PEDIATRICS Volume 137 , number 3 , March 2016 :e 20154511
Getting Physical: The Hypothesis
Driven Physical Exam
Eric Balighian, MD, Michael A. Barone, MD, MPH
MONTHLY FEATURE
Department of Pediatrics, Johns Hopkins University School of Medicine, Baltimore, MarylandDOI: 10.1542/peds.2015-4511 Accepted for publication Dec 14, 2015
Address correspondence to Michael A. Barone, MD, MPH, Johns Hopkins University School of Medicine, Charlotte Bloomberg Children’s Hospital, 1800 Orleans St, Suite 8442, Baltimore, MD 21287. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2016 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no fi nancial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential confl icts of interest to disclose.
The value of teaching at the patient’s bedside has been recognized by generations of clinical teachers and students. In today’s complex and fast-paced medical environment, clinical instructors teach at the bedside less frequently than in the past.1,2
When learning the physical examination, medical students are often taught a series of 100+ anatomy-focused maneuvers.3
The “head-to-toe” approach can help students practice complex maneuvers and develop an awareness of normal findings, but it has limitations in emphasizing the diagnostic relevance of the physical examination.4
Teachers should guide students to transition from a head-to-toe physical examination to one used to support or refute potential diagnoses.
Emphasizing the physical examination’s critical role in clinical reasoning can help to support improved diagnostic skills5,6 and may lead to a cost
conscious approach to testing. Numerous recommendations in the Choosing Wisely compendium highlight the critical role of the physical examination in high value care.7 As part of the ongoing
Council on Medical Student Education in Pediatrics series on skills used by great clinical teachers, this article introduces the Hypothesis Driven Physical Exam (HDPE).5,6
CONNECTING THE PHYSICAL EXAMINATION TO CLINICAL REASONING
An overview of clinical reasoning has been previously outlined in the series of articles from the Council on Medical Student Education in Pediatrics.8 Perhaps the most
important concept relevant to the physical examination is the search for, or anticipation of, specific findings identified from the history to confirm or exclude diagnoses. Experienced clinical teachers do this without conscious thought by activating stored medical knowledge. The sum of their learning and experience is bundled in the form of illness scripts: packaged information, which consists of memory points on mechanism, epidemiology, natural history, and clinical presentation of disease. Emphasizing how certain elements of the physical examination link to the “clinical presentation” or to other parts of an illness script is a fundamental element of teaching the HDPE.9
THE HDPE IN ACTION
Walking through a case can illustrate ways to emphasize the HDPE approach to clinical diagnosis.
A CASE
A 4-year-old boy is brought to clinic with a rash on his lower extremities. He is afebrile with
To cite: Balighian E and Barone MA. Getting Physical: The Hypothesis Driven Physical Exam. Pediatrics. 2016;137(3): e20154511
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
BALIGHIAN and BARONE
normal vital signs and is not ill appearing. The clinic nurse mentions to you the child seems to have petechiae on both legs. The student, preparing to see the patient, tells you she plans to ask questions about recent fever, illness, trauma, exposures, and travel, as well as the child’s immunization history.
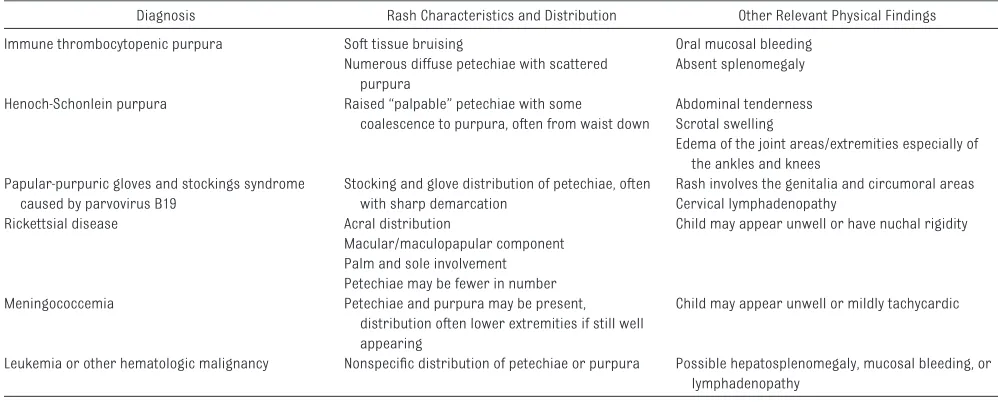
You quickly guide the student through a differential diagnosis of lower extremity petechiae in a well-appearing, afebrile child by using a HDPE framework. The differential diagnosis, limited for this example, would include immune thrombocytopenic purpura, Henoch-Schonlein purpura, and papular-purpuric gloves and stockings syndrome caused by parvovirus B19. You also caution the student not to miss a potentially devastating diagnosis such as rickettsial disease, meningococcemia, and leukemia. Thus, the key features of the physical examination would be useful to consider (Table 1).
