University of Huddersfield Repository
Rodriguez, Alison
We are here for a good time not a long time: Being and caring for a child with a lifelimiting condition
Original Citation
Rodriguez, Alison (2009) We are here for a good time not a long time: Being and caring for a child with a lifelimiting condition. Doctoral thesis, University of Huddersfield.
This version is available at http://eprints.hud.ac.uk/id/eprint/6963/
The University Repository is a digital collection of the research output of the University, available on Open Access. Copyright and Moral Rights for the items on this site are retained by the individual author and/or other copyright owners. Users may access full items free of charge; copies of full text items generally can be reproduced, displayed or performed and given to third parties in any format or medium for personal research or study, educational or notforprofit purposes without prior permission or charge, provided:
• The authors, title and full bibliographic details is credited in any copy; • A hyperlink and/or URL is included for the original metadata page; and • The content is not changed in any way.
For more information, including our policy and submission procedure, please contact the Repository Team at: [email protected].
‘We are here for a good time not a long time:
Being and caring for a child with a life-limiting condition’
ALISON MARIE RODRIGUEZ
A thesis submitted to the University of Huddersfield in partial fulfillment of
the requirements for the degree of Doctor of Philosophy
The University of Huddersfield
Acknowledgements
I would like to thank all of the professionals, children and parents who took part in this research, for their time, their experiences and their thoughts. I have guaranteed their anonymity so cannot acknowledge them personally, but I hope I have done justice to their accounts.
This thesis has been a journey for me and what I have learnt over the years has been invaluable. Lessons learnt from the participants of this study, the loss of a partner, close family members, and the birth of my gorgeous daughter Iris, have each allowed a more full appreciation of life and of the impact of life-limiting illness. It is all encompassing; relationships change, roles shift, and a sense of meaning and purpose become all the more prominent. Love and happiness take a whole new meaning. These events and related conversations have helped shape my worldview.
I share the following acknowledgements:
~ Professor Nigel King
You are a guiding force. I marvel at your abilities – writing, editing, discussing and developing ideas. Your support and guidance have helped me so much. I hope that in time, I will be able to make such valuable contributions as you have made, to the field of applied psychological research and to the lived experiences of those within it. Thank you, I am indebted.
~ My husband, Yoan.
You have endured many moments and your patience and understanding has persevered. ~ My daughter, Iris.
Thank you for being patient with mummy doing this work. I promise that now I will have more time to play.
~ My Mum.
Thank you for helping me with Iris. Without you helping me with childcare, I would not have been able to complete this work.
~ Antoni, and my good friends Michael, Maryam, Eva, Karen & Eamonn.
You each have watched me struggle, cry, laugh and celebrate through the duration of this work. Your love and friendship means the world to me.
I thank you all for ‘being there’.
Life is what happens to you while you’re busy making other plans
Abstract
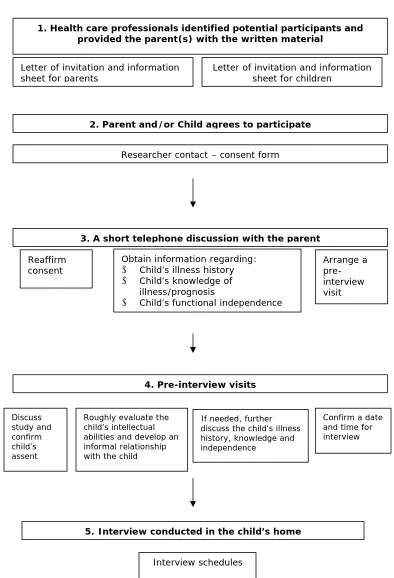
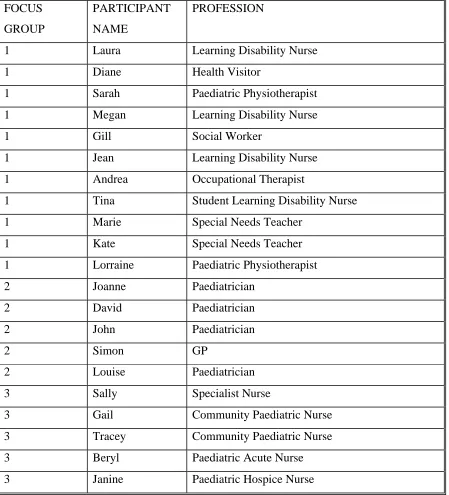
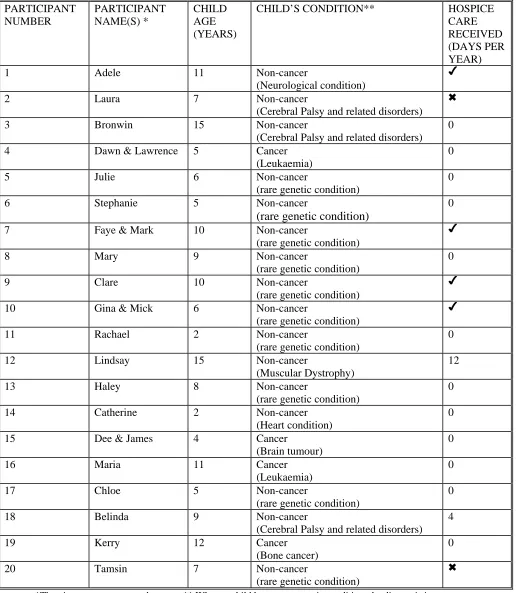
This research project sets out to explore the lived experience of Being and caring for a child with a Life Limiting Condition. This research uses van Manen’s (1990) conceptualisation of hermeneutic phenomenology that is both a research methodology and a method. The first empirical work is a preliminary study using focus groups with professionals. The findings of this work acts as a backdrop to the further two studies that involve interviewing, in-depth, twenty eight parents and five children. The second study details the parents’ lived experiences and the final study looks at five parent-child dyads and their combined lifeworlds. In keeping with the phenomenological methodology, data was analysed using Template Analysis (King, 2004).
It is a rare opportunity to observe and speak with children with Life Limiting Conditions and so gain insight into their lives. Their vulnerability is often characterised by rare and difficult-to-diagnose conditions, significantly shortened life spans with compromised quality of life. For the participants, the experience of Life Limiting illness was not only personal, but was also transactional, communicative and profoundly social. The challenge is one of Being thrown into an abnormal unready world which compels one to consider the paradoxical temporality of the here and now. This brings recognition of being the same as others in a lived space, but also being different in a fundamental way that has a significant impact. The challenge is met by adapting to the environment to find new ways of Being.
Disseminated findings
Papers
1. Rodriguez, A. & King, N. (2008) The lived experience of parenting a child with a life-limiting condition: a focus on the mental health realm. Palliative & Supportive Care. (In press).
Oral Presentations
1. Rodriguez, A. June (2007) A Phenomenological investigation of the lived experiences of children with life-limiting conditions. Postgraduate Research Conference. School of Human & Health Sciences. University of Huddersfield.
2. Rodriguez, A. & King, N. June (2007) The lived experience of children with life-limiting conditions. The 10th Congress of the European Association for Palliative Care. Budapest. Hungary
Poster Presentations
1. Rodriguez, A. & King, N. September (2008) Conducting interviews with children with life-limiting conditions: The methodological needs and nuances. The BPS Qualitative Methods Conference. The University of Leeds.
