R E S E A R C H
Open Access
Quantification of upper limb position sense
using an exoskeleton and a virtual reality
display
Anne Deblock-Bellamy
1,2, Charles Sebiyo Batcho
1,2,3, Catherine Mercier
1,2,3and Andreanne K. Blanchette
1,2,3*Abstract
Background:Proprioceptive sense plays a significant role in the generation and correction of skilled movements and, consequently, in most activities of daily living. We developed a new proprioception assessment protocol that enables the quantification of elbow position sense without using the opposite arm, involving active movement of the evaluated limb or relying on working memory. The aims of this descriptive study were to validate this assessment protocol by quantifying the elbow position sense of healthy adults, before using it in individuals who sustained a stroke, and to investigate its test-retest reliability.
Methods:Elbow joint position sense was quantified using a robotic device and a virtual reality system. Two assessments were performed, by the same evaluator, with a one-week interval. While the participant’s arms and hands were occluded from vision, the exoskeleton passively moved the dominant arm from an initial to a target position. Then, a virtual arm representation was projected on a screen placed over the participant’s arm. This virtual representation and the real arm were not perfectly superimposed, however. Participants had to indicate verbally the relative position of their arm (more flexed or more extended; two-alternative forced choice paradigm) compared to the virtual representation. Each participant completed a total of 136 trials, distributed in three phases. The angular differences between the participant’s arm and the virtual representation ranged from 1° to 27° and changed pseudo-randomly across trials. No feedback about results was provided to the participants during the task. A discrimination threshold was statistically extracted from a sigmoid curve fit representing the relationship between the angular difference and the percentage of successful trials. Test-retest reliability was evaluated with 3 different complementary approaches, i.e. a Bland-Altman analysis, an intraclass correlation coefficient (ICC) and a standard error of measurement (SEm).
Results:Thirty participants (24.6 years old; 17 males, 25 right-handed) completed both assessments. The mean discrimination thresholds were 7.0 ± 2.4 (mean ± standard deviation) and 5.9 ± 2.1 degrees for the first and the second assessment session, respectively. This small difference between assessments was significant (−1.1 ± 2.2 degrees), however. The assessment protocol was characterized by a fair to good test-retest reliability (ICC = 0.47). Conclusion:This study demonstrated the potential of this assessment protocol to objectively quantify elbow position sense in healthy individuals. Futures studies will validate this protocol in older adults and in individuals who sustained a stroke.
Keywords:Assessment, Proprioception, Robotic, Stroke, Sensory, Virtual reality, Upper limb
* Correspondence:[email protected]
1
Center for Interdisciplinary Research in Rehabilitation and Social Integration (CIRRIS), 525 Boulevard Wilfrid-Hamel, Quebec City (QC) G1M 2S8, Canada 2Faculty of Medicine, Universite Laval, 1050 Avenue de la Medecine, Quebec
City (QC) G1V 0A6, Canada
Full list of author information is available at the end of the article
Background
Proprioception is defined as the ability to perceive body segment positions and movements in space [1]. Sensory receptors involved in proprioception are mostly located in muscle [2–4], joint [5,6] and skin [3,7]. Propriocep-tive sense is known to play a significant role in motor control [8–11] and learning [8, 12], particularly in the absence of vision. The importance of proprioceptive in-puts has been demonstrated while studying individuals who presented lack of proprioception due to large-fiber sensory neuropathy [11, 12]. Despite an intact motor system, somatosensory deafferentation may lead to limi-tations in several activities involving motor skills, such as eating or dressing [12]. These disabilities may also be observed in individuals with proprioceptive impairments due to a stroke. Indeed, approximately half of the indi-viduals who sustained a stroke present proprioceptive impairments in contralesional upper limb [13]. After a stroke, proprioception is known to be related to recovery of functional mobility and independence in activities of daily living (ADL; [14]). Fewer individuals with signifi-cant proprioceptive and motor losses (25%) were inde-pendent in ADL than individuals with motor deficits alone (78%). Moreover, fewer individuals with proprio-ceptive deficits (60%) after a stroke are discharged from the hospital directly to home compared to those without proprioceptive deficits (92%) [15].
Although the negative impact of proprioceptive im-pairments on motor and functional recovery is known, a large proportion of clinicians (70%) report not using standardised assessment to evaluate somatosensory defi-cits in patients with a stroke [16]. In clinical and re-search settings, proprioception is most frequently assessed with limb-matching tasks. Two types of match-ing tasks have commonly been used: the ipsilateral re-membered matching task and the contralateral concurrent matching task [17]. In an ipsilateral remem-bered matching task, the evaluator or robotic device brings the patient’s limb to a target joint position, when the patient’s eyes are closed, keeps the limb in this pos-ition for several seconds, and then moves back the limb to the initial position. The patient needs to memorize the reference position and replicate it with the same (ip-silateral) limb. This task cannot, however, be used to evaluate proprioception in individuals with working memory issues, which represent around 25% of individ-uals who sustained a stroke [18]. In such cases, the matching error observed could reflect memory deficits, rather than proprioceptive impairments. Moreover, upper limb paresis affects 76% of individuals who sus-tained a stroke [19], making the task’s execution difficult or impossible. Assessing proprioception with the less af-fected arm as the indicator arm is therefore frequently considered in patients with hemiparesis. Indeed, in a
contralateral concurrent matching task, the patient has to reproduce a mirror image of the evaluated limb pos-ition with the opposite (contralateral) limb [17]. How-ever, considering that 20% of individuals who sustained a stroke also presents proprioceptive impairment on the ipsilateral side of the lesion [13], it would be difficult to ascertain whether the error is due to deficits in the evaluated arm, the opposite arm or both. In addition, in-terhemispheric communication is required in a contra-lateral concurrent matching task. Individuals with asymmetric stroke or with transcallosal degeneration would therefore be particularly disadvantaged while being assessed with a contralateral concurrent matching task [17].
