals, drug substitution should always be considered as a management option. Prevalence and severity of overgrowth has been shown to be very different even with drugs of a similar chemical structure. For example, nifedipine and amlodipine, though share the same chemical structure, yet amlodipine has a prevalence of overgrowth of half that of nifedipine
[90]. Decrease in overgrowth has been reported after substitution with
verapamil and isradipine [23, 29].
However, drug substitution should only be considered for those patients where the new medication can offer some advantage for control of their hypertension and also in patients who present with clinically significant overgrowth and are at high risk from either corrective surgery or recurrence after gingivectomy [88]. Few studies
reported regression of overgrowth as early as one week after drug withdrawal [91].
Although such as change in medication may improve the gingival tissue, it does not necessarily lead to the complete resolution of overgrowth which may need corrective gingival remodeling along with oral hygiene maintenance. However, when drug substitution is considered the dentist must liaise with the patient’s physician to review their current medication. As the drugs have unwanted effect, the morbidity of GO needs to be compared with other possible unwanted effects arising from alternative medication [88].
Oral hygiene maintenance:
Controversy still exists regarding the nature of the relationship between plaque and expression of GO as to whether plaque accumulation is the cause of the gingival changes or the consequence of it. Individual case reports have shown that meticulous self-administered oral hygiene, alongside professionally delivered oral hygiene and scaling and root planning can result in complete resolution of overgrowth [92, 93].
Local environmental factors that enhance plaque accumulation such as faulty restorations, broken teeth or carious lesions should be eliminated and any fixed or removable prostheses should be designed to minimize plaque retention. Oral hygiene therapy, while of some benefit to few patients, failed to completely reduce the development of overgrowth [88].
Such patients may require other modalities of treatment.
Animal studies have shown that regular application of a chlorhexidine solution resulted in significantly less overgrowth than in control animals [94]. Short courses of azithromycin and metronidazole
have been evaluated in GO due to cyclosporine treatment and found to be beneficial in few patients [95]. Suggested mechanism include reduction
of concomitant bacterial infection and hence inflammation and also by increasing the phagocytic activity of gingival fibroblasts [96, 97]. However,
antibiotic supplement in NIGO and their effect is yet to be evaluated.
Surgical approach:
Scalpel gingivectomy:
Gingivectomy is regarded as the “standard treatment” for any DIGO [98]. The excess tissue is released by means of a long bevel incision
which should ideally allow the complete removal of pocket tissue as part of the excised tissue mass. However, peri-operative haemorrhage is the main disadvantage of scalpel excision due to highly vascularized and inflamed overgrown gingival tissues. Studies have evaluated the aesthetic outcomes of patients treated with flap surgery and gingivectomy and found that gingivectomy treated patients have a smoother gingival surface than that treated by a flap surgery [99].
Electrosurgery:
Electrosurgery techniques have been proposed by few authors [100]. Although such techniques possess advantage of adequate
haemostasis, they have disadvantage of causing a surrounding zone of thermal necrosis, which may impede wound healing [88]. However use of
Laser gingivectomy:
Lasers have remarkable cutting ability and they also generate a coagulated tissue layer along the surface of the laser incision which promotes healing [102]. Other advantages include a relative bloodless
operating field, greater accuracy in making incisions, sterilization of the operating field, minimal swelling and scarring and much less post operative pain [27, 88, 103]. In a split-mouth crossover design study, the
author compared laser to scalpel gingivectomy and demonstrated a significant lower rate of recurrence rate in laser gingivectomy over a six month follow-up period. However advantageous, laser treatment is expensive and long term benefits of laser gingivectomy need to be established [88].
Flap Surgery:
The periodontal flap is preferred when the GO involved more than six teeth and when there is evidence of attachment loss combined with osseous defect. Popora et. al. suggested an apically displaced full thickness flap which may possess the advantage to preserve the attached gingival [104]. This surgical approach is more suitable to eliminate
periodontal pocket, to improve the alveolar bone morphology and to improve the esthetics when moderate periodontitis with GO is treated.
Treatment outcomes and recurrent rate:
Though various treatment modalities have been suggested for DIGO, it should be emphasized that these treatment options do not necessarily prevent recurrence and patients should be made aware of this fact [6]. The recurrence rate of severe gingival enlargement in
nifedipine treated patients after surgical therapy was found to be about 40% within 18 months after active treatment [28]. One of our patient who
was treated by scalpel gingivectomy showed marked recurrence within 6 months of treatmen. (Fig. 5c).
