ARTICLE
Maternal Psychological Adjustment and Knowledge
of Infant Development as Predictors of Home Safety
Practices in Rural Low-Income Communities
Adam J. Zolotor, MD, MPHa,b, Margaret Burchinal, PhDc,d, Debra Skinner, PhDc,e, Marjorie Rosenthal, MD, MPHf,g, and the Key Family Life Project Investigators
aDepartment of Family Medicine,bInjury Prevention Research Center,cFrank Porter Graham Child Development Institute, andeDepartment of Anthropology, University
of North Carolina, Chapel Hill, North Carolina;dDepartment of Education, University of California, Irvine, California;fDepartment of Pediatrics andgRobert Wood Johnson
Clinical Scholars Program, Yale University, New Haven, Connecticut
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
Maternal psychological adjustment and understanding of child development are thought to influence implementation of safety practices; however, the extent to which either factor is related has been examined with small samples and without attention to potentially confounding variables.
What This Study Adds
Maternal psychological symptoms are strongly associated with the use of all types of home safety practices, and knowledge of development is only associated with imple-mentation of practices requiring installation. This study demonstrates high rates of im-plementation and barriers to imim-plementation.
ABSTRACT
BACKGROUND.Unintentional injury is the leading cause of death among toddlers in the United States. Toddlers spend the majority of time at home, and the use of recom-mended safety practices can prevent many injuries.
OBJECTIVE.Maternal psychological adjustment and understanding of child development are thought to influence the implementation of safety practices; however, the extent to which either factor is related has been examined with small samples and without attention to potential confounding. We hypothesize that mothers’ use of safety practices will be higher when mothers have more knowledge of development and better psychological adjustment.
METHODS.This study is part of the Family Life Project, a longitudinal birth cohort of children from poor rural communities (n⫽1611) and an ethnographic sample (n⫽
36). Mothers in the birth cohort completed scales to measure knowledge of devel-opment, psychological adjustment, and home safety practices. Factor analysis of the safety scale resulted in 4 subscales. Each subscale was predicted from maternal knowledge and adjustment in multivariable regression. Mothers in the ethnographic study described sources of information about home safety, current practices, and barriers.
RESULTS.Analyses indicated that mothers with better psychological adjustment were more likely to implement all of the safety practices, and mothers with more knowl-edge about development were more likely to minimize subtle hazards and install
safety devices. An interaction between maternal adjustment and knowledge suggested that mothers with psycho-logical distress were more likely to install safety devices if they had greater knowledge of development. Mothers reported that health care providers were the primary source of safety information, and barriers to implementation included poverty and lack of stable housing.
CONCLUSIONS.Knowledge of development and better psychological adjustment are associated with improved home safety. Knowledge about development is especially important for mothers with poor mental health. Pediatricians and designers of injury-prevention programs should consider the role of maternal mental health in child safety.Pediatrics
2008;121:e1668–e1675
A
CCOUNTING FOR 43.3%of deaths, unintentional injury is the leading cause of death among children in the United States. Moreover, 20.6 million children each year sustain nonfatal injuries requiring medical attention or limiting activities.1Risk factors for childhood injury include poverty,2,3male gender,2,4child age,5child activity level,2,5single-parent household,6maternal mental health symptoms,7–9and parental alcohol abuse.10
The Consumer Product Safety Commission and the American Academy of Pediatrics advocate that the imple-mentation of home safety practices may prevent injury.11–13Rivara14 describes how home safety practices function
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-1255
doi:10.1542/peds.2007-1255
Key Words
home safety, injury, maternal knowledge and practice, maternal mental health
Abbreviations
FLP—Family Life Project
RKKSS—Russell Keeping Kids Safe Scale KIDI—Knowledge of Infant Development Instrument
BSI—Brief Symptom Index-18 GSI—Global Severity Index IBR—Infant Behavior Record Accepted for publication Nov 28, 2007
Address correspondence to Adam J. Zolotor, MD, MPH, University of North Carolina, CB 7595, Chapel Hill, NC 27599-7595. E-mail: [email protected]
best if they are inexpensive, widely available, easy to understand, well accepted, reliable, and independent of the need for vigilance. Home safety practices, however, are used at low rates.15–19
Previous studies have shown that the use of home safety practices is increased for parents with greater knowledge of child development and decreased for par-ents with increased psychological symptoms.4,8–10
Al-though suggestive, these studies were limited by small sample sizes, lack of representative sampling, and failure to adjust for potential confounding demographic, family, and child factors.20
This study uses data from an ongoing longitudinal study of infants in low-income rural communities that includes both a large birth cohort and a smaller ethno-graphic sample. Our primary aim was to determine whether parents who demonstrate better psychological adjustment or knowledge of infant development report higher rates of home safety practices, controlling for documented risk factors for injury. Our secondary aim was to determine how frequently mothers report using these safety practices, their primary sources of informa-tion, and perceived barriers to implantation.
