Journal of Pakistan Association of Dermatologists. 2014;24 (3):270-274.
Address for correspondence Dr. Feroza Fatima,
Department of Dermatology, Abbasi Shaheed Hospital, Karachi Email: [email protected]
Case Report
A case report of congenital insensitivity to pain
and anhidrosis
Feroza Fatima, Naseema Kapadia, Maria Farooqi, Maryam Noshad, Shehmona Faisal, Sehar Athar, Nadia, Maria, Yosuf
Department of Dermatology, Abbasi Shaheed Hospital, Karachi, Pakistan
Abstract Congenital insensitivity to pain with anhidrosis (CIPA) is a rare disorder characterized by episodes of fever and pain insensitivity despite the fact that all other sensory modalities remain intact or minimally impaired. Other clinical features are self-mutilated behaviour, mental retardation and anhydrosis. We present a case first time from Pakistan, 9- and 4-year-old brother and sister respectively, diagnosed as CIPA clinically with the above-mentioned clinical characteristics.
Key words
Congenital, insensitivity, pain, anhidrosis, Pakistan.
Introduction
Congenital insensitivity to pain with anhidrosis (CIPA) or hereditary sensory and autonomic neuropathy (type IV) is an extremely rare autosomal recessive disorder.1 Less than 60 cases are available in the medical literature.2
Patients with CIPA show an absence of unmyelinated fibers and loss of small myelinated ones.3,4,5 This results into absence of epidermal nerve fibers and fibers around the sweat glands which forms the morphological basis of analgesia and anhidrosis in CIPA. Senses of touch and pressure are not impaired in these patients.1Self-mutilating behavior occurs due to a lack of pain perception. CIPA patients may injure themselves using their teeth.6 Finger biting, laceration and ulceration of the tongue; lips and oral mucosa are frequently observed. These ulcers lead to several local and systemic
problems, such as infection, tongue bleeding, malnutrition, halitosis. Oral self-mutilation is found to decrease with age and with social and/or emotional development of the patients, however not completely eliminated.6,7 Furthermore, dental luxation and severe attrition are normally found.
Case Report
Journal of Pakistan Association of Dermatologists. 2014;24 (3):270-274.
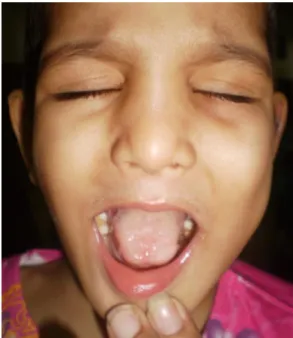
Figure 1 Bitten and scarred tongue irregular tip.
Figure 2 Unerupted permanent teeth after extraction of primary teeth.
Figure 3 Multiple ulcers on hands.
Figure 4 Loss of big and small toes and secondary infection of soft tissues.
There was also history of multiple hospital admissions with recurrent attacks of high grade fever along with febrile fits. A full sepsis work-up showed no positive results and cause of the fever was not found. Frequency of fever episodes aggravated during summer months. Fever was relieved with cold sponging along with some intravenous medication during hospital admissions.
There was also history of self-mutilating behavior since early childhood. After their teeth started to grow in, they began to chew their fingers and bit off the tip of their tongue and lips. This self-mutilating behavior exhibited an absence of normal reaction to painful stimuli such as falls, cuts, and injections (e.g. for vaccinations). Few of their primary teeth were extracted because of repeated tongue biting by a dental surgeon.
Journal of Pakistan Association of Dermatologists. 2014;24 (3):270-274.
Their tongue had been bitten off and tip was irregular in shape (Figure 1). Their teeth were irregularly placed and few of them were un-erupted after extraction of primary teeth by dentist (Figure 2). They had scars from injuries on different parts of body including scalp. Deformed interphalangeal joints of fingers
(Figure 3) and toes along with multiple ulcers
on both feet were obvious finding on examination. The big toes and 5th toes bilaterally of male sibling were missing, because of multiple traumas and self-mutilation (Figure 4). The peripheral pulses were normal.
Most of the nails of hands and feet were dystrophic because of self removal. Scalp hair was thin, sparse and brown in color. Neurologic examination revealed depressed deep tendon reflexes and decreased tactile sensitivity. The patients seemed to respond appropriately to thermal stimuli. However, there was no reaction to painful stimuli.
They showed normal lacrimation, salivation and corneal reflex. They were active and of normal intelligence, but in speaking, they could utter only a few words like mamma, baba etc.
Paraclinical investigations were common to both patients. Laboratory examination including complete blood count, serum electrolytes, liver function tests, renal function tests, uric acid, creatinine kinase, were normal in range. Radiographs of left leg (brother) and left arm (sister) showed fracture of tibia and dislocation of elbow and wrist joint respectively, accidently noticed by their parents.