Significant determinants of recurrence were found to be gingival inflammation and poor compliance with maintenance visits [105].
Vishaka et. al. recommend a repeated follow-up visit of a 3 month interval for periodontal maintenance therapy in patients taking drugs associated with gingival enlargement [8]. Each recall appointment should
include detailed oral hygiene instructions, complete periodontal prophylaxis and supra and sub-gingival calculus removal as needed [8].
For patients with severe GO and who require continuous drug therapy for various medical reasons, gingivectomy must be repeated periodically due to the recurrent nature of overgrowth [105, 106].
Fig. 9: A concise model for treatment of NIGO
CONCLUSION
It should be anticipated that DIGO will continue to be a predicament until safe and equally reliable medications are developed and fully utilized. With increasing geriatric community, the use of CCB with the potential to cause GO will increase. Prevention and treatment of this unnecessary side effect needs active participation from triads involved in its use; the physician, dental professional and the patient himself.
In view of the fact that the prescribed drug is the causative agent for GO the physicians should be able to identify the changes in oral cavity of their patients. Regrettably, most medical education curricula do
not include sufficient information to appreciate oral biology and oral pathology. Hence efforts to increase awareness about this condition within the medical community should continue to aid in early identification of patients susceptible to DIGO. It would also be obligatory that a physician should have a dental opinion before describing drugs that may induce GO.
and to carefully examine gingival tissue for enlargement or morphological alteration as an integral part of their comprehensive oral examination.
Patient’s compliance in maintaining good oral hygiene and adherence to regular follow-up is essential in successfully treating this condition. Thus there is a great need for physician, dental professional and the patient himself to work together in the care of DIGO.
REFERENCE:
1. Hassell TM, Hefti AF. Drug-induced gingival overgrowth: Old problem, new problem. Cri t. Rev. Oral. Biol. Med.,1991; 2(1): 103-37.
2. Triveni MG, Rudrakshi C, Mehta DS. Amlodipine-induced gingival overgrowth. J. Indian Soc. Periodontol., 2009; 13(3): 160-3.
3. Miranda J, Brunet L, Roset P, Berini L, Farré M, Mendieta C. Prevalence and risk of gingival enlargement in patients treated with nifedipine. J. Periodontol.,2001; 72(5): 605-11.
4. Lafzi A, Farahani RM, Shoja MA. Amlodipine-induced gingival hyperplasia. Med. Oral. Patol. Oral. Cir. Bucal., 2006; 11(6): E480-2.
5. Trackman PC, Kantarci A. Connective tissue metabolism and gingival overgrowth. Crit. Rev. Oral. Biol. Med.,2004; 15(3): 165-75.
6. Marshall RI, Bartold PM. A clinical review of drug-induced gingival overgrowth. Aust. Dent. J.,1999; 44(4): 219-32. 7. Rees TD, Levine RA. Systemic drugs as a risk factor for
periodontal disease initiation and progression. Compend. Contin. Educ. Dent.,1995; 16: 20-42.
8. Grover V, Kapoor A, Marya CM. Amlodipine induced gingival hyperplasia. J. Oral. Health Comm. Dent.,2007; 1(1): 19-22. 9. Lokkan P, Skomedal T. Gingival hyperplasia induced by calcium
channel blockers. Rare or frequent in Norway? Tidsskr. Nor. Laegeforen.,1992; 112: 1978-80.
10. Kimball O. The treatment of epilepsy with sodium dephenylhydantoinate. JAMA 1939; 112: 1244-45.
11. Glossmann H, Ferry D, Goll A, Striessnig J, Zernig G. Calcium Channels: introduction into the molecular pharmacology, in cardiovascular effects of dihyfropyridine-type calcium antagonists and agonists. Fleckenstein A, Van Breemen C, Gross R, Hoffmeister F. Eds., Springer Verlag, Berlin, 1985; 113. 12. Nakou M, Kamma JJ, Andronikaki A, Mitsis F. Subgingival
microflora associated with nifedipine-induced gingival overgrowth. J. Periodontol.,1998; 69(6): 664-9.
