Dietary Intakes
Full text
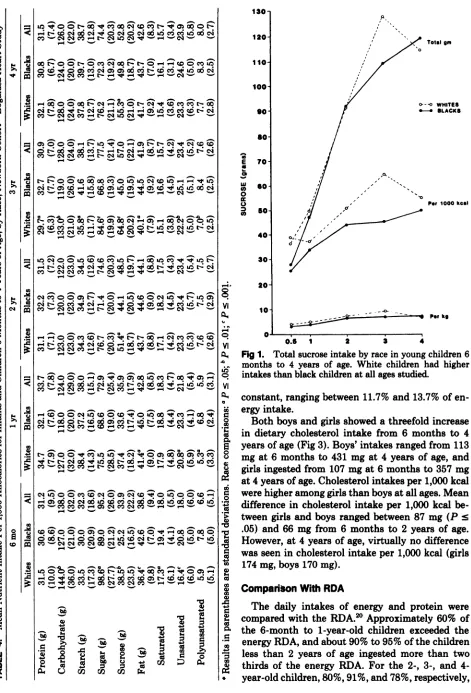
Figure
Related documents
The trials different groups of people face today are the same trials once faced by the millions of Americans who preceded us.. Today’s women and men can fight together for rights
Other categories including research supervision ability and student research funding, which fell under the main theme of fair research, and finally the theme of just management
Date of Birth Driver’s License Number State Marital Status Number of Dependents.. Corporation/LLC/Partnership Name Federal Tax Identification Number (EIN) D &
The distributor may seek to limit the producer’s right to terminate until distributor has recouped its advance (assuming it has given the producer an advance.) Another
It is possible that a segment is stored at multiple peers in the set cover, in this case the requesting client can pick a peer based on some other criteria such as delay or number
• Storage node - node that runs Account, Container, and Object services • ring - a set of mappings of OpenStack Object Storage data to physical devices To increase reliability, you
Political Parties approved by CNE to stand in at least some constituencies PLD – Partido de Liberdade e Desenvolvimento – Party of Freedom and Development ECOLOGISTA – MT –
While anxiety may be a common feature of attending any con- sultation [19], we have shown that it might be height- ened in the case of paediatric diabetes consultations because