In order to study proprioception in individuals who sustained a stroke, we developed an assessment protocol, that combines the use of an exoskeleton and a virtual reality system, enabling the quantification of position sense without using the opposite arm, involving active movement of the evaluated limb or relying on working memory. The primary objective of the present study was to validate the assessment protocol by quantifying the elbow joint position sense of healthy adults, before using this protocol with individuals who sustained a stroke. As a secondary objective, test-retest reliability of the assess-ment protocol was investigated.
Methods Participants
Participants were recruited in this descriptive study using a convenience sample. They were included if they were between 18 and 55 years old and were excluded if they had any history of musculoskeletal disorder of the dominant upper limb or any neurological condition that could affect their performance. This study was approved by the institutional ethics review board. All subjects pro-vided written informed consent prior to their participa-tion in the study. Based on sample size formula proposed by Zou [20], it was determined that a minimal sample size of 19 participants was required for this ex-periment (hypothesized intraclass correlation coefficient = 0.7; α=0.05; β=0.95). According to Springate [21], a sample of at least 25–30 participants should be used to provide an adequate estimate of the random error. A sample size of 30 participants was therefore recruited to evaluate the stability of the assessment protocol.
General procedure
health questionnaires. These questionnaires were used to determine participants’ eligibility (history of neuro-logical and/or musculoskeletal disorders), to establish their sociodemographic profile (age, gender, dominance, weight, height, occupation, and leisure activities) and to compare qualitatively their level of perceived fatigue and stress at the beginning of both assessment sessions. After the participant’s installation, the assessment of dominant upper limb proprioception was performed. The duration of this first session was approximately 90 min, including 40–45 min for the proprioception as-sessment itself. The second session was devoted exclu-sively to the proprioception assessment and the total duration was approximately 45 min. Four different eval-uators participated in this experiment. For each partici-pant, the same evaluator carried out both assessments.
Proprioception assessment
The assessment protocol enabled the identification of the smallest angular difference, between the participant’s arm and a virtual arm representation projected on a screen located over participant’s arm, that each partici-pant was able to discriminate (discrimination threshold) using a two-alternative forced choice paradigm.
The proprioception assessment was performed using the KINARM Exoskeleton Lab (BKIN, Technologies Ltd., Kingston, Ontario, Canada). It consists of 2 motorised upper limb exoskeletons (Fig.1a) that enable passive arm movements in the horizontal plane and a two-dimensional virtual reality (VR) display. This VR system projected a virtual arm representation on a screen placed over the participant’s upper limb (Fig. 1b). The KINARM Exoskeleton Lab has been previously used to assess proprioception and motor functions in stroke [22–26] and traumatic brain injury adult populations [27]. However, in these studies, a contralateral concur-rent matching task was used to assess position sense [22–26], contrary to the present experiment.
During the proprioception assessment, participant sat in a wheelchair base with each arm supported against gravity by the exoskeletons (wrist in neutral position, forearm in pronation, shoulder at 65 degrees of horizon-tal abduction). At first, the evaluator adjusted the exo-skeletons to fit in the participant. These adjustments were recorded and reproduced in the second session. The exoskeleton and VR display were then calibrated, in accordance with the company recommendations, to cor-rectly measure arm position data and to properly align the virtual representation. The alignment and the length of the virtual forearm were determined based on the participant’s arm. The size of the hand was proportion-ally adjusted based on the forearm dimensions.
In each trial, the exoskeleton passively moved the dominant forearm (towards elbow flexion or extension) from an initial position to a target position. Shoulder position was maintained at 65° of horizontal abduction throughout the entire protocol (0 degrees of horizontal abduction corresponding to arm raised to the side). The upper limbs were occluded from vision. Four different initial positions (30, 55, 70, 95° of elbow flexion) and two target positions (50 and 75° of elbow flexion) were used and randomized to avoid anticipation from the par-ticipants. The amplitude of the angular displacement be-tween initial and target position was systematically 20° and the displacement was performed in 4 s, correspond-ing to a velocity of 5 deg./s, for each trial. Elbow joint angular positions and velocities were obtained from KINARM motor encoders. Once the robot completed the passive displacement towards target position, a vir-tual arm representation was projected on the screen. This virtual representation was not perfectly superim-posed over the real arm, however. The angular difference (Fig. 1c) between the participant’s arm and the virtual representation ranged from 1° to 27°, towards flexion or extension and changed pseudo-randomly across trials. For each trial, the participant was instructed to verbally
b
c
a
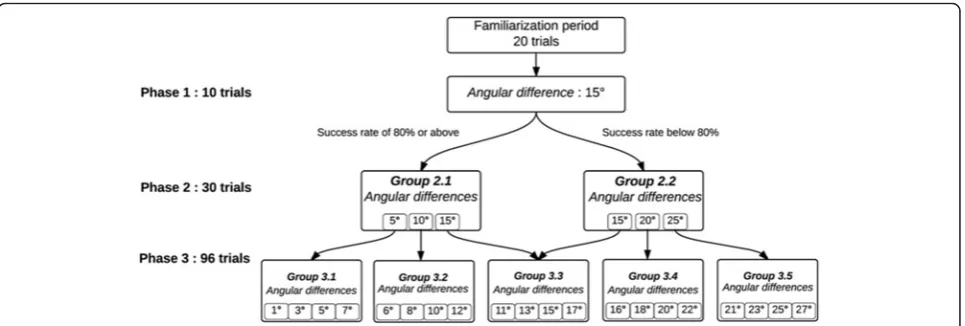
identify the relative position of their arm (more flexed or more extended) compared to the virtual representation. Each assessment consisted of 136 trials, distributed in three phases of 10, 30 and 96 trials (Fig. 2). Verbal an-swers given by the participant were noted by the evalu-ator. No feedback about results was provided to the participant during the task.