METHODS
The Family Life Project (FLP) was designed as a mixed-method, longitudinal study of families living in 2 US rural areas with high rates of child poverty. Eastern North Carolina and central Pennsylvania were selected to represent the black South and Appalachia regions. A stratified sample was used to oversample low-income families in both states and black families in North Caro-lina.21
FLP recruiters identified 5471 women who gave birth between September 2004 and August 2005, 72% of whom were eligible because they spoke English and planned to live in the state for 2 years. Of those eligible, 68% were willing to participate, of whom 58% were randomly sampled for recruitment. Of those invited to participate, 82% completed their first home visit and were considered enrolled. At each subsequent home visit, the primary caregiver of the selected child was identified for interviews (2, 6, 15, 24, and 36 months). The current study uses data from the 2-, 6-, and 15-month interviews. This is the period of development most critical for implementing home safety practices in-cluded in this study.22
The FLP includes an ethnographic component to pro-vide another methodologic perspective on the meaning and context of parent beliefs and practices.23A separate
sample of 36 families in North Carolina was selected for the ethnographic study. These families resided in the same counties as the birth cohort and were similar in terms of poverty status and race. Pregnant women were recruited between February 2003 and February 2004 from health departments, parenting classes, a home health agency, clinics, and health fairs. Mothers were interviewed on a variety of topics related to parenting practices and child development every 6 to 8 weeks beginning prenatally and continuing for 2 years with 2
follow-up interviews conducted in the third year for an average of 17 to 18 interviews per mother.
Measures
Structured interviews were conducted at enrollment, at 6 months, and at 15 months. Home visits lasted 2 to 3 hours and included mother and child observations, child-based tasks, and structured questionnaires. At the North Carolina site, the ethnographic sample partici-pated in a semistructured interview to provide more in-depth information on the mothers’ knowledge of and barriers to implementing safety practices. The structured interview was not administered to these mothers.
The primary dependent variable of interest in this study is the use of home safety measures. These were assessed by interview of the primary caregiver at the 15-month visit. The Russell Keeping Kids Safe Scale (RKKSS) is an obser-vational checklist,24which we adapted for maternal
self-report. This instrument includes questions about use of 24 common home safety measures, such as electrical socket covers. Mothers responded using a 5-point scale, reporting whether they do these activities never, hardly ever, half the time, most of the time, and all of the time. This scale has not been used previously with self-report; however, a sim-ilar home safety checklist has been validated by comparing maternal self-report with observed implementation.25We
used maternal self-report to minimize the length of the home interview.
Knowledge of infant development was measured at the 2-month visit using an abbreviated version of the Knowledge of Infant Development Inventory (KIDI), a 20-item scale designed to assess adults’ knowledge of typical child development and parenting of children from birth to 2 years, including statements such as, “Infants do some things just to make trouble for their parents like crying a long time or pooping in their dia-pers (agree, disagree, not sure).”26In this study, we used
the number of correct answers divided by 20, resulting in a continuous proportion (0 –1). This summary score showed moderate reliability with, an␣of .63.
The Brief Symptom Inventory-18 (BSI)27 was filled
out by the primary caregiver at the 6-month visit. This is a short, sensitive, self-report index for psychological dis-tress. The BSI contains 18 items that are divided evenly across 3 dimensions: somatization, depression, and anx-iety. A total score, referred to as the Global Severity Index (GSI), was computed from the 3 dimensions and converted to atscore. Within this sample, the GSI had an excellent reliability (␣⫽.91), and scores ranged from 33 to 81, with higher scores representing more psycho-logical symptoms.27
At the 6-month interview, primary caregivers were asked to report demographic information, education, race, ethnicity, and an inventory of people in the home. At each visit, primary and secondary caregivers were asked about household income. This was divided by the federal poverty level to calculate a ratio of income to need.
After the 15-month visits, an adaptation of the Infant Behavior Record (IBR)28 was completed by both home
used to study children during administration of various cognitive and developmental tests.29 In the present
study, the IBR was applied to behavior observed during the entire visit.28,29 Two interviewers rated gross body
movements on a 9-point scale between 1 (“stays quietly in one place, with practically no self-initiated move-ment”) and 9 (“hyperactive; cannot be quieted for sed-entary tests”). Mean scores of the 2 observers were cal-culated.
Analytic Methods
Analyses of the cohort sample data were conducted by using Stata 8.2 (Stata Corp, College Station, TX), and survey weights were applied to adjust for oversampling of low-income families in both sites and for black fami-lies in North Carolina. The use of survey weights calcu-lated based on census date for race and income allows for the calculation of population-based estimates of ef-fect representing rural areas of Pennsylvania and North Carolina with concentrated child poverty. Descriptive statistics were calculated according to region to facilitate comparisons.
To identify underlying constructs and to reduce the number of dependent variables from the RKKSS home safety questionnaire, we used a factor analysis with va-rimax rotation. Four factors emerged based on loadings with eigenvalues ⬎1. A new variable was created for each factor by calculating a mean of the items loading on that factor.
