JOURNAL OFCLINICALMICROBIOLOGY, Mar. 2010, p. 972–976 Vol. 48, No. 3 0095-1137/10/$12.00 doi:10.1128/JCM.01829-09
Copyright © 2010, American Society for Microbiology. All Rights Reserved.
Performance of Fusidic Acid (CEM-102) Susceptibility Testing
Reagents: Broth Microdilution, Disk Diffusion, and Etest
Methods as Applied to
Staphylococcus aureus
䌤
Ronald N. Jones,
1,2Mariana Castanheira,
1* Paul R. Rhomberg,
1Leah N. Woosley,
1and Michael A. Pfaller
1,3JMI Laboratories, North Liberty, Iowa 523171; Tufts University School of Medicine, Boston, Massachusetts 021112; and
University of Iowa College of Medicine, Iowa City, Iowa 522423
Received 17 September 2009/Returned for modification 28 October 2009/Accepted 22 December 2009
Fusidic acid (CEM-102) is an established antistaphylococcal agent that has been used in clinical practice for more than 4 decades. The activity of fusidic acid against 778 isolates ofStaphylococcus aureuscollected from U.S. (53.8% were methicillin-resistantS. aureus[MRSA]) and Canadian (46.5% were MRSA) medical centers was assessed to determine the intermethod accuracy of the Clinical and Laboratory Standards Institute (CLSI) and Etest methods. Broth microdilution MIC results were compared by scattergram analysis to zone diameters around commercially available 5- and 10-g disks. Acceptable correlation (rⴝ0.74 to 0.76) was observed for the two disk concentrations, and applying breakpoints of<1g/ml (>22 mm) for susceptibility (S) and>4
g/ml (<19 mm) for resistance (R) provided 99.9% absolute intermethod categorical agreement. Reference CLSI MIC versus Etest MIC results (rⴝ0.77; 728 strains) showed 55.4% identical results and agreement of 99.7% ⴞ one log2 dilution. The diagnostic susceptibility testing reagents (including Etest) for fusidic acid
(CEM-102) performed at an excellent level of intermethod agreement for the proposed breakpoint criteria.
Staphylococcus aureus is a leading cause of skin and skin structure infections (SSSI), hospital- and community-acquired bacterial pneumonia, and nosocomial bloodstream infections (BSI) (3, 9, 14). Resistance to methicillin (oxacillin) amongS. aureus(MRSA) isolates ranges from 30% to more than 60% and is present worldwide (9, 10, 17). Furthermore, hospital-associated strains of MRSA (HA-MRSA) are often multidrug-resistant (MDR), exhibiting resistance to all-lactam agents, penems, carbapenems, aminoglycosides, macrolides, tetracy-clines, trimethoprim, and fluoroquinolones (3). The emer-gence of MRSA strains with reduced vancomycin susceptibility further reduces treatment options (4). Although community-associated MRSA (CA-MRSA) presently remains susceptible to clindamycin, most tetracyclines, and trimethoprim-sulfameth-oxazole, its emergence as a cause of infection in health care facilities is a growing source of concern (19). These resistance issues associated with such a virulent and prevalent pathogen have spurred the development of new antistaphylococcal agents, as well as reconsideration of the role of older agents with demonstrated antistaphylococcal activity (4, 10). Regard-ing MDR-MRSA, it has been suggested that the use of an agent such as fusidic acid may prove useful in treating these difficult infections and could help to delay the inevitable de-velopment of resistance to newer agents, such as linezolid and daptomycin (15). A promising feature of fusidic acid is the lack of cross-resistance with other antimicrobial classes as a result of the unique mode of action that inhibits bacterial protein synthesis at the translational stage (2, 12, 15).
Although fusidic acid has been used throughout much of the world for more than 40 years (1, 15), U.S. Food and Drug Administration (FDA) licensure has never been obtained, and the drug is not currently available in the United States. As a result, resistance to fusidic acid is extremely uncommon among U.S. strains of S. aureus, including methicillin-susceptible, MRSA, and vancomycin-intermediate and -resistant strains, as well as those strains with decreased susceptibility to linezolid and daptomycin. Despite the fact that in vitro susceptibility testing of fusidic acid has been performed for many years, fusidic acid is not presently included in the tables of the Clin-ical and Laboratory Standards Institute (CLSI), and interpre-tive breakpoints for MIC and disk diffusion testing of fusidic acid againstS. aureusare not available (11, 20).