The assessment began with a period of familiarization, including a total of 20 trials. Indeed, 10 trials were first done with a visual feedback of the real arm to confirm the participant’s understanding of the instructions. Then, the participant had to complete 10 additional trials with-out visual feedback, to familiarize himself with the vir-tual environment and the experimental task. During this familiarization phase (not in the other phases), a total of 4 trials were performed when the virtual representation was exactly superimposed over the real arm in order to verify KINARM’s calibration. Considering that the proto-col aimed at identifying a precise discrimination thresh-old in as few trials as possible for each participant, the difficulty level of the experimental task was adapted to the participant’s capacity based on a decision tree (Fig.2). The angular difference was initially set at 15° for the first phase (10 trials), and then adjusted in the fol-lowing phases according to the participant’s percentage of successful trials obtained in the previous phase, based on an adaptive psychophysical method. As described in Taylor and Creelman [28], an adaptive method consists of a sequence of trials, which begins by testing at some arbitrary initial level (Phase 1). After a predefined num-ber of trials, a new testing level is determined, and so on (Phases 2 and 3). In the second and third phases, several angular differences were tested repeatedly in random
order. An angular difference successfully identified in 80% of the trials or more was considered as detected. Participants were therefore categorized based on their capacity to detect elbow joint position.
Preliminary data showing the feasibility of using this assessment protocol in individuals with a stroke have been published in abstract form [29].
Statistical analysis
Parametric descriptive statistics, such as mean, standard deviation (SD) and frequency, were used to describe sociodemographic data (age, gender, dominance).
To quantify position sense for each participant, a discrimination threshold was statistically extracted from a sigmoid curve fit representing the relationship between the angular difference (x) and the percentage of successful trials (y) (Fig. 3). The best curve fit was found through the least squares (ordinary) fitting method. For each assessment, a discrimination thresh-old corresponding to the angular difference at 75% of successful trials was calculated based on the following 4-parameter logistic equation:
y¼Lowerþ ðUpper−LowerÞ
1þ10ðLogEC50−XÞHillSlope
Considering the two-alternative forced choice para-digm, Lower (Y value at the lower plateau) and Upper (Y value at the upper plateau) were fixed at 50 and 100%, respectively. EC50 corresponds to the X value when the Y is halfway between the Upper and Lower values. HillSlope describe the steepness of the curve.
Similar methods of discrimination/detection threshold identification were used in previous studies [30–33].
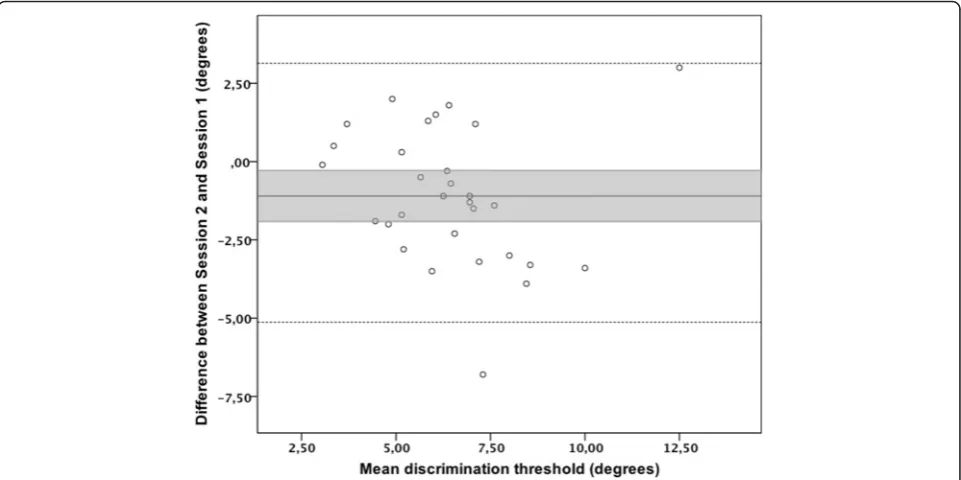
In order to assess test-retest reliability, different complementary approaches were used, as recom-mended in Lexell et al. [34]. A Bland-Altman plot was used to reflect the spread of the score difference (Session 2 - Session 1) around the mean discrimin-ation threshold and to determine the presence or ab-sence of a bias between discrimination thresholds obtained in both assessments. Relative reliability, re-ferring to the degree to which individuals maintain their position in a sample with repeated measure-ments [35], was quantified with a two-way mixed sin-gle measure ICC (2,1) for absolute agreement. ICC was interpreted according to Fleiss [36], where an ICC < 0.4 indicates a poor reproducibility, an ICC be-tween 0.4 and 0.75 indicates a fair to good reproduci-bility and an ICC≥0.75 indicates an excellent reproducibility. Absolute reliability, referring to the variability of the scores from trial to trial which is not dependent on the sample [37], was obtained with the standard error of measurement (SEm). The SEm, calculated as follows SEm¼pffiffiffiffiffiffiffiffiffiffiffiffiWMS (where WMS represents the mean squared error term extracted from the repeated measures analysis of variance [34]), is an indicator of the dispersion of the measurement errors to estimate participant’s scores from their ob-served score [38].
Data analyses and statistics were performed using Microsoft Excel 15.18 (Microsoft Corporation, Red-mond, Washington, USA), GraphPad Prism 7 (Graph-Pad Software, Inc., La Jolla, California, USA), IBM SPSS Statistics 24.0 (SPSS Inc., Chicago, Illinois, USA) and R 3.3.3 (The R Foundation for Statstical Computing, Vienna, Austria).
Results
Thirty healthy adults (17 males, 25 right-handed, mean age ± SD: 24.6 ± 3.3 years old) participated in the present study.