The home safety scale scores were correlated with the ratings of maternal adjustment, knowledge of develop-ment, and child and family characteristics. We then used regression to predict home safety total and scale scores from maternal psychological adjustment and knowledge of development, with all of the covariates included as potential confounders resulting in 5 main-effects mod-els. A second step assessed the interaction between ad-justment and knowledge development for the home safety total and scale scores, resulting in 5 additional regression models.
Analysis of the ethnographic data entailed content analysis of the transcriptions, aided by reduction and display of data in matrices that summarized relevant information for each family. These approaches are widely used and well established in qualitative social science research,30–32providing systematic procedures for
extraction, reduction, and comparison of textual data. Two researchers, including the third author, indepen-dently read all of the transcripts and summarized in a data display matrix information about mothers’ safety beliefs and practices, barriers to implementing safety practices, and sources of safety information. They then examined these categories across respondents to deter-mine the range of responses and predominant themes related to each topic.
RESULTS
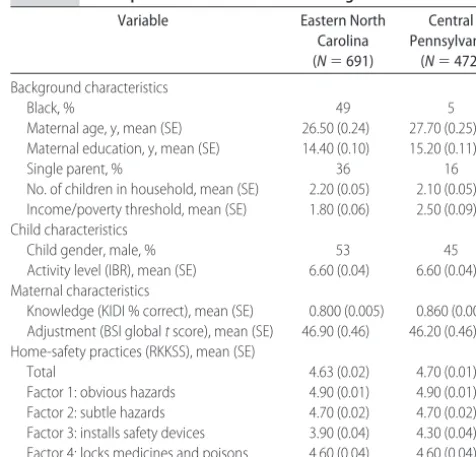
Descriptive statistics for the birth cohort sample are shown in Table 1. Almost half (49%) of the North Caro-lina sample but only 5% of the Pennsylvania sample was
black. The mean maternal age was 27 years. Most moth-ers (64% North Carolina and 84% Pennsylvania) re-ported a partner or husband in the home. The average number of children in subject households was just over 2 years. Half of the index children selected for the study were boys. The average maternal mental health symp-toms on the BSI was similar (meantscore: 47), suggest-ing that most mothers were not reportsuggest-ing high levels of distress (t score: ⬎60). The average infant gross motor activity score suggested that most infants were not viewed as hyperactive.
Analysis of both the birth cohort data and the ethno-graphic sample indicated that most mothers reported high levels of implementation of home safety practices. In the birth cohort, the RKKSS mean score was high in both sites (4.6 in North Carolina and 4.7 in Pennsylvania of a possible 5). Ethnographic findings also indicated a high implementation of home safety practices. Mothers expressed an awareness of hazards in the household and identified a range of practices that they implemented to safeguard their children. Constant and close supervision was most noted, followed by moving dangerous items out of reach and child-proofing the house with outlet covers, safety gates, and locks.
The ethnographic data revealed that mothers re-ported learning about safety practices primarily through their health care providers and yielded insights into bar-riers to implementation. Mothers said that at every visit their health care providers gave written information and verbal advice on practices such as infant-proofing the house, monitoring the child, and installing smoke detec-tors. Reasons given in the ethnographic interviews for not implementing safety features included: (1) living in someone else’s home and not being able to alter the environment; (2) being without a job and not having the money to buy devices; and (3) believing that the child
TABLE 1 Descriptive Statistics of Each Rural Region
Variable Eastern North Carolina (N⫽691)
Central Pennsylvania
(N⫽472)
Background characteristics
Black, % 49 5
Maternal age, y, mean (SE) 26.50 (0.24) 27.70 (0.25) Maternal education, y, mean (SE) 14.40 (0.10) 15.20 (0.11)
Single parent, % 36 16
No. of children in household, mean (SE) 2.20 (0.05) 2.10 (0.05) Income/poverty threshold, mean (SE) 1.80 (0.06) 2.50 (0.09) Child characteristics
Child gender, male, % 53 45
Activity level (IBR), mean (SE) 6.60 (0.04) 6.60 (0.04) Maternal characteristics
Knowledge (KIDI % correct), mean (SE) 0.800 (0.005) 0.860 (0.005) Adjustment (BSI globaltscore), mean (SE) 46.90 (0.46) 46.20 (0.46) Home-safety practices (RKKSS), mean (SE)
Total 4.63 (0.02) 4.70 (0.01)
would quickly learn how to outmaneuver safety devices so there was little use installing them.
Factor analysis of the RKKSS safety items from the birth cohort yielded 4 factor results: (1) a factor for minimizing obvious hazards (medicines, bags, and poi-sons) with 9 items (␣⫽.81); (2) a factor representing minimizing subtle hazards (tripping, entrapment, and falling) with 9 items (␣⫽.74); (3) a factor representing the use of safety items that require purchase and instal-lation (socket covers, gates, and cabinet locks) with 4 items (␣ ⫽.68); and (4) a factor representing keeping hazards locked up with 2 items (␣⫽.72). See Table 2 for a description of items loading on each factor.