Previous authors have demonstrated that susceptibility of staphylococci to fusidic acid may be indicated at MICs of
ⱕ0.25,ⱕ0.5, orⱕ1g/ml and resistance at MICs ofⱖ2g/ml (11, 15, 20). Recently, Skov et al. (20) utilized CLSI reference broth microdilution and disk diffusion methods to propose staphylococcal susceptibility interpretive criteria ofⱕ0.5g/ml (ⱖ21 mm) and resistance criteria ofⱖ2g/ml (ⱕ18 mm). The EUCAST (13) organization has selectedⱕ1g/ml as suscep-tibility breakpoint for MIC testing. In the present study, we provide additional fusidic acid MIC and disk diffusion data to support the findings of Skov et al. (20) or EUCAST (13) and, in addition, evaluate the utility of the Etest (AB Biodisk, Solna, Sweden) methodology for testing this agent against a large North American collection ofS. aureusstrains (13, 20).
A total of 778 nonduplicate clinical isolates of S. aureus
(52% MRSA) from patients with SSSI or BSI were obtained from more than 30 medical centers in the United States and Canada between 1997 and 2006. A subset of CA-MRSA iso-lates (50 strains from the United States) were tested as a * Corresponding author. Mailing address: 345 Beaver Kreek Centre,
Suite A, North Liberty, IA 52317. Phone: (319) 665-3370. Fax: (319) 665-3371. E-mail: [email protected].
䌤Published ahead of print on 6 January 2010.
972
on May 16, 2020 by guest
http://jcm.asm.org/
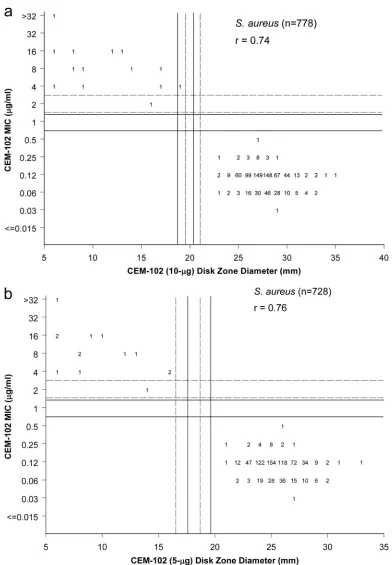
FIG. 1. (a) Scattergram comparing fusidic acid (CEM-102) broth microdilution MIC results with zone diameters obtained with a 10-g fusidic acid disk for 778 isolates ofS. aureus. The solid lines indicate the interpretive breakpoints proposed by Skov et al. (20). The broken lines indicate alternative MIC (ⱕ1g/ml) and disk diffusion (ⱖ22 mm) interpretive criteria consistent with EUCAST guidelines (13). Values show the number of isolates with each result. (b) Scattergram comparing fusidic acid (CEM-102) broth microdilution MIC results with zone diameters obtained with a 5-g fusidic acid disk for 728 isolates ofS. aureus. The solid lines indicate the interpretive breakpoints proposed by Skov et al. (20), and broken lines indicate a proposed higher MIC breakpoint ofⱕ1g/ml. Values show the number of isolates with each result.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:2.585.95.487.83.648.2]resistance subset only. All isolates (778 overall) were for-warded to the monitoring laboratory (JMI Laboratories, North Liberty, IA) for subsequent identification confirmation and reference antimicrobial susceptibility testing. Identification was performed using an automated system (Vitek; bioMerieux, Hazelwood, MO) or conventional manual methods, as re-quired.