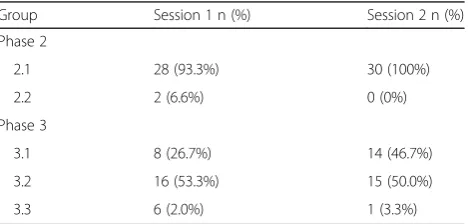
The distribution of participants across categories, representing their capacity to discriminate elbow joint position, can be observed in Table 1. In Phase 2, all participants, except one, were categorized in Group 2.1, regardless of the assessment session. In Phase 3 of the Session 1, participants were distributed across Groups 3.1, 3.2 and 3.3, with a majority (53.3%) in Group 3.2. In Session 2, these percentages were slightly different, with percentage of participants al-most equally distributed between Groups 3.1 and 3.2. Modifications on the categorization across sessions were therefore observed. While 14 participants remained in the same group, 13 participants moved to a group testing smaller errors, and 3 participants moved to a group testing larger errors.
Quantifying the elbow position sense of healthy participants
Mean discrimination thresholds of healthy participants were 7.0° ± 2.4° and 5.9° ± 2.1° (mean ± SD) for Sessions 1 and 2, respectively (Fig. 4), with a mean difference be-tween assessments of−1.1° ± 2.2°.
In Session 2, participants included in Group 3.1 had discrimination thresholds ranging from 3.0 to 6.3 de-grees, while discrimination thresholds measured in Group 3.2 participants ranged between 5.6 and 8.3 de-grees. The only participant categorized in Group 3.3 had a discrimination threshold of 14.0 degrees.
Mean coefficients of determination (R-squared), indi-cating the goodness of the sigmoid curve fit, were 0.91 ± 0.07 (range: 0.77–1.0) for Session 1 and 0.93 ± 0.05 (range: 0.76–1.0) for Session 2.
Test-retest reliability
A Bland-Altman plot representing the differences be-tween discrimination threshold measured in Sessions 2 Fig. 3Sigmoid curve fit representing the relationship between the
angular difference and the percentage of successful trials in a representative participant (Group 3.2). This figure combined results of Phase 1, 2 and 3
Table 1Participants’categorization based on their capacity to detect elbow joint position
Group Session 1 n (%) Session 2 n (%)
Phase 2
2.1 28 (93.3%) 30 (100%)
2.2 2 (6.6%) 0 (0%)
Phase 3
3.1 8 (26.7%) 14 (46.7%)
3.2 16 (53.3%) 15 (50.0%)
and 1 as a function of the mean of both assessments showed that the line of equality (Mean difference = 0) is located outside the 95% confidence interval (95% CI) of the mean difference (Fig.5), suggesting a significant bias [34] of−1.1° ± 2.2°. The intraclass correlation coefficient (ICC) for absolute agreement between discrimination threshold measured in Sessions 1 and 2 was 0.47 (95% CI: 0.14–0.71) indicating a fair to good test-retest reli-ability. Moreover, the SEm was 1.5°, which represents 25.4% of the mean discrimination threshold measured in the second session.
Discussion
We developed a position sense assessment protocol, which combines a robotic device and a virtual reality dis-play, that enables the quantification of elbow position sense without using the opposite arm, involving active movement of the evaluated limb or relying on working memory, considering these abilities may be impaired after a stroke. As a preliminary step of validation, this experi-ment showed that this assessexperi-ment protocol can quantify elbow position sense of healthy young adults (mean threshold: around 6.5 degrees), with a fair to good test-retest reliability. Moreover, it enabled quantification on a continuous scale, as demonstrated by the overlap in dis-crimination thresholds despite participants’categorization (Group 3.1 = 3.0–6.3 degrees; Group 3.2 = 5.6–8.3 degrees in Session 2).
Quantifying the elbow position sense
This new proprioception assessment protocol can ob-jectively quantify the position sense with a discrimin-ation threshold (in degrees), contrary to the most commonly used proprioception clinical assessments, which are predominantly using ordinal or dichotomous scales. The Rivermead Assessment of Somatosensory Performance (RASP) and the Nottingham Sensory As-sessment (NSA) were identified, by clinicians, as the most frequently used standardised somatosensory as-sessments that include a proprioception testing [16]. The NSA evaluates somatosensory impairments through 7 sub-tests, including an appreciation of movement Fig. 4Mean discrimination threshold (degree) for each assessment
session. Error bars represent SD. * =p< 0.05
perception and direction. The patient is asked to repro-duce a mirror image of the movement with the other arm, while he/she is blindfolded. Proprioception is then evaluated on a 4-level ordinal scale, where 0 = no move-ment perceived; 1 = appreciation of the movemove-ment taking place; 2 = direction of movement sense, but inaccurate position; 3 = joint position sense, within 10° of the pos-ition [39]. The RASP evaluates 7 different sensory mo-dalities, including joint movement and movement direction discrimination. The patient has to report orally if a movement is perceived (movement discrimination) and in which direction the segment is moved (“up” or “down”; direction discrimination). For each trial, pro-prioception movement and direction discrimination are evaluated using a dichotomous scale, where 0 represents a missed trial, and 1 represents a successful trial [40]. These clinical tools present some limitations for proprio-ception assessment, however. The identification of pro-prioceptive deficits may be possible with these tools, but it remains difficult to assess the severity of impairment and demonstrate patient’s progression while using di-chotomous or ordinal scales. Moreover, the evaluator has to subjectively evaluate the participant’s capacity. These tests cannot be used in healthy subjects (ceiling effect) and, consequently, standard norms cannot be de-termined to facilitate the interpretation of the score. Contrary to the RASP and the NSA, our proprioception assessment protocol allows a quantification of elbow position sense on a continuous scale. Consequently, it is reasonable to believe that it enables a more precise measurement and provides a more sensitive assessment, which is essential to evaluate the effectiveness of a clin-ical intervention.