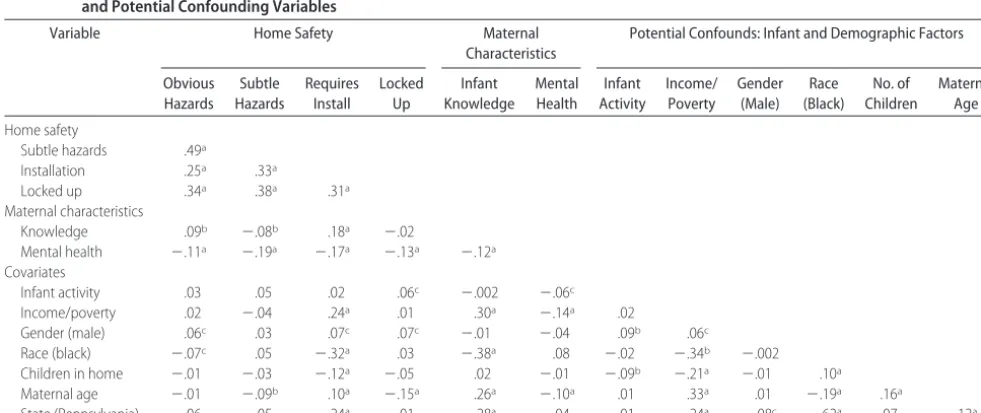
The correlations in Table 3 show the associations between home safety total and factor scores with se-lected predictors. Mothers reporting more psychological distress reported implementing fewer safety practices. Mothers with more knowledge about development re-ported adopting more home safety practices on the total score and on the factors representing minimizing
obvi-ous hazards and installing safety equipment. In contrast, knowledge was negatively correlated with reducing sub-tle hazards. The covariates showed expected associa-tions: higher income was related to installing safety equipment; mothers of boys were more likely to report minimizing obvious hazards, installing safety equip-ment, and locking up hazards; older and white mothers were more likely to report installing safety devices and minimizing subtle hazards; and mothers with more ac-tive infants were more likely to report locking up hazards.
Regression analyses of the birth cohort data indicated that maternal psychological adjustment was related to all of the types of safety practices, and knowledge of devel-opment was related to installation of safety equipment and minimizing subtle hazards (Table 4). Maternal dis-tress was negatively related to all of the safety practices as expected, and knowledge of infant development was positively associated with installation of safety equip-ment as expected ( ⫽ .57; P ⬍ .05), and negatively
TABLE 2 Specific Items Related to Each Factor of the RKKSS
Factor 1: Minimize Obvious Hazards
Factor 2: Minimize Subtle Hazards
Factor 3: Requires Install Factor 4: Hazards Locked Up
␣⫽.81 ␣⫽.74 ␣⫽.68 ␣⫽.72
Keep bags away Water containers out of reach Safety plugs in outlets Keep medicines locked in cabinet Keep sharp objects away Cords out of reach Install toddler safety gate Cleaning products locked up Store products in original containers Head trap items out of reach Install cabinet locks
Safety caps on medicines Breakable objects out of reach Keep plate cover over outlets Matches and lighters away Keep child from falling in tub
Cooking handles out of reach Stairs free of clutter Heat appliances out of reach Floors free of clutter Keep cords in good condition Floors free of loose rugs Firearms out of reach Hygiene products our of reach
␣⫽Cronbach’s alpha.
TABLE 3 Correlations Between Total and Factor Scores for the Implementation of Home Safety Practices, Knowledge of Infant Development, and Potential Confounding Variables
Variable Home Safety Maternal
Characteristics
Potential Confounds: Infant and Demographic Factors
Obvious Hazards
Subtle Hazards
Requires Install
Locked Up
Infant Knowledge
Mental Health
Infant Activity
Income/ Poverty
Gender (Male)
Race (Black)
No. of Children
Maternal Age
Home safety
Subtle hazards .49a
Installation .25a .33a
Locked up .34a .38a .31a
Maternal characteristics
Knowledge .09b ⫺.08b .18a ⫺.02
Mental health ⫺.11a ⫺.19a ⫺.17a ⫺.13a ⫺.12a
Covariates
Infant activity .03 .05 .02 .06c ⫺.002 ⫺.06c
Income/poverty .02 ⫺.04 .24a .01 .30a ⫺.14a .02
Gender (male) .06c .03 .07c .07c ⫺.01 ⫺.04 .09b .06c
Race (black) ⫺.07c .05 ⫺.32a .03 ⫺.38a .08 ⫺.02 ⫺.34b ⫺.002
Children in home ⫺.01 ⫺.03 ⫺.12a ⫺.05 .02 ⫺.01 ⫺.09b ⫺.21a ⫺.01 .10a
Maternal age ⫺.01 ⫺.09b .10a ⫺.15a .26a ⫺.10a .01 .33a .01 ⫺.19a .16a
State (Pennsylvania) .06 ⫺.05 .24a ⫺.01 .28a ⫺.04 .01 .24a .08c ⫺.62a .07 .12a aPvalue is⬍.001.
associated with minimizing subtle hazards ( ⫽ ⫺.23;
P⬍.05). In addition, poverty, black race, and number of children in the household were modest negative predic-tors of installing safety devices; infant activity level was a positive predictor of 2 of the summary scores; and maternal age was a negative predictor of 3 summary scores.