All strains were tested by the CLSI broth microdilution method using prepared and validated frozen-form panels in cation-adjusted Mueller-Hinton broth (6). Fusidic acid (also known as CEM-102; Cempra) reference powder was obtained from Cempra Pharmaceuticals (Chapel Hill, North Carolina). Disk diffusion testing (all strains) was performed according to the CLSI method (5) using Mueller-Hinton agar and two disk concentrations (5 [728 strains] and 10g [778 strains]). The zone diameters were measured to the nearest mm using a caliper (Fig. 1a). Etest was performed as recommended by the manufacturer (AB Biodisk) using Mueller-Hinton agar, with inoculums of 1⫻108to 2⫻108CFU/ml (5) and incubation at
37°C in air for 18 to 24 h. The MIC was read at 80% inhibition relative to the growth of the control. The organism collection (excluding the CA-MRSA subset) (728 strains) was used to directly compare the two disk tests and the reference versus Etest MIC results (Fig. 1, 2, and 3). All fusidic acid-nonsus-ceptible strains (14 total) were found with each test method.
Quality control (QC) was performed concurrently with all testing determinations, usingS. aureusATCC 29213 (MIC) or ATCC 25923 (disks) and S. pneumoniae ATCC 49619. The proposed QC ranges for MIC and disk diffusion (10g) tests forS. aureusATCC 29213 and ATCC 25923 were 0.06 to 0.25 g/ml and 24 to 32 mm, respectively. The ranges forS.
pneu-moniae ATCC 49619 were 4 to 32 g/ml and 8 to 16 mm, respectively (16). Among 61 replicates, all QC values were within control ranges (8, 16).
Broth microdilution test results were compared to zone di-ameters of inhibition around 5- and 10-g fusidic acid disks by scattergram analysis and regression line equations. Interpre-tive zone size criteria were established using the error rate-bounded method of Metzler and DeHaan (18) as described by CLSI document M23-A3 (7). Correlation between the MIC methods (broth microdilution and Etest) was performed by scattergram and regression analysis. The essential agreement between the two methods was calculated, as well as the per-centage of results within plus-or-minus one log2dilution step, optimized to 95% (7).
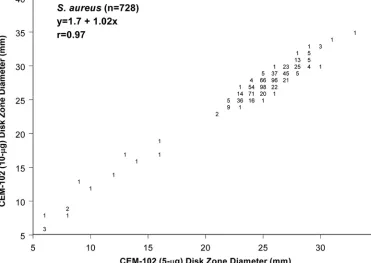
[image:3.585.101.472.74.337.2]Among strains of S. aureus tested in this study, 14 were resistant to fusidic acid as defined by a breakpoint ofⱖ2g/ml (Fig. 1a). Excellent correlation (r⫽0.74) was noted between broth microdilution MICs and zone diameters obtained with the 10-g disk test (Fig. 1a). Using a susceptible MIC break-point of ⱕ0.5 or ⱕ1 g/ml, correlate zone diameter break-points could be selected to accurately distinguish susceptible wild-type strains from less-susceptible isolates. Examples of breakpoints for the 10-g fusidic acid disk and the CLSI method ofⱖ21 mm for susceptibility andⱕ18 mm for resis-tance (see solid vertical and horizontal lines in Fig. 1a) were published by Skov et al. (20). Applying these to the results in Fig. 1a, the absolute intermethod categorical agreement was 99.9%, with only one minor error. A slight adjustment toⱖ22 mm (S) andⱕ19 mm (R) produced complete (100.0%) inter-method accord. Using a higher susceptibility MIC ofⱕ1g/ml (13) and the same correlate zone diameters also yielded a very FIG. 2. Scattergram showing the excellent correlation obtained with a 5-g and 10-g fusidic acid disk diffusion tests (728 strains). Values show the number of isolates with each result.
974 NOTES J. CLIN. MICROBIOL.
on May 16, 2020 by guest
http://jcm.asm.org/
high level of intermethod agreement (99.7%), but the modifi-cation of the zone diameter criteria toⱖ22 mm (S) andⱕ19 mm (R) returned the agreement to 99.9%. These results are in close agreement with those criteria suggested by Toma and Barriault (21), also using the CLSI method, a 10-g disk, and Mueller-Hinton medium.