13. Silverstein LH, Koch JP, Lefkove MD, Garnick JJ, Singh B, Steflik DE. Nifedipine-induced gingival enlargement around dental implants: a clinical report. J Oral Implantol 1995;21(2):116-20. 14. Hallmon WW, Rossmann JA. The role of drugs in the
pathogenesis of gingival overgrowth, A collective review of current concepts. Periodontol 2000;21:176-96.
15. Lucas RM, Howell LP, Wall BA. Nifedipine-induced gingival hyperplasia:a histochemical and ultrastructural study. J Periodontol1985;56:211-215.
16. Naidoo LC, Stephen LX. Nifedipine-induced gingival hyperplasia: non-surgical management of a patient. Spec Care Dentist
1999;19(1):29-34.
17. Wynn RL. Calcium channel blockers and gingival hyperplasia.
Gen Dent1991;39:240-3.
18. Tagawa T, Nakamura H, Murata M. Marked gingival hyperplasia induced by nefedipine. Int J Oral Maxillofacial Surg1990 ;19:72-3.
19. Harel-Raviv M, Eckler M, Lalani K, Raviv E, Gornitsky M. Nifedipine-induced gingival hyperplasia a comprehensive review and analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1995;79(6):715-22.
20. Yusof WZW. Gingival hyperplasia: an intra-oral side effect of phenytoin, nifedipine and cyclosporine therapies. Sing Med J
1988;29:498-503.
21. Long TW. Nifedipine in: management of clinical prescription drugs. Philadelphia: Harper & Row, publishers 1964;590-5. 22. Ramon Y, Besar S, Kishon Y, Engelberg I. Gingival hyperplasia
caused by nifedipine-a preliminary report. Int J Cardiol
1984;5(2):195-206.
23. Lederman D, Lumerman H, Reuben S, Freedman P. Gingival hyperplasia associated with nifedipine therapy. Oral Surg
1984;57(6):620-2.
24. Van der Wall E, Tuinzing D, Hiss J. Gingival hyperplasia: a possible side effect of nifedipine. Ned Tijdschn Geneeskd
1984;128(41):1954-5.
25. Shaftic A, Widdup L, Abate M, Jacknowitz A. Nifedipine-induced gingival hyperplasia. Drug Intell Clin Pharm1986;20:602-5.
26. Slavin J, Taylor J. Cyclosporine, nifedipine, and gingival hyperplasia. Lancet1987;2(8561):739.
27. Barak S, Engelberg I, Hiss J. Gingival hyperplasia caused by nifedipine. Histopathologic findings. J periodontal1987 ;58:639-42.
28. Pradhan S, Mishra P, Joshi S. Drug induced gingival enlargement-a review. PGNM2009;8(2).
29. Westbrook P, Bednarczyk EM, Carlson M, Sheehan H, Bissada NF. Regression of nifedipine-induced gingival hyperplasia following switch to a same class calcium channel blocker, isradipine. J Periodontol 1997;68(7):645-50.
30. Panahi O, Melody FR, Kennet P, Tamson MK. Drug induced (calcium channel blockers) gingival hyperplasia. JMBS
2011;2(1):10-2.
31. Shouda J, Nakamoto H, Sugahara S, Okada H, Suzuki H. Incidence of gingival hyperplasia caused by calcium antagonists in continuous ambulatory peritoneal dialysis patients. Adv Perit Dial1999;15:153-5.
32. Ellis JS, Seymour RA, Steele JG, Robertson P, Butler TJ, Thomason JM. Prevalence of gingival overgrowth induced by cal cium channel blockers: a community-based study. J Periodontol
1999;70(1):63-7.
33. Chee WW, Jansen CE. Phenytoin hyperplasia occurring in relation to titanium implants: a clinical report. Int J Oral Maxillofac Implants1994;9:107-109.
34. Nery EB, Edson RG, Lee KK, Pruthi VK, Watson J. Prevalence of nifedipine-induced gingival hyperplasia. J Periodontal
1995;66(7):572-8.
35. Missouris GG, Kalaitzidis RG, Cappuccio FP, MacGregor GA. Gingival hyperplasia caused by calcium channel blockers. J Hum Hypertens2000;14(2):155-6.
36. Carranza FA. Gingival enlargement. In: Carranza FA, ed. Glickman’s Clinical Periodontology. Philadelphia: W.B. Sanders Co.; 1990:125-148.