PROMOTING AND INTEGRATING THE HDPE INTO DAILY PRACTICE: STRATEGIES
Direct Observation
You elect to join the student and directly observe her assess the patient.
1. Ask the student for her initial differential diagnosis after she gathers the history but before she proceeds with the physical examination. When appropriate, explain this teaching moment respectfully to the patient and the parent at the bedside.
2. Guide the student toward physical examination findings, which help support or exclude possible diagnoses.
3. Observe the student performing the physical examination and give feedback on her physical examination skills.
4. Reconsider the differential diagnosis again, emphasizing how it may have changed after the examination.
5. Supplement the student’s
differential diagnosis with additional considerations if needed, and then demonstrate the examination features, which help to discriminate among the additional choices.
This strategy can also be used when listening to a student’s clinical
presentation. Prompts such as, “What physical findings, present or absent, could help you to differentiate among the diagnoses?” When doing this, try to then dedicate some time to reviewing the physical examination at the bedside.
Reviewing Notes
You read the student’s note on the 4-year-old boy with petechiae. The note includes many nonrelevant findings that do not help support the student’s assessment or plan.
1. Inform the student in advance that the physical examination sections of written notes are reviewed for diagnostic relevance and reasoning.
2. Review the note with specific attention to:
⚬ The student’s documentation of relevant parts of the examination. For example, a detailed description of the distribution of the petechiae
⚬ Negative findings of importance. For example, lack of
splenomegaly.
2
TABLE 1 Key Features of the Physical Examination
Diagnosis Rash Characteristics and Distribution Other Relevant Physical Findings Immune thrombocytopenic purpura Soft tissue bruising Oral mucosal bleeding
Numerous diffuse petechiae with scattered purpura
Absent splenomegaly Henoch-Schonlein purpura Raised “palpable” petechiae with some
coalescence to purpura, often from waist down
Abdominal tenderness Scrotal swelling
Edema of the joint areas/extremities especially of the ankles and knees
Papular-purpuric gloves and stockings syndrome caused by parvovirus B19
Stocking and glove distribution of petechiae, often with sharp demarcation
Rash involves the genitalia and circumoral areas Cervical lymphadenopathy
Rickettsial disease Acral distribution Child may appear unwell or have nuchal rigidity Macular/maculopapular component
Palm and sole involvement Petechiae may be fewer in number Meningococcemia Petechiae and purpura may be present,
distribution often lower extremities if still well appearing
Child may appear unwell or mildly tachycardic
Leukemia or other hematologic malignancy Nonspecifi c distribution of petechiae or purpura Possible hepatosplenomegaly, mucosal bleeding, or lymphadenopathy
TABLE 2 Script Sorting Grid
Red Eye Preauricular Lymph Node Bilateral Purulent Exudate Chemosis
Viral conjunctivitis ++ + +/− +
Bacterial conjunctivitis — — ++ ++
Allergic conjunctivitis — ++ – +++
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
PEDIATRICS Volume 137 , number 3 , March 2016 ⚬ A patient's assessment and
differential diagnosis supported by the physical examination.
3. Guide the student through making connections between physical findings and the diagnostic possibilities.
4. Follow-up with review of subsequent notes for improvement.
Small Group Teaching
You decide to discuss the case of the child with petechiae the following day with multiple students in a case-based learning session. One student presents the patient’s history and then you facilitate a discussion.
1. Ask each student to list a limited number of important features they would seek on the patient’s physical examination. “Based on the patient’s history thus far, and our working differential diagnosis, what are 3 or 4 specific findings you would look for on the patient’s physical exam?” (eg, palpable petechiae, splenomegaly, mucosal lesions, joint swelling).