Figures 1b and 2 demonstrate the excellent agreement for the 5-g fusidic acid (CEM-102) disk results and reference broth microdilution tests (Fig. 1b) and the outstanding corre-lation between the 5- and 10-g disk zone diameters (r⫽0.97) (Fig. 2). Applying the breakpoint criteria suggested by Skov et al. (20) resulted in perfect (100.0%) intermethod agreement between the CLSI broth microdilution and the 5-g disk re-sults. Although the 5-g disk for fusidic acid could certainly be standardized for use, the 10-g disk is more widely available or preferred, with at least three manufacturers internationally.
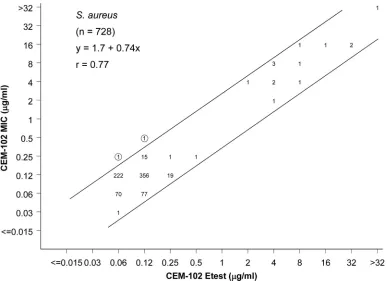
Figure 3 shows the correlation of the fusidic acid (CEM-102) reference broth microdilution results with the MICs produced by Etest. The essential agreement was 99.7%⫾one log2 dilu-tion step with 55.4% identical MIC results. A slight trend toward a lower MIC (31.2% of results were one log2dilution lower) was noted for the Etest. The Etest proved to be an acceptable alternative method to determine fusidic acid MIC results forS. aureus, with an intermethod agreement compa-rable to that for the CLSI disk diffusion method (e.g.,⬎99%). In summary, the in vitro diagnostic tests for fusidic acid (CEM-102) andS. aureusperformed at an acceptable level of intermethod agreement. The CLSI M07-A8 (6) broth microdi-lution method performed well, as did the reference agar disk diffusion method of CLSI M02-A10 (5), each showing excellent
intermethod categorical accuracy for either 5- or 10-g disks. For the 10-g disk, we propose zone diameter breakpoints of
ⱖ22 mm (ⱕ1g/ml), 20 to 21 mm (2g/ml), andⱕ19 mm (ⱖ4 g/ml) for the susceptible, intermediate, and resistant cate-gory, respectively, which would provide harmonization with current EUCAST criteria (13) (Table 1). Alternatively, the interpretive criteria of Skov et al. (20) would provide a compa-rable level of accurate intermethod performance. The Etest could be applied as an alternative MIC method with near-complete concordance by quantitative measure (MIC) and by category analyses. The potency of fusidic acid can be assessed with confi-dence by the standardized CLSI MIC and disk diffusion test methods and by the Etest during clinical trials in the United States and elsewhere. Such testing will be important in monitor-ing emergmonitor-ing resistant subpopulations, such as those that have appeared in several nations over the last few decades (15).
[image:4.585.99.486.67.348.2]This work was supported in part by educational/research grants from CEMPRA Pharmaceuticals.
[image:4.585.301.542.668.726.2]FIG. 3. Comparison of fusidic acid broth microdilution and Etest MIC results for 728 isolates ofS. aureus(r⫽0.77). Values show the number of isolates with each result. Solid lines represent the⫾1 log2dilution values for equivalent or identical MICs.
TABLE 1. Proposed interpretive breakpoints for fusidic acid againstS. aureus
Category MIC (g/ml) 10-g disk zone
diam (mm)
Susceptible ⱕ1 ⱖ22
Intermediate 2 20–21
Resistant ⱖ4 ⱕ19
on May 16, 2020 by guest
http://jcm.asm.org/
REFERENCES
1.Anderson, J. D.1980. Fusidic acid: new opportunities with an old antibiotic.
Can. Med. Assoc. J.122:765–769.
2.Besier, S., A. Ludwig, V. Brade, and T. A. Wichelhaus.2005. Compensatory adaptation to the loss of biological fitness associated with acquisition of
fusidic acid resistance inStaphylococcus aureus. Antimicrob. Agents
Che-mother.49:1426–1431.
3.Biedenbach, D. J., and R. N. Jones.2009. Multicenter evaluation of the in vitro activity of dalbavancin tested against staphylococci and streptococci in 5 European countries: results from the DECIDE Surveillance Program
(2007). Diagn. Microbiol. Infect. Dis.64:177–184.
4.Boucher, H. W., G. H. Talbot, J. S. Bradley, J. E. Edwards, D. Gilbert, L. B. Rice, M. Scheld, B. Spellberg, and J. Bartlett.2009. Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America. Clin.