Contents of Thesis
CHAPTER 1: INTRODUCTION
11
1.1 My interest in the phenomena under study 12
1.2 Issues of definition 14
1.3 Policy 17
1.4 Practice 23
1.5 The structure of the thesis 25
CHAPTER 2: LITERATURE REVIEW
29
2.1 Perspectives on grief 29
2.2 The lived experience of life limiting conditions 37
2.2.1 Children’s understandings of death 39 2.2.2 Communication with children 41 2.2.3 Working with dying children and their families 49
A good death 52
Interactions with families 54
2.2.4 The family’s lifeworld 56
Support 57
Care 60
2.3 Summary and rationale for the current research 62
CHAPTER 3: PHILOSOPHICAL INFLUENCES
653.1 Constructionism 65
3.2 Introducing Phenomenology 66
3.2.1 Intentionality 68
3.2.2 Hermeneutics 69
CHAPTER 4: METHOD
804.1 My approach: Hermeneutic phenomenology 80
4.2 Overall design 84
4.2.1 Samples and recruitment 85
Professionals 85
Parents and children 86
4.2.2 Interview design and procedure 90
Professionals 90
Parents and children 92
4.2.3 Analysis 94
Template Analysis 95
Hermeneutic phenomenological writing 98
4.3 Ethics 100
4.4 Study quality 103
4.5 Conclusion 106
CHAPTER 5: THE PROFESSIONAL FOCUS GROUPS
107
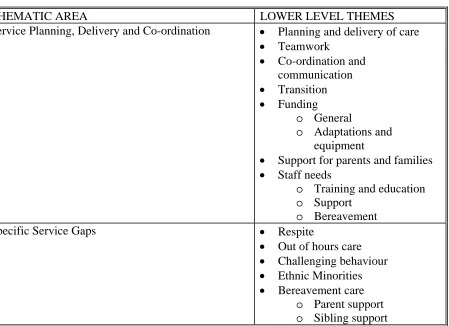
5.1 Overview 107
5.2 Service planning, delivery and co-ordination 109
5.2.1 Planning and delivery of care and teamwork 109 5.2.2 Co-ordination and communication 113 5.2.3 Transition and funding 115 5.2.4 Support for parents and families 121
5.2.5 Staff needs 124
5.3 Specific service gaps 130
5.3.1 Respite and out of hours care 130 5.3.2 Challenging behaviour 136
5.3.3 Ethnic minorities 137
5.3.4 Bereavement care 138
CHAPTER 6: THE PARENT INTERVIEWS
1476.1 Overview 147
6.2 The beginning 151
6.2.1 The diagnosis and its immediate impact 151 6.2.2 New experiences and foci 153
6.3 An inner incentive and drive to provide 155
6.3.1 Maintaining control 155 6.3.2 Parent-professional relations 158
6.4 Trying to maintain life balance 165
6.4.1 Social life and employment 165
6.5 Feeling responsible for others 169
6.5.1 Sibling care 169
6.5.2 Open communication 170
6.5.3 Disrupted family functioning 171
6.6 Psychological effects 173
6.6.1 Social withdrawal 173
6.6.2 Depression, anxiety and fears for the future 175
6.7 Fear of reaching the bottom line 178
6.7.1 Communication with others 178 6.7.2 Struggling to cope and facing the future 180
6.8 Discussion 182
CHAPTER 7: THE PARENT-CHILD DYADS
186
7.1 Overview 186
7.2 The Murphys: Paula and Amy 190
7.2.1 Interview locations and characteristics 191
(i) Tracing the early days 191
(ii) Interactions with professionals 193
(iii) Critical incidents/life events 195
(iv) Issues of appearance 199
7.3 The Thompsons: Sandra and Bobby 201 7.3.1 Interview locations and characteristics 202
(i) Tracing the early days 202
(ii) Interactions with professionals 203
(iii) Critical incidents/life events 205
(iv) Issues of appearance 208
(v) Now and the future 211
7.4 The Burtons: Edward and Sophie 213
7.4.1 Interview locations and characteristics 213
(i) Tracing the early days 214
(ii) Critical incidents/life events 214
(iii) Issues of appearance 218
(iv) Now and the future 219
7.5 The Hills: Maria and Danny 222
7.5.1 Interview locations and characteristics 222
(i) Tracing the early days 222
(ii) Interactions with professionals 223
(iii) Critical incidents/life events 225
(iv) Now and the future 226
7.6 The Roberts’: Gail and Peter 228
7.6.1 Interview locations and characteristics 228
(i) Interactions with professionals 229
(ii) Critical incidents/life events 232
(iii) Issues of appearance 232
(iv) Now and the future 234
7.7 Integrative theme: Protectiveness 237
CHAPTER 8: DISCUSSION OF ESSENTIAL FINDINGS
2478.1 The essential themes 247
8.1.1 Process of developing the essential themes 250 8.1.2 Being normal in an abnormal unready world 251 8.1.3 Paradoxical temporality of the here and now 253
8.2 Reflection on the methodology 256
8.3 Strengths and limitations 260
8.4 Implications 263
8.5 Recommendations for further research 266
8.6 Unique contribution 267
8.7 Conclusion 270
References
272Appendices
1: Membership of academic and research steering groups 291 2: Ethics materials regarding participation in the professional focus group discussions. 296 3: Ethics materials regarding participation in the parent interviews. 304 4: Ethics materials regarding participation in the child interviews. 311
5: The focus group agendas. 319
6: Parent and child interview schedules. 324 7: Outcomes of the consensus conference. 354
LIST of TABLES
1.2: Classification of LLCs in children 15 1.3: Implications/opportunities of the End of Life Care Strategy for children’s
palliative care 20
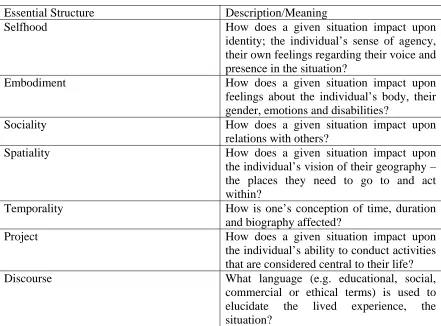
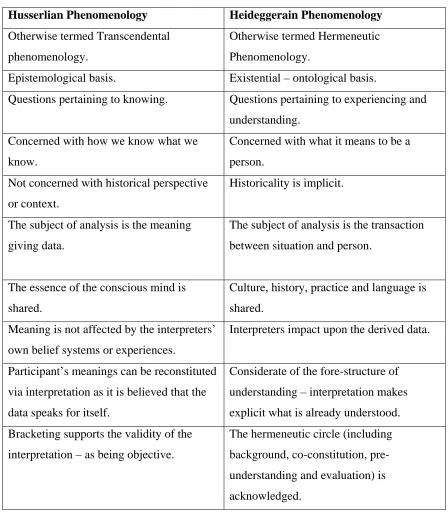
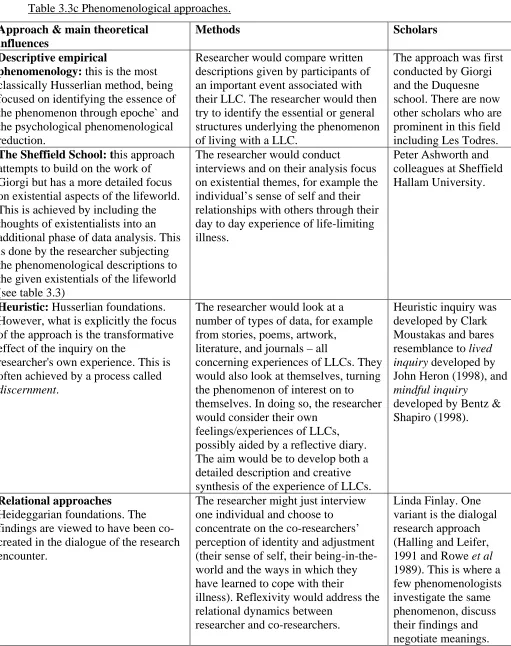
3.3: The essential structures of the lifeworld 72 3.3b: The key practical differences between Husserlian and Heideggerian
phenomenological research 75 3.3c: Phenomenological approaches 77 4.1: Research activities and related thesis parts 82 5.1: Participant characteristics – focus groups 108 5.1b: Summarised focus group coding template 109 6.1: Participant characteristics – parent interviews 148 6.1b: Summarised parent interview coding template 149 7.1: Summary of parent-child dyad analysis template 189 8.1: Poems representing the paradoxical temporality of the here and now 256
LIST of FIGURES
Chapter 1: Introduction
***
life are increasingly beyond my reach and small events assume greater importance: watching a flock of birds preparing to migrate, seeing seeds grow in the garden and experiencing the sun on my face. The progressive nature of my condition has meant that just when I should be gaining independence and control of my life - I am now 22 - I have become more dependent and reliant on other people, mainly my parents, to do everything for me except think, and sometimes they even try to do that for me! (Nick Wallis, ‘My Life Long Desires’ Guardian Newspaper, January 15th, 2007).