In an attempt to address the limitations of the RASP and the NSA, other proprioception assessment tools using a continuous scale were developed. For example, the Wrist Position Sense Test (WPST) quantifies the capacity to perceive wrist position after a passive move-ment [41]. The assessmove-ment device consists of a box-like apparatus with a one-degree-interval scale, a splint for the forearm and hand fixed on the base and a curtain, to avoid arm visual feedback. A pointer enables subjects to indicate perceived wrist position, without any visual feedback of wrist position. Similarly to our protocol, the aim of the WPST is to objectively quantify the position sense, in degrees, without requiring motor and cognitive abilities [41]. Experimenter biases are, however, more likely to occur. Indeed, arm movement (velocity, range) and position may vary within and between assessments while using the WPST considering that passive move-ment needs to be performed by the examiner. Robotic devices may offer the possibility to reduce the potential influence of experimenter on the assessment. Wrist pro-prioceptive function has been assessed by Cappello et al.
[42] using the Wrist Robot, which is a 3-degree of free-dom manipulandum. A 2-alternative forced choice para-digm was employed; participants having to verbally indicate which of two different displacements was larger. As stimuli were presented consecutively, working mem-ory may however be a confounder in this assessment. A 2-alternative forced choice paradigm was also used to evaluate the ability to detect arm displacement con-trolled by a planar robot [33]. This protocol also soli-cited memory to recall stimuli for comparison. Memory deficits would not interfere in the matching task devel-oped by Rinderknecht et al. [43]. After a passive move-ment performed by a robotic device, participants had to indicate the perceived wrist position by adjusting the gauge indicator position on a touchscreen. Ingemanson et al. [44] demonstrated that finger proprioception as-sessment might also be possible through the use of an exoskeleton. In this task, participants were instructed to press the spacebar on a keyboard when they perceived their index and middle fingers were overlapped during a passive crisscross movement. This task assesses “ dy-namic position sense” at the fingers, but is neither fin-ger- nor joint-specific. Dukelow et al. [25] quantified upper limb position sense of healthy and stroke individ-uals using a robotic arm position-matching task. A robot moved participants’arm to one of the nine positions and they had to mirror-match that position with the opposite upper limb. In this matching-task, proprioceptive deficits in the contralateral upper limb could however bias the interpretation of results. In all these robotic-based pro-prioception assessment tasks, the involvement of the examiner was minimal.
Our assessment protocol took into consideration some of the potential confounders, since it enables the quanti-fication of elbow position sense without using the op-posite arm, involving active movement of the evaluated limb or relying on working memory. Another bias may however be introduced with the proposed approach. Since the identification of elbow relative position volves a comparison with a virtual representation, it in-volves a judgement based on proprioceptive and visual information. Multimodal sensory integration processes can be impaired in populations with central nervous sys-tem lesion, such as stroke.
Position sense thresholds in healthy population
errors ranging from 2.2° ± 1.6 to 6.0° ± 2.5°, depending on the amplitude of the movement, when elbow joint position sense was tested with a contralateral concurrent matching task [45]. Carey et al. focused on wrist position identification following a passive movement administered by the examiner [41]. The mean difference between the real position and the estimated position (20 trials) was 6.1° ± 1.8° in healthy individuals. A comparable absolute error of 5.9° ± 3.1° was observed with a similar protocol, but this time a robotic apparatus passively moved the upper limb [43]. In another study of wrist proprioception, an absolute error of 4.7° ± 0.3° was measured when partici-pants were asked to actively reproduce the wrist configur-ation previously reached after a movement executed by a robotic device [46]. For the lower extremity, Venancio et al. evaluated knee position sense by looking at the angular differences between an initial reference position and the position actively reproduced by healthy participants [47]. After three trials, a mean relative error of 5.8° ± 4.4° was obtained while targeting angular positions located be-tween 40° and 60° of knee flexion.
A cut-off of 75% in the assessment protocol was used to determine the discrimination threshold. This cut-off was previously used in other studies [32,33]. This choice may have influenced the magnitude of the discrimin-ation threshold. A cut-off corresponding to a lower per-centage of successful trials would likely result in a lower threshold. As an example, a different percentage was used in a study aiming at the identification of ankle movement detection thresholds [31]. Indeed, the authors justified their decision of using a 50% cut-off with their protocol design, which was a voluntary choice design, in-stead of a two-alternative forced choice. They obtained a movement error detection threshold of 5.3° ± 2.1°.
Test-retest reliability
In the present study, a difference of less than 2° was ob-tained between both assessments. Even if the magnitude of this difference seems quite small, it was statistically significant. Three sources of bias may explain the differ-ence between thresholds measured in Sessions 1 and 2: the evaluator, the assessment tool and the participant. Different strategies were adopted to minimise potential biases induced by these factors. First of all, the assess-ment protocol involved a minimal contribution of the evaluator, which was the same in both assessments. All evaluators were trained to use the protocol, the robotic device, as well as the analysis softwares. Regarding the assessment protocol, the position adjustment parameters used in the first assessment were reproduced in the sec-ond. Before each assessment, the participant’s arm was calibrated following the BKIN Technologies’ recommen-dations. The same decision tree was used during both assessments. Finally, the difference between threshold
measured in Sessions 1 and 2 may be explained by real change in participants’ capacity to discriminate their elbow position. Results of the Bland-Altman analysis showed a negative shift in the difference scores related to the mean threshold. This significant bias may reflect the presence of a learning effect. A similar effect was ob-served in a study investigating test-retest reliability of several KINARM robot tasks characterizing sensori-motor and/or cognitive performance [48]. In this study, an increased performance in some parameters was ob-served between the first and the second sessions, but not between the second and the third session. In an at-tempt to limit the anticipated learning effect, the present protocol included a familiarization phase; it might not have been enough, however. Implementing a practice session before testing may eliminate this learning effect. Future studies need to include more practice trials or an additional session to limit the learning effect.