37. Fu E, Nieh S, Wikesjo UME, Fu-Gong L, Shen EC. Gingival overgrowth and dental alveolar alterations: possible mechanisms of cyclosporine-induced tooth migration. An experimental study in the rat. J Periodontol 1997;68:1231-6. 38. Hassell TM, Cooper GC. Phenytoin-induced gingival overgrowth
in mongrel cat model. In phenytoin-induced teratology and gingival pathology (Eds Hassell TM, Johnson MC, Dudley KH). Pp. 147-162. Raven Press, New York.
39. Barclay S, Thomason JM, Idle JR, Seymour RA. The incidence and severity of nifedipine-induced gingival overgrowth. J Clin Periodontol 1992;19(5):311-4.
40. Fujii A, Matsumoto H, Nakao S, Teshigawara H, Akimoto Y. Effect of calcium-channel blockers on cell proliferation, DNA synthesis and collagen synthesis of cultured gingival fibroblasts derived from human nifedipine responders and non-responders. Arch Oral Biol 1994;39(2):99-104.
41. Vogel RI. Gingival hyperplasia and folic acid deficiency from anticonvulsive drug therapy; a theoretical relationship. J Theor Biol 1977;67:269-78.
42. Brunet L, Miranda J, Farre M, Berini L, Mendieta C. Gingival enlargement induced by drugs. Drug Saf1996;15:219-31. 43. Brown RS, Beaver WT, Bottomley WK. On the mechanism of
drug-induced gingival hyperplasia. J Oral Pathol Med
1991;20:201-9.
44. Sooriyamoorthy M, Gower DB, Elay BM. Androgen metabolism in gingival hyperplasia induced by nifedipine and cyclosporine. J Periodontal Res1990;25:25-30.
45. Seymour RA, Ellis JS, Thomason JM. Risk factors for drug-induced gingival overgrowth. J Clin Periodontol2000 ;27(4):217-23.
46. Daley TD, Wysocki GP, Day C. Clinical and pharmacologic correlations in cyclosporine-induced gingival hyperplasia. Oral Surg Oral Med Oral Pathol1986;62(4):417-21.
47. McGaw T, Lam S, Coates J. Cyclosporin-induced gingival overgrowth: correlation with dental plaque scores, gingival scores, and cyclosporine levels in serum and saliva. Oral Surg Oral Med Oral Pathol1987;64(3):293-7.
48. Pernu HE, Pernu LMH, Huttunen KRH, Nieminen PA, Knuuttila MLE. Gingival overgrowth among renal transplant recipients related to immunosuppressive medication and possible local background factors. J Periodontol 1992;63(6):548-53.
50. Thomason JM, Seymour RA, Rice N. The prevalence and severity of cyclosporine and nifedipine-induced gingival overgrowth. J Clin Periodontol1993;20:37-40.
51. Bullon P, Machuca G, Martinez-Sahuquillo A, Rios JV, Rojas L, Lacalle JR. Clinical assessment of gingival hyperplasia in patients treated with nifedipine. J Clin Periodontol1994;21:256-9. 52. Somacarrera ML, Herandez G, Acero J, Moskow BS. Localisation
of gingival overgrowth in heart transplant patients undergoing cyclosporine therapy. J Periodontol1994;65:666-70.
53. Seymour RA, Thomason JM, Ellis JS. The pathogenesis of drug-induced gingival overgrowth. J Clin Periodontol1996;23:165-75. 54. Dahllof G, Otteskog P, Modeer T. Phenytoin potentiates accessory cell dependent DNA synthesis in human lymphocytes in vitro. Scand J Dent Res1986;94(3):202-7.
55. Kinane DF, Drummond JR, Chisholm DM. Langerhans cells in human chronic gingivitis and phenytoin-induced gingival hyperplasia. Arch Oral Biol1990;35(7):561-4.
56. Walsh LJ, Seymour GJ, Powell RN. The regulation of Langerhans cell T6. DR and DQ antigen expression: an hypothesis. J Oral Pathol 1988;17(1):43-6.
57. Modeer T, Andersson G. Regulation of epidermal growth factor receptor metabolism in gingival fibroblasts by phenytoin in vitro. J Oral Pathol Med1990;19(4):188-91.