The introductory excerpt illustrates how a life limiting condition (LLC) can affect every part of the patient’s life. Wallis (2007) illustrates lived experiences of exclusion, of others ill placed perceptions, of dependence and reliance. But interestingly he also talks of being happy, enjoying life and of appreciating the small things. This short but rich description of Being enticed me into wondering how LLCs are lived in their entirety by children and parents. There is little published qualitative research into the lived experience of life-limiting illness and of parenting a child with a LLC. Therefore, there is also a paucity of material in the literature to which health or social care professionals can turn to, to begin to develop an understanding of the experience. Equally, there is also little for a parent or child to compare their own experience with.
This chapter will detail my interest in the phenomena under study and will set the scene for the thesis. Issues of definition, policy and practice will be discussed, before the structure of the thesis is outlined.
1.1 My interest in the phenomena under study
for her sick child, financially, physically and emotionally. Yet I also saw a woman who displayed incredible strength in a multitude of ways and a child who appeared ‘happy’ irrespective of his condition. Angered at my own ignorance and uncertain what to say, I found myself asking her to tell me what it was like to live with a child who has a LLC. Her words gave me a poignant sense of what it was like: her words framed the impetus for this study.
Well they just say that his care is palliative, its all palliative, I mean they can’t tell me can they, they can’t answer me, I mean nearly every other week they were telling me that he wouldn’t survive another day.
It is argued that we have often failed to recognise the special care that these families need:
Due to the fact that my son’s physical condition started to deteriorate when he was four years old, almost his entire life was a visible expression of that frailty and impermanence. As we lived our different sides of the experience within the family, it was obvious that his physical and cognitive impairments, his final illness and his death were, although unusual, simply one expression of our common human experience…Reflecting Frank’s (1995) description of an ill body as one of essential chaos, my son’s life was rendered completely chaotic and unpredictable as the result of impairment…Living alongside my son as he visibly journeyed from life to death in fifteen years, took me to the centre of life within death and death within life, a paradox we all live with, but spend most of our time in denial of (Murray 2003:523-524).
face social isolation, burnout, mental and physical exhaustion and marriage break-up (Lindesay, 1999).
This thesis provides an exploration of the experience of living with a LLC within the framework of a phenomenological approach. The main aims of this work are as follows:
1. To elucidate the lived experiences of children with life-limiting conditions (LLCs) and their parents.
2. To consider the implications of these lived experiences for health and social care professionals.
1.2 Issues of definition
This area of research has been confounded by problems of definition and the semantics of whether conditions are life-threatening or life-limiting. The latest contribution proposed is that a life-threatening illness is one where there is a possibility that a medical intervention might prove successful (even if the treatment poses a threat to life). LLCs are those for which there is currently no available cure and the condition is likely to lead to the child dying prematurely. In practice, the distinction is often arbitrary since an individual child may oscillate between the two definitions especially during acute exacerbations of the illness, for example in children with cystic fibrosis.
For the purpose of this thesis a LLC is defined as:
Any illness or condition developed in childhood whereby the child is likely to die before adulthood or with a limited expectation of life thereafter. Alternatively, any condition developed in childhood that, without intervention, will cause a child to die prematurely (NHS Executive 1998:5).
adolescence. The needs of children with LLCs and their families are complex and a large proportion have long term needs. Many of the conditions are associated with progressive deterioration, rendering the child increasingly dependent on parents and carers.
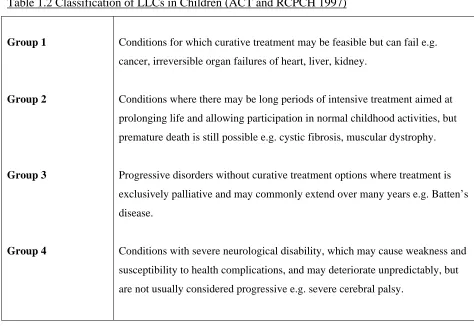
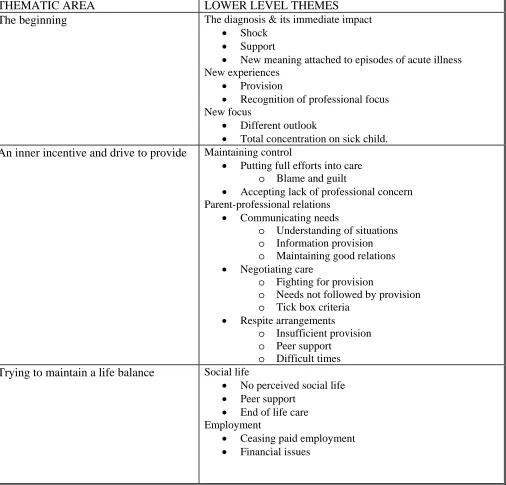
[image:16.612.83.557.263.589.2]LLCs have been classified into four broad disease related groups by The Association for Children with Life-Threatening or Terminal Conditions and their Families (ACT) and The Royal College of Paediatrics and Child Health (RCPCH) (1997) and are detailed in Table 1.2.
Table 1.2 Classification of LLCs in Children (ACT and RCPCH 1997)
Group 1
Group 2
Group 3
Group 4
Conditions for which curative treatment may be feasible but can fail e.g. cancer, irreversible organ failures of heart, liver, kidney.
Conditions where there may be long periods of intensive treatment aimed at prolonging life and allowing participation in normal childhood activities, but premature death is still possible e.g. cystic fibrosis, muscular dystrophy.
Progressive disorders without curative treatment options where treatment is exclusively palliative and may commonly extend over many years e.g. Batten’s disease.
Conditions with severe neurological disability, which may cause weakness and susceptibility to health complications, and may deteriorate unpredictably, but are not usually considered progressive e.g. severe cerebral palsy.
LLC (ACT and RCPCH 1997). Estimates for mortality are based upon a study by While, Citrone and Cornish (1996) who listed LLCs leading to premature death and identified the number of deaths for the period 1989 to 1991 from OPCS data for England and Wales. They reported that approximately 1,100 children die each year from LLCs of which 40% are from cancers, 20% from heart disease and 40% from other conditions. The limitations associated with the reporting and coding of cause of death and differences in the practice of recording the primary cause of death are clearly recognised. Lenton, Stallard, Lewis and Mastroyamopoulou (2001) produced estimates that could be extrapolated to the UK population, but not applicable to many parts of the world where both LLCs and expectations are significantly different.