Discussion
Hereditary sensory and autonomic neuropathies (HSAN) are a group of disorders characterized by insensitivity to noxious stimuli and
autonomic dysfunction, associated with pathological abnormalities of the peripheral nerves. Five types of HSANs have been identified by Dyck.8 Type IV congenital insensitivity to pain with anhidrosis (CIPA) is characterized by inexplicable episodes of fever at an early age, in addition to insensitivity to pain and self-mutilation. Those affected do not sweat or cry.9 Though CIPA is a very rare disorder, more than 300 cases have been reported from Japan, with about 60 cases reported from the United States of America.10
CIPA, which was first described in 1951, results from a defect in neural crest differentiation and the system responsible for pain and temperature sensations, the first order afferent system. Ultrastructural and morphometric studies of the peripheral nerves reveal loss of unmyelinated and small myelinated fibers and no innervation to the sweat glands. These features suggest that a defect in the differentiation and migration of neuronal crest elements and possible degradation of the nerve growth factor/neurotrophic tyrosine receptor kinase 1 (NGF/NTRK 1) pathway may be responsible for CIPA.18 Mutation of this gene inhibits the development of nerve growth factor (NGF), and dependent sensory and autonomic neurons during the embryonic period.11 NGF plays a crucial role in pain generation and hyperalgesia during episodes of acute and chronic pain.11 Insensitivity to pain can cause self-mutilating behavior for these patients.4 In most cases, bite injuries to the tongue, lips and fingers begin with the eruption of the primary teeth.12
Journal of Pakistan Association of Dermatologists. 2014;24 (3):270-274.
and full denture therapy.3But it is an extremely radical treatment and causes bone loss.
We believe that treatment of these patients depends on the patients’ age and intelligence, as well as, the parents’ attitude and cooperation. Due to painless injuries, the bones, joints and soft tissues of the extremities, as well as, the orbits, nasal cavities and oral cavity undergo mutilating effects, for which the parents seek medical attention and treatment.13 Bar-On et al.13 have also described preventive measures for orthopedic complications such as use of special shoe ware, periods of non weight-bearing, surgical wide debridement and curative osteotomy for deformity. Sathiaseelan and Rayar
.
14 have called CIPA, the "mystery of broken bones" after the case of a 15-years-old boy who was wrongly labeled as a case of osteogenesis imperfecta due to recurring fractures since the age of 4.Skin complications due to anhidrosis15 and ocular complications due to painless injuries16,17 are not uncommon. On cutaneous examination, patients may has swelling, changes of dry gangrene, discoloration and ulceration involving both great toes and the tips of fingers and toes, along with cellulitis.18
Prevention of self-mutilation in CIPA patients should involve a team of multidisciplinary physicians, as well as, a dentist. Treatment of these patients is quite difficult and information regarding this issue is scarce in dental literature. Therefore, treatment of these patients is diverse and predicated upon individual cases. Conventional radical full mouth teeth extraction should be avoided in CIPA patients and it should be the last alternative therapy.
References
1. Nagasako EM, Oaklander AL, Dworkin RH. Congenital insensitivity to pain: an update. Pain. 2003;101:213-9.
2. Schalka MM, Corrêa MS, Ciamponi AL. Congenital insensitivity-to-pain with anhidrosis (CIPA): a case report with 4-year follow-up. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:769-73. 3. Kouvelas N, Terzoglou C. Congenital
insensitivity to pain with anhidrosis: case report. Pediatr Dent. 1989;11:47-51. 4. Nolano M, Crisci C, Santoro L et al. Absent
innervation of skin and sweat glands in congenital insensitivity to pain with anhidrosis. Clin Neurophysiol. 2000;111:1596-601.
5. Erdem TL, Ozcan I, Ilgüy D, Sirin S. Hereditary sensory and autonomic neuropathy: review and a case report with dental implications. J Oral Rehabil. 2000;27:180-3.
6. Neves BG, Roza RT, Castro GF. Traumatic lesions from congenital insensitivity to pain with anhidrosis in a pediatric patient: dental management. Dent Traumatol. 2009;25:545-9.
7. Dyck PJ. Inherited neuronal degeneration and atrophy affecting peripheral motor, sensory, and autonomic neurons. In: Dyck PJ, Thomas PK, Lambert EM (Editors). Peripheral Neuropathy. Philadelfia: WB Saunders; 1984. P.1600-55.
8. Schulman H, Tsodikow V, Einhorn M, Levy Y et al. Congenital insensitivity to pain with anhidrosis (CIPA): the spectrum of radiological findings. Pediatr Radiol. 2001;31:701-5.
9. Indo Y, Tsuruta M, Hayashida Y et al. Mutations in the TRKA/NGF receptor gene in patients with congenital insensitivity to pain with anhidrosis. Nat Genet. 1996;13:485-8.
10. Congenital insensitivity to pain with anhidrosis. Wikipedia. 13 September, 2007 11. Hefti FF, Rosenthal A, Walicke PA et al.
Novel class of pain drugs based on antagonism of NGF. Trends Pharmacol Sci. 2006;27:85-91.
Journal of Pakistan Association of Dermatologists. 2014;24 (3):270-274.
13. Bar-On E, Weigl D, Parvari R, Katz K et al. Congenital Insensitivity to Pain. J Bone Joint Surg Br. 2002;84:252-7.
14. Sathiaseelan S, Rayar U. The mystery of the broken bones. CMAJ. 2003;169:1189-90. 15. Hafez HZ, Awad SM. Congenital
insensitivity to pain with anhidrosis. Egypt Dermatol Online J. 2007;3:5.
16. Levy J, Monos T, Levy J et al. Intrasinus wood foreign body causing orbital cellulitis in congenital insensitivity to pain with
anhidrosis. Ophthal Plast Reconstr Surg. 2004;201:81-3.
17. Amano S, Fukuoka S, Usui T et al. Ocular manifestations of congenital insensitivity to pain and anhidrosis. Am J Ophthalmol. 2006;141:472-7.