58. Dill RE, Miller EK, Weil T, Lesley S, Farmer GR, Lacopino AM. Phenytoin increases gene expression for platelet-derived growth factor B chain in macrophages and monocytes. J Periodontol
1993;64(3):169-73.
59. Das SJ, Olsen I. Keratinocyte growth factor is upregulated by the hyperplasia-inducing drug nifedipine. Cytokine
2000;12(10):1566-9.
60. Seymour RA. Effects of medications on the periodontal tissues in health and disease. Periodontol 20002006;40:120-9.
61. Thomason JM, Seymour SA, Ellis JA, Kelly PJ, Parry G, Dark J et al., Iatrogenic gingival overgrowth in cardiac transplantation. J Periodontol1995;66(8):742-6.
62. James JA, Marley JJ, Jamal S, Campbell BA, Short CD, Johnson RW, et al., The calcium channel blocker used with cyclosporine has an effect on gingival overgrowth. J Clin Periodontol
2000;27(2):109-115.
63. Sokolow M, Mcllroy MB. Clinical Cardiology, 4th ed. Los Altos, CA:
Lange Medical Publishers; 1986:132-196.
64. Nishikawa S, Nagata T, Morisaki I, Oka T, Ishida H. Pathogenesis of drug-induced gingival overgrowth. A review of studies in the rat model. J Periodontol1996;67(5):463-71.
65. Ishida H, Kondoh T, Kataoka M, Nishikawa S, Nakagawa T, Morisaki I, et al., Factors influencing nifedipine-induced gingival overgrowth in rats. J Periodontol1995;66(5):345-50.
66. Kantor ML, Hassell TM. Increased accumulation of sulfated glycosaminoglycans in cultures of human fibroblasts from phenytoin-induced gingival overgrowth. J Dent Res
1983;62:383-7.
67. Seymour RA, Heasman PA. Drugs and the periodontium. J Clin Periodontol1988;15(1):1-16.
68. Seymour RA, Jacobs DJ. Cyclosporin and gingival tissues. J Clin Periodontol1992;19(1):1-11.
69. Laison PA. Gingival overgrowth in a patient treated with nifedipine (Procardia). Periodontol Case Reports1986;8:64-6. 70. Ellis JS, Seymour RA, Monkman SC, Idle JR. Gingival
sequestration of nifedipine in nifedipine-induced gingival overgrowth. Lancet1992;339(8806):1382-3.
71. Bokenkamp A, Bohnhorst B, Beier C, Albers N, Offner G, Brodehl J. Nifedipine aggravates cyclosporine A-induced gingival hyperplasia. Pediatr Nephrol1994;8(2):181-5.
72. Margiotta V, Pizzo I, Pizzo G, Barbaro A. Cyclosporin and nifedipine-induced gingival overgrowth in renal transplant patients: correlations with periodontal and pharmacological parameters and HLA-antigens. J Oral Pathol Med1996 ;25:128-34.
73. O’Valle F, Mesa F, Aneiros J, Gomez-Morales M, Lucena MA, Ramirez C, et al., Gingival overgrowth induced by nifedipine and cyclosporine A. Clinical and morphometric study with image analysis. J Clin Periodontol1995;22:591-7.
74. Wilson RF, Morel A, Smith D, Koffman CG, Ogg CS, Rigden SP, et al., Contribution of individual drugs to gingival overgrowth in adult and juvenile renal transplant patients treated with multiple therapy. J Clin Periodontol1998;25:457-64.
75. Wondimu B, Sandberg J, Modeer T. Gingival overgrowth in renal transplant patients administered cyclosporine A in mixture or in capsule form. A longitudinal study. Clin Transplant1996 ;10:71-6.
76. Sousa CP, Navarro CM, Sposto MR. Clinical assessment of nifedipine-induced gingival overgrowth in a group of Brazilian patients. ISRN Dent 2011;2011:102047.
77. Seymour RA, Smith DG. The effect of a plaque control programme on the incidence and severity of cyclosporine-induced gingival changes. J Clin Periodontol1991;18:107-10. 78. Frankel SI. Dilantin sodium in the treatment of epilepsy. JAMA
1940;114:1320-1.
79. Harris TH, Ewart JR. Complications following the use of sodium diphenylhydantoinate (Dilantin) therapy. Journal of the Oklahoma Medical Association1942;35:365-70.