Children with LLCs are said to have palliative care needs. Palliative care is the holistic care of patients whose disease is not responsive to curative treatments (National Council for Hospice and Specialist Palliative Care Services, 1996). Palliative care was originally synonymous with end-of-life care – typically the adult with cancer reached a point in their disease when active treatment was no longer effective and life expectancy was measured in weeks or months. This approach also worked well for children with malignant diseases. However, there is a far larger group of children with non-malignant diseases whose condition is diagnosed early in life for example, congenital malformations, for which there is no active treatment and death is expected in childhood. It seems entirely appropriate to call the care they require, palliative care, even though it may span a longer period of time. Palliative care for children, centres on the quality of life for the child and provides support for the family, manages distressing symptoms and provides respite and care through death and bereavement (ACT and RCPCH 1997).
designed palliative care approaches support children and families to lead as normal lives as possible.
1.3 Policy
According to the recent Department of Health document: Commissioning Children’s and Young People’s Palliative Care Services (2005); every child with a LLC and their family should be able to access services that:
• Promote their quality of life by managing pain, adverse symptoms and specialist palliative care needs.
• Integrate multi-agency assessment of the child’s needs, involving them and their families as much as they want, in decisions about how their needs could be met in a choice of settings including home, hospital or hospice.
• Are coordinated at the point of delivery across health, social services and education.
• Respond to their changing needs as they move from children’s services to adult services.
• Are delivered by competent staff.
• Are planned in partnership and provided by a network of agencies, including the statutory and voluntary sector.
• Provide information in appropriate formats and language about services and the child’s condition and treatment.
include the public service agreement targets for long term conditions, access to services, and patient and user experience as set out in ‘Improvement, Expansion and Reform: The Next Three Years’ Priorities and Planning Framework, 2003-2006 (2004)’, the ‘NSF for Long Term Conditions’ (DoH 2004), and the forthcoming White Paper on ‘Out of Hospital Care’. Building on the five key outcomes that are set out in ‘Every Child Matters: Change for Children’ (2004) and ‘The Children Act’ (2004), Standard 8 of the Children’s NSF expects high quality palliative care to be available for all children who need it.
Partnership working is considered to be crucial and is a core principle in the following key policies:
• Every Child Matters: Change for Children agenda (DoH 2004)
• The NSF for Children, Young People and Maternity Services (DoH 2004)
• Making it Better for Children and Young People (DoH 2007)
• Aiming High for Disabled Children (HM Treasury/Dept of Education and Skills 2007)
• The Children’s Plan (Dept for Children, Schools and Families 2007)
In addition, ‘Better Care: Better lives’ (DoH 2008) published in February of 2008, builds on the ‘Palliative Care Services for Children and Young People in England’ report that was published in May 2007. The report was the result of an independent review of children’s palliative care services which involved wide ranging consultation. The 2008 document is considered to be the next step in encouraging change. There are three aims:
1. To highlight key aspects of the independent review
2. To challenge and inspire local commissioners to prioritise the needs of this patient group
To try and ensure children’s palliative care services are given priority and planned well, the following eight goals are put forward by ‘Better Care: Better Lives’:
1. Improved data
2. Equality of access to universal services 3. Responsible and accountable leadership
4. Choice in preferred place of care and widening of community services 5. Better end of life care
6. Stronger commissioning and value for money
7. Successful transition between children’s and adult’s services 8. Planning and developing an effective and responsive workforce
Phase two has been planned and will take the title of ‘The Children’s Palliative Care Project’, whereby support materials will be developed and road show events organised throughout the country. This will be to publicise the strategy and to help localities to develop their own strategies for delivery.
Table 1.3 Implications/opportunities of the End of Life Care Strategy for children’s palliative care (adapted from ACT briefing for
members, July 18th 2008).
Strategy point Meaning for children’s services? Linkage to ‘Better Care:
Better Lives’ (BCBL)
Way forward
Differences are highlighted re:
place of death between age groups
• Those dying in young adult life
(15 – 44) or in the middle years
(45-64) are more likely to die at
home.
• Children and people aged 75-84
have the highest in-patient death
rates.
This point identifies discrepancies
across the age ranges. Is it the case
that more young adults are able to
die at home because district nurses
are more accessible for support in
the home, alongside specialist nurses
for example Macmillan and Marie
Curie nurses?
Is it the case that more children die
in hospital because community
services are inadequate to provide
support? Or is it because it has been
the family’s choice for the child to
die in hospital?
BCBL suggests that
community services are
developed to support
children and young people
away from the hospital
setting e.g. home or
children’s hospice.
Survey what services are available
that provide home/community care
to children and young people with
palliative care needs.
Determine if workforce
development plans are aiming to
look at the staffing numbers needed
to provide 24 hour support and care
to children and young people with
palliative care needs. Do these
plans also look at the needs of the
non-statutory sector? Are there any
education and training plans a foot
to ensure staff are appropriately
Strategy point Meaning for children’s services? Linkage to ‘Better Care:
Better Lives’ (BCBL)
Way forward
Because medical care has advanced
many of children and young people
with LLCs who need palliative care
are living for longer periods and
can achieve a good quality of life if
they and their families are well
supported by services. However,
the support they require is complex
and as such a lot of careful planning
is required by commissioners when
considering transition to adult
services and in planning end of life
care services.
It is expected that children’s, young
people’s and adult services will
consider the needs of young people.
BCBL outlines a key
objective – that transition
from children’s to adult
services is planned and
purposeful for young
people with LLCs.
Determine who leads on children’s
palliative care in the local Primary
Care Trust (PCT).
Determine who leads on end of life
care in the local PCT.
Determine how transition is being
viewed by commissioners and if
young people with palliative care
needs are being considered in any
work on transition and end of life
Strategy point Meaning for children’s services? Linkage to ‘Better Care:
Better Lives’ (BCBL)
Way forward
The bereavement needs of children
and adolescents should be
acknowledged and information and
support provided that is aligned
with their development and level of
understanding. Staff need to know
that adolescents may wish to be
totally aware of all the processes
surrounding death and their
parent(s) or guardian(s) will require
support to understand this need.
In addition, where a child or young
person has been a caregiver in the
home, this role should be
acknowledged and respected at the
time of death and in planning post
death arrangements.
Is it possible for children’s services
to share their bereavement expertise
with adult services to develop local
response to need?
Not really considered by
BCBL. However, there is
recognition of the needs of
siblings when looking at
overall need for
bereavement support.
Determine what services are
provided in the area.
Look at forging links with other
providers to maximise local
bereavement services that can be
offered.
In addition, the UK government has introduced a number of policies directed at improving support given to carers. The Carers (Recognition and Services) Act (Department of Health 1995) acknowledged carers’ rights to have their needs assessed. The National Carers’ Strategy (1998) set forth a process of consultation intended to determine strategies for addressing carers’ needs, leading to the strategy document
Caring about Carers (Department of Health 1999) and the Carers and Disabled Children Act (Department of Health 2000). Both the Health Act Partnership in Action (Department of Health 1998) and the White Paper Valuing People (Department of Health 2001) highlighted pooling of budgets and integration of services in order to facilitate better services for carers (Walker & Dewar 2001; Read 2002). The importance of effective, joined-up multiagency provision of services has long been recognised as important for disabled children and their families. The many issues identified in the literature have been recently reiterated in the report of the external working group for disabled children, as part of the Children’s National Service Framework (Department of Health 2003). One specific group of these children has recently become the focus of interest – namely those children with LLCs, with a recent investment of £48 million from the New Opportunities Fund to develop children’s palliative care services (Lenton, Franck & Salt 2004).