Infect. Dis.48:1–12.
5.CLSI.2009. Performance standards for antimicrobial disk susceptibility tests; approved standard M02-A10, 10th ed. Clinical and Laboratory Standards Institute, Wayne, PA.
6.CLSI.2009. Methods for dilution antimicrobial susceptibility tests for bac-teria that grow aerobically; approved standard M07-A8, 8th ed. Clinical and Laboratory Standards Institute, Wayne, PA.
7.CLSI.2008. Development of in vitro susceptibility testing criteria and quality control parameters; approved guideline M23-A3, 3rd ed. Clinical and Lab-oratory Standards Institute, Wayne, PA.
8.CLSI.2009. Performance standards for antimicrobial susceptibility testing; 19th informational supplement. M100-S19. Clinical and Laboratory Stan-dards Institute, Wayne, PA.
9.Corey, G. R.2009.Staphylococcus aureusbloodstream infections: definitions
and treatment. Clin. Infect. Dis.48(Suppl. 4):S254–S259.
10.Cornaglia, G., and G. M. Rossolini.2009. Forthcoming therapeutic perspec-tives for infections due to multidrug-resistant Gram-positive pathogens. Clin.
Microbiol. Infect.15:218–223.
11.Coutant, C., D. Olden, J. Bell, and J. D. Turnidge.1996. Disk diffusion interpretive criteria for fusidic acid susceptibility testing of staphylococci by
the National Committee for Clinical Laboratory Standards method. Diagn.
Microbiol. Infect. Dis.25:9–13.
12.Dobie, D., and J. Gray. 2004. Fusidic acid resistance inStaphylococcus aureus. Arch. Dis. Child.89:74–77.
13.EUCAST.2009. Breakpoint tables for interpretation of MICs and zone diameters. The European Committee on Antimicrobial Susceptibility Testing. http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files /Disk_test_documents/EUCAST_breakpoints_v1.0_20091221.pdf. 14.Hoban, D. J., D. J. Biedenbach, A. H. Mutnick, and R. N. Jones.2003.
Pathogen of occurrence and susceptibility patterns associated with pneumo-nia in hospitalized patients in North America: results of the SENTRY
Antimicrobial Surveillance Study (2000). Diagn. Microbiol. Infect. Dis.45:
279–285.
15.Howden, B. P., and M. L. Grayson.2006. Dumb and dumber—the potential waste of a useful antistaphylococcal agent: emerging fusidic acid resistance in
Staphylococcus aureus. Clin. Infect. Dis.42:394–400.
16.Jones, R. N., and J. E. Ross.2009. Initial quality control (QC) ranges for CEM-102 (fusidic acid [FA]) using the CLSI multi-laboratory M23-A3 study design, abstr. D1435. Proc. 49th Intersci. Conf. Antimicrob. Agents Che-mother., American Society for Microbiology, Washington, DC.
17.Lode, H. M. 2009. Clinical impact of antibiotic-resistant Gram-positive
pathogens. Clin. Microbiol. Infect.15:212–217.
18.Metzler, C. M., and R. M. DeHaan.1974. Susceptibility tests of anaerobic
bacteria: statistical and clinical considerations. J. Infect. Dis.130:588–594.
19.Moran, G. J., A. Krishnadasan, R. J. Gorwitz, G. E. Fosheim, L. K. McDougal, R. B. Carey, and D. A. Talan.2006. Methicillin-resistantS. aureus
infections among patients in the emergency department. N. Engl. J. Med.
355:666–674.
20.Skov, R., N. Frimodt-Moller, and F. Espersen.2001. Correlation of MIC methods and tentative interpretive criteria for disk diffusion susceptibility testing using NCCLS methodology for fusidic acid. Diagn. Microbiol. Infect.
Dis.40:111–116.
21.Toma, E., and D. Barriault.1995. Antimicrobial activity of fusidic acid and disk diffusion susceptibility testing criteria for Gram-positive cocci. J. Clin.
Microbiol.33:1712–1715.
976 NOTES J. CLIN. MICROBIOL.