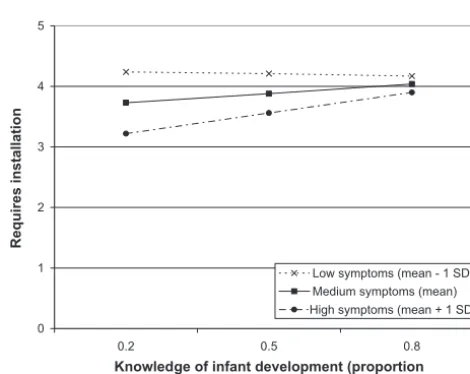
In addition, we tested whether knowledge about de-velopment moderated the association between maternal adjustment and home safety practices. The interaction term significantly contributed to predicting installation of safety devices ( ⫽ .06; P ⫽ .005). The interaction term was not significant in any other model and was, therefore, dropped from the models, as shown. Further-more, for ease of interpretation, the simple model with-out the interaction term is shown for the regression predicting installation of safety devices. The interaction indicated that knowledge of development was a strong predictor of installing safety devices among mothers with more psychological distress but not among less distressed mothers. The interaction is graphically repre-sented in Fig 1 by estimating the predicted regression line for mothers whose psychological adjustment scores were low (1 SD below the mean), average (at the mean), and high (1 SD above the mean). Figure 1 demonstrates that knowledge of development is important in predict-ing the use of safety practices requirpredict-ing installation among respondents with high mental health symptoms but not for mothers with average or fewer mental health symptoms. Two mothers from the ethnographic sample illustrate these relationships (see Appendix). Both had significant mental health symptoms. The mother in case 1 had inappropriate expectations of her toddler’s devel-opment and failed to implement safety measures. In case 2, the mother had depression, but with appropriate ed-ucation about development from her child’s doctor and an early childhood education program, she successfully implemented home safety practices.
DISCUSSION
This study demonstrates that parents of young children in rural, low-income areas in the Appalachian region in Pennsylvania and eastern North Carolina report high implementation of recommended home safety practices. In the ethnographic study, pediatricians were reported as the primary source of information regarding these practices, but mothers reported that they were less likely to implement these recommended practices when they were unemployed, lived in someone else’s home, or believed that their child would quickly learn how to get around them. Implementation of all types of home safety practices was more common when mothers re-ported better psychological adjustment. Installation of devices was more common for mothers with more
0 1 2 3 4 5
8 . 0 5
. 0 2
. 0
Knowledge of infant development (proportion correct)
Requires installation
Low symptoms (mean - 1 SD) Medium symptoms (mean) High symptoms (mean + 1 SD)
FIGURE 1
Association between maternal knowledge of infant development and implementation of home safety practices that require installation for mothers who report low, medium, and high levels of psychological symptoms (predicted regression lines at GSI mean:⫺2 SDs⫽2 SDs).
TABLE 4 Survey Weighted Linear Regression Models Predicting Home Safety Practices From Maternal Knowledge and Psychological Adjustment (nⴝ1083)
Variable Home Safety Total Obvious Hazards Subtle Hazards Safety Devices Installed
Poisons Locked Up
 SE  SE  SE  SE  SE
Maternal characteristics
Knowledge .08 0.11 .22 0.15 ⫺.23a 0.11 .57a 0.27 ⫺.097 0.27
Mental health ⫺.01b 0.001 ⫺.002a 0.001 ⫺.01b 0.001 ⫺.01b 0.003 ⫺.01c 0.003
Covariates
Pennsylvania .02 0.03 .01 0.02 ⫺.01 0.03 .11 0.07 .005 0.07
Income/poverty .01 0.01 ⫺.002 0.005 ⫺.001 0.01 .04c 0.01 .02 0.01
Child gender .05a 0.02 .03 0.02 .02 0.02 .12 0.06 .10 0.06
Black ⫺.07a 0.03 ⫺.01 0.03 .006 0.04 ⫺.46b 0.09 .06 0.08
Maternal age ⫺.005c 0.01 ⫺.004c 0.001 ⫺.006c 0.002 .004 0.01 ⫺.02b 0.01
Children in home ⫺.03c 0.01 ⫺.01 0.01 ⫺.02 0.01 ⫺.09c 0.03 ⫺.04 0.03
Infant activity .03a 0.01 .02a 0.01 .03a 0.01 .04 0.03 .04 0.03
knowledge of infant development only when mothers reported psychological distress.