1.4 Practice
In the UK there are several different models of delivering palliative care to children, which have developed separately but are now increasingly working together (Hain 2002):
• The outreach model – a disease based approach, comprising paediatric outreach nurses liaising with a specialist paediatric consultant. This model is typified by paediatric oncology services, and increasingly emulated (for example by neonatal and respiratory teams).
• The community nursing teams – these liaise where necessary with paediatric consultants. These teams can have a particular role in the care of many children with non-cancer LLCs.
Indeed, care for children with LLCs is delivered in many forms in all areas of the UK. The growth of services has traditionally been based on local interest and the availability of charitable funds. The heterogeneity of the patient population makes flexibility a key feature of any service and care for children with LLCs. Similarly, the complex needs of each family are unlikely to be met by a single service, which makes co-ordination of a number of different services and professionals an important element of care (Hynson and Sawyer 2001).
ACT and RCPCH (1997) made comprehensive recommendations for service development in relation to the care of children with LLCs. In addition to general legislation and government policy, their guidelines identified baseline principles to underpin service development. These included:
1. Joint planning and commissioning between health, social and education providers 2. Flexibility and choice for children, parents and families
3. Child/ family centred care 4. Continuity of care
5. Staff with training and expertise 6. Transition to adult services.
devise care plans based on limited experience and evidence. Good quality community care for children with complex healthcare needs should not only meet the medical and technological aspects of care, but also focus on enhancing the quality of life (QoL) for the child and providing support for the family (Abu-Saad 2001).
Few robust clinical studies have been conducted in this area because of the complexity and rarity of many conditions, the many variables involved with these vulnerable children, the difficulty of assessing children with communication problems, and the many ethical dilemmas around researching the patient group. The research agenda is broad and covers many different areas (Edmond and Eaton 2004), and despite the increasing number of studies and policies related to improving supports for parents who are carers, the acquisition of accessible and appropriate respite services remains problematic (Sloper 1999). This in turn raises further questions about the nature and type of provision required by children and families who have a long term condition and the interface between disabled children’s services and palliative care services.
1.5 The structure of the thesis
To elucidate the lived experiences of children with LLCs and their parents, this research uses van Manen’s (1990) conceptualisation of hermeneutic phenomenology that is both a research methodology and a method. In the context of research methodology, hermeneutic phenomenology refers to a certain theoretical philosophical framework in
‘pursuit of knowledge’ (van Manen 1990:28). The methodological premise of van Manen advocates the philosophical belief that human knowledge and understanding can be gained from analysing the prereflective descriptions of people who have lived the experience in question. In other words, the essence of the phenomenon is uncovered by gathering text from those living it and then interpreting this text.
in investigating how different people, in the context of particular individual and societal life circumstances, set out to make sense of certain aspects of human existence and the interpretations that are made of those existences (Heidegger 1962). Far reaching travels, lengthy home visits, in-depth conversations, extensive note taking and reflective practice were other central elements of the research method and my development as a qualitative researcher. It is a phenomenological study in which lived experiences of the world of everyday life are the central focus, and an idea that will be discussed extensively in the methodology chapters (Chapters 3 and 4).
Life-limiting illness will be explored by examining the views of professionals via three focus groups and then by interviewing in-depth twenty eight parents and five children. The children and parent participants will be questioned with regard to their understanding of their world through expression of their thoughts and perceptions. In doing so, I follow van Manen’s methodological research approach in which human situatedness is placed centrally, based on the belief that human beings and the meanings they assign to their experiences can be best understood from the experiential reality of their life worlds (van Manen 1990). This means that the voices of participants are incorporated in the research to provide a description of life-limiting illness as it frames their lives.
Chapter two details the literature review. Here, the background issues to the phenomena under study are addressed. The literature review draws on research within chronic illness, disability and life-limiting illness and the possible impact on families is highlighted. The chapter culminates with a summary outlining any presuppositions’ gained from the literature, detailing current gaps in knowledge, the main research aim and questions of the current study.
demonstrated that through phenomenological thinking, it is possible to understand such experiences and therefore, subsequently, to act effectively in our dealings with people. I will detail the way in which the methodology, positioned within the interpretivist approach, was developed to draw out the intricacies and intimacies of the lived experience.
Chapter four outlines the research design and the methods conducted in this study, by detailing theoretical and practical procedures. It describes the data collection techniques – focus groups and interviews and outlines van Manen’s (1990) phenomenological approach as combined with King’s (2004) Template Analysis – used to organise the findings. This chapter also details the ethical issues of the study and how they were dealt with.
Due to the scale and complexity of the research findings, three chapters are dedicated to their description and discussion:
• Chapter five details the professional focus groups study – three focus groups were conducted with a number of professionals from health and social care backgrounds. These findings provide a backdrop to the lived experiences of children with LLCs and their parents.
• Chapter six details the parent study - here the focus is on a number of interviews conducted with parents whose children were not interviewed.
• Chapter seven details the parent-child dyads study – here I look at data gleaned from parents and their own children.
Chapter 2: Literature Review
***
When a child dies in a children’s ward…. There is a whispering and a scuffling behind the scenes, a furtive moving of white covered trolleys in and out of the ward, usually during the night. Nurses and doctors are pre-occupied and do not answer questions and are unduly irritable. Above all, there is a stupid pretence that nothing unusual is happening… but do we really think that the ‘secret’ is not known to every child on the ward? (Yudkin 1967, cited in Judd 1996:40).
Have things changed? Over forty years on and with the introduction of palliative paediatric care, one would expect that there now is a greater professional awareness of the impact of a LLC on children and their families. Hopefully, the day to day lives and experiences of those facing premature death are more supported by systems of care, and are less taboo subjects for all.
This literature review will evaluate the research to date which holds resonance with the lived experience of LLCs for ‘the professional’, ‘the parent’ and ‘the child’ and will build a rationale that advocates the phenomenological study of professionals, parents and children to elucidate the richness and complexities of their lived experience of LLCs.
2.1 Perspectives on grief
Interestingly, many professionals and the general public continue to understand grief and bereavement as linear and time bound. For example, recently I accessed a number of cancer and bereavement related charity websites to find advice that was attuned to Kubler-Ross’ (1969) model of grief.