Test-retest mean difference obtained in the present study (1.1°) was smaller than the error highlighted when using other common clinician tools measuring range of motion in degrees. For example, test-retest reliability of a standard manual goniometer was inves-tigated in individuals who undergone surgery after elbow, forearm or wrist injury. The mean difference between both assessments was 3.2° for elbow flexion, and 3.5° for elbow extension [49].
The intraclass correlation coefficient calculated for our proprioception assessment protocol reflected a fair to good relative reliability. This result is similar to the test-retest reliability of the most frequently used standardised sensory assessments with stroke population [16]. The NSA presents a fair to good intra-rater agreement for the elbow’s position sense task in patients who sustained a stroke, as suggested with a Kappa coefficient of 0.71 [50]. For the RASP, Pearson’s correlation coefficients were 0.83 and 0.50 for the proprioceptive movement discrimination and for the direction discrimination, respectively. The WPST was characterized by an excellent test-retest reli-ability (r= 0.88–0.92) when administered to a population of stroke survivors [41]. Test-retest reliability was also in-vestigated in a few robot-based assessment protocols. In Dukelow et al. [25], a moderate to excellent inter-rater re-liability (r= 0.70–0.86) was obtained when participants with a stroke underwent 2 robotic assessment sessions, within a few minutes, conducted by two different exam-iners. Rinderknecht et al. [43] reported an ICC of 0.68, corresponding to a fair to good reliability, for the absolute error obtained with a robotic assessment of wrist proprio-ception in healthy subjects.
of between-subjects variability in discrimination thresh-olds had an impact on ICC calculation [37]. The ICC is therefore likely to be higher when calculated with data collected in a population with proprioceptive deficits.
While the ICC is an estimate of relative reliability, the SEm provides an indication of absolute reliability. The latter quantifies the precision of individual score on a given assessment with the same units as the measure-ment [37]. A SEm of 1.5° was obtained in the present study, which represents 25.4% of the mean discrimin-ation threshold measured in the second session. A SEm of 2.7°, which represents 44.3% of the mean absolute error (6.1°), was obtained with the WPST [41]. Rinder-knecht et al. [43] have reported a SEm of 2.1°, corre-sponding to 35.6% of the mean absolute error (5.9°). The protocol proposed in the present study seems, therefore, to offer a more accurate measurement in degrees than these two protocols.
Limitations of the study and future directions
Our position sense assessment protocol enables the quantification of elbow position sense without using the opposite arm, involving active movement of the evalu-ated limb or relying on working memory, considering sensorimotor and cognitive functions may be impaired after a stroke. Other consequences of stroke, such as vis-ual disorders, extreme fatigue, hemispatial neglect, and attentional deficits, may render the use of the proposed assessment protocol difficult, even impossible. Each ap-proach has its own limitation, and therefore it is likely that different approaches could bring a complementary perspective on proprioceptive deficits after a stroke. Tak-ing into account that most functional activities involve multiple joint movements in three dimensions, the fact that this assessment protocol evaluated a single upper limb joint in the horizontal plane should be considered as a limitation. In addition, the possibility that some partici-pants contracted their muscles during the experiment cannot be eliminated, despite clear instructions asking them to maintain their arm as relaxed as possible and to avoid helping the exoskeleton to execute the movement. Upper limb muscle activation should have been moni-tored with electromyography surface electrodes to make sure that participants remain passive.
Another limitation is that this assessment protocol needs specialized and expensive equipment, physical space, time to administer and expertise to collect and analyse the data, which could limit its clinical applica-tion. Testing duration of this proprioception assessment (approximately 40–45 min) is too long to be considered for clinical purposes. Other quantitative proprioception tools (robotic or non-robotic) have a significantly shorter assessment time, ranging from 2.5 min to 15 min [41, 43, 51–53], thus demonstrating their potential for
application in clinical settings. Nonetheless, there are ways to potentially reduce the duration of the proposed assessment protocol without deteriorating its reliability. For example, increasing velocity of angular displacement could contribute in reducing assessment duration. In the proposed assessment, a velocity of 5 deg./s was used to move the arm between initial and target position. An in-creased velocity could be tested in further studies, while keeping in mind that inducing adverse effects such as spasticity must be avoided while assessing persons with central nervous system lesion. Moreover, a different adaptive psychophysical method, such as the Parameter estimation by Sequential Testing (PEST; [28]), may in-crease the precision of the threshold while minimizing the number of trials required to estimate it and conse-quently reducing assessment duration. The proposed robotic-based protocol may currently find utility as a research tool for future studies focusing on the effective-ness of innovative rehabilitation approaches on proprio-ception in different populations who sustained a central nervous system lesion. Since the sample size was limited and the data were collected specifically in healthy young adults, results of the present study cannot be generalized to older adults or individuals who had a stroke. Future research is therefore needed to validate this assessment protocol in these populations.
Conclusion
Considering that there is a need for proprioception as-sessment tool adapted for persons presenting multiple deficits following a stroke, we develop a new protocol enabling the assessment of position sense without using the opposite arm and without relying on working mem-ory. As a preliminary step, it was demonstrated that this assessment protocol can objectively quantify elbow pos-ition sense (in degrees) of healthy young adults, with a fair to good test-retest reliability. After some modifica-tions, such as including a longer familiarization phase and the addition of muscle activation monitoring, this elbow position sense assessment protocol will be tested in older adults and individuals who sustained a stroke.
Abbreviations
95% CI:95% confidence interval; ICC: Intraclass Correlation Coefficient; KINARM: Kinesiological Instrument for Normal and Altered Reaching Movements; NSA: Nottingham Sensory Assessment; RASP: Rivermead Assessment of Somatosensory Performance; SD: Standard Deviation; SEm: Standard Error of Measurement; VR: Virtual reality; WPST: Wrist Position Sense Test
Acknowledgements
Funding
This work was supported by the Physiotherapy Foundation of Canada and the Quebec Rehabilitation Research Network. ADB received a studentship from the Centre for interdisciplinary research in rehabilitation and social integration (CIRRIS). The funding bodies had no role in the design of the study, data collection and analysis, interpretation of data, and in writing the manuscript.