80. Addy V, McElnay J, Eyre D, Campbell N, D’Arcy P. Risk factors in phenytoin-induced gingival overgrowth. J Periodontol
1983;54:373-77.
81. Babcock JR. Incidence of gingival hyperplasia associated with dilantin therapy in a hospital population. JADA1965 ;71:1447-50.
82. Ellis JS, Seymour RA, Robertson P, Butler TJ,Thomason JM. Photographic scoring of gingival overgrowth. J Clin Periodontol
2001;28:81-5.
83. Angelopoulos AP, Goaz PW. Incidence of diphenylhydantoin hyperplasia. Oral Surg Oral Med Oral Pathol1972;34:898-906. 84. Miller CS, Damm DD. Incidence of Verapamil-induced gingival
hyperplasia in a dental population. J Periodontol 1992;63:453-6. 85. Seymour RA, Smith DG, Turnbull DN. The effects of phenytoin and sodium valporate on the periodontal health of adult epileptic patients. J Clin Periodontol 1985;12:413-9.
86. Heijl L, Sundin Y. Nitrendipine-induced gingival overgrowth in dogs. J Dent Res1987;66:282.
87. Van der Wall EE, Tuinzing DB, Hes J. Gingival hyperplasia induced by nifedipine, an arterial vasodilating drug. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1985;60:38-40. 88. Mavrogiannis M, Ellis JS, Thomason JM, Seymour RA. The
management of drug-induced gingival overgrowth. J Clin Periodontol 2006;33:434-9.
89. Thomason JM, Seymour RA. Phenytoin-induced gingival overgrowth in general medical practice. J Dent Res 1990;69:969. 90. Ellis JS, Seymour RA, Taylor JJ, Thomason JM. Prevalence of gingival overgrowth in transplant patients immunospressed with tacrolimus. J Clin Periodontol2004;31:126-31.
91. Raman PG, Mishra VN, Singh D. Nifedipine induced gingival hyperplasia. J Assoc Physicians India1988;36:231-3.
92. Clantar M. Nifedipine-induced gingival overgrowth: remission following non-surgical therapy. Dent Update1996;23:374-7. 93. Hancock RH, Swan RH. Nifedipine-induced gingival overgrowth.
Report of a case treated by controlling plaque. J Clin Periodontol
1992;19:12-4.
94. Pillati GL, Sampaio JE. The influence of chlorhexidine on the severity of cyclosporine A-induced gingival overgrowth. J Periodontol 1997;68:900-4.
95. Glaude R, Snyder ME. Intracellular accumulation of azithromycin by cultured human fibroblasts. Antimicrob Agents Chemother
1990;34:1056-1060.
96. Mesa FL, Osuna A, Aneiros J, Gonzalez-Jaranay M, Bravo J, Junco P, et al., Antibioti c treatment of incipient drug-induced gingival overgrowth in adult renal transplant patients. J Periodontol Res
2003;38:141-6.
97. Paik JW, Kim CS, Cho KS, Chai JK, Kim CK, Choi SH. Inhibition of cyclosporine A-induced gingival overgrowth by azithromycin through phagocytosis: an in vivo and in vitro study. J Periodontol
2004;75:380-7.
98. Thompson EC, Gillespie JB. Hyperplasia of the gums following Dilantin therapy, with gingivectomy for correction. JADA
1941;28:1613-5.
99. Pilloni A, Camargo PM, Carere M, Carranza FA Jr. Surgical treatment of cyclosporine A and nifedipine-induced gingival enlargement: gingivectomy versus periodontal flap. J Periodontol
1998;69:791-7.
100.Liboon J, Funkhouser W, Terri s DJ. A comparison of mucosal incisions made by scalpel, CO2 laser, electrocautery and constant-voltage electrocautery. Otolaryng Head Neck
1997;116:379-85.
101.Wlaker C Jr, Tomich CE, Hutton CE. Treatment of phenytoin-induced gingival hyperplasia by electrosurgery. J Oral Surg
1980;38:306-11.
102.Goharkhay K, Mori tz A, Wilder-Smith P, Schoop U, Kluger W, Jakolitsch S, Sperr W. Effects on oral soft tissue produced by a diode laser in vitro. Laser Surg Med1999;25:401-6.