However, the linear models of grief and their related concepts have been questioned by some clinicians and theorists (Cowan & Murphy, 1985, Worthington, 1989, 1994). Questions have been raised particularly in relation to the length of time considered to be ‘normal’ to continue grieving, and there have been queries centred on the assumption that failure to achieve resolution of grief is abnormal. Indeed, the five-stage model attributed to Kubler-Ross that was actually evolved from individuals facing their own death, not grief from bereavement - is not fully supported by research and has been labelled superficial, inadequate and misleading my some authors (Corr, 1993). During the 1970s the model of dying was morphed into a model or stages of grief. This may have been a result of its prominence in undergraduate sociology and psychology courses and Kubler-Ross’ use of non academic language which made the model easily accessible to the media and general public (Friedman & James, 2008). Accordingly, there have been no real world examples of the existence of stages, or any evidence that suggests people actually move from stage one through to stage five. Instead, it is argued that humans cope in many ways, not just these ‘five’ and there also appears to be no prescribed or necessary ways in which people should cope with death and dying. Just as there is no ‘right’ or ‘wrong’ way to die. Instead, coping with dying is a richer and more complex process than merely progressing through certain ill-defined stages. Indeed, Kubler-Ross herself in her opening paragraph of ‘On Grief and Grieving’ (Kubler-Ross & Kessler, 2004:1) states:
There is however, some empirical research to support a dynamic conceptualisation of grief. If anything is conceptualised as dynamic, this means that interactions are multiple and multiply connected. Furthermore, it is the multiplicity of the interactions through time which produces effects. In other words, grief cannot be meaningfully reduced to single or limited numbers of factors or variables (Bogg & Geyer, 2007). In a study by Cowles (1996), focus group participants from a variety of cultural backgrounds in the United States were asked to draw on their own personal experiences of grief. Their definitions of grief were similar to those in the professional literature. Irrespective of their culture, they viewed grief as a dynamic, all encompassing and highly individualised process. Participants agreed that culture or cultural background is a key component of the ways in which people respond to actual or potential health problems. They also believed that, though mourning rituals or traditions may be culturally defined and prescribed, each person experiences grief in his or her own way. In addition, grief happens to everyone and in different ways and across all age groups. The participants discussed their own grieving and experiences of how others have responded to death differently within their own culture. As a result, they were not judgemental about others’ experiences of grief. Others’ experiences were viewed as just different, not as wrong or pathological in any way. Most participants stated that the progression of grief is unpredictable and that changes over time vary. In addition, it was argued that grief does not necessarily have a particular end point. Indeed, the bereaved may continue to grieve for many years.
addressed this phenomenon for parents and children. Although, where parents have been satisfied with end of life care after they have lost their child, their grief response is in fact less severe than those who were not satisfied with end of life care (Seecharin, Andresen, Norris & Toce, 2004). As a result, Carter & Levetown (2004) advocate that bereavement interventions commence prior to a death of a child. However, one difficulty with the concept of anticipatory mourning is that it leads to the assumption that an expected death is easier to deal with than an unexpected death. Many clinicians have observed that, despite education around anticipatory mourning, families are rarely prepared for the reality of their child’s death. Davies (1993) noted that parents and siblings, who have accepted the inevitable outcome of the child’s illness, often talk about the death in less logical terms such as, ‘But I didn’t think he would die until he graduated’ or ‘I thought he would wait until I got home from school’ (p.141).
In summary, at the most obvious level, scientific studies have failed to support any real world sequence of emotional phases of adaptation to loss or to identify any clear endpoint to grieving that would designate a state of ‘recovery’. Neither is it clear that a universal or normative pattern of grieving exists that would justify the confident diagnosis of symptomatic deviance from a healthy grieving template as grief that could be labelled ‘disordered’ or ‘pathological’. More interestingly, some critics of linear or stage models have started to focus on the ways in which such indirectly disempower the bereaved and care givers by their indication that grieving people must pass through a sequence of psychological transitions that are a result of external events. They have queried the inference that emotional states should be of most relevance in theories of grieving, and as such they appear to marginalise both meanings and actions of individuals (Friedman & James, 2008). Finally, some theorists have begun to question the individualistic nature of traditional theories, which construe grief as an entirely private process, inconsiderate of the context of human relatedness (Neimeyer, 1998).
meaning of loss in human experience. These theories share key elements. They are sceptical about the universality of an expected emotional trajectory that ensues from psychological imbalance and leads on to readjustment. These theories have a greater appreciation of more complex patterns of adaptation. They are moving away from the ideology that ‘successful grieving’ happens once the bereaved removes their mental attention from the person who has died, and instead focuses on the potential mental well being that can evolve from having potentially continued symbolic bonds with the deceased person. This is a very important shift as it counters the dominant ideology since Freud.
Contemporary psychoanalysts, especially those who work from object relations theory, self psychology and relational psychoanalysis have moved on from Freud’s psychological model of instinctual energy and isolated mental functioning. Mitchell (1993) highlights the move to accepting life as being fundamentally embedded in relationships and interpersonally oriented meaning. Psychological life is no longer viewed as private or predicatable and as such many long held beliefs are being reconstructed (Stolorow & Atwood, 1996). As a result, many theorists are questioning the standard Freudian model of mourning and its key characteristics (Gaines 1997, Hagman 1993, Kaplan 1995, Shane & Shane 1990, Shapiro 199, Shelby 1994). In his work ‘Detachment and continuity: The two tasks of mourning’, Robert Gaines (1997) stated:
Emphasis on the need to detach from the lost object has obscured another aspect of the work of mourning, which is to repair the disruption to the inner self-other relationship caused by the actual loss… this is the task I call “creating continuity” (p.549).
Grief is resolved through the creation of a loving, growing relationship with the dead that recognises the new psychological or spiritual (rather than corporeal) dimensions of the relationship (p.552).
A fundamental argument of these new psychoanalytic and constructivist models (Neimeyer, 1998) of mourning is the need to maintain the attachment to the deceased, and the importance of maintaining a sense of the meaningfulness of the relationship that survives the loss. Kaplan (1995) commented on the importance of keeping the dialogue going with the deceased and has stressed the role of ‘creating continuity’. In addition Shapiro (1994) has discussed the social factors that can maintain the connection and Hagman (1995) has discussed the transformation and internal restructuralisation of the attachment to the deceased person.
These models appear to be more attentive to broad cognitive processes that are entailed in mourning, thus supplementing the traditional focus on the emotional consequences of loss. They de-emphasise universal syndromes of grieving and instead focus on ‘local’ practices or cultural variations in accommodating loss. They argue for a greater awareness of the outcomes of major loss, in terms of the individual’s identity, and for an understanding of how the bereaved may come to re-define themselves and they also have an increased appreciation of the possibility of learning and developing through loss. These approaches also have a broadened focus. They are not just interested in individual survivors but also how grief is negotiated within families and wider social forums. A further prominent theme in these newer theories is their insistence that meaning reconstruction in response to a loss is the central process in grieving (Neimeyer, 1998).
coping and positive affect are a result of ‘positive reappraisal’, a so called cognitive reframing of an experience to be able to view it in a more positive way. In her revised model, she talks of this reframing as a characteristic of meaning based coping, but stresses that further research is needed to explore the content and specific meanings attributed to experiences and how these occur over time.
In line with this new understanding there are a number of changes in clinical practice:
1. Each person’s response to bereavement is unique, and what is normal and what is pathological must be considered in the context of the patient’s specific personality, relationship to the deceased person, and his or her familial and cultural background. Openness to psychological individuality and a willingness to explore the unique bereavement response of the patient is crucial.
2. What therapists call ‘pathological responses’ may be unsuccessful strategies to maintain meaning and preserve the attachment to the lost object. Treatment requires not relinquishment but an exploration of the continuing value of the attachment to the survivor, with a consequent reconstruction of the meaning of that person in the context of the survivor’s ongoing life.
3. Bereavement results in a crisis in the meanings by which a persons life is given structure and substance. Therefore, pathological grief is meaningful, however disturbed and painful it appears.
5. Mourning is fundamentally an intersubjective process, and many problems arising from bereavement are due to the failure of other survivors to engage with the bereaved person in mourning together. (Hagman, 2001:25).
2.2 The lived experience of LLCs
Children with LLCs face an untimely death, but as highlighted in the introduction to this thesis, children are now living longer with their LLCs than ever before, due to medical and technical advances in care. However, these positive outcomes related to increased lifespan create other issues that impact on lived experiences and care, for example:
• How does the child perceive their LLC?