2. Guide the students further: “How would each physical finding, or lack of the finding, support your diagnostic hypotheses?”
Additional Learning Exercises
Emphasizing the physical examination’s role in clinical
reasoning can also be accomplished by assigning students brief learning exercises before or after a patient encounter or clinic session. Examples of such exercises include script sorting and the use of visual Venn diagrams.9 These exercises
can be completed by the student during a prescribed amount of time (overnight, before the next clinical session or patient, etc.) and can then be reviewed with a preceptor.
Script Sorting
Script sorting allows students to assign a weight or priority to certain competing diagnoses on the basis of elements of the history or, as in this example, the physical examination of a child with a red eye. The teacher and/or the student create the grid for the student to complete (Table 2).
Visual Venn Diagrams
A visual representation of the diagnostic possibilities can be an effective teaching method. Students are asked to contribute common or shared features (in areas where circles overlap) and should prioritize eliciting findings that are specific or differentiating (nonoverlapping areas). An example is presented for abdominal pain (Fig 1).
CONCLUSIONS
The HDPE can be used on a daily basis and need not be a time-intensive teaching strategy. Learning the physical examination in a rote head-to-toe manner may be an effective early learning strategy for students, but the physical examination’s clinical utility will be increased if driven by diagnostic hypotheses. The HDPE can be a stimulus to return to bedside teaching. Furthermore, the great clinical teacher can emphasize the role of the physical examination, putting focus on the important concepts of clinical reasoning and high value care.
ABBREVIATION
HDPE: Hypothesis Driven Physical Exam
REFERENCES
1. Crumlish CM, Yialamas MA, McMahon GT. Quantifi cation of bedside teaching by an academic hospitalist group. J Hosp Med. 2009;4(5):304–307
2. LaCombe MA. On bedside teaching. Ann Intern Med. 1997;126(3):217–220
3. Yudkowsky R, Downing S, Klamen D, Valaski M, Eulenberg B, Popa M. Assessing the head-to-toe physical examination skills of medical students.
Med Teach. 2004;26(5):415–419
4. Yudkowsky R, Otaki J, Lowenstein T, Riddle J, Nishigori H, Bordage G. A hypothesis-driven physical examination learning and assessment procedure for medical students: initial validity evidence. Med Educ. 2009;43(8):729–740
5. Yudkowsky R, Otaki J, Bordage G, Lowenstein T, Riddle J, Nishigori H. Hypothesis-driven physical examination student handbook. MedEdPORTAL Publications; 2011. Available at: https:// www. mededportal. org/ publication/ 8294. Accessed December 14, 2015
6. Nishigori H, Masuda K, Kikukawa M, et al. A model teaching session for the hypothesis-driven physical examination. Med Teach. 2011;33(5):410–417
7. Choosing Wisely Master List. ABIM Foundation. Available at: www. choosingwisely. org/ clinician- lists/ . Accessed October 2, 2015
8. Fleming A, Cutrer W, Reimschisel T, Gigante J. You too can teach clinical reasoning! Pediatrics. 2012;130(5):795–797
9. Stuart E, Slavin S, Butani L,
Blankenburg R, Konopasek L. Clinical reasoning. In: Morgenstern B, ed.
Guidebook for Clerkship Directors, Chapter 8. North Syracuse, NY: Gegensatz Press; 2012
3
FIGURE 1
Abdominal pain.
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
DOI: 10.1542/peds.2015-4511 originally published online February 23, 2016;
2016;137;
Pediatrics
Eric Balighian and Michael A. Barone
Getting Physical: The Hypothesis Driven Physical Exam
Services
Updated Information &
http://pediatrics.aappublications.org/content/137/3/e20154511 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/137/3/e20154511#BIBL This article cites 6 articles, 1 of which you can access for free at:
Subspecialty Collections
dev_sub
http://www.aappublications.org/cgi/collection/teaching_curriculum_ Teaching/Curriculum Development
b
http://www.aappublications.org/cgi/collection/medical_education_su Medical Education
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml Information about ordering reprints can be found online:
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
DOI: 10.1542/peds.2015-4511 originally published online February 23, 2016;
2016;137;
Pediatrics
Eric Balighian and Michael A. Barone
Getting Physical: The Hypothesis Driven Physical Exam
http://pediatrics.aappublications.org/content/137/3/e20154511
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2016 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news