This study extends the literature in several ways. A previous study using a small convenience sample with-out consideration of potential confounders demon-strated that knowledge of infant development was asso-ciated with increased use of home safety practices.20The
current study adds to that work by demonstrating that, when demographic and child characteristics are also considered, this is true only for those safety practices requiring installation. Second, it offers a possible expla-nation for the previously identified association between injury and maternal depressive symptoms,8low internal
locus of control,7 or general stress3,9; that is, maternal
psychological adjustment predicts home safety practices, which may predict injury rates. Finally, this study is important in its explicit targeting of low-income and minority mother-infant dyads. Poor and minority chil-dren have been shown to be at higher risk for nearly all types of injuries.2,33–35Findings that can be applied to this
population may have a greater potential to impact injury rates.
The interaction between maternal psychological symptoms and knowledge may be especially important to injury prevention. Mothers with low levels of psycho-logical distress report high levels of implementing safety practices requiring installation regardless of knowledge of infant development. Improved knowledge only in-creases implementation of these practices among moth-ers with high levels of psychological symptoms. This is demonstrated by Fig 1 and is illustrated by case examples in the Appendix. Injury-prevention efforts may best be targeted to mothers with both high levels of psycholog-ical symptoms and low knowledge, and these efforts could be directed at improving knowledge or treating depression.
A noteworthy finding indicated that, whereas poverty was not a consistent predictor when psychological ad-justment was also considered, it was related to whether families installed safety devices in both the regression analysis of the birth cohort data and the ethnographic interviews. Children living in poverty are at higher risk of nearly all types of injury.1,5Installed devices are
pas-sive and do not require caregiver vigilance to improve safety. The use of safety devices by poor families may be as simple as giving them these inexpensive devices. Poor families have been found to have more child safety hazards in the home3and express the most interest in
low-cost safety equipment.36
Child gender is closely related to the total implemen-tation of home safety practices and 3 of 4 subscales when examined alone but not when considered with other factors. This is likely because of confounding of gender with observed infant activity, with boys having higher levels of gross motor activity. This is consistent with previous work that has shown that boys are at greater risk of injury but that this is mostly explained by activity level and behavioral factors of boys.7,37
In the ethnographic component of this study, nearly all of the subjects reported that their child’s pediatrician, family physician, or clinic was an important source of
information regarding safety. This extends the finding that primary care providers are the preferred source of information about child safety to include rural, low-income families. A previous study found that, in more typical, nonpoor American families, physicians were the preferred source of information regarding safety.15This is
in contrast to a large multinational study in Europe where the most commonly sited sources of information were family, television, and friends.38
This study has several limitations. First, the outcome of interest, the use of home safety practices, relies on self-report. The instrument was derived from an obser-vational checklist of home safety practices, but the va-lidity of self-report is unknown. However, the checklist items demonstrate good scalability; self-report of home safety measures has been used in many previous injury research studies39–41; has been validated as consistent
with observed home safety practices25; and self-report is
how clinicians and injury-prevention specialists make decisions about services, anticipatory guidance, and pol-icy. Second, this study is an observational cohort study. Because of its longitudinal design (KIDI collected at 6 months and RKKSS at 15 months), an association pro-vides a necessary, but not sufficient, condition for deter-mining a causal inference. Lastly, we chose to report statistical significance for P values of ⬍.05 rather than correct for multiple testing. We had 2 primary explana-tory variables of interest: knowledge of development and psychological adjustment. The relationship between knowledge of development and home safety practices is of marginal significance (P⬍.05) but is reported because of consistency with previous research and our wish to balance the risk of a type 1 error with the risk of a type 2 error.
Findings from this study can be applied directly to the design of emerging strategies for injury prevention. First, the identification and treatment of maternal mental health disorders may be critical elements of childhood injury programs that seek to increase the use of home safety practices. Second, educating parents about infant development may improve home safety practices, espe-cially those practices that require installation. This is particularly true for mothers experiencing high levels of psychological distress. Third, the ethnographic compo-nent of this study confirms the importance of the role of the primary care clinician in providing information and education around home safety for toddlers. Mothers with low knowledge of infant development and high levels of mental health symptoms may have children with the greatest risk of injury in the home. These fam-ilies may be in greatest need of parenting education, safety education, and maternal mental health assess-ment and treatassess-ment.
APPENDIX: ETHNOGRAPHIC CASE STUDIES THAT ILLUSTRATE THE RELATIONSHIP AMONG MATERNAL PSYCHOLOGICAL SYMPTOMS, KNOWLEDGE, AND IMPLEMENTATION OF HOME SAFETY PRACTICES
Case 1
with Todd’s father. Pearl was diagnosed with depression and hospitalized with postpartum depression after her oldest child’s birth. She described herself as “moody” and seemed exhausted and listless. She took antidepres-sants but stopped taking them because of adverse effects like nightmares. Pearl described Todd at age 2 as “always being into stuff.” Her main strategy to ensure his safety was “just to watch him.” When asked about what else she did to keep her 2 children safe, she said, “You can’t protect ’em, not unless you put pillows around ’em in a padded room. I mean you can like put the safety things up for the knobs and the plugs and the stuff like that and go all out and buy that. But it’s not gonna do you no good ’cause once it’s been around long enough and they see you open it they’re gonna learn how to open it eventually.”