• Do they realise their condition is palliative?
• Does their stage of development impact upon their understanding of death?
• How do parents and professionals recognise different developmental needs and the concerns an individual child may have?
• To what extent should the child have a say in any treatment/palliative care decisions?
• What happens when a child may wish to know more or less than what the parent desires them to know?
• How do parents cope with the uncertainty of the LLC?
These issues alone make it apparent that the palliative care of paediatric patients can be far more complex psycho-socially than for adults. It is now forty years since physicians, lead by Dame Cicely Saunders, recognised the particular needs of the adult patient and their families with incurable disease, but it seems to have taken much longer for these needs to have been recognised by paediatricians and policy makers - regarding children.
achieve a better understanding of the reality of their life worlds. Here, we can draw on existential psychology which is grounded in a rich philosophical history. The tradition argues that human beings have a unique capacity that allows them to choose to become aware of and responsible for their own existence or Being in the world. Key existential themes include human freedom (Sartre, 1956), agency and responsibility (Heidegger, 1962, Levinas, 1969), self-transcendence (Frankl, 1992), and the quest for meaning (Frankl, 1961, 1988, 1992), and they each have significance when a person has to come to terms with life while confronting imminent death.
There is no greater existential crisis than that of facing one’s own death or the death of your child. Existentialism is based on the fundamental premise that human beings have the capacity to question and reflect upon their own existence, that is, ‘to be or not to be’ (Heidegger, 1962). As such, we are cognitively aware of our existence, as well as of our potential for nonexistence. The ways in which individuals live their lives in the face of such uncontrollability, creates the basis for existential psychology. Issues of interest within existential psychology include patient anxiety (for example, Heidegger’s (1962) notion of ‘existential angst’ as ‘being-toward-death’), guilt (for example Heidegger’s (1962) notion of ‘indebtedness to being’) and denial (for example Sartre’s (1956) notion of ‘bad faith’). Indeed, trying to find meaning (Frankl, 1992) and reasons to be alive become pivotal existential resources for helping patients come to terms with their past and their present, and to accept an uncertain future.
2.2.1 Children’s understandings of death
Patterns of understanding in children are fluid; children’s individual experiences, environment, including family environment, their intellectual capacities, their emotional profiles, ethnic, cultural and religious backgrounds – all contribute to how and when they come to fully understand the meanings of their illness and untimely death. What developmental theories have in common is the recognition that a child learns first that death occurs and then that it is both irreversible and inevitable, the child finally becoming concerned with details, such as physical changes. What the theories fail to acknowledge however, is the impact of life events on development, including life-limiting illness itself. It is argued that, a cognitively aware child with a LLC will typically acquire a precocious understanding of illness and death. However, to reject the contribution of psychology would mean explanations of childhood were completely social (Faulkner, 1993).
view children as reflexive – they can be critical and creative, actively monitor situations and people and as a consequence of their experiences and accrued knowledge, they go on to modify or reject norms. Thus, we may find that children with LLCs do not adhere to pre-defined stages of cognitive development (Piaget 1960) and that their understandings of their illness and death and dying may not be aligned to the biological age or assumed level of cognitive development (Morss 2002).
adolescence, children are thought to be fearful and troubled about death, which they often see as cruelly unpredictable. However, they can also be logical and consistent; they can spend time thinking about the meanings and impact of death and how they think death will affect those around them. We are also aware that through adolescence, young people can develop a careless attitude towards their well-being and take on risky behaviours, as if to defy the reality of death. At this age, they can be openly angry and express that anger through refusal to adhere to their treatment regimes. They may also struggle with major issues of their identity in the face of their sudden shortened future (Stillion & Papadatou 2002).
In accordance, Michelson & Steinhorne (2007) argue that to address the psychosocial needs of children with LLCs, we must still consider the child’s developmental level. Infants and children with limited verbal ability and no concept of death depend upon sensations and a physical relationship to their surroundings. Being held, comforted, and soothed provides much of their support. In the preschool years, children may benefit from clear, unambiguous explanations about what is happening to them. In the primary school years, important interventions could include supporting a child’s efforts to understand the situation, letting the child have control where possible, and allowing the child to participate in medical decisions when appropriate. For adolescent patients, reinforcing self esteem, respecting privacy, and again allowing participation in medical decisions are important aspects of care (Michelson & Steinhorne 2007).
2.1.2 Communication with children
their illness, prognosis, and concerns seemed less anxious than children who were deprived of this opportunity.
Interestingly, Richard Lansdown, a doctor at the great Ormond street hospital for sick children in London was interviewed by Dorothy Judd (1996) about his views on children’s attitudes to death. At this time he had worked with dying children for over twenty years. With this wealth of experience, I find his comments insightful and they appear to be more in line with the social constructivist’s take on psychological development:
with cancer, because there’s such a taboo about the subject. Well, I think you’ve got to be much more sophisticated than either of those views, and take your cue from the children’s understanding. What really counts is when the child sees another child dying. It is crucial when a child knows of another child who has died of the same condition… children may be told that they may die. Their parents may say to children, ‘if you don’t take your medicine, you will die’, but children also hear mum saying, ‘if you don’t tidy your bedroom, I’ll kill you’, and she doesn’t really mean that. And granny talks about ‘I’m dying for a cup of tea’, but she doesn’t really mean that either. But when Elizabeth in the next bed dies of leukaemia, and she’s got leukaemia like I have, then that really does hit me in the guts. That is a crucial time, a turning point in children’s development and understanding of mortality (p.41-42).
Judd continued to ask Lansdown if he thought all children have the same sense of the seriousness of their illness. He stated that he did not feel they did. He admittedly contradicted the literature and in particular the work of Bluebond-Langer (1978), in referring to a number of children he had cared for. He argued that many children have an unconscious fear of dying, which they would deny if you talked about it to them. What he thought was key to a child’s awareness of their terminal illness, was whether they had been an inpatient or not, and if they had experienced the loss of other children. As a result, Lansdown said that he was very wary of adopting a generalised practice suggestive of ‘all children know this, all children believe that’.
discussion but these are maybe better recognised by the more experienced practitioners (Faulkner 1993).
Clarke, Davies, Jenney & Eiser (2004) investigated the issue of how and what to communicate to children with Cancer about their condition. The professionals in this study found that many parents find decisions about what to tell their child with cancer difficult. Although there is evidence in practice of the complex nature of this issue and how perhaps an approach to fit all is not appropriate, in this study it was found that open communication was generally considered the best policy and most health care professionals actively encouraged parents to talk openly and honestly about the illness with the child. But one then questions to what extent there are formal support mechanisms in place for parents and if not to what extent professionals have the time to support parents through this process. Interestingly, however, parents in this study differed in their perceptions in terms of what they thought they should convey to their child. In this study fifty five parents of children (thirty six boys and nineteen girls, mean age was seven years) newly diagnosed with acute lymphoblastic leukaemia (ALL) were interviewed about:
1. How the child reacted following diagnosis 2. Their views about what to tell their child
3. Factors influencing communication with their child.
In other studies, the pivotal role played by health professionals in promoting partnership and negotiation in communication is critical to families in coming to terms with their child’s diagnosis, prognosis and associated health needs (Callery & Smith 1991, Casey 1995, Coyne 1997). Coupled with this, there is a developing interest by doctors in the bio-psychosocial model of health (Ong, DeHaer, Hoos & Lammes 1995) which predicates a shift from an authoritarian and paternalistic relationship between doctors and parents to one which, more like nursing, values and promotes partnership and negotiation in healthcare. Thus, there is very much the scope now for professionals to tailor the care to the needs of families and for families to lead decision processes (Sharp & Strauss 1992, Eiser 1993, Eiser, Havermans & Eiser 1995, Fairhurst & May 1995). In addition, health policy makers are being urged to ascribe a higher status to children and parents and to incorporate their views into the formulation of strategies (Aynsley-Green, Barker, Burr, Macfarlane, Morgan, Sibert, Turner, Viner, Materson & Hall 2000).