Availability of data and materials
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
Authors’contributions
ADB, CSB, CM and AKB conceived and designed the experiment. Data collection were performed by ADB and AKB. ADB, CSB, CM and AKB contributed to data analysis and interpretation. ADB and AKB wrote the first draft of the manuscript. All authors read, edited and approved the final manuscript.
Ethics approval and consent to participate
This study was approved by the Institut de réadaptation en déficience physique de Québec (IRDPQ) research ethics board (reference number: 2015–423). All subjects provided written informed consent prior to their participation in the study.
Consent for publication Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author details
1Center for Interdisciplinary Research in Rehabilitation and Social Integration
(CIRRIS), 525 Boulevard Wilfrid-Hamel, Quebec City (QC) G1M 2S8, Canada. 2Faculty of Medicine, Universite Laval, 1050 Avenue de la Medecine, Quebec
City (QC) G1V 0A6, Canada.3Department of Rehabilitation, Universite Laval, 1050 Avenue de la Medecine, Quebec City (QC) G1V 0A6, Canada.
Received: 10 April 2017 Accepted: 6 March 2018
References
1. Goble DJ, Anguera JA. Plastic changes in hand proprioception following force-field motor learning. J Neurophysiol. 2010;104:1213–5.
2. Goodwin GM, McCloskey DI, Matthews PB. The contribution of muscle afferents to kinaesthesia shown by vibration induced illusions of movement and by the effects of paralysing joint afferents. Brain. 1972;95:705–48. 3. Gandevia SC, McCloskey DI. Joint sense, muscle sense, and their
combination as position sense, measured at the distal interphalangeal joint of the middle finger. J Physiol. 1976;260:387–407.
4. Clark FJ, Burgess RC, Chapin JW. Proprioception with the proximal interphalangeal joint of the index finger. Evidence for a movement sense without a static-position sense. Brain. 1986;109:1195–208.
5. Burgess PR, Clark FJ. Characteristics of knee joint receptors in the cat. J Physiol. 1969;203:317–35.
6. Clark FJ. Information signaled by sensory fibers in medial articular nerve. J Neurophysiol. 1975;38:1464–72.
7. Clark FJ, Horch KW, Bach SM, Larson GF. Contributions of cutaneous and joint receptors to static knee-position sense in man. J Neurophysiol. 1979; 42:877–88.
8. Ghez C, Sainburg R. Proprioceptive control of interjoint coordination. Can J Physiol Pharmacol. 1995;73:273–84.
9. Gordon J, Ghilardi MF, Ghez C. Impairments of reaching movements in patients without proprioception. I Spatial errors J Neurophysiol. 1995;73: 347–60.
10. Sainburg RL, Ghilardi MF, Poizner H, Ghez C. Control of limb dynamics in normal subjects and patients without proprioception. J Neurophysiol. 1995; 73:820–35.
11. Ghez C, Gordon J, Ghilardi MF, Christakos CN, Cooper SE. Roles of proprioceptive input in the programming of arm trajectories. Cold Spring Harb Symp Quant Biol. 1990;55:837–47.
12. Rothwell JC, Traub MM, Day BL, Obeso JA, Thomas PK, Marsden CD. Manual motor performance in a deafferented man. Brain. 1982;105:515–42. 13. Carey LM, Matyas TA. Frequency of discriminative sensory loss in the hand
after stroke in a rehabilitation setting. J Rehabil Med. 2011;43:257–63. 14. Tyson SF, Hanley M, Chillala J, Selley AB, Tallis RC. Sensory loss in
hospital-admitted people with stroke: characteristics, associated factors, and relationship with function. Neurorehabil Neural Repair. 2008;22:166–72. 15. Smith DL, Akhtar AJ, Garraway WM. Proprioception and spatial neglect after
stroke. Age Ageing. 1983;12:63–9.
16. Pumpa LU, Cahill LS, Carey LM. Somatosensory assessment and treatment after stroke: an evidence-practice gap. Aust Occup Ther J. 2015;62:93–104. 17. Goble DJ. Proprioceptive acuity assessment via joint position matching:
from basic science to general practice. Phys Ther. 2010;90:1176–84. 18. Lesniak M, Bak T, Czepiel W, Seniow J, Czlonkowska A. Frequency and
prognostic value of cognitive disorders in stroke patients. Dement Geriatr Cogn Disord. 2008;26:356–63.
19. Rathore SS, Hinn AR, Cooper LS, Tyroler HA, Rosamond WD. Characterization of incident stroke signs and symptoms: findings from the atherosclerosis risk in communities study. Stroke. 2002;33:2718–21.
20. Zou G. Sample size formulas for estimating intraclass correlation coefficients with precision and assurance. Stat Med. 2012;31:3972–81.
21. Springate SD. The effect of sample size and bias on the reliability of estimates of error: a comparative study of Dahlberg's formula. Eur J Orthod. 2012;34:158–63. 22. Coderre AM, Zeid AA, Dukelow SP, Demmer MJ, Moore KD, Demers MJ,
Bretzke H, Herter TM, Glasgow JI, Norman KE, et al. Assessment of upper-limb sensorimotor function of subacute stroke patients using visually guided reaching. Neurorehabil Neural Repair. 2010;24:528–41.
23. Kenzie JM, Semrau JA, Findlater SE, Herter TM, Hill MD, Scott SH, Dukelow SP. Anatomical correlates of proprioceptive impairments following acute stroke: a case series. J Neurol Sci. 2014;342:52–61.