Case 2
Kriste was 32 when she had her son, Evan. She lived with her husband and 4 children in a single-wide mobile home. Kriste was diagnosed with depression in 2002 and took medication until she began breastfeeding. When Evan was a toddler, Kriste occasionally felt the need for antidepressant medication but said she could not afford to buy it or go to the doctor to get her prescription renewed. For Evan, she saw danger all around because he “was into everything.” She talked about her steps to child proofing the house: “I figured out that if they’re going in there I need to buy a gate and put it up. The plugs, I got them free from a baby store. And then I seen them little locks in the store, so I bought them for the cabinets. I seen ’em and said, ‘oh that’s a good idea!’ ” Kriste said that she learned about all of these safety precautions from the child’s doctor and from a person associated with an early childhood education program.
ACKNOWLEDGMENTS
Funding for this project was provided by the National Institute of Child Health and Human Development grant P01-HD-39667, with cofunding provided by National Institute on Drug Abuse and by the Maternal and Child Health Bureau grant R40-MC04293-01-03.
The Family Life Project key investigators included Lynne Vernon-Feagans (principal investigator), Martha Cox, Clancy Blair, Margaret Burchinal, Linda Burton, Keith Crnic, Ann Crouter, Patricia Garrett-Peters, Mark Greenberg, Stephanie Lanza, Roger Mills-Koonce, Debra Skinner, Emily Werner, and Michael Willoughby.
We thank the families for allowing us into their lives. We also thank Jim Peak, Eloise Neebe, and Karen Cai for managing the data; Carol Runyan for assistance with the article; and Karolyn Forbes for editorial assistance.
REFERENCES
1. Danseco ER, Miller TR, Spicer RS. Incidence and costs of 1987–1994 childhood injuries: demographic breakdowns.
Pe-diatrics. 2000;105(2). Available at: www.pediatrics.org/cgi/
content/full/105/2/e27
2. Schwebel DC, Brezausek CM, Ramey SL, Ramey CT. Interac-tions between child behavior patterns and parenting:
implica-tions for children’s unintentional injury risk.J Pediatr Psychol.
2004;29(2):93–104
3. Glik DC, Greaves PE, Kronenfeld JJ, Jackson KL. Safety haz-ards in households with young children.J Pediatr Psychol.1993; 18(1):115–131
4. Rivara FP, Bergman AB, LoGerfo JP, Weiss NS. Epidemiology of childhood injuries. II. Sex differences in injury rates.Am J
Dis Child.1982;136(6):502–506
5. Dal Santo JA, Goodman RM, Glik D, Jackson K. Childhood unintentional injuries: factors predicting injury risk among preschoolers.J Pediatr Psychol.2004;29(4):273–283
6. O’Connor TG, Davies L, Dunn J, Golding J, for the ALSPAC Study Team. Distribution of accidents, injuries, and illnesses by family type. Pediatrics.2000;106(5). Available at: www.pediatrics.org/ cgi/content/full/106/5/e68
7. Damashek AL, Williams NA, Sher KJ, Peterson L, Lewis T, Schweinle W. Risk for minor childhood injury: an investigation of maternal and child factors. J Pediatr Psychol. 2005;30(6): 469 – 480
8. Methany AP. Injuries among toddlers: contributions from child, mother, and family. In: Chess S, Thomas A, Hertzig M,
eds. Annual Progress in Child Psychiatry and Child Development
1987. New York, NY: Brunner/Mazel; 1988:521–535
9. Greaves PE, Glik D, Kronenfeld J, Jackson K. Determinants of controllable in-home child safety hazards. Health Educ Res.
1994;9(3):307–314
10. Bijur PE, Kurzon M, Overpeck MD, Scheidt PC. Parental alco-hol use, problem drinking, and children’s injuries.JAMA.1992; 267(23):3166 –3171
11. American Academy of Pediatrics. Tipp: The Injury Prevention Program. Available at: www.aap.org/family/tippmain.htm. Ac-cessed November 2, 2007
12. Consumer Product Safety Commission. Baby safety checklist. Available at: www.cpsc.gov/cpscpub/pubs/shower/images/206. pdf. Accessed November 2, 2007
13. Consumer Product Safety Commission. Childproofing your home: 12 safety devices to protect your children. Available at: www.cpsc.gov/cpscpub/pubs/grand/12steps/12steps.html. Ac-cessed November 2, 2007
14. Rivara FP. Epidemiology of childhood injuries. I. Review of current research and presentation of conceptual framework.
Am J Dis Child.1982;136(5):399 – 405
15. Eichelberger MR, Gotschall CS, Feely HB, Harstad P, Bowman LM. Parental attitudes and knowledge of child safety: a na-tional survey.Am J Dis Child.1990;144(6):714 –720
16. Mock C, Arreola Rissa C, Trevino Perez R, et al. Childhood injury prevention practices by parents in Mexico. Inj Prev.