For many dying children it is argued that their primary concern is to have their parents near but to also be able to communicate their thoughts and fears with others (Liben & Goldman, 1998). These two needs can place contradictory pressures on children. At home they are assured of the presence of their parents which helps to reduce a sense of abandonment. At the same time, care at home may give children fewer opportunities to explore the very issues they may sense are ‘off-limits’ for their parents. To maintain open communication is then very challenging. With children dying from cancer, it has been found that there is a kind of ‘mutual pretence’ where, in order to protect their parents, children allow them to decide and set limits on open discussion about illness and death. Another aspect that may limit communication is chronic and severe pain for a child, making it extremely difficult to actually articulate their feelings (Savins 2002).
impact on the grieving process, by leaving a sense of unfinished buisiness. However, communication is more than just speech. Non-verbal forms of communication can also be highly relevant such as tone of voice, posture, mood, touches, hugs, lap sitting, as they all offer an enriching and vital context for a child. Recognizing a child’s non-verbal cues can be vitally important. Expressive therapies such as drawing, art, music, puppetry, story-telling and drama can help children to explore issues around their deaths, to express their thoughts and feelings, anger, fear, loss of hope and so on as well as their unmet needs. There is also a strong case for using drawing with both dying and grieving children (Wellings 2001). Younger children with fewer verbal skills can express themselves through drawings and these can help family and carers to understand the child’s world view. For older children, the internet and e-mail are resources whereby they can share their experiences with others in a similar situation. There is also the growing reality that children with LLCs are living longer into adolescence and young adulthood and need current support to help them in their realistic assessment of all their premature death means to them (Clatworthy, Simon, & Tiederman 1999).
easily be neglected and its value dismissed because the child has no long term future, a decision that may be especially prevalent in social care systems that are financially deeply constrained. This would be to ignore the extent to which education and play give children a sense of normality and continuity. It can also give them a sense of purpose and permit them to develop short term goals. There is a large body of evidence suggesting children have high resilience, that they are able to draw strength from their experiences and successfully integrate themselves into society (Zani 1995).
In addition, children value choices but they need to make choices within safe boundaries. Attig (1996) argues that including children in decision-making about treatment options, symptom control, and so on helps them to shape their daily lives and can substantially reduce reactions of helplessness and powerlessness. It is important for them to be given full opportunities to try and understand all that is happening to them: they need to be encouraged to express their feelings appropriate to their levels of development. Children also need honest communication: answers to their questions and someone to listen to their fears. Children are perceptive and often understand verbal and non-verbal cues better than professionals and families realise (Goldman 1996).
There is surprisingly little literature on how children cope with hospitalisation and how they are affected by it. Experiencing hospitalisation may weaken children’s coping capabilities (Spirito, Stark & Gill 1995), but this could be influenced by the nature of the experiences. Having accurate information about what hospitalisation entails is associated with less distress (Siegel & Weinstein 1983). However, how far children experience problems during and after hospitalisation may be explained by prior functioning (Siegel & Weinstein 1983).
years. Expressive play with art and music may be helpful in encouraging children to share their fears and feelings (Gray 1998). Children seven to twelve years of age may fear abandonment, destruction, and body mutilation. It is suggested (Stevens 1993) that they need people to be truthful with them and to foster their sense of control over their deteriorating body. Friends are also important to children of this age and it is argued they should be encouraged to visit. One of the tasks of adolescence includes separation from parental control. Adolescents often struggle with the paradox of wanting support and yet wanting to meet challenges by themselves. They may prefer to talk to and confide in a peer group, especially with others in a similar situation. As with younger children, adolescents may be more concerned about their family and friends than about themselves. They tend not to be afraid of death so much as afraid of dying. Professionals are therefore encouraged to listen carefully to understand the adolescent’s perceptions of their own illness and prognosis, as advocated by Lansdown (1996) previously. Privacy and a sense of independence are also important to an adolescent, as is peer contact and support. Offering choices may also give adolescents a sense of being in control, and may reduce anger, frustration, depression and anxiety. Creative tasks such as writing poems, letters or a journal or drawing have been shown to release pent-up emotions. In addition, many adolescents want to know that they will be remembered. Creating a permanent record to leave behind, such as a video, tape or photograph, may be valuable (Stevens 1993).
2.2.3 Working with dying children and their families
In her book ‘Give sorrow words: working with dying children’ (1996), Dorothy Judd includes diary excerpts of her work as a psychotherapist (spanning three months) with a seven year old boy. The excerpts are an illustration of how emotionally involved professionals working with children with LLCs can be. Dorothy details how she tried to keep her emotions under control and highlights the difficulties in knowing what to say to both child and family when one knows that the child is dying, despite her expertise. Leading up to the given excerpt, she details the child patient ‘Robert’ undergoing a bone marrow transplant, using his father’s marrow. Afterwards barrier nursing is employed and continued even in times where there appears to be little hope. ‘Robert’ then goes through very dramatic bodily changes, and his parents struggle to cope with this. In addition, Judd observes how Robert appears to cope with his anxieties, his pain and frustrations. The three months cited are three months of this child slowly dying; for a person outside of this life world, the account is difficult to read as it is written with such illuminating prose. To illustrate:
p.121 (23rd October):
with what feels like the more important removal of an emotional barrier between us. I stay a little while quietly by him. He has hardly opened his eyes since his mother left. I feel he reserves that way of actively ‘holding on’ with his eyes for when she is in the room. I say goodbye and mention to him that we can carry on with the story book next time… later in talking to one of the sisters she expresses her upset at ‘the grotesque appearance’ of Robert. ‘Bloated, absolutely awful, absolutely horrendous’. She says ‘and he is conscious of what is happening to him, and so aware that his body is not functioning properly’… I feel relieved that this sister, with her many years of experience of this work… is also in touch with what we agree is ‘torture’.
Robert died on 17th December, having been able to communicate up until that very day.
p.158-160 (17 December):
pyjama top he wore before he became desperately ill… Outside the hospital, the darkness of the night is regaled by the Christmas lights. I curse the Christmas trees and the Christmas lights… Later, at home, I feel the need to care physically for my healthy seven year old. I look at him, stretched out in the bath, and gain succour from his health, while feeling a shiver of shock at the coffin-like surround of the bath. I have to begin my own process of mourning Robert.
p.160-161 (18th December)
I go up to the children’s ward to add my last notes to Robert’s medical files. I read the medical notes for yesterday. These are some extracts:
7:15am Very weak
7:30am Fairly rapid deterioration. Pneumonia. 9:30am Very unwell. Morphine prescribed.
10:10am No spontaneous respiration. No pulse. Certified dead (by the Senior House Officer).
with death through my work… to really share the process with the dying and their families, I have to find a balance: somewhere between the raw pain they are feeling, and the defended state of some of the medical team, in order to be most useful to them. Weeks later, I go back to Robert’s medical file, and see that someone has written in the date of his death under the ‘date of discharge’ column, and then inscribed, in big letters, ‘RIP’.
To witness suffer