24. Otaka E, Otaka Y, Kasuga S, Nishimoto A, Yamazaki K, Kawakami M, Ushiba J, Liu M. Clinical usefulness and validity of robotic measures of reaching movement in hemiparetic stroke patients. J Neuroeng Rehabil. 2015;12:66. 25. Dukelow SP, Herter TM, Scott SH. Independence of limb position sense and
motor impairments following stroke. Stroke. 2010;41:493.
26. Dukelow SP, Herter TM, Bagg SD, Scott SH. The independence of deficits in position sense and visually guided reaching following stroke. J Neuroeng Rehabil. 2012;9:72.
27. Debert CT, Herter TM, Scott SH, Dukelow S. Robotic assessment of sensorimotor deficits after traumatic brain injury. J Neurol Phys Ther. 2012;36:58–67. 28. Taylor M, Creelman CD. PEST: efficient estimates on probability functions.
J Acoust Soc Am. 1967;41:782–7.
29. Deblock-Bellamy A, Batcho CS, Mercier C, Milot MH, Blanchette AK. Robotic assessment to quantify upper limb position sense in patients with stroke: preliminary results. Lausanne: European Congress of NeuroRehabilitation; 2017.
30. Roosink M, Robitaille N, McFadyen BJ, Hebert LJ, Jackson PL, Bouyer LJ, Mercier C. Real-time modulation of visual feedback on human full-body movements in a virtual mirror: development and proof-of-concept. J Neuroeng Rehabil. 2015;12:2.
31. Fournier Belley A, Bouffard J, Brochu K, Mercier C, Roy JS, Bouyer L. Development and reliability of a measure evaluating dynamic proprioception during walking with a robotized ankle-foot orthosis, and its relation to dynamic postural control. Gait Posture. 2016;49:213–8.
32. Elangovan N, Herrmann A, Konczak J. Assessing proprioceptive function: evaluating joint position matching methods against psychophysical thresholds. Phys Ther. 2014;94:553–61.
33. Simo L, Botzer L, Ghez C, Scheidt RA. A robotic test of proprioception within the hemiparetic arm post-stroke. J Neuroeng Rehabil. 2014;11:77. 34. Lexell JE, Downham DY. How to assess the reliability of measurements in
rehabilitation. Am J Phys Med Rehabil. 2005;84:719–23.
35. Atkinson G, Nevill AM. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998;26:217–38. 36. Fleiss JL. The design and analysis of clinical experiments. New York:
37. Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. 2005;19:231–40. 38. Brown JD. Standard error vs. standard error of measurement standard
error vs. standard error of measurement. JALT Testing Eval SIG Newsl. 1999;3:20–5.
39. Lincoln NB, Jackson JM, Adams SA. Reliability and revision of the Nottingham sensory assessment for stroke patients. Physiotherapy. 1998;84: 358–65.
40. Winward CE, Halligan PW, Wade DT. The Rivermead assessment of somatosensory performance (RASP): standardization and reliability data. Clin Rehabil. 2002;16:523–33.
41. Carey LM, Oke LE, Matyas TA. Impaired limb position sense after stroke: a quantitative test for clinical use. Arch Phys Med Rehabil. 1996;77:1271–8. 42. Cappello L, Elangovan N, Contu S, Khosravani S, Konczak J, Masia L.
Robot-aided assessment of wrist proprioception. Front Hum Neurosci. 2015;9:198. 43. Rinderknecht MD, Popp WL, Lambercy O, Gassert R. Reliable and rapid
robotic assessment of wrist proprioception using a gauge position matching paradigm. Front Hum Neurosci. 2016;10:316.
44. Ingemanson ML, Rowe JB, Chan V, Wolbrecht ET, Cramer SC, Reinkensmeyer DJ. Use of a robotic device to measure age-related decline in finger proprioception. Exp Brain Res. 2016;234:83–93.
45. Adamo DE, Martin BJ, Brown SH. Age-related differences in upper limb proprioceptive acuity. Percept Mot Skills. 2007;104:1297–309.
46. Marini F, Squeri V, Morasso P, Masia L. Wrist proprioception: amplitude or position coding? Front Neurorobot. 2016;10:13.
47. Venancio J, Lopes D, Lourenco J, Ribeiro F. Knee joint position sense of roller hockey players: a comparative study. Sports Biomech. 2016;15:162–8. 48. Little CE, Emery C, Black A, Scott SH, Meeuwisse W, Nettel-Aguirre A, Benson
B, Dukelow SPS. Test-retest reliability of KINARM robot sensorimotor and cognitive assessment: in pediatric ice hockey players. J Neuroeng Rehabil. 2015;12:78.
49. Armstrong AD, MacDermid JC, Chinchalkar S, Stevens RS, King GJ. Reliability of range-of-motion measurement in the elbow and forearm. J Shoulder Elb Surg. 1998;7:573–80.
50. Lincoln NB, Crow JL, Jackson JM, Water GR, Adams SA, Hodgson P. The unreliability of sensory assessments. Clin Rehabil. 1991;5:273–82. 51. Dukelow SP, Herter TM, Moore KD, Demers MJ, Glasgow JI, Bagg SD,
Norman KE, Scott SH. Quantitative assessment of limb position sense following stroke. Neurorehabil Neural Repair. 2010;24:178–87.
52. Kalisch T, Kattenstroth JC, Kowalewski R, Tegenthoff M, Dinse HR. Age-related changes in the joint position sense of the human hand. Clin Interv Aging. 2012;7:499–507.
53. Rinderknecht MD, Lambercy O, Raible V, Liepert J, Gassert R. Age-based model for metacarpophalangeal joint proprioception in elderly. Clin Interv Aging. 2017;12:635–43.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal • We provide round the clock customer support
• Convenient online submission • Thorough peer review
• Inclusion in PubMed and all major indexing services • Maximum visibility for your research
Submit your manuscript at www.biomedcentral.com/submit