2002;8(4):303–305
17. Morrongiello BA, Kiriakou S. Mothers’ home safety practices for preventing six types of childhood injuries: what do they do, and why?J Pediatr Psychol.2004;29(4):285–297
18. Peterson L, Farmer J, Kashani JH. Parental injury prevention endeavors: a function of health beliefs?Health Psychol.1990; 9(2):177–191
19. Hu X, Wesson D, Parkin P, Rootman I. Pediatric injuries: pa-rental knowledge, attitudes and needs. Can J Public Health.
1996;87(2):101–105
20. Rivara FP, Howard D. Parental knowledge of child develop-ment and injury risks.J Dev Behav Pediatr.1982;3(2):103–105 21. Vernon-Feagans L, Pancsofar N, Willoughby MT, Odum E, Quade A. Predictors of maternal language input during a pic-ture book task in the home: the mediational role of the quality of the home environment.J Appl Dev Psychol.2008; In press 22. American Academy of Pediatrics.Implementing Safety Counseling
in Office Practice. Elk Grove Village, IL: American Academy of
23. Creswell JW, Plano VL.Designing and Conducting Mixed Method
Research. Thousand Oaks, CA: Sage; 2006
24. Russell KM, Champion VL. Health beliefs and social influence in home safety practices of mothers with preschool children.
Image J Nurs Sch.1996;28(1):59 – 64
25. Morrongiello BA, House K. Measuring parent attributes and supervision behaviors relevant to child injury risk: examining the usefulness of questionnaire measures.Inj Prev.2004;10(2): 114 –118
26. McPhee DL.Knowledge of Infant Development Inventory. Chapel Hill, NC: University of North Carolina; 1981
27. Derogotis L.Brief Symptom Inventory 18. Minneapolis, MN: NCS Pearson, Inc; 2000
28. Bayley N.Bayley Scales of Mental Development. New York, NY: Psychological Corporation; 1969
29. Stifter CA, Corey J. Vagal regulation and observed social be-havior in infancy.Soc Dev.2001;10:189 –201
30. Bernard HR, Ryan GW. Text analysis: qualitative and quanti-tative methods. In: Bernard HR, ed. Handbook of Methods in
Cultural Anthropology. Walnut Creek, CA: AltaMira Press; 1998
31. Miles MB, Huberman M.Qualitative Data Analysis, an Expanded
Source Book. 2nd ed. Thousand Oaks, CA: Sage; 1994
32. Tashakkori A, Teddlie C.Handbook of Mixed Methods in the Social
and Behavioral Sciences. Thousand Oaks, CA: Sage; 2003
33. Delgado J, Ramirez-Cardich ME, Gilman RH, et al. Risk factors for burns in children: crowding, poverty, and poor maternal education.Inj Prev.2002;8(1):38 – 41
34. Shenassa ED, Stubbendick A, Brown MJ. Social disparities in housing and related pediatric injury: a multilevel study.Am J
Public Health.2004;94(4):633– 639
35. Khambalia A, Joshi P, Brussoni M, Raina P, Morrongiello B, Macarthur C. Risk factors for unintentional injuries due to falls in children aged 0 – 6 years: a systematic review.Inj Prev.2006; 12(6):378 –381
36. van Weeghel I, Kendrick D, Marsh P. Accidental injury: risk and preventative interventions. Arch Dis Child. 1997;77(1): 28 –31
37. Morrongiello BA, Ondejko L, Littlejohn A. Understanding tod-dlers’ in-home injuries: I. Context, correlates, and determi-nants.J Pediatr Psychol.2004;29(6):415– 431
38. Vincenten JA, Sector MJ, Rogmans W, Bouter L. Parents’ perceptions, attitudes and behaviours towards child safety: a study in 14 European countries. Int J Inj Contr Saf Promot.
2005;12(3):183–189
39. Posner JC, Hawkins LA, Garcia-Espana F, Durbin DR. A ran-domized, clinical trial of a home safety intervention based in an emergency department setting. Pediatrics. 2004;113(6): 1603–1608
40. Hapgood R, Kendrick D, Marsh P. Do self reported safety behaviours predict childhood unintentional injuries?Inj Prev.
2001;7(1):14 –17
41. Gielen AC, Wilson ME, McDonald EM, et al. Randomized trial of enhanced anticipatory guidance for injury prevention.Arch
DOI: 10.1542/peds.2007-1255
2008;121;e1668
Pediatrics
Adam J. Zolotor, Margaret Burchinal, Debra Skinner and Marjorie Rosenthal
Predictors of Home Safety Practices in Rural Low-Income Communities
Maternal Psychological Adjustment and Knowledge of Infant Development as
Services
Updated Information &
http://pediatrics.aappublications.org/content/121/6/e1668 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/121/6/e1668#BIBL This article cites 26 articles, 7 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/home_safety_sub Home Safety
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2007-1255
2008;121;e1668
Pediatrics
Adam J. Zolotor, Margaret Burchinal, Debra Skinner and Marjorie Rosenthal
Predictors of Home Safety Practices in Rural Low-Income Communities
Maternal Psychological Adjustment and Knowledge of Infant Development as
http://pediatrics.aappublications.org/content/121/6/e1668
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.